The Length of Residence is Associated with Cardiovascular Disease Risk Factors among Foreign-English Teachers in Korea

Abstract
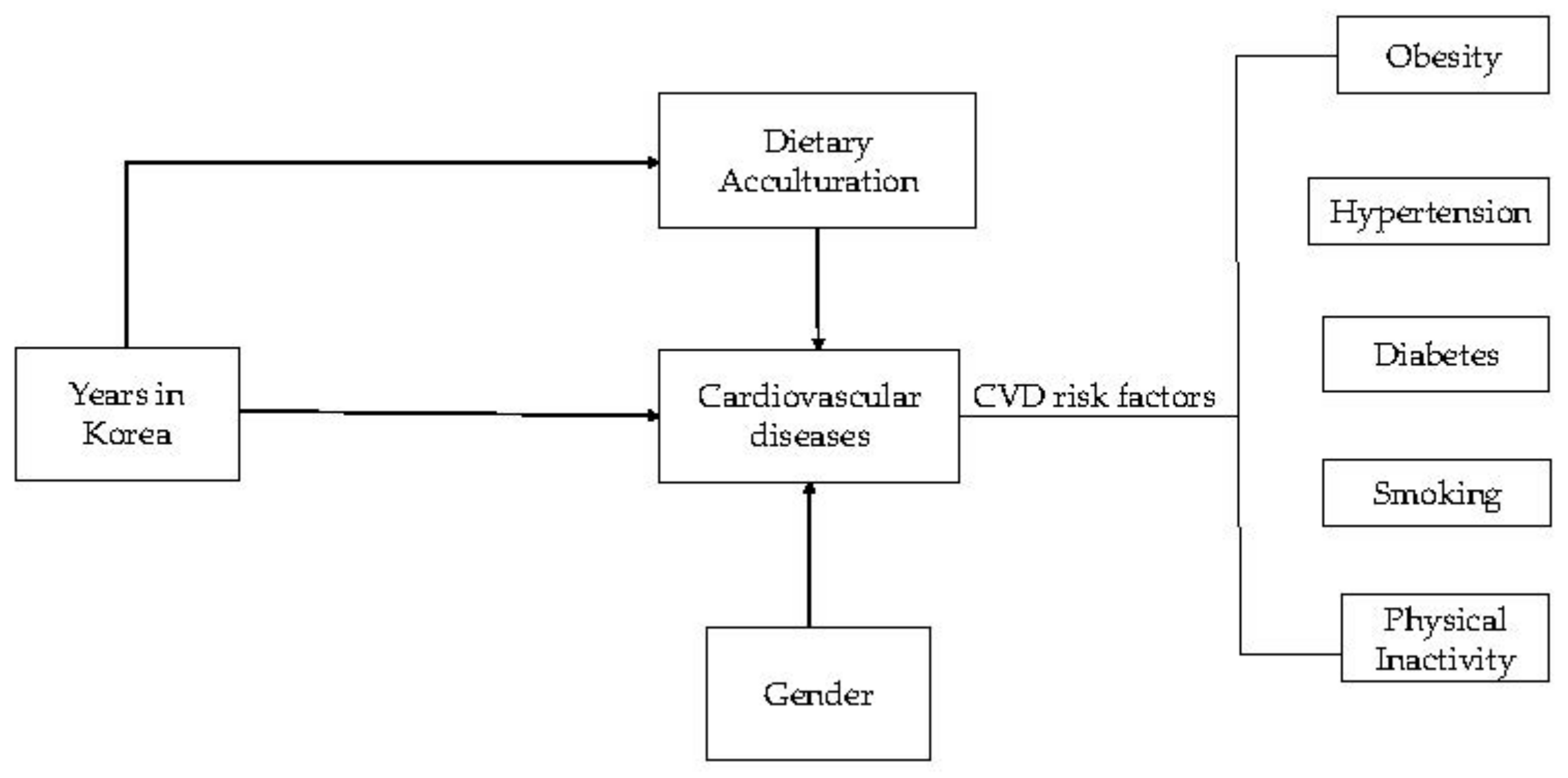
1. Introduction
2. Materials and Methods
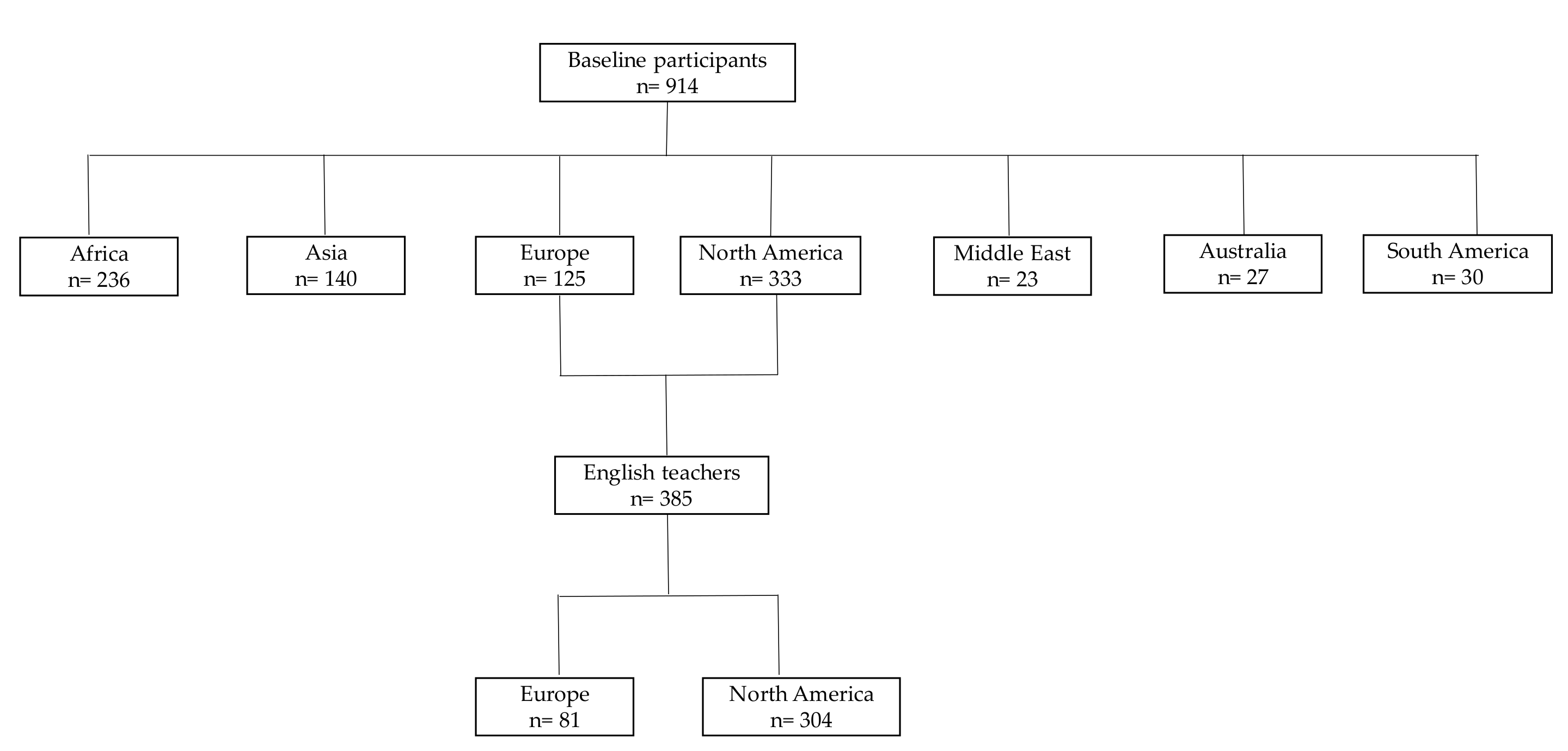
2.1. Study Population and Sample
2.1.1. Acculturation Variables
2.1.2. Cardiovascular Risk Factors
2.2. Human Subjects Research Approval
2.3. Statistical Analysis
3. Results
3.1. Univariate Analyses
3.2. Cardiovascular Risk Factors
3.2.1. Gender and CVD Risk Factors
3.2.2. Length of Residence and CVD Risk Factors
3.2.3. Length of Residence in Multivariate Analyses
4. Discussion
Limitations
5. Conclusions
Conflicts of Interest
References
- Jin, K.; Gullick, J.; Neubeck, L.; Koo, F.; Ding, D. Acculturation is associated with higher prevalence of cardiovascular disease risk-factors among Chinese immigrants in Australia: Evidence from a large population-based cohort. Eur. J. Prev. Cardiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Mendis, S.; Puska, P.; Norrving, B. Global Atlas on Cardiovascular Disease Prevention and Control; World Health Organization in Collaboration with the World Heart Federation and the World Stroke Organization: Geneva, Switzerland, 2011; pp. 3–18. [Google Scholar]
- Chiu, M.; Austin, P.C.; Manuel, D.G.; Tu, J.V. Cardiovascular Risk Factor Profiles of Recent Immigrants vs. Long-term Residents of Ontario: A Multi-ethnic Study. Can. J. Cardiol. 2012, 28, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Mooteri, S.N.; Petersen, F.; Dagubati, R.; Pai, R.G. Duration of residence in the United States as a new risk factor for coronary artery disease (The Konkani Heart Study). Am. J. Cardiol. 2004, 93, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Obiang-Obounou, B.W. Dietary Acculturation of Foreign Students in Daegu, Korea. J. Hum. Nutr. Food Sci. 2015, 3, 1068–1076. [Google Scholar]
- Koya, D.L.; Egede, L.E. Association between length of residence and cardiovascular disease risk factors among an ethnically diverse group of United States immigrants. J. Gen. Intern. Med. 2007, 22, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Commodore-Mensah, Y.; Ukonu, N.; Obisesan, O.; Aboagye, J.K.; Agyemang, C.; Reilly, C.M.; Dunbar, S.B.; Okosun, I.S. Length of Residence in the United States is Associated With a Higher Prevalence of Cardiometabolic Risk Factors in Immigrants: A Contemporary Analysis of the National Health Interview Survey. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Heo, J.; Park, S.H. The exploration of acculturation and health among immigrants from non-eastern cultures. Qual. Health Res. 2014, 24, 1138–1149. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.-J.; Kim, C.S.; Kim, T.W. Chinese Immigrants in Korea: The Relationship between Interpersonal Communication and Acculturation. Asian Pac. Migr. J. 2014, 23, 325–344. [Google Scholar] [CrossRef]
- Kim, S. Soft talk, hard realities: Multiculturalism as the south korean government’s decoupled response to international migration. Asian Pac. Migr. J. 2015, 24, 51–78. [Google Scholar] [CrossRef]
- Im, H.; Lee, K.Y.; Lee, H.Y. Acculturation stress and mental health among the marriage migrant women in busan, south korea. Community Ment Health J. 2014, 50, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Doo-Sub, L.S.K. Acculturation and self-rated health among foreign women in korea. Health Soc. Welfare Rev. 2014, 34, 453–483. [Google Scholar]
- Jun, H.-J.; Ha, S.-K. Social capital and assimilation of migrant workers and foreign wives in south korea: The case of wongok community. Habitat Int. 2015, 47, 126–135. [Google Scholar] [CrossRef]
- Kim, M.; Park, G.S.; Windsor, C. Marital power process of korean men married to foreign women: A qualitative study. Nur. Health Sci. 2013, 15, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.M. The Changing Role of English in Korea: From English as a Tool for Advancement to English for Surviva. Pan-Pac. Assoc. Appl. Linguist. 2005, 9, 227–240. [Google Scholar]
- Satia-Abouta, J. Dietary Acculturation: Definition, process, Assessment, and implication. Int. J. Hum. Ecol. 2003, 4, 71–86. [Google Scholar] [CrossRef]
- Okafor, M.T.; Carter-Pokras, O.D.; Picot, S.J.; Zhan, M. The relationship of language acculturation (English proficiency) to current self-rated health among African immigrant adults. J. Immigr. Minor. Health 2013, 15, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Satia, J.A.; Patterson, R.E.; Kristal, A.R.; Hislop, T.G.; Yasui, Y.; Taylor, V.M. Development of scales to measure dietary acculturation among Chinese-Americans and Chinese-Canadians. J. Am. Diet. Assoc. 2001, 101, 548–553. [Google Scholar] [CrossRef]
- Rodriguez, F.; Hicks, L.S.; Lopez, L. Association of acculturation and country of origin with self-reported hypertension and diabetes in a heterogeneous Hispanic population. BMC Public Health 2012, 12, 768. [Google Scholar] [CrossRef] [PubMed]
- WHO Expert Committee on Physical Status. The Use and Interpretation of Anthropometry. In Physical Status: The Use and Interpretation of Anthropometry: Report of a WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1995; p. x. 452p. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000; p. xii. 253p. [Google Scholar]
- Nguyen, H.H.; Smith, C.; Reynolds, G.L.; Freshman, B. The effect of acculturation on obesity among foreign-born Asians residing in the United States. J. Immigr. Minor. Health 2015, 17, 389–399. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines Approved by the Guidelines Review Committee. In Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Koolhaas, C.M.; Dhana, K.; Schoufour, J.D.; Ikram, M.A.; Kavousi, M.; Franco, O.H. Impact of physical activity on the association of overweight and obesity with cardiovascular disease: The Rotterdam Study. Eur. J. Prev. Cardiol. 2017, 24, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Lakka, T.A.; Bouchard, C. Physical activity, obesity and cardiovascular diseases. In Handbook of Experimental Pharmacology; Springer: Berlin, Germany, 2005; pp. 137–163. [Google Scholar]
- Mosca, L.; Barrett-Connor, E.; Kass Wenger, N. Sex/Gender Differences in Cardiovascular Disease Prevention. What a Difference a Decade Makes. Circulation 2011, 124, 2145–2154. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.E.; Daugherty, S.L. Gender disparities in cardiovascular disease prevention. Heart 2017. [Google Scholar] [CrossRef] [PubMed]
- Hertz, R.P.; Unger, A.N.; Cornell, J.A.; Saunders, E. Racial disparities in hypertension prevalence, awareness and management. Arch. Intern. Med. 2005, 165, 2098–2104. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.M.; Kim, H.C.; Kang, D.R. Sex differences in hypertension prevalence and control: Analysis of the 2010–2014 Korea National Health and Nutrition Examination Survey. PLoS ONE 2017, 12, e0178334. [Google Scholar] [CrossRef] [PubMed]
- Everett, B.; Zajacova, A. Gender Differences in Hypertension and Hypertension Awareness Among Young Adults. Biodemogr. Soc. Biol. 2015, 61, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, K.; Ji, H. Sex differences in primary hypertension. Biol. Sex Differ. 2012, 3, 7. [Google Scholar] [CrossRef] [PubMed]
- Hu, G.; Barengo, N.C.; Tuomilehto, J.; Lakka, T.A.; Nissinen, A.; Jousilahti, P. Relationship of physical activity and body mass index to the risk of hypertension: A prospective study in Finland. Hypertension 2004, 43, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Niskanen, L.; Laaksonen, D.E.; Nyyssonen, K.; Punnonen, K.; Valkonen, V.P.; Fuentes, R.; Tuomainen, T.P.; Salonen, R.; Salonen, J.T. Inflammation, abdominal obesity and smoking as predictors of hypertension. Hypertension 2004, 44, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Siahpush, M. Ethnic-immigrant differentials in health behaviors, morbidity and cause-specific mortality in the United States: An analysis of two national data bases. Hum. Biol. 2002, 74, 83–109. [Google Scholar] [CrossRef] [PubMed]
- Gadd, M.; Sundquist, J.; Johansson, S.E.; Wandell, P. Do immigrants have an increased prevalence of unhealthy behaviours and risk factors for coronary heart disease? Eur. J. Cardiovasc. Prev. Rehabil. 2005, 12, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Agyemang, C.; Owusu-Dabo, E.; de Jonge, A.; Martins, D.; Ogedegbe, G.; Stronks, K. Overweight and obesity among Ghanaian residents in The Netherlands: How do they weigh against their urban and rural counterparts in Ghana? Public Health Nutr. 2009, 12, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Delavari, M.; Sønderlund, A.L.; Swinburn, B.; Mellor, D.; Renzaho, A. Acculturation and obesity among migrant populations in high income countries—A systematic review. BMC Public Health 2013, 13, 458. [Google Scholar] [CrossRef] [PubMed]
- Steyn, N.P.; McHiza, Z.J. Obesity and the nutrition transition in Sub-Saharan Africa. Ann. N. Y. Acad. Sci. 2014, 1311, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Moon, S.; Popkin, B.M. The nutrition transition in South Korea. Am. J. Clin. Nutr. 2000, 71, 44–53. [Google Scholar] [PubMed]
- Lee, M.J.; Popkin, B.M.; Kim, S. The unique aspects of the nutrition transition in South Korea: The retention of healthful elements in their traditional diet. Public Health Nutr. 2002, 5, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Klitzke, C.J.; Anderson, L.; Walker, S.; Sikorsksi, R.; Moersfelder, B.; Richardson, A. Evidence of the Nutrition Transition in South Korea. J. Am. Diet. Assoc. 2009, 109 (Suppl. S9), A92. [Google Scholar] [CrossRef]
- Obiang-Obounou, B.W.; Mpelega, L.L. A critical review of the occurrence of depression among married Asian female immigrants in South Korea. Afr. J. Gend. Women Stud. 2017, 2, 101–110. [Google Scholar]



{kind=link}
{kind=link}
| Total (n = 385) | Europe (n = 81) | North America (n = 304) | |
|---|---|---|---|
| Age at interview (years) | |||
| Mean (SD) | 33.23 (8.50%) 1 | 33.33 (8.36%) | 33.20 (8.55%) |
| Range | 20–68 | 22–63 | 20–68 |
| Gender | |||
| Female | 216 (56.0%) | 31 (38.3%) | 185 (60.7%) |
| Male | 170 (44.0%) | 50 (61.7%) | 120 (39.3%) |
| Education | |||
| High School | 8 (2.1%) | 3 (3.7%) | 5 (1.6%) |
| Undergraduate | 196 (50.8%) | 36 (44.4%) | 160 (52.5%) |
| Post-graduate | 182 (47.2%) | 42 (51.9%) | 140 (45.9%) |
| Marital status | |||
| Single | 219 (56.7%) | 40 (49.4%) | 179 (58.7%) |
| Married | 167 (43.3%) | 41 (50.6%) | 126 (41.3%) |
| CVD Risk Factors | Total | Female | Male | p Value |
|---|---|---|---|---|
| Hypertension | ||||
| Yes | 46 (11.9%) 1 | 16 (7.4%) | 30 (17.6%) | 0.002 |
| Diabetes | ||||
| Yes | 3 (0.8%) | 1 (0.5%) | 2 (1.2%) | 0.433 |
| Smoking | ||||
| Yes | 43 (11.1%) | 15 (6.9%) | 28 (16.5%) | 0.003 |
| Body Mass Index (kg/m2) | ||||
| Underweight | 5 (1.3%) | 4 (1.9%) | 1 (0.6%) | |
| Normal | 198 (51.3%) | 122(56.5%) | 76 (44.7%) | 0.003 |
| Overweight/obese | 183 (47.4%) | 90 (41.7%) | 93 (47.4%) | |
| Physical Inactive | ||||
| Yes | 235 (63.3%) | 147 (70.3%) | 88 (54.3%) | 0.001 |
| Typical Korean diet | ||||
| Yes | 328 (96.5%) | 187 (95.9%) | 141 (97.2%) | 0.574 |
| Duration of Residence in Korea | |||||
|---|---|---|---|---|---|
| CVD risk factors | Total | <1 year | 1 to 4 years | Over 5 years | p value |
| Hypertension | |||||
| Yes | 46 (11.9%) | 6 (9.8%) | 13 (8.0%) | 27 (16.7%) | 0.046 |
| Diabetes | |||||
| Yes | 3 (0.8%) | 0 (0.0%) | 1 (0.6%) | 2 (1.2%) | 0.621 |
| Smoking | |||||
| Yes | 43 (11.1%) | 5 (8.2%) | 15 (9.2%) | 23 (14.2%) | 0.262 |
| Body Mass Index (kg/m2) | |||||
| Underweight | 5 (1.3%) | 3 (4.9%) | 1 (0.6%) | 1 (0.6%) | 0.028 |
| Normal | 198 (51.3%) | 34 (55.7%) | 89 (54.6%) | 75 (46.3%) | |
| Overweight/obese | 183 (47.4%) | 24 (39.3%) | 73 (44.8%) | 86 (53.1%) | |
| Physical Inactive | |||||
| Yes | 235 (63.3%) | 39 (63.9%) | 112 (72.3%) | 84 (54.2%) | 0.046 |
| Typical Korean diet | |||||
| Yes | 328 (96.5%) | 48 (94.1%) | 137 (96.5%) | 143 (97.3%) | 0.571 |
| CVD Risk-Factors | Length of Residence | Adjusted OR (95%CI) | p Value |
|---|---|---|---|
| Hypertension | <5 years | Ref | |
| Over 5 years | 2.16 (1.18–3.96) | 0.011 * | |
| Diabetes | <5 years | Ref | |
| Over 5 years | 4.33 (0.45–41.80) | 0.168 | |
| Smoking | <5 years | Ref | |
| Over 5 years | 1.51 (0.95–2.41) | 0.080 ** | |
| Overweight/Obesity | <5 years | Ref | |
| Over 5 years | 1.49 (1.11–2.01) | 0.009 *** | |
| Physical Inactivity | <5 years | Ref | |
| Over 5 years | 0.54 (0.40–0.74) | 0.000 *** | |
| Korean typical diet | <5 years | Ref | |
| Over 5 years | 1.47 (0.59–3.69) | 0.410 |
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obiang-Obounou, B.W. The Length of Residence is Associated with Cardiovascular Disease Risk Factors among Foreign-English Teachers in Korea. Behav. Sci. 2018, 8, 2. https://doi.org/10.3390/bs8010002
Obiang-Obounou BW. The Length of Residence is Associated with Cardiovascular Disease Risk Factors among Foreign-English Teachers in Korea. Behavioral Sciences. 2018; 8(1):2. https://doi.org/10.3390/bs8010002
Chicago/Turabian StyleObiang-Obounou, Brice Wilfried. 2018. "The Length of Residence is Associated with Cardiovascular Disease Risk Factors among Foreign-English Teachers in Korea" Behavioral Sciences 8, no. 1: 2. https://doi.org/10.3390/bs8010002
APA StyleObiang-Obounou, B. W. (2018). The Length of Residence is Associated with Cardiovascular Disease Risk Factors among Foreign-English Teachers in Korea. Behavioral Sciences, 8(1), 2. https://doi.org/10.3390/bs8010002