Self vs. Other Raters’ Assessment of Emotional Intelligence in Private and Public Hospitals: A Comparative Study



Abstract
1. Introduction
2. Emotional Intelligence
2.1. Emotional Intelligence Models
2.1.1. Ability Models
2.1.2. Trait Models
2.1.3. Mixed Models
2.2. Emotional Intelligence in Healthcare
3. Research Theoretical Model and Hypotheses Development
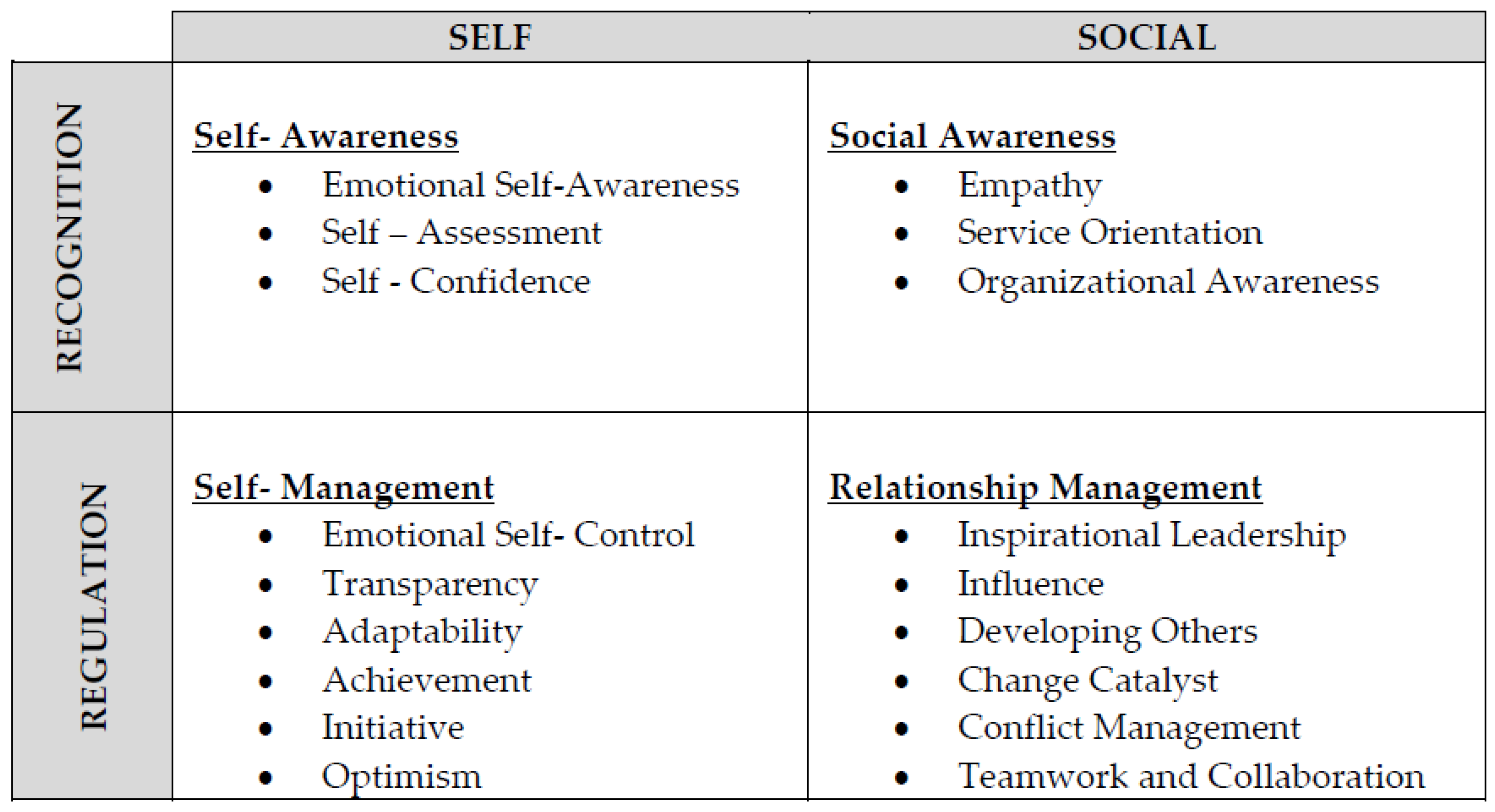
- Self-awareness consists of emotional self-awareness, self-assessment, and self-confidence.
- Social awareness dimension consists of empathy, service orientation, and organizational awareness.
- Self-management dimension consists of emotional self-control, transparency, adaptability, achievement, initiative, and optimism.
- Relationship management dimension consists of inspirational leadership, influence, developing others, change catalysts, teamwork and collaboration, and conflict management.
Research Hypotheses
4. Research Methodology
4.1. Research Population and Sample
4.2. Data Collection Instrument
4.3. Validity and Reliability
5. Findings
6. Discussion
6.1. The Levels of Emotional Intelligence among Managers of Private and Public Hospitals
6.2. The Differences between Self and Other Raters’ Assessments of the Levels of Emotional Intelligence among Managers in the Private Hospitals
6.3. The Differences between Self and Other Raters’ Assessments of the Levels of Emotional Intelligence among Managers in the Public Hospitals
7. Conclusions
Findings of the Study
8. Recommendations and Implications
- The need to raise emotional intelligence awareness in Jordan’s public and private hospitals through the development of specialized training programs (Aldaod et al. 2019; Al-Hamdan et al. 2017). Such training should be given for both managerial and non-managerial employees in ways that incorporate the concept of emotional intelligence and emphasize the practical aspect of it.
- There is a need to acknowledge that emotional intelligence can be learned and developed through training and practice as well (Daher 2015; Aldaod et al. 2019). This includes developing new criteria for recruiting managers in public and private hospitals in Jordan, considering emotional intelligence dimensions, and knowing that emotional intelligence is linked with superior leadership performance (Goleman 2001, 2017).
- The need to design and customize programs that help exploit more-practiced emotional intelligence dimensions of self-awareness and social awareness. Such dimensions should be considered as a foundation to improve less-practiced dimensions of self-management and relationship management for managers in public and private hospitals. This implies that emotional intelligence development is an incremental process (Goleman and Cherniss 2001; Cartwright and Pappas 2008; Daher 2015).
- The need to develop a 360-degree feedback process for managers in Jordanian public and private hospitals in which supervisors, peers, and subordinates provide direct reports on performance feedbacks. Thus, in addition to self-perception, managers can receive inputs and insights about how others in their professional context perceive and evaluate them. In this way, the gaps between self and others’ assessments of the managers can be minimized.
9. Limitations and Future Research
- Respondents were unfamiliar with emotional intelligence and its relationship with effective leadership and better organizational outcomes.
- Researchers faced some difficulties in distributing the questionnaires due to a lack of published data about the number of managers in Jordanian hospitals. Therefore, researchers were forced to go to each target hospital individually in cooperation with human resources managers in the selected hospitals. Then, the number of the conveniently located managers and raters was determined by the HR managers, while two private hospitals refused to participate due to privacy policies.
- Researchers found few previous studies that investigated the levels of managerial emotional intelligence and differences among managers and other raters in the public and private health sectors in Jordan.
- Conduct similar research in other governorates’ hospitals as well as hospitals with less than 100 beds, including more raters for a manager as each rater sees different aspects of the person (Wolff 2005). This can help reveal more interpretable results and more data to evaluate the gap between self and raters’ assessments of emotional intelligence.
- Replicate the study with an investigation of the emotional intelligence competencies within the emotional intelligence dimensions to address more areas of deficiency that might be uncovered.
- Understanding factors that influence the emotional intelligence of managers in Jordan’s public and private hospitals would be an important topic for future research.
- Replicate the study to reveal more comprehensive results on the overall levels of emotional intelligence for managerial and non-managerial employees in the Jordanian hospitals.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Alawneh, Afnan R., and Rateb J. Sweis. 2016. The relationship between emotional intelligence level and the effectiveness of a project manager: The case of Jordan. International Journal of Information, Business and Management 8: 13. [Google Scholar]
- Aldaod, Sawsan M., Rateb J. Sweis, Afnan R. Alawneh, and Mais Jaradat. 2019. Emotional intelligence effect in health sector: A literature review. International Journal of Information, Business and Management 11: 8–94. [Google Scholar]
- Al-Hamdan, Zaid, Islam Ali Oweidat, Ibrahim Al-Faouri, and Estelle Codier. 2017. Correlating Emotional Intelligence and Job Performance among Jordanian Hospitals’ Registered Nurses. In Nursing Forum 52: 12–20. [Google Scholar] [CrossRef] [PubMed]
- Araujo, Segundo Vito Aliaga Araujo, and Scott. N. Taylor. 2012. The influence of emotional and social competencies on the performance of Peruvian refinery staff. Cross Cultural Management: An International Journal 19: 19–29. [Google Scholar] [CrossRef]
- Alsayyed, Niveen M., Taghrid S. Suifan, Rateb J. Sweis, and Basheer A. Kilani. 2020. The impact of transformational leadership on organisational performance case study: The University of Jordan. International Journal of Business Excellence 20: 169–90. [Google Scholar] [CrossRef]
- Andrei, Federica, A. B. Siegling, Ariel M. Aloe, Bruno Baldaro, and Konstantinos V. Petrides. 2016. The incremental validity of the Trait Emotional Intelligence Questionnaire (TEIQue): A systematic review and meta-analysis. Journal of Personality Assessment 98: 261–76. [Google Scholar] [CrossRef]
- Bar-On, Reuven. 1997. Emotional intelligence. International Journal of Sociology and Social Policy 29: 164–75. [Google Scholar]
- Bar-On, Reuven. 2004. The Bar-On Emotional Quotient Inventory (EQ-i): Rationale, description and summary of psychometric properties. In Measuring Emotional Intelligence: Common Ground and Controversy. Hauppauge: NovaScience Publishers, pp. 115–45. [Google Scholar]
- Bibi, Akthtar, A. Saleem, M. Adnan Khalid, and N. Shafique. 2020. Emotional intelligence and aggression among university students of Pakistan: A correlational study. Journal of Aggression, Maltreatment & Trauma 29: 1–15. [Google Scholar]
- Bibi, Saleha, Sirda Saqlain, and Bushra Mussawar. 2016. Relationship between emotional intelligence and self esteem among Pakistani university students. Journal of Psychology & Psychotherapy 6: 1–6. [Google Scholar]
- Boyatzis, Richard E., and Fabio Sala. 2004. The Emotional Competence Inventory (ECI). In Measuring Emotional Intelligence. Edited by Glenn Geher. Hauppauge: Nova Science Publishers, pp. 147–80. [Google Scholar]
- Burckle, M., and Richard Boyatzis. 1999. Can You Assess Your Own Emotional Intelligence? Evidence Supporting Multi-Rater Assessment. Boston: Hay/Mc Ber Research Report. [Google Scholar]
- Caruso, David R., John D. Mayer, and Peter Salovey. 2002. Relation of an ability measure of emotional intelligence to personality. Journal of Personality Assessment 79: 306–20. [Google Scholar] [CrossRef]
- Cartwright, Susan, and Constantinos Pappas. 2008. Emotional intelligence, its measurement and implications for the workplace. International Journal of Management Reviews 10: 149–71. [Google Scholar] [CrossRef]
- Cavallo, Kathleen, and Dottie Brienza. 2002. Emotional Competence and Leadership Excellence at Johnson & Johnson: The Emotional Intelligence and Leadership Study. Available online: http://www.eiconsortium.org/reports/jj_ei_study.html (accessed on 1 February 2018).
- Chan, Joanne C., Emily N. Sit, and Woonming Lau. 2014. Conflict management styles, emotional intelligence and implicit theories of personality of nursing students: A cross-sectional study. Nurse Education Today 34: 934–39. [Google Scholar] [CrossRef]
- Cherry, Michael Albert. 2011. Health Care Leadership: “Emotional Intelligence Competencies of Hospitalist Leaders”. Ph.D. dissertations, Olivet Nazarene University, Bourbonnais, IL, USA. Paper 20. [Google Scholar]
- Cope, Vicki, and Melanie Murray. 2017. Leadership styles in nursing. Nursing Standard 31: 61–70. [Google Scholar] [CrossRef] [PubMed]
- Day, Arla L., and Sarah A. Carroll. 2004. Using an ability-based measure of emotional intelligence to predict individual performance, group performance, and group citizenship behaviours. Personality and Individual Differences 36: 1443–58. [Google Scholar] [CrossRef]
- Daher, Nick. 2015. Emotional and Cultural Intelligences as an Assessment Tool for Recruiting, Selecting and Training Individual Candidates. International Journal of Business & Public Administration 12: 1. [Google Scholar]
- De Haro, Jose Manuel, Juan Luis Castejon, and Raquel Gilar. 2020. Personality and salary at early career: The mediating effect of emotional intelligence. The International Journal of Human Resource Management 31: 1844–62. [Google Scholar] [CrossRef]
- Extremera, Natalio, Sergio Mérida-López, Nicolas Sánchez-Álvarez, and Cirenia Quintana-Orts. 2018. How does emotional intelligence make one feel better at work? The mediational role of work engagement. International Journal of Environmental Research and Public Health 15: 1909. [Google Scholar] [CrossRef]
- Fleenor, John W., James W. Smither, Leanne E. Atwater, Phillip W. Braddy, and Rachel E. Sturm. 2010. Self–other rating agreement in leadership: A review. The Leadership Quarterly 21: 1005–34. [Google Scholar] [CrossRef]
- Gastwirth, Joseph L., Yulia R. Gel, and Weiwen Miao. 2009. The impact of Levene’s test of equality of variances on statistical theory and practice. Statistical Science 24: 343–60. [Google Scholar] [CrossRef]
- Gilar-Corbí, Raquel, Teresa Pozo-Rico, Barbara Sánchez, and Juan Luis Castejón. 2018. Can emotional competence be taught in higher education? A randomized experimental study of an emotional intelligence training program using a multimethodological approach. Frontiers in Psychology 9: 10–39. [Google Scholar] [CrossRef]
- Giorgi, Gabriele, Milda Perminienė, Francesco Montani, Javier Fiz-Perez, Nicola Mucci, and Giulio Arcangeli. 2016. Detrimental effects of workplace bullying: Impediment of self-management competence via psychological distress. Frontiers in Psychology 7: 60. [Google Scholar] [CrossRef] [PubMed]
- Goleman, Daniel. 2001. An EI-based theory of performance. In The Emotionally Intelligent Workplace: How to Select for, Measure, and Improve Emotional Intelligence in Individuals, Groups, and Organizations. Edited by C. Cherniss and D. Goleman. San Francisco: Jossey-Bass, pp. 27–44. [Google Scholar]
- Goleman, Daniel. 2006. The socially intelligent. Educational Leadership 64: 76–81. [Google Scholar]
- Goleman, Daniel. 2017. Emocionálna Inteligencia. Bratislava: Citadella, p. 432. [Google Scholar]
- Goleman, Daniel, and Cary Cherniss. 2001. The Emotionally Intelligent Workplace: How to Select for, Measure, and Improve Emotional Intelligence in Individuals, Groups, and Organizations. San Francisco: Jossey-Bass. [Google Scholar]
- Goleman, Daniel, Richard E. Boyatzis, and Annie McKee. 2002. Primal Leadership: Learning to Lead with Emotional Intelligence. Boston: Harvard Business School Press. [Google Scholar]
- Goleman, Daniel, Richard E. Boyatzis, and Annie McKee. 2004. Primal Leadership: Learning to Lead with Emotional Intelligence. 303. Watertown: Harvard Business Review Press. [Google Scholar]
- Goleman, Daniel, Richard E. Boyatzis, and Annie McKee. 2013. Primal Leadership: Unleashing the Power of Emotional Intelligence. Boston: Harvard Business School Press. [Google Scholar]
- Haavisto, Elina, Maija Hupli, Nina Hahtela, Asta Heikkilä, Pirjo Huovila, Eeva-Liisa Moisio, Lea Yli-Koivisto, and Kirsi Talman. 2019. Structure and content of a new entrance exam to select undergraduate nursing students. International Journal of Nursing Education Scholarship 16: 1–15. [Google Scholar] [CrossRef] [PubMed]
- Hassali, Mohamed Azimi Ahmad, Rabia Hussain, Fahad Saleem, Qaiser Iqbal, Mohammad Arief, Akram Ahmad, and Sameer Dhingra. 2017. Perceived Emotional Intelligence and Its Association with the Demographic Characteristics among Pharmacy Students: A Cross-Sectional Study. Journal of Pharmacy Practice and Community Medicine 3: 108–13. [Google Scholar] [CrossRef]
- Hay, Michael. 2002. Strategies for survival in the war of talent. Career Development International 7: 52–55. [Google Scholar] [CrossRef]
- Higuchi, Yuji, Masatoshi Inagaki, Toshihiro Koyama, Yoshihisa Kitamura, Toshiaki Sendo, Maiko Fujimori, and Norihto Yamada. 2017. Emotional Intelligence and its Effect on Pharmacist and Pharmacy Students with Autistic-like Traits. American Journal of Pharmaceutical Education 81: 74. [Google Scholar]
- Johnson, Denni R. 2016. Emotional Intelligence and Public Health Education: A Prescriptive Needs Assessment. Pedagogy in Health Promotion 2: 193–200. [Google Scholar] [CrossRef]
- Jordan, Peter J., Neal M. Ashkanasy, Charmine E. Härtel, and Gregory S. Hooper. 2002. Workgroup emotional intelligence: Scale development and relationship to team process effectiveness and goal focus. Human Resource Management Review 12: 195–214. [Google Scholar] [CrossRef]
- Joseph, Dana L., and Daniel A. Newman. 2010. Emotional intelligence: An integrative meta-analysis and cascading model. Journal of Applied Psychology 95: 54. [Google Scholar] [CrossRef]
- Kaiser, K. E. 2009. Emotional Intelligence Abilities of the Physician Executive. Ph.D. dissertations, University of La Verne, La Verne, CA, USA. [Google Scholar]
- Kanesan, P., and Norsiah Fauzan. 2019. Models of emotional intelligence: A review. e-Bangi 16: 1–9. [Google Scholar]
- Kassymzhanova, A., and M. Mun. 2013. Emotional Intelligence as the Object of Research in Modern Psychology. Procedia-Social and Behavioral Sciences 82: 892–94. [Google Scholar] [CrossRef][Green Version]
- Kotzé, Martina, and Petrus Nel. 2017. Personal factor effects on authentic leadership. Journal of Psychology in Africa 27: 47–53. [Google Scholar] [CrossRef]
- Lawani, Uyi. 2016. Executives’ ability to conduct boundary spanning activities: The role of personality, emotional intelligence and trust. Journal of International Business Disciplines 11: 36–46. [Google Scholar]
- Lorincová, Silvia. 2018. Human resource and corporate culture: Gender-based differences in the assessment. Central European Journal of Labour Law and Personnel Management 1: 28–45. [Google Scholar]
- Magbity, J. B., A. M. A. Ofei, and D. Wilson. 2020. Leadership styles of nurse managers and turnover intention. Hospital Topics 98: 45–50. [Google Scholar] [CrossRef] [PubMed]
- Mahasneh, Ahmad Mohammed Mousa. 2013. Investigation relationship between emotional intelligence and personality traits among sample of Jordanian University students. Cross-Cultural Communication 9: 82–86. [Google Scholar]
- Mayer, John D., David R. Caruso, and Peter Salovey. 2016. The ability model of emotional intelligence: Principles and updates. Emotion Review 8: 290–300. [Google Scholar] [CrossRef]
- Mayer, John D., Peter Salovey, and David R. Caruso. 2004. Target Articles: Emotional Intelligence: Theory, findings, and implications. Psychological Iinquiry 15: 197–215. [Google Scholar] [CrossRef]
- McCleskey, Jim Allen. 2014. Emotional intelligence and leadership: A review of the progress, controversy, and criticism. International Journal of Organizational Analysis 22: 76–93. [Google Scholar] [CrossRef]
- Mérida-López, Sergio, Martin Sánchez-Gómez, and Natalio Extremera. 2020. Leaving the teaching profession: Examining the role of social support, engagement and emotional intelligence in teachers’ intentions to quit. Psychosocial Intervention 29: 141–51. [Google Scholar] [CrossRef]
- Meisler, Galit, and Eran Vigoda-Gadot. 2014. Perceived organizational politics, emotional intelligence and work outcomes: Empirical exploration of direct and indirect effects. Personnel Review 43: 116–135. [Google Scholar] [CrossRef]
- Miao, Chao, Ronald H. Humphrey, and Shanshan Qian. 2018. Emotional intelligence and authentic leadership: A meta-analysis. Leadership & Organization Development Journal 39: 679–690. [Google Scholar]
- Ministry of Health in Jordan MOH. 2018. Available online: https://corona.moh.gov.jo/en (accessed on 5 December 2022).
- Minárová, Minárová, Denisa Malá, and Filip Smutný. 2020. Emotional intelligence of managers in family businesses in Slovakia. Administrative Sciences 10: 84. [Google Scholar] [CrossRef]
- Mintz, Laura Janine, and James K. Stoller. 2014. A systematic review of physician leadership and emotional intelligence. Journal of Graduate Medical Education 6: 21–31. [Google Scholar] [CrossRef] [PubMed]
- Mishra, Parshant, and Upinder Dhar. 2001. Emotional intelligence as a correlate of thinking orientation among future managers. Indian Journal of Industrial Relations 36: 323–338. [Google Scholar]
- Mishar, Reziki, and Yuni Ros Bangun. 2014. Create the EQ modelling instrument based on Goleman and Bar-on models and psychological defense mechanisms. Procedia-Social and Behavioral Sciences 115: 394–406. [Google Scholar] [CrossRef]
- Mühlfeit, Jan, and Melina Costi. 2016. The Positive Leader: How Energy and Happiness Fuel Top-Performing Teams. London: Pearson. [Google Scholar]
- Nieto-Flores, María-Pilar, M. Pilar Berrios, and Natalio Extremera. 2019. Job Search Self-Efficacy as a Mediator between Emotional Intelligence and the Active Job Search Process/Autoeficacia de Búsqueda Como Mediadora de la Inteligencia Emocional y la Búsqueda Activa de Empleo. Revista de Psicología Social 34: 86–109. [Google Scholar] [CrossRef]
- Petrides, Konstantinos V. 2009. Psychometric properties of the Trait Emotional Intelligence questionnaire (TEIQue). In Assessing Emotional Intelligence. Theory, Research, and Applications. Edited by C. Stough, D. H. Saklofske and J. D. Parker. Boston: Springer, pp. 85–101. [Google Scholar]
- Petrides, Konstantinos V. 2010. Trait emotional intelligence theory. Industrial and Organizational Psychology 3: 136–39. [Google Scholar] [CrossRef]
- Petrides, Konstantinos V., and Adrian Furnham. 2001. Trait emotional intelligence: Psychometric investigation with reference to established trait taxonomies. European Journal of Personality 15: 425–48. [Google Scholar] [CrossRef]
- Piqueras, Jose A., Ornela Mateu-Martínez, Javuer Cejudo, and Juan Carlos Pérez-González. 2019. Pathways into psychosocial adjustment in children: Modeling the effects of trait emotional intelligence, social-emotional problems, and gender. Frontiers in Psychology 10: 507. [Google Scholar] [CrossRef]
- Pillay, Rubin. 2008. Managerial competencies of hospital managers in South Africa: A survey of managers in the public and private sectors. Human Resources for Health 6: 1–7. [Google Scholar] [CrossRef] [PubMed]
- Roth, Christine G., Karen W. Eldin, Vijayalakshmi Padmanabhan, and Ellen M. Friedman. 2019. Twelve tips for the introduction of emotional intelligence in medical education. Medical Teacher 41: 746–49. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, Saritha Alfrida, and Jyoti. S. Madgaonkar. 2013. Testing the developmental ability of leader’s emotional intelligence with age on ESCI. European Scientific Journal 9: 19. [Google Scholar]
- Sanchez-Gomez, Martin, Edgar Breso, and Gabriele Giorgi. 2021. Could emotional intelligence ability predict salary? A cross-sectional study in a multioccupational sample. International Journal of Environmental Research and Public Health 18: 1322. [Google Scholar] [CrossRef] [PubMed]
- Santana López, Borja N., Yeray G. Santana Padilla, M. Desampardos Bernat Adell, Jesús María González Martín, and Luciano Santana Cabrera. 2022. Feelings of the health personnel in Spain, towards their work, after five waves of the COVID-19 pandemic. Science Progress 105: 00368504221102798. [Google Scholar] [CrossRef]
- Sekaran, Uma, and Roger Bougie. 2016. Research Methods for Business: A Skill Building Approach. New York: John Wiley & Sons. [Google Scholar]
- Seymour, Nicole, Sandy Jansen, Lucy Feng, Stephanie Ayres, Zubin Austin, Jamie A. Seabrook, and Philip M. Jones. 2017. Impact of emotional intelligence coaching on job satisfaction of pharmacists during organizational changes. Journal of Hospital Administration 6: 39–45. [Google Scholar] [CrossRef]
- Sharp, Gary, Lorna Bourke, and Matthew J. Rickard. 2020. Review of emotional intelligence in health care: An introduction to emotional intelligence for surgeons. ANZ Journal of Surgery 90: 433–40. [Google Scholar] [CrossRef]
- Shih, Hsi-An, and Ely Susanto. 2010. Conflict management styles, emotional intelligence, and job performance in public organizations. International Journal of Conflict Management 21: 147–68. [Google Scholar] [CrossRef]
- Snell, Anita J., Don Briscoe, and Graham Dickson. 2011. From the inside out: The engagement of physicians as leaders in health care settings. Qualitative Health Research 21: 952–967. [Google Scholar] [CrossRef]
- Tannous, Adel, and Jehan Matar. 2010. The relationship between depression and emotional intelligence among a sample of Jordanian children. Procedia-Social and Behavioral Sciences 5: 1017–1022. [Google Scholar] [CrossRef][Green Version]
- Tyczkowski, Brenda, Christine Vandenhouten, Janet Reilly, Gsurav Bansal, Sylvia M. Kubsch, and Raelynn Jakkola. 2015. Emotional intelligence (EI) and nursing leadership styles among nurse managers. Nursing Administration Quarterly 39: 172–80. [Google Scholar] [CrossRef] [PubMed]
- Webb, Christian A., Sophie DelDonno, and William D. Killgore. 2014. The role of cognitive versus emotional intelligence in Iowa Gambling Task performance: What’s emotion got to do with it? Intelligence 44: 112–19. [Google Scholar] [CrossRef] [PubMed]
- Wolff, S. B. 2005. Hay Group, McClelland Center for Research and Innovation. The Emotional Competence Inventory (ECI) Technical Manual. Available online: http://www.eiconsortium.org/pdf/ECI_2_0_Technical_Manual_v2.pdf (accessed on 1 February 2018).


{kind=link}
| Items | Factor | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| SA-ESA3 | 0.875 | |||
| SA-ESA2 | 0.866 | |||
| SA-ESA1 | 0.852 | |||
| SA-ESA4 | 0.838 | |||
| SA-SC1 | 0.792 | |||
| SA-SC4 | 0.775 | |||
| SA-SC3 | 0.740 | |||
| SA-SC2 | 0.733 | |||
| SA-ASA3 | 0.854 | |||
| SA-ASA4 | 0.809 | |||
| SA-ASA1 | 0.663 | |||
| SA-ASA2 | 0.966 | |||
| Component | |||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| SM-T1 | 0.859 | ||||
| SM-T4 | 0.856 | ||||
| SM--O2 | 0.841 | ||||
| SM-T2 | 0.821 | ||||
| SM--O1 | 0.697 | ||||
| SM--O4 | 0.660 | ||||
| SM--O3 | 0.650 | ||||
| SM-Ad1 | 0.610 | ||||
| SM-T3 | 0.590 | ||||
| SM-Ad2 | 0.489 | ||||
| SM-I4 | 0.469 | ||||
| SM-Ad4 | 0.436 | ||||
| SM-Ac3 | 0.965 | ||||
| SM-Ac4 | 0.875 | ||||
| SM-Ac2 | 0.795 | ||||
| SM-Ac1 | 0.464 | ||||
| SM-Ad3 | 0.439 | ||||
| SM-ESC3 | 0.899 | ||||
| SM-ESC4 | 0.692 | ||||
| SM-ESC1 | 0.486 | ||||
| SM-I1 | 0.895 | ||||
| SM-ESC2 | 0.622 | ||||
| SM-I2 | 0.794 | ||||
| SM-I3 | 0.478 | ||||
| Component | |||
|---|---|---|---|
| 1 | 2 | 3 | |
| ScA-SO2 | 0.980 | ||
| ScA-SO1 | 0.904 | ||
| ScA-SO3 | 0.878 | ||
| ScA-SO4 | 0.782 | ||
| ScA-OA3 | 0.854 | ||
| ScA-E3 | 0.731 | ||
| ScA-E2 | 0.695 | ||
| ScA-E1 | 0.668 | ||
| ScA-E4 | 0.473 | ||
| ScA-OA2 | 0.943 | ||
| ScA-OA1 | 0.931 | ||
| ScA-OA4 | 0.608 | ||
| Component | ||||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| RM-DO2 | 1.009 | |||
| RM-DO4 | 0.954 | |||
| RM-DO3 | 0.933 | |||
| RM-IL4 | 0.748 | |||
| RM-IL3 | 0.735 | |||
| RM-DO1 | 0.735 | |||
| RM-CC1 | 0.696 | |||
| RM-CC3 | 0.683 | |||
| RM-IL1 | 0.671 | |||
| RM-IL2 | 0.610 | |||
| RM-I2 | 0.554 | |||
| RM-TC3 | 0.518 | |||
| RM-CC4 | 0.498 | |||
| RM-CM3 | 0.934 | |||
| RM-CM4 | 0.744 | |||
| RM-TC4 | 0.583 | |||
| RM-TC2 | 0.527 | |||
| RM-I1 | 0.427 | |||
| RM-I4 | 0.857 | |||
| RM-I3 | 0.686 | |||
| RM-CM1 | 0.647 | |||
| RM-CM2 | 0.539 | |||
| RM-CC2 | 0.853 | |||
| RM-TC1 | 0.564 | |||
| Study Contrast | Number of Items | Cronbachs’ Alpha Coefficient |
|---|---|---|
| Self-Awareness | 12 | 0.860 |
| Emotional Self-Awareness | 4 | 0.962 |
| Self-Confidence | 4 | 0.853 |
| Self-Assessment—Agreeableness | 3 | 0.989 |
| Self-Assessment—Defensiveness | 1 | 0.869 |
| Self-Management | 24 | 0.898 |
| Self-Management F 1 | 12 | 0.811 |
| Self-Management F 2 | 5 | 0.944 |
| Self-Management F 3 | 3 | 0.926 |
| Self-Management F 4 | 2 | 0.843 |
| Self-Management F 5 | 2 | 0.793 |
| Social Awareness | 12 | 0.944 |
| Service Orientation | 4 | 0.716 |
| Empathy | 5 | 0.887 |
| Organizational Awareness | 3 | 0.941 |
| Relationship Management | 24 | 0.888 |
| Relationship Management F 1 | 13 | 0.955 |
| Relationship Management F 2 | 5 | 0.876 |
| Relationship Management F 3 | 4 | 0.817 |
| Relationship Management F 4 | 2 | 0.834 |
| Overall Emotional Intelligence | 72 | 0.966 |
| Variable/Dimension | Private Mean | SD | Public Mean | SD | Leven’s Statistic F | Sig. |
|---|---|---|---|---|---|---|
| Self-Awareness | 3.756 | 0.409 | 3.847 | 0.495 | 2.056 | 0.052 |
| Self-Management | 3.482 | 0.414 | 3.550 | 0.349 | 2.942 | 0.087 |
| Social Awareness | 3.889 | 0.453 | 3.944 | 0.532 | 2.678 | 0.069 |
| Relationship Management | 3.417 | 0.411 | 3.590 | 0.383 | 0.068 | 0.795 |
| Emotional Intelligence | 3.636 | 0.342 | 3.733 | 0.349 | 0.379 | 0.539 |
| t | Sig. p-Value (2-Tailed) | df | Mean Difference * | ||
|---|---|---|---|---|---|
| Equal variances assumed | −2.576 | 0.010 | 356 | −0.097 | |
| Equal variances not assumed | −2.565 | 0.011 | 276.285 | −0.097 | |
| Self-Awareness | Equal variances assumed | −1.89 | 0.060 | 356 | −0.091 |
| Equal variances not assumed | −1.802 | 0.073 | 240.076 | −0.091 | |
| Self-Management | Equal variances assumed | −1.581 | 0.115 | 356 | −0.068 |
| Equal variances not assumed | −1.654 | 0.099 | 319.224 | −0.068 | |
| Social Awareness | Equal variances assumed | −1.043 | 0.298 | 356 | −0.055 |
| Equal variances not assumed | −1.002 | 0.317 | 245.664 | −0.055 | |
| Relationship Management | Equal variances assumed | −3.967 | 0.000 | 356 | −0.174 |
| Equal variances not assumed | −4.037 | 0.000 | 295.567 | −0.174 | |
| Variable/Dimension | Self/Mean | SD | Raters/Mean | SD | Leven’s Statistic F | Sig. |
|---|---|---|---|---|---|---|
| Self-Awareness | 3.814 | 0.387 | 3.697 | 0.424 | 0.022 | 0.883 |
| Self-Management | 3.570 | 0.411 | 3.394 | 0.406 | 0.710 | 0.400 |
| Social Awareness | 3.994 | 0.426 | 3.783 | 0.456 | 0.076 | 0.782 |
| Relationship Management | 3.458 | 0.385 | 3.376 | 0.433 | 0.500 | 0.480 |
| Emotional Intelligence | 3.709 | 0.356 | 3.562 | 0.367 | 1.841 | 0.176 |
| t | Sig. p-Value (2-Tailed) | df | Mean Difference | ||
|---|---|---|---|---|---|
| Emotional Intelligence | Equal variances assumed | 3.270 | 0.001 | 222 | 0.147 |
| Equal variances not assumed | 3.270 | 0.001 | 213.487 | 0.147 | |
| Self-Awareness | Equal variances assumed | 2.155 | 0.032 | 222 | 0.117 |
| Equal variances not assumed | 2.155 | 0.032 | 220.218 | 0.117 | |
| Self-Management | Equal variances assumed | 3.214 | 0.002 | 222 | 0.176 |
| Equal variances not assumed | 3.214 | 0.002 | 221.968 | 0.176 | |
| Social Awareness | Equal variances assumed | 3.592 | 0.000 | 222 | 0.212 |
| Equal variances not assumed | 3.592 | 0.000 | 220.99 | 0.212 | |
| Relationship Management | Equal variances assumed | 1.498 | 0.136 | 222 | 0.082 |
| Equal variances not assumed | 1.498 | 0.136 | 218.989 | 0.082 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sweis, R.J.; Aldaod, S.; Alsayyed, N.M.; Sukkari, L.S. Self vs. Other Raters’ Assessment of Emotional Intelligence in Private and Public Hospitals: A Comparative Study. Adm. Sci. 2022, 12, 194. https://doi.org/10.3390/admsci12040194
Sweis RJ, Aldaod S, Alsayyed NM, Sukkari LS. Self vs. Other Raters’ Assessment of Emotional Intelligence in Private and Public Hospitals: A Comparative Study. Administrative Sciences. 2022; 12(4):194. https://doi.org/10.3390/admsci12040194
Chicago/Turabian StyleSweis, Rateb Jalil, Sawsan Aldaod, Niveen Mazen Alsayyed, and Lilana Salem Sukkari. 2022. "Self vs. Other Raters’ Assessment of Emotional Intelligence in Private and Public Hospitals: A Comparative Study" Administrative Sciences 12, no. 4: 194. https://doi.org/10.3390/admsci12040194
APA StyleSweis, R. J., Aldaod, S., Alsayyed, N. M., & Sukkari, L. S. (2022). Self vs. Other Raters’ Assessment of Emotional Intelligence in Private and Public Hospitals: A Comparative Study. Administrative Sciences, 12(4), 194. https://doi.org/10.3390/admsci12040194