The Role of Regular Eating and Self-Monitoring in the Treatment of Bulimia Nervosa: A Pilot Study of an Online Guided Self-Help CBT Program

Abstract
:1. Introduction
1.1. Treatment Delivery Formats to Increase Access
1.1.1. Guided Self-Help
1.1.2. Online Self-Help
1.2. Behavioural Components of CBT
1.2.1. Self-Monitoring
1.2.2. Regular Eating: The Three-Hour Rule
2. Materials and Methods
2.1. Participants
2.2. Materials
2.2.1. Binge Eating eTherapy Program (BEeT)
2.2.2. SMS Reminders
2.3. Psychometric Measures
2.3.1. Eating Disorder Examination Questionnaire (EDE-Q)
2.3.2. Kessler Psychological Distress Scale (K10)
2.3.3. Eating Disorder Quality of Life Questionnaire (EDQOL)
2.3.4. Three-Factor Eating Questionnaire (TFEQ)
2.3.5. General Information and Demographics
2.3.6. General Mental Health
2.3.7. Self-Harm and Suicidality Risk Assessment
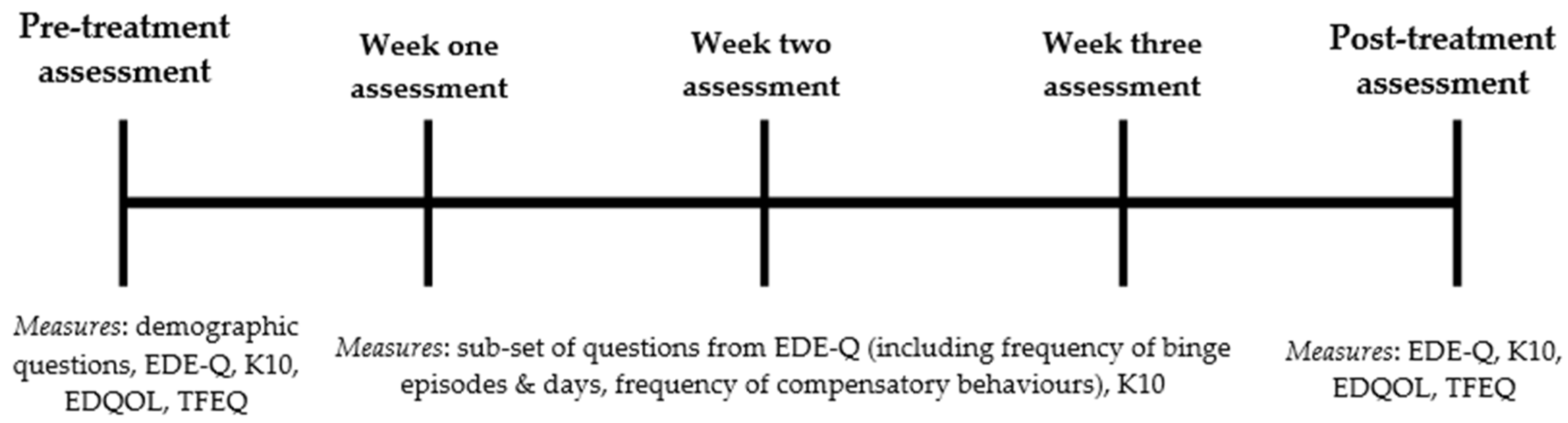
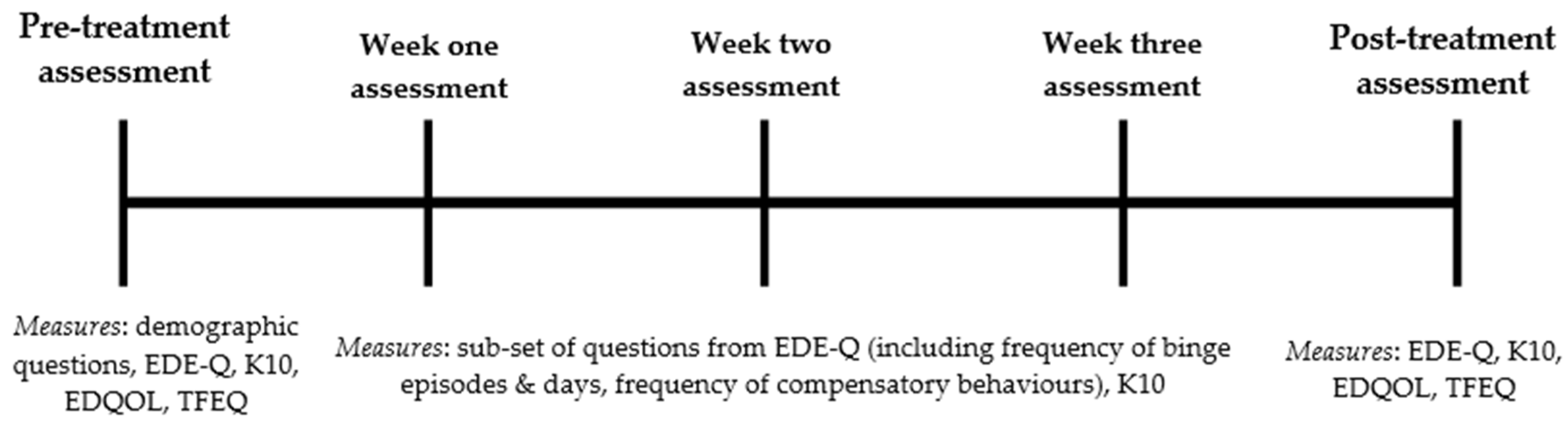
2.4. Procedure
2.5. Statistical Analysis
3. Results
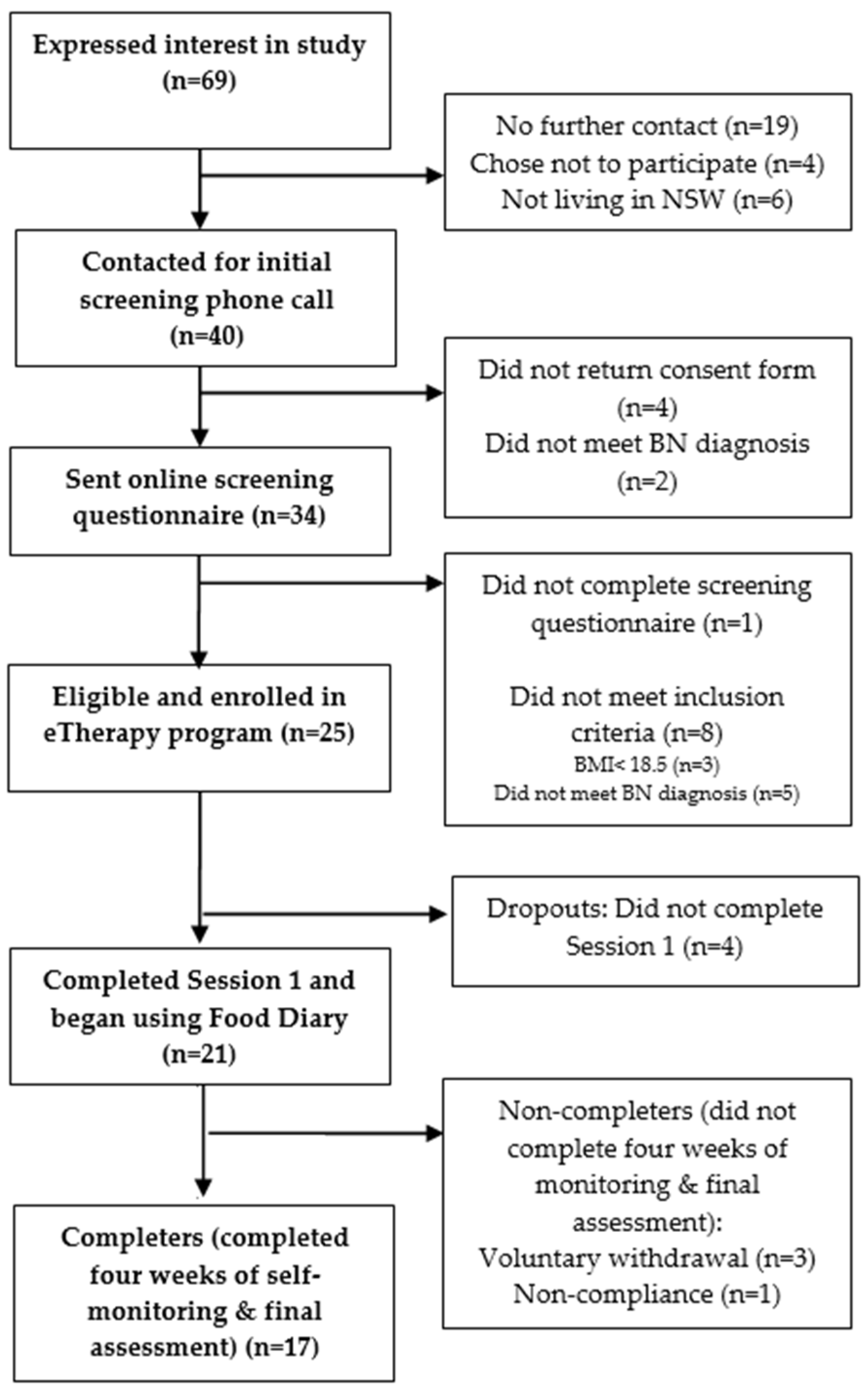
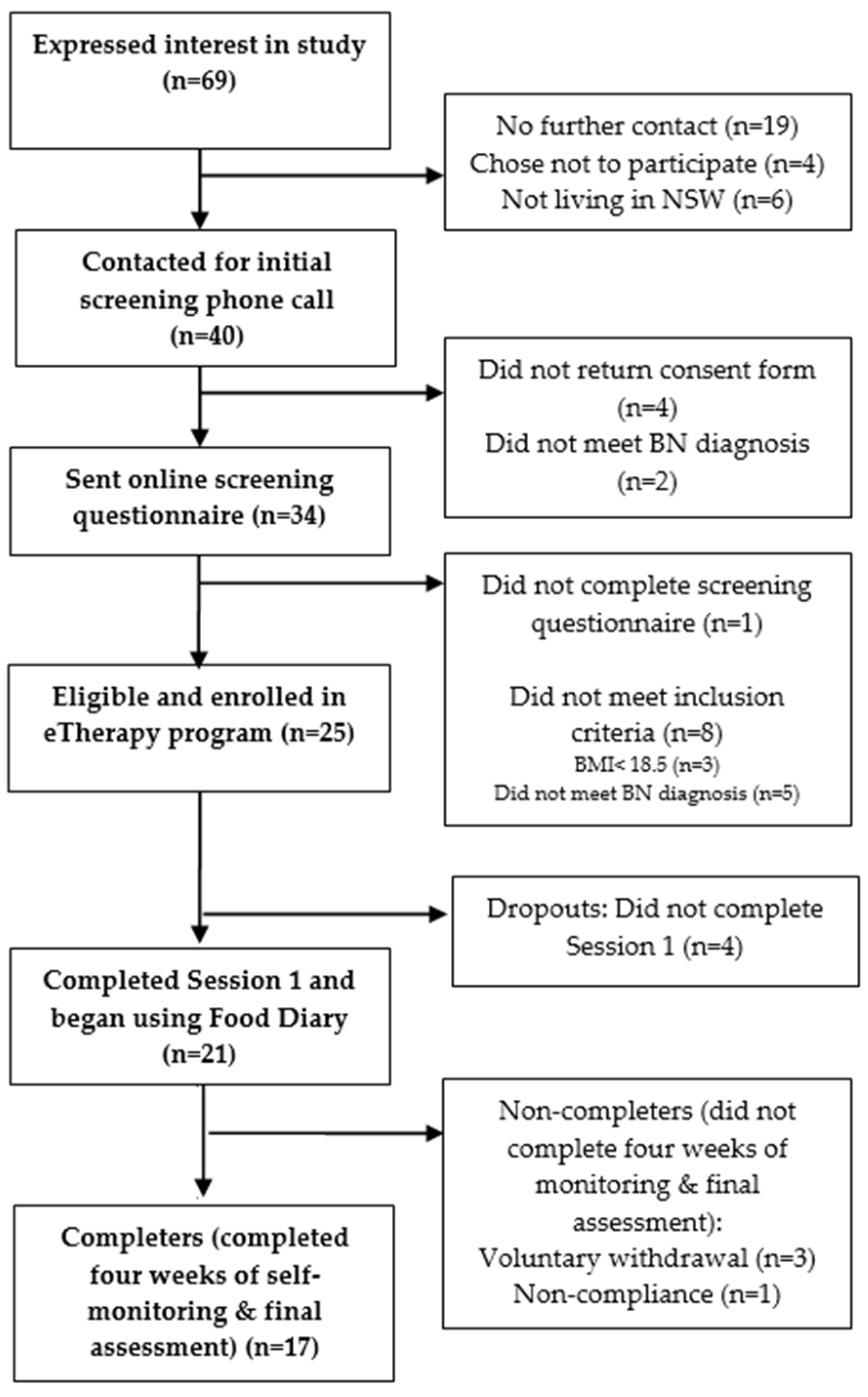
3.1. Participant Characteristics
3.2. Attrition and Compliance
3.3. Treatment Outcomes
3.4. Predictors of Outcome and Dropout
4. Discussion
4.1. Attrition and Compliance
4.2. Treatment Outcomes
4.3. Predictors of Treatment Compliance and Outcome
4.4. Strengths, Limitations and Future Research
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hay, P.; Chinn, D.; Forbes, D.; Madden, S.; Newton, R.; Sugenor, L.; Touyz, S.; Ward, W. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders. Aust. N. Z. J. Psychiatry 2014, 48, 977–1008. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Mental Health. Eating Disorders: Core Interventions in the Treatment and Management of Anorexia Nervosa, Bulimia Nervosa and Related Eating Disorders; NICE guideline (CG9); British Psychological Society: Leicester, UK; Royal College of Psychiatrists: London, UK, 2004. [Google Scholar]
- Hart, L.M.; Granillo, M.T.; Jorm, A.F.; Paxton, S.J. Unmet need for treatment in the eating disorders: A systematic review of eating disorder specific treatment seeking among community cases. Clin. Psychol. Rev. 2011, 31, 727–735. [Google Scholar] [CrossRef] [PubMed]
- National Eating Disorders Collaboration (NEDC). Eating Disorders Prevention, Treatment and Management: An Evidence Review; Commissioned by the Commonwealth Department of Health and Aging; National Eating Disorders Collaboration: Canberra, Australia, 2010. [Google Scholar]
- Tobin, D.L.; Banker, J.D.; Weisberg, L.; Bowers, W. I know what you did last summer (and it was not CBT): A factor analytic model of international psychotherapeutic practice in the eating disorders. Int. J. Eat. Disord. 2007, 40, 754–757. [Google Scholar] [CrossRef] [PubMed]
- Waller, G. Evidence-based treatment and therapist drift. Behav. Res. Ther. 2009, 47, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Stuhldreher, N.; Konnopka, A.; Wild, B.; Herzog, W.; Zipfel, S.; Löwe, B.; König, H.H. Cost-of-illness studies and cost-effectiveness analyses in eating disorders: A systematic review. Int. J. Eat. Disord. 2012, 45, 476–491. [Google Scholar] [CrossRef] [PubMed]
- Williams, C. New technologies in self-help: Another effective way to get better? Eur. Eat. Disord. Rev. 2003, 11, 170–182. [Google Scholar] [CrossRef]
- Latner, J.D.; Wilson, G.T. Self-monitoring and the assessment of binge eating. Behav. Ther. 2002, 33, 465–477. [Google Scholar] [CrossRef]
- Hay, P.; Bacaltchuk, J.; Stefano, S. Psychotherapy for bulimia nervosa and binging. Cochrane Database Syst. Rev. 2004, 1, 1–73. [Google Scholar]
- Fairburn, C.G. Overcoming Binge Eating, 1st ed.; Guilford Press: New York, NY, USA, 1995. [Google Scholar]
- Palmer, R.L.; Birchall, H.; McGrain, L.; Sullivan, V. Self-help for bulimic disorders: A randomised controlled trial comparing minimal guidance with face-to-face or telephone guidance. Br. J. Psychiatry 2002, 181, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Thiels, C.; Schmidt, U.; Troop, N.; Treasure, J.; Garthe, R. Binge frequency predicts outcome in guided self-care treatment of bulimia nervosa. Eur. Eat. Disord. Rev. 2000, 8, 272–278. [Google Scholar] [CrossRef]
- Treasure, J.; Schmidt, U.; Troop, N.; Tiller, J.; Todd, G.; Turnbull, S. Sequential treatment for bulimia nervosa incorporating a self-care manual. Br. J. Psychiatry 1996, 168, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Agras, W.S.; Crow, S.J.; Halmi, K.A.; Mitchell, J.E.; Wilson, G.T.; Kraemer, H.C. Outcome predictors for the cognitive behavior treatment of bulimia nervosa: Data from a multisite study. Am. J. Psychiatry 2000, 157, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Carrard, I.; Rouget, P.; Fernández-Aranda, F.; Volkart, A.C.; Damoiseau, M.; Lam, T. Evaluation and deployment of evidence based patient self-management support program for bulimia nervosa. Int. J. Med. Inform. 2006, 75, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Aranda, F.; Núñez, A.; Martínez, C.; Krug, I.; Cappozzo, M.; Carrard, I.; Rouget, P.; Jiménez-Murcia, S.; Granero, R.; Penelo, E.; et al. Internet-based cognitive-behavioral therapy for bulimia nervosa: A controlled study. Cyberpsychol. Behav. 2009, 12, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.E.; Crosby, R.D.; Wonderlich, S.A.; Crow, S.; Lancaster, K.; Simonich, H.; Swan-Kremeier, L.; Lysne, C.; Myers, T.C. A randomized trial comparing the efficacy of cognitive–behavioral therapy for bulimia nervosa delivered via telemedicine versus face-to-face. Behav. Res. Ther. 2008, 46, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, N.; Arcelus, J.; Beecham, J.; Dawson, H.; Doherty, F.; Eisler, I.; Gallagher, C.; Gowers, S.; Isaacs, G.; Johnson-Sabine, E.; et al. Cognitive-behavioural therapy for adolescents with bulimic symptomatology: The acceptability and effectiveness of internet-based delivery. Behav. Res. Ther. 2009, 47, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Ruwaard, J.; Lange, A.; Broeksteeg, J.; Renteria-Agirre, A.; Schrieken, B.; Dolan, C.V.; Emmelkamp, P. Online cognitive–behavioural treatment of bulimic symptoms: A randomized controlled trial. Clin. Psychol. Psychother. 2013, 20, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Ortiz, V.C.; Munro, C.; Stahl, D.; House, J.; Startup, H.; Treasure, J.; Williams, C.; Schmidt, U. A randomized controlled trial of internet-based cognitive-behavioural therapy for bulimia nervosa or related disorders in a student population. Psychol. Med. 2011, 41, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Ljotsson, B.; Lundin, C.; Mitsell, K.; Carlbring, P.; Ramklint, M.; Ghaderi, A. Remote treatment of bulimia nervosa and binge eating disorder: A randomized trial of Internet-assisted cognitive behavioural therapy. Behav. Res. Ther. 2007, 45, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Robinson, P.H.; Serfaty, M.A. The use of e-mail in the identification of bulimia nervosa and its treatment. Eur. Eat. Disord. Rev. 2001, 9, 182–193. [Google Scholar] [CrossRef]
- Bauer, S.; Okon, E.; Meermann, R.; Kordy, H. Technology-enhanced maintenance of treatment gains in eating disorders: Efficacy of an intervention delivered via text messaging. J. Consult. Clin. Psychol. 2012, 80, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, U.; Andiappan, M.; Grover, M.; Robinson, S.; Perkins, S.; Dugmore, O.; Treasure, J.; Landau, S.; Eisler, I.; Williams, C. Randomised controlled trial of CD–ROM-based cognitive–behavioural self-care for bulimia nervosa. Br. J. Psychiatry 2008, 193, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Cooper, Z. The Eating Disorder Examination (12th ed.). In Binge Eating: Nature, Assessment and Treatment; Fairburn, C.G., Wilson, G.T., Eds.; Guilford Press: New York, NY, USA, 1993; pp. 317–360. [Google Scholar]
- Walsh, S.; Golden, E.; Priebe, S. Systematic review of patients’ participation in and experiences of technology-based monitoring of mental health symptoms in the community. Br. Med. J. Open 2016, 6, e008362. [Google Scholar] [CrossRef] [PubMed]
- Tregarthen, J.P.; Lock, J.; Darcy, A.M. Development of a smartphone application for eating disorder self-monitoring. Int. J. Eat. Disord. 2015, 48, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Geller, J.; Srikameswaran, S. What effective therapies have in common. Adv. Eat. Disord. Theor. Res. Pract. 2015, 3, 191–197. [Google Scholar] [CrossRef]
- Longmore, R.J.; Worrell, M. Do we need to challenge thoughts in cognitive behavior therapy? Clin. Psychol. Rev. 2007, 27, 173–187. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Jones, R.; Peveler, R.C.; Carr, S.J.; Solomon, R.A.; O’Connor, M.E.; Burton, J.; Hope, R.A. Three psychological treatments for bulimia nervosa: A comparative trial. Arch. Gen. Psychiatry 1991, 48, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Korotitsch, W.J.; Nelson-Gray, R.O. An overview of self-monitoring research in assessment and treatment. Psychol. Assess. 1999, 11, 415–425. [Google Scholar] [CrossRef]
- Wilson, G.T.; Vitousek, K.M. Self-monitoring in the assessment of eating disorders. Psychol. Assess. 1999, 11, 480–489. [Google Scholar] [CrossRef]
- Hildebrandt, T.; Latner, J. Effect of self-monitoring on binge eating: Treatment response or ‘binge drift’? Eur. Eat. Disord. Rev. 2006, 14, 17–22. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Agras, W.S.; Walsh, B.T.; Wilson, G.T.; Stice, E. Prediction of outcome in bulimia nervosa by early change in treatment. Am. J. Psychiatry 2004, 161, 2322–2324. [Google Scholar] [CrossRef] [PubMed]
- Le Grange, D.; Doyle, P.; Crosby, R.D.; Chen, E. Early response to treatment in adolescent bulimia nervosa. Int. J. Eat. Disord. 2008, 41, 755–757. [Google Scholar] [CrossRef] [PubMed]
- Raykos, B.C.; Watson, H.J.; Fursland, A.; Byrne, S.M.; Nathan, P. Prognostic value of rapid response to enhanced cognitive behavioral therapy in a routine clinic sample of eating disorder outpatients. Int. J. Eat. Disord. 2013, 46, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Thompson-Brenner, H.; Shingleton, R.M.; Sauer-Zavala, S.; Richards, L.K.; Pratt, E.M. Multiple measures of rapid response as predictors of remission in cognitive behavior therapy for bulimia nervosa. Behav. Res. Ther. 2015, 64, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Vall, E.; Wade, T.D. Predictors of treatment outcome in individuals with eating disorders: A systematic review and meta-analysis. Int. J. Eat. Disord. 2015, 48, 946–971. [Google Scholar] [CrossRef] [PubMed]
- Cash, T.F.; Hrabosky, J.I. The effects of psychoeducation and self-monitoring in a cognitive-behavioral program for body-image improvement. Eat. Disord. 2003, 11, 255–270. [Google Scholar] [CrossRef] [PubMed]
- Nichols, S.; Gusella, J. Food for thought: Will adolescent girls with eating disorders self-monitor in a CBT group. Can. Child Psychiatry Rev. 2003, 12, 37–39. [Google Scholar]
- Fairburn, C.G. Cognitive Behavior Therapy and Eating Disorders; Guilford Press: New York, NY, USA, 2008. [Google Scholar]
- Cooper, M.; Todd, G.; Wells, A. Treating Bulimia Nervosa and Binge Eating: An Integrated Metacognitive and Cognitive Therapy Manual; Routledge, Taylor & Francis Group: London, UK, 2009. [Google Scholar]
- Zendegui, E.A.; West, J.A.; Zandberg, L.J. Binge eating frequency and regular eating adherence: The role of eating pattern in cognitive behavioral guided self-help. Eat. Behav. 2014, 15, 241–243. [Google Scholar] [CrossRef] [PubMed]
- Telch, C.F.; Agras, S.W. The effects of short-term food deprivation on caloric intake in eating-disordered subjects. Appetite 1996, 26, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.; Passi, V.; Bryson, S.; Agras, W.S. Patterns of eating and abstinence in women treated for bulimia nervosa. Int. J. Eat. Disord. 2005, 38, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents: Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 68, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Hiripi, E.; Pope, H.G.; Kessler, R.C. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C.M.; Masheb, R.M.; Wilson, G.T. Subtyping binge eating disorder. J. Consult. Clin. Psychol. 2001, 69, 1066–1072. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C.M.; White, M.A.; Masheb, R.M. DSM-IV psychiatric disorder comorbidity and its correlates in binge eating disorder. Int. J. Eat. Disord. 2009, 42, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Bohon, C.; Marti, C.N.; Fischer, K. Subtyping women with bulimia nervosa along dietary and negative affect dimensions: Further evidence of reliability and validity. J. Consult. Clin. Psychol. 2008, 76, 1022–1033. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Fairburn, C.G.; Beglin, S.J. Eating Disorder Examination Questionnaire (6.0). In Cognitive Behavior Therapy and Eating Disorders; Fairburn, C.G., Ed.; Guildford Press: New York, NY, USA, 2008; pp. 309–315. [Google Scholar]
- Fairburn, C.G.; Marcus, M.D.; Wilson, G.T. Cognitive-Behavioral Therapy for Binge Eating and Bulimia Nervosa: A Comprehensive Treatment Manual. In Binge Eating: Nature, Assessment and Treatment; Fairburn, C.G., Wilson, G.T., Eds.; Guildford Press: New York, NY, USA, 1993; pp. 361–404. [Google Scholar]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behav. Res. Ther. 2003, 41, 509–528. [Google Scholar] [CrossRef]
- Luce, K.H.; Winzelberg, A.J.; Das, S.; Osborne, M.I.; Bryson, S.W.; Taylor, C.B. Reliability of self-report: Paper versus online administration. Comput. Hum. Behav. 2007, 23, 1384–1389. [Google Scholar] [CrossRef]
- Peterson, C.B.; Crosby, R.D.; Wonderlich, S.A.; Joiner, T.; Crow, S.J.; Mitchell, J.E.; Bardone-Cone, A.M.; Klein, M.; Le Grange, D. Psychometric properties of the eating disorder examination-questionnaire: Factor structure and internal consistency. Int. J. Eat. Disord. 2007, 40, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Engel, S.G.; Wittrock, D.A.; Crosby, R.D.; Wonderlich, S.A.; Mitchell, J.E.; Kolotkin, R.L. Development and psychometric validation of an eating disorder-specific health-related quality of life instrument. Int. J. Eat. Disord. 2006, 39, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Banasiak, S.J.; Paxton, S.J.; Hay, P. Guided self-help for bulimia nervosa in primary care: A randomized controlled trial. Psychol. Med. 2005, 35, 1283–1294. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.A.; Muller, S.L.; Reas, D.L.; Thaw, J.M. Cognitive bias in eating disorders: Implications for theory and treatment. Behav. Modif. 1999, 23, 556–577. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Coker, S.; Fleming, C. An evaluation of the efficacy of supervised cognitive behavioral self-help for bulimia nervosa. J. Psychosom. Res. 1996, 40, 281–287. [Google Scholar] [CrossRef]
- Perkins, S.S.; Murphy, R.R.; Schmidt, U.U.; Williams, C. Self-help and guided self-help for eating disorders. Cochrane Database Syst. Rev. 2006, 4, 1–3. [Google Scholar]
- Ilardi, S.S.; Craighead, W.E. The role of nonspecific factors in cognitive-behavior therapy for depression. Clin. Psychol. Sci. Pract. 1994, 1, 138–155. [Google Scholar] [CrossRef]
- Steel, Z.; Jones, J.; Adcock, S.; Clancy, R.; Bridgford-West, L.; Austin, J. Why the high rate of dropout from individualized cognitive-behavior therapy for bulimia nervosa? Int. J. Eat. Disord. 2000, 28, 209–214. [Google Scholar] [CrossRef]
- Chen, E.Y.; Le Grange, D. Subtyping adolescents with bulimia nervosa. Behav. Res. Ther. 2007, 45, 2813–2820. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Coker, S.; Fleming, C. Self-help for bulimia nervosa: A preliminary report. Int. J. Eat. Disord. 1994, 16, 401–404. [Google Scholar] [CrossRef]
- Steele, A.L.; Bergin, J.; Wade, T.D. Self-efficacy as a robust predictor of outcome in guided self-help treatment for broadly defined bulimia nervosa. Int. J. Eat. Disord. 2011, 44, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Hay, P.J.; Claudino, A.M. Bulimia nervosa: Online interventions. Br. Med. J. Clin. Evid. 2015, 3, 1–16. [Google Scholar]
- Nelson, R.O.; Boykin, R.A.; Hayes, S.C. Long-term effects of self-monitoring on reactivity and on accuracy. Behav. Res. Ther. 1982, 20, 357–363. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Participant Feature | Frequency (%) |
|---|---|
| Employed | 60 |
| Student | 24 |
| White/Caucasian | 84 |
| Asian | 12 |
| Metropolitan residence | 64 |
| Regional residence * | 24 |
| Rural residence | 12 |
| Comorbid anxiety | 32 |
| Comorbid depression | 40 |
| Comorbid substance/alcohol issues | 16 |
| Receiving concurrent treatment | 76 |
| Frequent alcohol consumption (4 or more times per week) | 36 |
| Past suicidality | 60 |
| Active suicidality (within previous 28 days) | 20 |
| Past self-harm | 48 |
| Active self-harm (within previous 28 days) | 12 |
| Outcome | Pre-Treatment Means (SD) | Post-Treatment Means (SD) | p Value | Test Statistic Wald χ2 (df = 1) |
|---|---|---|---|---|
| EDE-Q | ||||
| Objective binge frequency | 23.7 (16.63) | 14.9 (12.55) | p < 0.001 * | 21.62 |
| Objective binge days | 17.9 (6.17) | 10.8 (9.31) | p < 0.001 * | 12.99 |
| Loss of control frequency | 21.0 (12.01) | 14.1 (13.87) | p < 0.001 * | 12.47 |
| Subjective binge days (n = 16) | 9.7 (9.60) | 7.4 (6.26) | p = 0.401 | 0.70 |
| Purge frequency (n = 13) | 20.4 (20.45) | 14.4 (18.85) | p = 0.038 | 4.30 |
| Laxative use frequency (n = 7) | 11.9 (11.45) | 9.3 (10.61) | p = 0.071 | 3.25 |
| Excessive exercise frequency (n = 11) | 9.5 (10.58) | 6.5 (8.42) | p = 0.123 | 2.38 |
| Dietary restraint | 4.1 (1.14) | 2.9 (1.84) | p = 0.001 * | 10.75 |
| Eating concern | 4.1 (1.11) | 3.0 (1.41) | p = 0.001 * | 10.18 |
| Shape concern | 5.3 (0.72) | 4.5 (1.25) | p = 0.002 * | 9.92 |
| Weight concern | 5.0 (0.60) | 4.4 (1.48) | p = 0.076 | 3.14 |
| Global score | 4.6 (0.55) | 3.7 (1.31) | p < 0.001 * | 12.86 |
| Other Outcomes | ||||
| EDQOL global score | 1.9 (0.71) | 1.8 (0.865) | p = 0.564 | 0.33 |
| TFEQ global score | 34.5 (4.91) | 34.7 (4.61) | p = 0.888 | 0.02 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barakat, S.; Maguire, S.; Surgenor, L.; Donnelly, B.; Miceska, B.; Fromholtz, K.; Russell, J.; Hay, P.; Touyz, S. The Role of Regular Eating and Self-Monitoring in the Treatment of Bulimia Nervosa: A Pilot Study of an Online Guided Self-Help CBT Program. Behav. Sci. 2017, 7, 39. https://doi.org/10.3390/bs7030039
Barakat S, Maguire S, Surgenor L, Donnelly B, Miceska B, Fromholtz K, Russell J, Hay P, Touyz S. The Role of Regular Eating and Self-Monitoring in the Treatment of Bulimia Nervosa: A Pilot Study of an Online Guided Self-Help CBT Program. Behavioral Sciences. 2017; 7(3):39. https://doi.org/10.3390/bs7030039
Chicago/Turabian StyleBarakat, Sarah, Sarah Maguire, Lois Surgenor, Brooke Donnelly, Blagica Miceska, Kirsty Fromholtz, Janice Russell, Phillipa Hay, and Stephen Touyz. 2017. "The Role of Regular Eating and Self-Monitoring in the Treatment of Bulimia Nervosa: A Pilot Study of an Online Guided Self-Help CBT Program" Behavioral Sciences 7, no. 3: 39. https://doi.org/10.3390/bs7030039
APA StyleBarakat, S., Maguire, S., Surgenor, L., Donnelly, B., Miceska, B., Fromholtz, K., Russell, J., Hay, P., & Touyz, S. (2017). The Role of Regular Eating and Self-Monitoring in the Treatment of Bulimia Nervosa: A Pilot Study of an Online Guided Self-Help CBT Program. Behavioral Sciences, 7(3), 39. https://doi.org/10.3390/bs7030039