
Brief Repeated Attention Training for Psychological Distress: Findings from Two Experiments

 , ,
, ,
Abstract
1. Introduction
The Current Study
2. Materials and Methods
2.1. Sample
2.2. Measures
2.2.1. Psychological Distress
2.2.2. Mood Dysfunction
2.3. Experimental Task Description
2.4. Presence of Attentional Bias
2.5. Analysis Plan
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AT | Attention Training |
| DASS | Depression, Anxiety, and Stress Scale |
| IMS | Immediate Mood Scale |
| PST | Positive Search Training |
| VS | Visual Search |
Appendix A

{kind=link}
{kind=link}
| Control | T | df | p | SMD | ||
|---|---|---|---|---|---|---|
| T1 DASS Stress | T2 DASS Stress | −0.93 | 72 | 0.354 | −0.109 | [−0.339, 0.121] |
| T1 DASS Stress | T3 DASS Stress | 1.74 | 12 | 0.107 | 0.483 | [−0.102, 1.051] |
| T2 DASS Stress | T3 DASS Stress | 1.35 | 12 | 0.203 | 0.373 | [−0.197, 0.93] |
| T1 DASS Anxiety | T2 DASS Anxiety | 1.57 | 72 | 0.121 | 0.184 | [−0.048, 0.415] |
| T1 DASS Anxiety | T3 DASS Anxiety | −1.39 | 10 | 0.193 | −0.42 | [−1.029, 0.207] |
| T2 DASS Anxiety | T3 DASS Anxiety | −2.38 | 10 | 0.039 | −0.717 | [−1.37, −0.035] |
| T1 DASS Depression | T2 DASS Depression | 1.70 | 72 | 0.093 | 0.199 | [−0.033, 0.43] |
| T1 DASS Depression | T3 DASS Depression | 0.88 | 14 | 0.393 | 0.228 | [−0.289, 0.737] |
| T2 DASS Depression | T3 DASS Depression | 0.84 | 14 | 0.414 | 0.217 | [−0.299, 0.726] |
| T1 IMS Total | T2 IMS Total | −1.30 | 71 | 0.200 | −0.153 | [−0.384, 0.08] |
| T1 IMS Total | T3 IMS Total | −2.49 | 17 | 0.023 | −0.587 | [−1.081, −0.078] |
| T2 IMS Total | T3 IMS Total | −2.12 | 17 | 0.049 | −0.499 | [−0.983, −0.001] |
| T1 IMS Depression | T2 IMS Depression | −0.90 | 71 | 0.374 | −0.106 | [−0.337, 0.127] |
| T1 IMS Depression | T3 IMS Depression | −6.31 | 17 | <0.001 | −1.488 | [−2.155, −0.8] |
| T2 IMS Depression | T3 IMS Depression | −5.22 | 17 | <0.001 | −1.231 | [−1.839, −0.603] |
| T1 IMS Anxiety | T2 IMS Anxiety | −1.34 | 71 | 0.183 | −0.159 | [−0.39, 0.075] |
| T1 IMS Anxiety | T3 IMS Anxiety | −2.68 | 17 | 0.016 | −0.632 | [−1.132, −0.117] |
| T2 IMS Anxiety | T3 IMS Anxiety | −2.25 | 17 | 0.038 | −0.531 | [−1.02, −0.03] |
| Experimental | T | df | p | SMD | CI95% | |
| T1 DASS Stress | T2 DASS Stress | 0.70 | 78 | 0.486 | 0.079 | [−0.142, 0.299] |
| T1 DASS Stress | T3 DASS Stress | 1.41 | 23 | 0.171 | 0.288 | [−0.123, 0.694] |
| T2 DASS Stress | T3 DASS Stress | 1.17 | 22 | 0.253 | 0.245 | [−0.173, 0.657] |
| T1 DASS Anxiety | T2 DASS Anxiety | 3.10 | 78 | 0.003 | 0.348 | [0.12, 0.575] |
| T1 DASS Anxiety | T3 DASS Anxiety | −1.49 | 20 | 0.153 | −0.324 | [−0.76, 0.119] |
| T2 DASS Anxiety | T3 DASS Anxiety | −2.75 | 18 | 0.013 | −0.632 | [−1.119, −0.131] |
| T1 DASS Depression | T2 DASS Depression | 1.99 | 78 | 0.051 | 0.224 | [−0.001, 0.446] |
| T1 DASS Depression | T3 DASS Depression | 0.45 | 23 | 0.656 | 0.092 | [−0.31, 0.492] |
| T2 DASS Depression | T3 DASS Depression | 1.02 | 22 | 0.319 | 0.213 | [−0.203, 0.624] |
| T1 IMS Total | T2 IMS Total | −1.05 | 76 | 0.298 | −0.119 | [−0.343, 0.105] |
| T1 IMS Total | T3 IMS Total | −0.53 | 24 | 0.599 | −0.107 | [−0.499, 0.288] |
| T2 IMS Total | T3 IMS Total | 0.19 | 24 | 0.852 | 0.038 | [−0.355, 0.43] |
| T1 IMS Depression | T2 IMS Depression | −1.73 | 76 | 0.088 | −0.197 | [−0.422, 0.029] |
| T1 IMS Depression | T3 IMS Depression | −2.25 | 24 | 0.034 | −0.449 | [−0.857, −0.033] |
| T2 IMS Depression | T3 IMS Depression | −2.16 | 24 | 0.041 | −0.431 | [−0.837, −0.017] |
| T1 IMS Anxiety | T2 IMS Anxiety | −0.76 | 76 | 0.448 | −0.087 | [−0.31, 0.137] |
| T1 IMS Anxiety | T3 IMS Anxiety | −0.57 | 24 | 0.576 | −0.114 | [−0.506, 0.281] |
| T2 IMS Anxiety | T3 IMS Anxiety | −0.84 | 24 | 0.407 | −0.169 | [−0.562, 0.228] |
References
- Bar-Haim, Y., Lamy, D., Pergamin, L., Bakermans-Kranenburg, M. J., & Van Ijzendoorn, M. H. (2007). Threat-related attentional bias in anxious and nonanxious individuals: A meta-analytic study. Psychological Bulletin, 133(1), 1. [Google Scholar] [CrossRef] [PubMed]
- Basanovic, J., Kaiko, I., & MacLeod, C. (2021). Change in attentional control predicts change in attentional bias to negative information in response to elevated state anxiety. Cognitive Therapy and Research, 45(1), 111–122. [Google Scholar] [CrossRef]
- Bishop, S., Duncan, J., Brett, M., & Lawrence, A. D. (2004). Prefrontal cortical function and anxiety: Controlling attention to threat-related stimuli. Nature Neuroscience, 7(2), 184–188. [Google Scholar] [CrossRef]
- Bourke, C., Douglas, K., & Porter, R. (2010). Processing of facial emotion expression in major depression: A review. Australian & New Zealand Journal of Psychiatry, 44(8), 681–696. [Google Scholar] [CrossRef] [PubMed]
- Brosan, L., Hoppitt, L., Shelfer, L., Sillence, A., & Mackintosh, B. (2011). Cognitive bias modification for attention and interpretation reduces trait and state anxiety in anxious patients referred to an out-patient service: Results from a pilot study. Journal of Behavior Therapy and Experimental Psychiatry, 42(3), 258–264. [Google Scholar] [CrossRef]
- Burns, H., Hurst, A., Garay, P., Murray, N. E., Stewart, S. H., Mejia, J., Bagnell, A., Klein, R. M., & Meier, S. (2025). Attentional biases for dynamic stimuli in emerging adults with anxiety: A preliminary eye-tracking study. Journal of Psychiatric Research, 184, 262–271. [Google Scholar] [CrossRef]
- Corriveau, A., Chao, A. F., deBettencourt, M. T., & Rosenberg, M. D. (2024). Recognition memory fluctuates with sustained attention regardless of task relevance. Psychonomic Bulletin & Review, 32(2), 714–728. [Google Scholar] [CrossRef] [PubMed]
- Cristea, I. A., Kok, R. N., & Cuijpers, P. (2016). The effectiveness of cognitive bias modification interventions for substance addictions: A meta-analysis. PLoS ONE, 11(9), e0162226. [Google Scholar] [CrossRef]
- Dandeneau, S. D., Baldwin, M. W., Baccus, J. R., Sakellaropoulo, M., & Pruessner, J. C. (2007). Cutting stress off at the pass: Reducing vigilance and responsiveness to social threat by manipulating attention. Journal of Personality and Social Psychology, 93(4), 651–666. [Google Scholar] [CrossRef]
- Dennis-Tiwary, T. A., Roy, A. K., Denefrio, S., & Myruski, S. (2019). Heterogeneity of the anxiety-related attention bias: A review and working model for future research. Clinical Psychological Science, 7(5), 879–899. [Google Scholar] [CrossRef]
- De Voogd, E., Wiers, R. W., & Salemink, E. (2017). Online visual search attentional bias modification for adolescents with heightened anxiety and depressive symptoms: A randomized controlled trial. Behaviour Research and Therapy, 92, 57–67. [Google Scholar] [CrossRef]
- Dodd, H. F., Vogt, J., Turkileri, N., & Notebaert, L. (2017). Task relevance of emotional information affects anxiety-linked attention bias in visual search. Biological Psychology, 122, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Fodor, L. A., Georgescu, R., Cuijpers, P., Szamoskozi, Ş., David, D., Furukawa, T. A., & Cristea, I. A. (2020). Efficacy of cognitive bias modification interventions in anxiety and depressive disorders: A systematic review and network meta-analysis. The Lancet Psychiatry, 7(6), 506–514. [Google Scholar] [CrossRef]
- Hakamata, Y., Lissek, S., Bar-Haim, Y., Britton, J. C., Fox, N. A., Leibenluft, E., Ernst, M., & Pine, D. S. (2010). Attention bias modification treatment: A meta-analysis toward the establishment of novel treatment for anxiety. Biological Psychiatry, 68(11), 982–990. [Google Scholar] [CrossRef]
- Juth, P., Lundqvist, D., Karlsson, A., & Öhman, A. (2005). Looking for foes and friends: Perceptual and emotional factors when finding a face in the crowd. Emotion, 5(4), 379–395. [Google Scholar] [CrossRef]
- Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behaviour Research and Therapy, 33(3), 335–343. [Google Scholar] [CrossRef]
- Matheson, E., Wade, T. D., & Yiend, J. (2019). Utilising cognitive bias modification to remedy appearance and self-worth biases in eating disorder psychopathology: A systematic review. Journal of Behavior Therapy and Experimental Psychiatry, 65, 101482. [Google Scholar] [CrossRef]
- Mogg, K., & Bradley, B. P. (2016). Anxiety and attention to threat: Cognitive mechanisms and treatment with attention bias modification. Behaviour Research and Therapy, 87, 76–108. [Google Scholar] [CrossRef] [PubMed]
- Mogg, K., Waters, A. M., & Bradley, B. P. (2017). Attention bias modification (ABM): Review of effects of multisession ABM training on anxiety and threat-related attention in high-anxious individuals. Clinical Psychological Science, 5(4), 698–717. [Google Scholar] [CrossRef] [PubMed]
- Mogoaşe, C., David, D., & Koster, E. H. (2014). Clinical efficacy of attentional bias modification procedures: An updated meta-analysis. Journal of Clinical Psychology, 70(12), 1133–1157. [Google Scholar] [CrossRef]
- Moussally, J. M., Brosch, T., & Van der Linden, M. (2016). Time course of attentional biases toward body shapes: The impact of body dissatisfaction. Body Image, 19, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Nahum, M., Van Vleet, T. M., Sohal, V. S., Mirzabekov, J. J., Rao, V. R., Wallace, D. L., Lee, M. B., Dawes, H., Stark-Inbar, A., Jordan, J. T., Biagianti, B., Merzenich, M., & Chang, E. F. (2017). Immediate mood scaler: Tracking symptoms of depression and anxiety using a novel mobile mood scale. JMIR mHealth and uHealth, 5(4), e44. [Google Scholar] [CrossRef] [PubMed]
- Namaky, N., Beltzer, M. L., Werntz, A. J., Lambert, A. E., Isaacowitz, D. M., & Teachman, B. A. (2017). Moderators of age effects on attention bias toward threat and its association with anxiety. Journal of Affective Disorders, 216, 46–57. [Google Scholar] [CrossRef]
- Nejati, V., Fathi, E., Shahidi, S., & Salehinejad, M. A. (2019). Cognitive training for modifying interpretation and attention bias in depression: Relevance to mood improvement and implications for cognitive intervention in depression. Asian Journal of Psychiatry, 39, 23–28. [Google Scholar] [CrossRef]
- Nelson, A. L., Purdon, C., Quigley, L., Carriere, J., & Smilek, D. (2015). Distinguishing the roles of trait and state anxiety on the nature of anxiety-related attentional biases to threat using a free viewing eye movement paradigm. Cognition and Emotion, 29(3), 504–526. [Google Scholar] [CrossRef]
- Pine, R., Fleming, T., McCallum, S., & Sutcliffe, K. (2020). The effects of casual videogames on anxiety, depression, stress, and low mood: A systematic review. Games for Health Journal, 9(4), 255–264. [Google Scholar] [CrossRef]
- Pintzinger, N. M., Pfabigan, D. M., Tran, U. S., Kryspin-Exner, I., & Lamm, C. (2016). Attentional biases in healthy adults: Exploring the impact of temperament and gender. Journal of Behavior Therapy and Experimental Psychiatry, 52, 29–37. [Google Scholar] [CrossRef]
- Rued, H. A., Hilmert, C. J., Strahm, A. M., & Thomas, L. E. (2018). The influence of stress on attentional bias to threat: An angry face and a noisy crowd. Psychonomic Bulletin & Review, 26(3), 943–950. [Google Scholar] [CrossRef]
- See, J., MacLeod, C., & Bridle, R. (2009). The reduction of anxiety vulnerability through the modification of attentional bias: A real-world study using a home-based cognitive bias modification procedure. Journal of Abnormal Psychology, 118(1), 65. [Google Scholar] [CrossRef] [PubMed]
- Waters, A. M., Pittaway, M., Mogg, K., Bradley, B. P., & Pine, D. S. (2013). Attention training towards positive stimuli in clinically anxious children. Developmental Cognitive Neuroscience, 4, 77–84. [Google Scholar] [CrossRef]
- Zanon, C., Brenner, R. E., Baptista, M. N., Vogel, D. L., Rubin, M., Al-Darmaki, F. R., Gonçalves, M., Heath, P. J., Liao, H.-Y., Mackenzie, C. S., Topkaya, N., Wade, N. G., & Zlati, A. (2021). Examining the dimensionality, reliability, and invariance of the Depression, Anxiety, and Stress Scale–21 (DASS-21) across eight countries. Assessment, 28(6), 1531–1544. [Google Scholar] [CrossRef] [PubMed]
| Experimental | Control | ||||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Age M (SD) | 47.7 | (18.8) | 51.7 | (17.2) | |
| Gender | |||||
| Female | 58 | 65.9% | 49 | 64.5% | |
| Male | 20 | 22.7% | 16 | 21.1% | |
| Non-binary/Self-described | 1 | 1.1% | 0 | 0.0% | |
| Prefer not to say | 9 | 10.2% | 11 | 14.5% | |
| Educational Attainment | |||||
| Some secondary | 5 | 5.7% | 2 | 2.6% | |
| Completed secondary | 8 | 9.1% | 13 | 17.1% | |
| Vocational certificate | 11 | 12.5% | 13 | 17.1% | |
| Undergraduate degree | 30 | 34.1% | 21 | 27.6% | |
| Postgraduate degree | 24 | 27.3% | 14 | 18.4% | |
| Other | 2 | 2.3% | 3 | 3.9% | |
| Prefer not to say | 8 | 9.1% | 10 | 13.2% | |
| Employment | |||||
| Full-time | 19 | 21.6% | 17 | 22.4% | |
| Part-time | 13 | 14.8% | 14 | 18.5% | |
| Student | 4 | 4.5% | 2 | 2.6% | |
| Casual (non-contracted) | 19 | 21.5% | 13 | 17.1% | |
| Carer duties | 3 | 3.4% | 0 | 0.0% | |
| Not currently working | 22 | 25.0% | 19 | 25.0% | |
| Prefer not to say | 8 | 9.1% | 11 | 14.5% | |
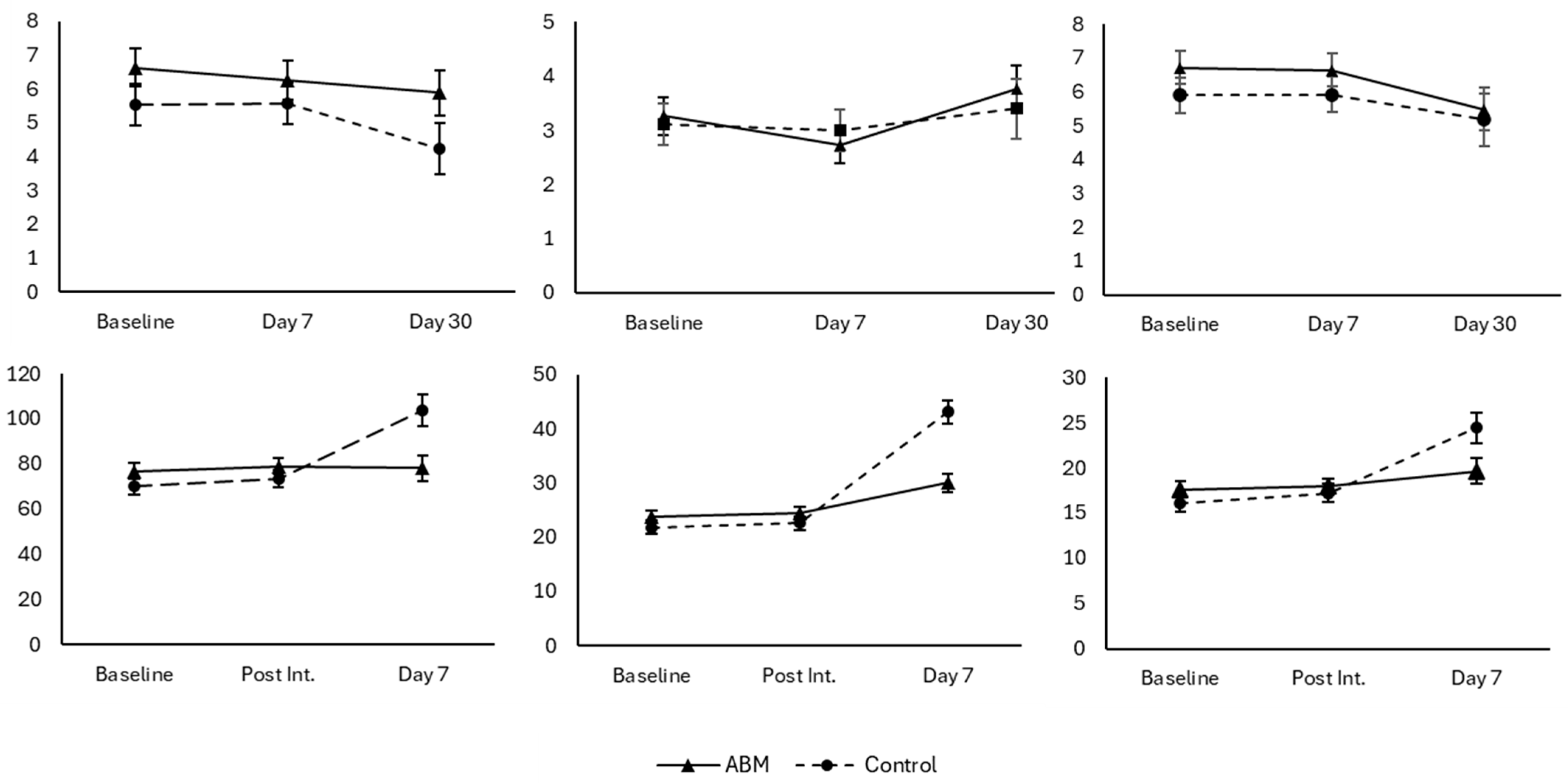
| Outcome measures | M | SD | M | SD | |
| IMS total baseline | 76.88 | 25.09 | 69.75 | 28.91 | |
| IMS total post-experiment | 78.41 | 27.97 | 73.53 | 34.01 | |
| IMS total day 7 | 76.32 | 45.34 | 98.72 | 51.90 | |
| IMS depression baseline | 23.59 | 9.34 | 21.74 | 10.23 | |
| IMS depression post-experiment | 24.32 | 10.08 | 22.66 | 11.60 | |
| IMS depression day 7 | 29.18 | 12.29 | 40.39 | 7.00 | |
| IMS anxiety baseline | 17.49 | 7.63 | 16.01 | 8.05 | |
| IMS anxiety post-experiment | 17.74 | 7.80 | 17.26 | 8.91 | |
| IMS anxiety day 7 | 18.75 | 9.88 | 23.61 | 9.60 | |
| DASS depression baseline | 6.52 | 5.40 | 5.36 | 4.85 | |
| DASS depression day 7 | 6.14 | 5.41 | 5.64 | 5.49 | |
| DASS depression day 30 | 5.24 | 4.03 | 3.33 | 3.56 | |
| DASS anxiety baseline | 3.26 | 3.07 | 2.96 | 3.22 | |
| DASS anxiety day 7 | 2.69 | 2.85 | 3.04 | 3.79 | |
| DASS anxiety day 30 | 3.57 | 2.64 | 2.55 | 1.37 | |
| DASS stress baseline | 6.68 | 4.39 | 5.73 | 4.62 | |
| DASS stress day 7 | 6.52 | 4.63 | 5.96 | 4.74 | |
| DASS stress day 30 | 4.96 | 3.18 | 4.77 | 2.55 | |
| Flowers | Happy-Angry | Happy-Neutral | Neutral-Happy | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | ||
| Age M (SD) | 30.74 | 8.31 | 26.92 | 8.97 | 31.16 | 8.76 | 29.51 | 11.89 | |
| Gender | |||||||||
| Female | 36 | 72.0% | 42 | 79.2% | 29 | 63.0% | 28 | 71.8% | |
| Male | 14 | 28.0% | 10 | 18.9% | 11 | 23.9% | 11 | 28.2% | |
| Non-binary | 0 | 0.0% | 1 | 1.9% | 6 | 13.1% | 0 | 0.0% | |
| Educational Attainment | |||||||||
| Some secondary | 0 | 0.0% | 2 | 3.8% | 0 | 0.0% | 0 | 0.0% | |
| Completed secondary | 3 | 6.0% | 6 | 11.3% | 2 | 4.4% | 3 | 7.7% | |
| Vocational certificate | 6 | 12.0% | 5 | 9.4% | 3 | 6.5% | 6 | 15.4% | |
| Bachelor’s degree | 30 | 60.0% | 33 | 62.3% | 22 | 47.8% | 22 | 56.4% | |
| Postgraduate degree | 11 | 22.0% | 7 | 13.2% | 17 | 37.0% | 7 | 17.9% | |
| Other | 0 | 0.0% | 0 | 0.0% | 2 | 4.3% | 1 | 2.6% | |
| Employment | |||||||||
| Full time | 18 | 35.3% | 10 | 18.9% | 16 | 34.8% | 14 | 35.9% | |
| Part time | 10 | 19.6% | 8 | 15.1% | 9 | 19.6% | 5 | 12.8% | |
| Casual | 1 | 2.0% | 2 | 3.8% | 2 | 4.3% | 1 | 2.6% | |
| Not currently employed | 2 | 3.9% | 3 | 5.7% | 1 | 2.2% | 1 | 2.6% | |
| Student | 20 | 39.2% | 30 | 56.6% | 18 | 39.1% | 18 | 46.2% | |
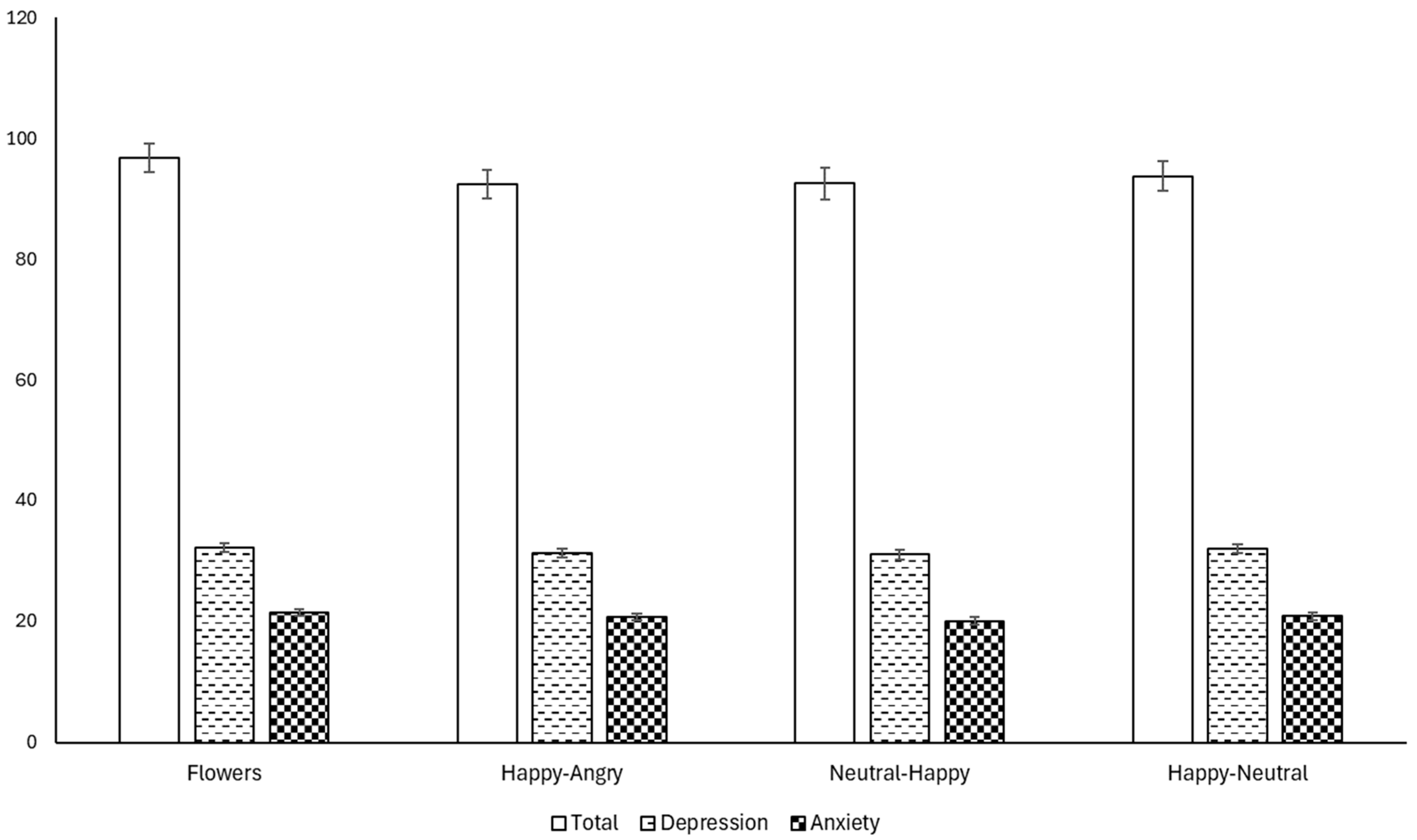
| Outcome Measures | M | SD | M | SD | M | SD | M | SD | |
| IMS depression baseline | 32.9 | 7.91 | 28.91 | 8.26 | 30.45 | 7.98 | 32.34 | 9.59 | |
| IMS depression post-experiment | 33.39 | 7.28 | 29.89 | 8.75 | 31.64 | 7.56 | 31.36 | 9.31 | |
| IMS anxiety baseline | 21.15 | 6.05 | 19.35 | 6.8 | 19.95 | 6.95 | 20 | 7.65 | |
| IMS anxiety post-experiment | 22 | 6.05 | 20.25 | 6.45 | 20.8 | 5.95 | 19.25 | 6.9 | |
| IMS total baseline | 99.5 | 20.54 | 88.51 | 23.24 | 91.47 | 23.49 | 93.54 | 30.74 | |
| IMS total post-experiment | 102 | 20.43 | 89.15 | 28.58 | 92.5 | 26.32 | 91.84 | 28.58 | |
| Control | Experimental | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Log10 Latency | Latency Change | Log10 Latency | Latency Change | |||||||||
| T1 | T2 | T3 | T2-T1 | T3-T1 | T3-T2 | T1 | T2 | T3 | T2-T1 | T3-T1 | T3-T2 | |
| T1 | ||||||||||||
| IMI Total | −0.189 | 0.123 | −0.008 | 0.398 ** | ||||||||
| IMS Depression | −0.193 | 0.146 | 0.030 | 0.481 *** | ||||||||
| IMS Anxiety | −0.116 | 0.061 | −0.008 | 0.352 * | ||||||||
| DASS Stress | −0.028 | 0.189 | −0.018 | 0.113 | ||||||||
| DASS Anxiety | −0.009 | 0.203 | −0.049 | 0.087 | ||||||||
| DASS Depression | 0.044 | 0.083 | 0.118 | 0.390 ** | ||||||||
| T2 | ||||||||||||
| IMS Total | −0.081 | 0.052 | 0.033 | −0.500 | 0.500 | 0.090 | 0.119 | 0.242 | 0.110 | 0.280 | ||
| IMS Depression | −0.098 | 0.020 | 0.001 | −0.451 | 0.469 | 0.109 | 0.184 | 0.338 * | 0.224 | 0.132 | ||
| IMS Anxiety | −0.057 | −0.039 | 0.062 | −0.214 | 0.214 | 0.043 | 0.035 | 0.168 | 0.083 | 0.185 | ||
| DASS Stress | −0.021 | −0.048 | 0.213 | −0.496 | 0.587 | −0.133 | −0.227 | 0.129 | 0.303 | 0.189 | ||
| DASS Anxiety | 0.006 | −0.250 | 0.211 | 0.000 | 0.076 | −0.101 | −0.054 | 0.084 | −0.108 | 0.173 | ||
| DASS Depression | 0.102 | 0.045 | 0.093 | −0.674 | 0.281 | 0.055 | 0.238 | 0.332 * | 0.128 | 0.483 | ||
| T3 | ||||||||||||
| IMS Total | 0.155 | 0.288 | −0.577 | 0.024 | 0.108 | −0.024 | ||||||
| IMS Depression | −0.121 | 0.073 | −0.182 | 0.076 | 0.183 | −0.238 | ||||||
| IMS Anxiety | −0.116 | −0.179 | 0.214 | 0.201 | −0.018 | −0.166 | ||||||
| DASS Stress | −0.300 | −0.091 | −0.200 | −0.300 | 0.703 ** | 0.188 | −0.262 | 0.703 | ||||
| DASS Anxiety | 0.258 | −0.572 | −0.775 | 0.258 | 0.325 | 0.085 | −0.108 | 0.325 | ||||
| DASS Depression | 0.131 | −0.518 | −0.393 | 0.131 | 0.234 | 0.485 * | 0.003 | 0.234 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skvarc, D.; Hyder, S.; Leary, L.; Watts, S.; Seecamp, M.; Burns, L.; Hayley, A. Brief Repeated Attention Training for Psychological Distress: Findings from Two Experiments. Behav. Sci. 2025, 15, 1052. https://doi.org/10.3390/bs15081052
Skvarc D, Hyder S, Leary L, Watts S, Seecamp M, Burns L, Hayley A. Brief Repeated Attention Training for Psychological Distress: Findings from Two Experiments. Behavioral Sciences. 2025; 15(8):1052. https://doi.org/10.3390/bs15081052
Chicago/Turabian StyleSkvarc, David, Shannon Hyder, Laetitia Leary, Shahni Watts, Marcus Seecamp, Lewis Burns, and Alexa Hayley. 2025. "Brief Repeated Attention Training for Psychological Distress: Findings from Two Experiments" Behavioral Sciences 15, no. 8: 1052. https://doi.org/10.3390/bs15081052
APA StyleSkvarc, D., Hyder, S., Leary, L., Watts, S., Seecamp, M., Burns, L., & Hayley, A. (2025). Brief Repeated Attention Training for Psychological Distress: Findings from Two Experiments. Behavioral Sciences, 15(8), 1052. https://doi.org/10.3390/bs15081052