
Developing the Public Speaking Anxiety Scale (PSAS) for Adolescents: The Mediating Role of Dysfunctional Emotion Regulation in the Effect of Irrational Beliefs on Public Speaking Anxiety

Abstract
1. Introduction
Present Study
2. Methods
2.1. Research Model
2.2. Study Group and Data Collection Process
2.3. Data Collection Tools
2.3.1. Public Speaking Anxiety Scale (PSAS)
2.3.2. Irrational Beliefs Scale (IBS)
2.3.3. Regulation of Emotions Questionnaire (REQ)
2.3.4. Social Anxiety Scale for Adolescents (SAS-A)
2.4. Data Analysis
3. Findings
3.1. Study 1. Validity and Reliability of the Public Speaking Anxiety Scale (PSAS)
3.1.1. Findings on Validity
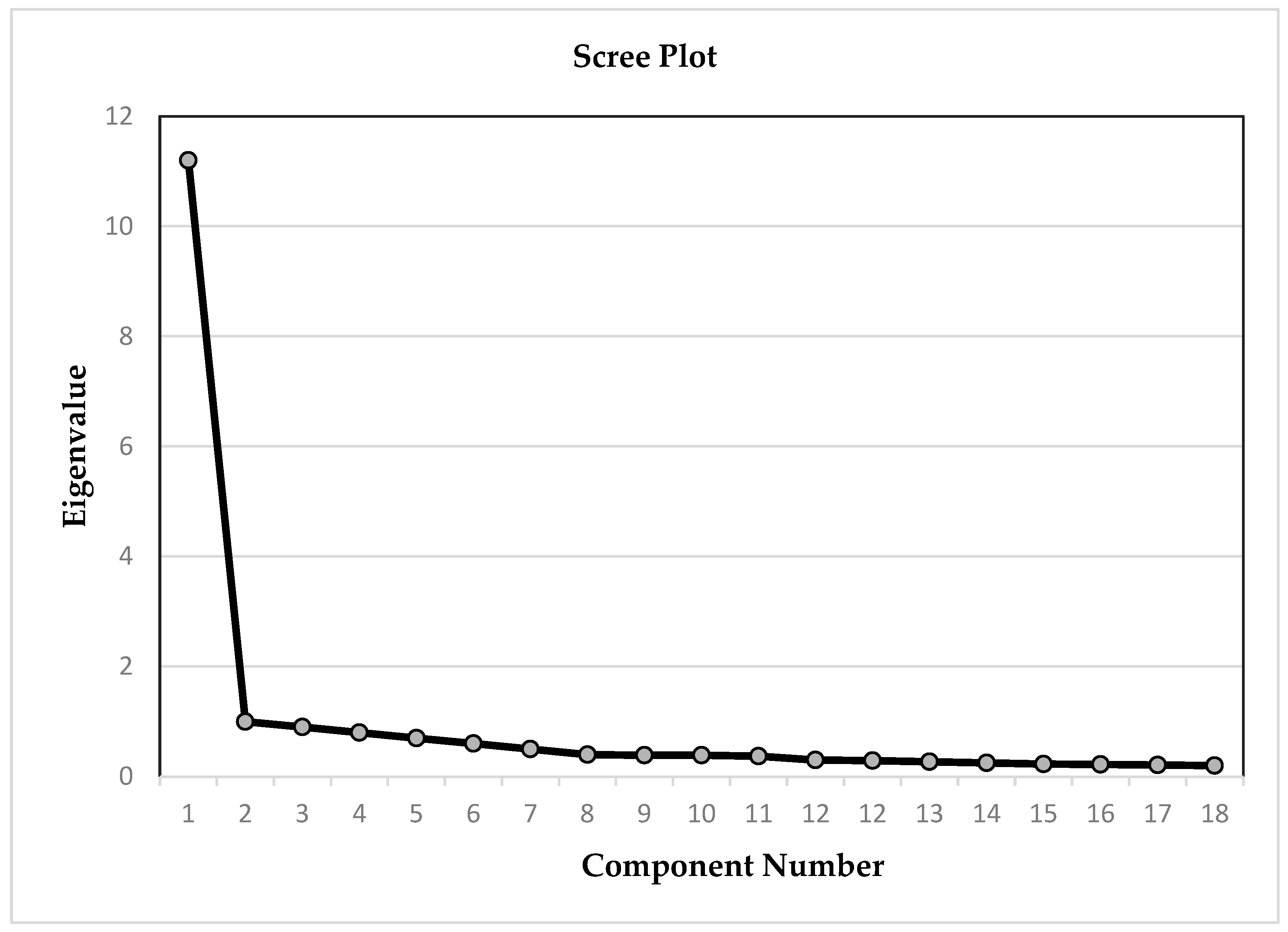
3.1.2. Findings from the Exploratory Factor Analysis
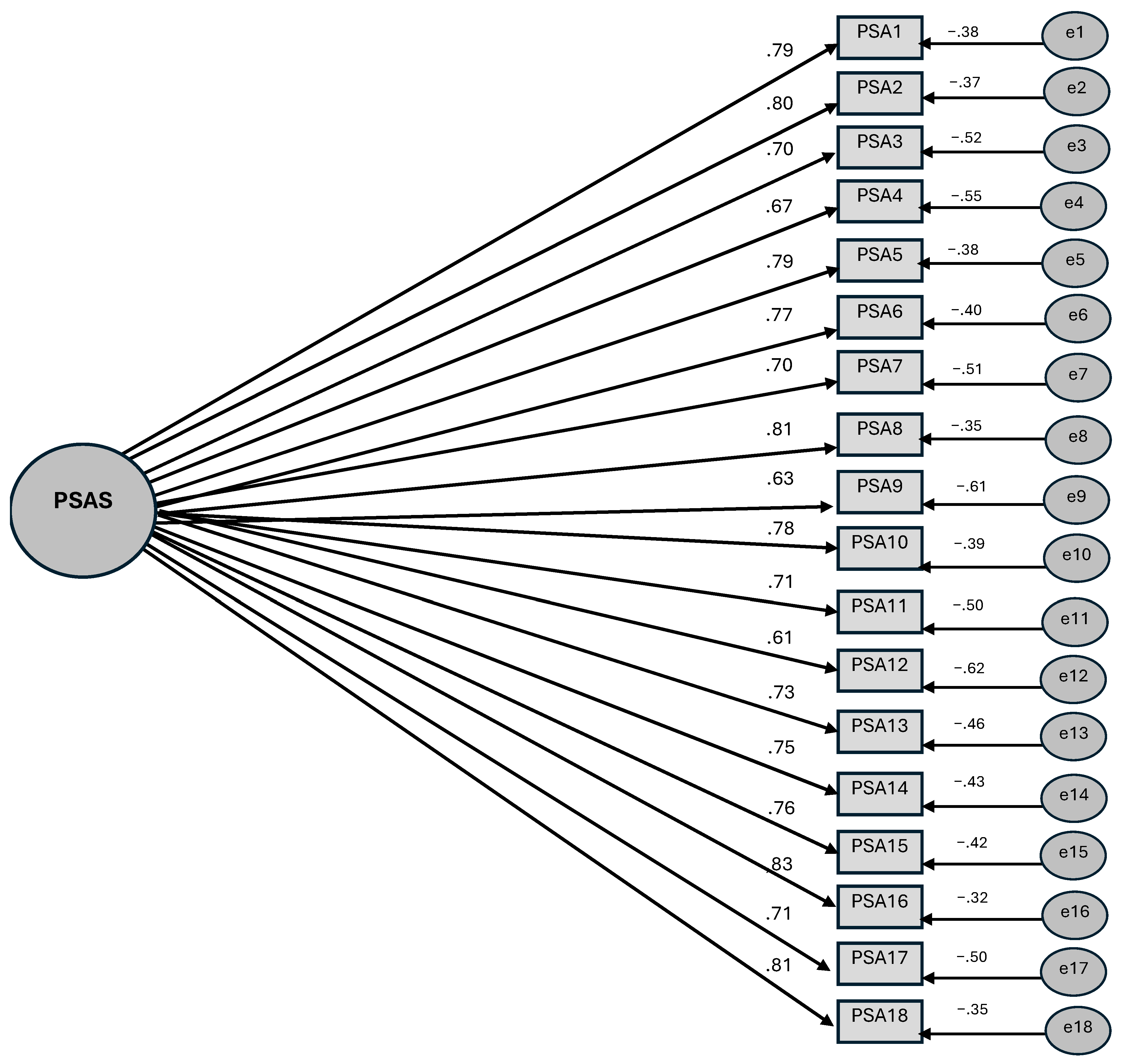
3.1.3. Findings from the Confirmatory Factor Analysis
3.1.4. Findings on Validity in Criterion Scale, Average Variance Extracted (AVE) and Composite Reliability (CR) Analysis
3.1.5. Findings on Reliability
3.1.6. Internal Consistency Findings
3.2. Repeated Test Findings
3.3. Study 2: Findings on the Correlational and Mediating Effects of Internal Dysfunctional and Extrinsic Dysfunctional Emotion Regulation on Public Speaking Anxiety and Irrational Beliefs in High School Students
4. Discussion
5. Limitations and Future Research Recommendations
- (1)
- The high degree of correlation between the PSAS and the criterion scale SAS-A may have been partially affected by the common method variance. In subsequent studies, a range of methods or measurement tools may be employed to ascertain more substantial relationships in the context of criterion scale validity.
- (2)
- Despite the multifaceted nature of public speaking anxiety, manifesting in behavioural, physiological and cognitive domains, the PSAS utilised in this study encompasses only a single dimension. In order to facilitate the formation of these dimensions with greater clarity, it is recommended that the items be elevated to a more distinct level through the implementation of multiple pilot applications during the scale development process.
- (3)
- The findings of the present study were only obtained from data collected from adolescents in Turkey. The question of the PSAS’s validity in other cultures can be investigated.
- (4)
- This study was conducted on cross-sectional data. It is posited that a longitudinal study of the same model in a process such as adolescence, where variability is experienced to a greater extent, will engender more generalisable results.
- (5)
- This study overlooked the issue of gender-related measurement invariance with regard to a significant variable in adolescence, namely public speaking anxiety. In subsequent studies, the measurement invariance or level of gender-related PSAS can be determined.
- (6)
- It has previously been demonstrated that internal dysfunctional emotion regulation strategies are rooted in the cognitive process (Carthy et al., 2010; Dixon et al., 2020). In consideration of the mediating role identified in this study, it is posited that school-based group activities for emotion regulation will be efficacious in preventing adolescents from experiencing social anxiety and similarly public speaking anxiety.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ambrosini, P. J., Bennett, D. S., & Elia, J. (2013). Attention deficit hyperactivity disorder characteristics: II. Clinical correlates of irritable mood. Journal of Affective Disorders, 145(1), 70–76. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association (APA). (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing. [Google Scholar]
- Aydın, A., & Sütçü, S. T. (2007). Ergenler için Sosyal Kaygı Ölçeğinin (ESKÖ) geçerlik ve güvenirliğinin incelenmesi. Çocuk ve Gençlik Ruh Sağlığı Dergisi, 14(2), 79–89. [Google Scholar]
- Bartholomay, E. M., & Houlihan, D. D. (2016). Public Speaking Anxiety Scale: Preliminary psychometric data and scale validation. Personality and Individual Differences, 94, 211–215. [Google Scholar] [CrossRef]
- Bates, G. W., Elphinstone, B., & Whitehead, R. (2021). Self-compassion and emotional regulation as predictors of social anxiety. Psychology and Psychotherapy: Theory, Research and Practice, 94(3), 426–442. [Google Scholar] [CrossRef] [PubMed]
- Behnke, R. R., & Beatty, M. J. (1981). A cognitive-physiological model of speech anxiety. Communication Monographs, 48(2), 158–163. [Google Scholar] [CrossRef]
- Behnke, R. R., Sawyer, C. R., & King, P. E. (1987). The communication of public speaking anxiety. Communication Education, 36(2), 138–141. [Google Scholar] [CrossRef]
- Beidel, D. C., & Turner, S. M. (2007). Shy children, phobic adults: Nature and treatment of social anxiety disorder (2nd ed.). American Psychological Association. [Google Scholar]
- Bernard, M. E. (1984). Childhood emotion and cognitive behavior therapy: A rationalemotive perspective. In P. C. Kendall (Ed.), Advances in cognitive-behavioral research and therapy (pp. 213–253). Academic Press, Inc. [Google Scholar]
- Biggs, B. K., Vernberg, E. M., & Wu, Y. P. (2012). Social anxiety and adolescents’ friendships: The role of social withdrawal. The Journal of Early Adolescent, 32(6), 802–823. [Google Scholar] [CrossRef]
- Blöte, A. W., Miers, A. C., Heyne, D. A., Clark, D. M., & Westenberg, P. M. (2014). The relation between social anxiety and audience perception: Examining Clark and Wells’ (1995) model among adolescents. Behavioural and Cognitive Psychotherapy, 42(5), 555–567. [Google Scholar] [CrossRef]
- Brandrick, C., Hooper, N., Roche, B., Kanter, J., & Tyndall, I. (2021). A comparison of ultra-brief cognitive defusion and positive affirmation interventions on the reduction of public speaking anxiety. The Psychological Record, 71, 109–117. [Google Scholar] [CrossRef]
- Breakey, L. K. (2005). Fear of public speaking-the role of the SLP. Seminars in Speech and Language, 2(26), 107–117. [Google Scholar] [CrossRef]
- Brockmeyer, T., Holtforth, M. G., Pfeiffer, N., Backenstrass, M., Friederich, H.-C., & Bents, H. (2012). Mood regulation expectancies and emotion avoidance in depression vulnerability. Personality and Individual Differences, 53(3), 351–354. [Google Scholar] [CrossRef]
- Brühl, A. B., Herwig, U., Delsignore, A., Jäncke, L., & Rufer, M. (2013). General emotion processing in social anxiety disorder: Neural issues of cognitive control. Psychiatry Research: Neuroimaging, 212(2), 108–115. [Google Scholar] [CrossRef] [PubMed]
- Carthy, T., Horesh, N., Apter, A., Edge, M. D., & Gross, J. J. (2010). Emotional reactivity and cognitive regulation in anxious children. Behaviour Research and Therapy, 48, 384–493. [Google Scholar] [CrossRef] [PubMed]
- Castella, K., Platow, M. J., Tamir, M., & Gross, J. J. (2018). Beliefs about emotion: Implications for avoidancebased emotion regulation and psychological health. Cognition and Emotion, 32(4), 773–795. [Google Scholar] [CrossRef]
- Cécillon, F. X., Mermillod, M., Leys, C., Lachaux, J. P., Le Vigouroux, S., & Shankland, R. (2024). Trait anxiety, emotion regulation, and metacognitive beliefs: An observational study incorporating separate network and correlation analyses to examine associations with executive functions and academic achievement. Children, 11(1), 123. [Google Scholar] [CrossRef]
- Chiu, K., Clark, D. M., & Leigh, E. (2021). Cognitive predictors of adolescent social anxiety. Behaviour Research and Therapy, 137, 103801. [Google Scholar] [CrossRef]
- Choi, Y. S., & Kim, J. M. (2008). The effects of irrational belief and social support on adolescents’ social anxiety. Journal of Families and Better Life, 26(2), 103–114. [Google Scholar]
- Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. Guilford Press. [Google Scholar]
- Cohen, J. (2013). Statistical power analysis for the behavioral science. Routledge. [Google Scholar]
- Çabuker, N. D., Çelik, S. B., & Aldemir, A. (2020). Topluluk Önünde Konuşma Kaygısı Ölçeğinin Türkçeye uyarlanması: Geçerlik ve güvenirlik çalışması. Elektronik Sosyal Bilimler Dergisi, 19(76), 1601–1610. [Google Scholar] [CrossRef]
- Çivitçi, A. (2009). Relationship between irrational beliefs and life satisfaction in early adolescents. Eurasian Journal of Educational Research, 37, 91–109. [Google Scholar]
- Dacey, J., & Kenny, M. (1997). Adolescent development. Brown & Benchmark Publishers. [Google Scholar]
- David, D., Lynn, S. J., & Ellis, A. (2009). Rational and irrational beliefs: Research, theory, and clinical practice. Oxford University Press. [Google Scholar]
- David, D., Schnur, J., & Belloiu, A. (2002). Another search for the “hot” cognitions: Appraisal, irrational beliefs, attributions, and their relation to emotion. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 15, 93–131. [Google Scholar] [CrossRef]
- Davison, G. C., & Zighelboim, V. (1987). Irrational beliefs in the articulated thoughts of college students with social anxiety. Journal of Rational Emotive Therapy, 5(4), 238–254. [Google Scholar] [CrossRef]
- De Lijster, J. M., Dieleman, G. C., Utens, E. M., Dierckx, B., Wierenga, M., Verhulst, F. C., & Legerstee, J. S. (2018). Social and academic functioning in adolescents with anxiety disorders: A systematic review. Journal of Affective Disorders, 230, 108–117. [Google Scholar] [CrossRef]
- Demir, T., & Melanlıoğlu, D. (2014). Speaking anxiety scale for secondary school education students: Validity and reliability study. Ankara University Journal of Faculty of Educational Sciences (JFES), 47(1), 103–124. [Google Scholar] [CrossRef]
- DeVellis, R. F., & Thorpe, C. T. (2021). Scale development: Theory and applications. Sage Publications. [Google Scholar]
- Dixon, M. L., Moodie, C. A., Goldin, P. R., Farb, N., Heimberg, R. G., & Gross, J. J. (2020). Emotion regulation in social anxiety disorder: Reappraisal and acceptance of negative self-beliefs. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 5(1), 119–129. [Google Scholar] [CrossRef] [PubMed]
- Duy, B., & Yıldız, M. A. (2014). Ergenler için Duygu Düzenleme Ölçeğinin Türkçeye uyarlanması. Turkish Psychological Counseling and Guidance Journal, 5(41), 23–35. [Google Scholar] [CrossRef]
- Ellis, A. (2013). Rational emotive therapy. In Albert Ellis revisited (pp. 25–37). Routledge. [Google Scholar]
- Feldman, D. B., & Silvia, P. J. (2010). Public speaking for psychologists: A lighthearted guide to research presentations, job talks, and other opportunities to embarrass yourself. American Psychological Association. [Google Scholar]
- Field, A. (2009). SPSS. Discovering statistics using SPSS (2nd ed.). Artmed. [Google Scholar]
- Fisher, P. H., Masia-Warner, C., & Klein, R. G. (2004). Skills for social and academic success: A school-based intervention for social anxiety disorder in adolescents. Clinical Child and Family Psychology Review, 7, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Fives, C. J., Kong, G., Fuller, J. R., & DiGiuseppe, R. (2011). Anger, aggression, and irrational beliefs in adolescents. Cognitive Therapy and Research, 35, 199–208. [Google Scholar] [CrossRef]
- Flett, G. L., Hewitt, P. L., & Cheng, W. M. W. (2008). Perfectionism, distress, and irrational beliefs in high school students: Analyses with an abbreviated survey of personal beliefs for adolescents. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 26, 194–205. [Google Scholar] [CrossRef]
- Fornell, C., & Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research, 18(1), 39–50. [Google Scholar] [CrossRef]
- Fremouw, W. J., & Breitenstein, J. L. (1990). Speech anxiety. In H. Leitenberg (Ed.), Handbook of social and evaluation anxiety (pp. 455–474). Springer. [Google Scholar]
- Fremouw, W. J., & Zitter, R. E. (1978). A comparison of skills training and cognitive restructuring-relaxation for the treatment of speech anxiety. Behavior Therapy, 9(2), 248–259. [Google Scholar] [CrossRef]
- Fuller, C. M., Simmering, M. J., Atinc, G., Atinc, Y., & Babin, B. J. (2016). Common methods variance detection in business research. Journal of Business Research, 69(8), 3192–3198. [Google Scholar] [CrossRef]
- Gallego, A., McHugh, L., Penttonen, M., & Lappalainen, R. (2022). Measuring public speaking anxiety: Self-report, behavioral, and physiological. Behavior Modification, 46(4), 782–798. [Google Scholar] [CrossRef] [PubMed]
- Golombek, K., Lidle, L., Tuschen-Caffier, B., Schmitz, J., & Vierrath, V. (2020). The role of emotion regulation in socially anxious children and adolescents: A systematic review. European Child & Adolescent Psychiatry, 29(11), 1479–1501. [Google Scholar] [CrossRef]
- Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26, 41–54. [Google Scholar] [CrossRef]
- Gratz, K. L., Weiss, N. H., McDermott, M. J., Dilillo, D., Messman-Moore, T., & Tull, M. T. (2017). Emotion dysregulation mediates the relation between borderline personality disorder symptoms and later physical health symptoms. Journal of Personality Disorders, 31, 433–448. [Google Scholar] [CrossRef]
- Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348. [Google Scholar] [CrossRef]
- Gündüz, A., & Demir, S. (2021). Konuşma Kaygısı Ölçeği’nin geliştirilmesi: Geçerlik ve güvenirlik çalışması. Fırat Üniversitesi Sosyal Bilimler Dergisi, 31(1), 145–159. [Google Scholar] [CrossRef]
- Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., & Tatham, R. L. (2013). Multivariate data analysis. Pearson Education Limited. [Google Scholar]
- Hannesdóttir, D. K. (2007). Reduction of fear arousal in young adults with speech anxiety through elicitation of positive emotions [Unpublished doctoral dissertation, Virginia Polytechnic Institute and State University]. [Google Scholar]
- Hannesdóttir, D. K., & Ollendick, T. H. (2007). The role of emotion regulation in the treatment of child anxiety disorders. Clinical Child and Family Psychology Review, 10(3), 275–293. [Google Scholar] [CrossRef] [PubMed]
- Harb, G. C., Eng, W., Zaider, T., & Heimberg, R. G. (2003). Behavioral assessment of public-speaking anxiety using a modified version of the social performance rating scale. Behaviour Research and Therapy, 41(11), 1373–1380. [Google Scholar] [CrossRef]
- Hatkevich, C., Sumlin, E., & Sharp, C. (2021). Examining associations between child abuse and neglect experiences with emotion regulation difficulties indicative of adolescent suicidal ideation risk. Frontiers in Psychiatry, 12, 630697. [Google Scholar] [CrossRef]
- Hofmann, S. G., & DiBartolo, P. M. (2000). An instrument to assess self-statements during public speaking: Scale development and preliminary psychometric properties. Behavior Therapy, 31(3), 499–515. [Google Scholar] [CrossRef]
- Hong, E. J., & Kangas, M. (2022). The relationship between beliefs about emotions and emotion regulation: A systematic review. Behaviour Change, 39(4), 205–234. [Google Scholar] [CrossRef]
- Jazaieri, H., Morrison, A. S., Goldin, P. R., & Gross, J. J. (2015). The role of emotion and emotion regulation in social anxiety disorder. Current Psychiatry Reports, 17, 531. [Google Scholar] [CrossRef]
- Keşaplı, G., & Çifçi, M. (2019). Ortaokul öğrencilerinin konuşma kaygısı. The Journal of Academic Social Science Studies, 1(54), 463–484. [Google Scholar] [CrossRef]
- Kinay, İ., & Özkan, E. (2014). Öğretmen adayları için Konuşma Kaygısı Ölçeği (ÖAKKÖ) geliştirilmesi: Geçerlik ve güvenirlik çalışması. Electronic Turkish Studies, 9(5), 1747–1760. [Google Scholar] [CrossRef]
- La Greca, A. M., Dandes, S. K., Wick, P., Shaw, K., & Stone, W. L. (1988). Development of the social anxiety scale for children: Reliability and concurrent validity. Journal of Clinical Child Psychology, 17, 84–91. [Google Scholar] [CrossRef]
- La Greca, A. M., & Lopez, N. (1998). Social anxiety among adolescents: Linkages with peer relations and friendships. Journal of Abnormal Child Psychology, 26, 83–94. [Google Scholar] [CrossRef]
- Lang, P. J. (1969). The mechanics of desensitization and the laboratory study of human fear. In C. Franks (Ed.), Assessment and status of the behavior therapies. McGraw-Hill. [Google Scholar]
- Leigh, E., & Clark, D. M. (2016). Cognitive therapy for social anxiety disorder in adolescents: A development case series. Behavioural and Cognitive Psychotherapy, 44(1), 1–17. [Google Scholar] [CrossRef]
- Li, C., Li, T., Cao, J., Su, H., Sun, H., & Cai, Y. (2019). Mediating role of attentional control in the relationship between irrational beliefs and social anxiety. Chinese General Practice, 22(25), 3132–3137. [Google Scholar] [CrossRef]
- Lin, X. B., Lee, T. S., Man, R. E. K., Poon, S. H., & Fenwick, E. (2021). Rasch analysis reveals multidimensionality in the Public Speaking Anxiety Scale. Health Services and Outcomes Research Methodology, 22(3), 332–348. [Google Scholar] [CrossRef]
- Lohr, J. M., & Bonge, D. (1981). On the distinction between illogical and irrational beliefs and their relationship to anxiety. Psychological Reports, 48, 191–194. [Google Scholar] [CrossRef]
- McCroskey, J. C. (1977). Oral communication apprehension: A summary of recent theory and research. Human Communication Research, 4(1), 78–96. [Google Scholar] [CrossRef]
- McCroskey, J. C. (1982). Oral communication apprehension: A reconceptualization. Annals of the International Communication Association, 6(1), 136–170. [Google Scholar] [CrossRef]
- McNatt, D. B. (2019). Enhancing public speaking confidence, skills, and performance: An experiment of service-learning. The International Journal of Management Education, 17(2), 276–285. [Google Scholar] [CrossRef]
- Miers, A. C., Blöte, A. W., Heyne, D. A., & Westenberg, P. M. (2014). Developmental pathways of social avoidance across adolescence: The role of social anxiety and negative cognition. Journal of Anxiety Disorders, 28(8), 787–794. [Google Scholar] [CrossRef]
- Moloudi, A., Arian, H., Mahdavi, M., Madah, F., & Roghaeeh Taghipour, R. T. (2022). Cognitive-behavioral therapy (CBT) in the form of Emotive Behavior Therapy (REBT) Intervention on irrational Beliefs and Anxiety of adolescent girls with social anxiety. Preventive Counseling, 3(2), 47–59. [Google Scholar] [CrossRef]
- Monson, T. C., & Snyder, M. (1977). Actors, observers, and the attribution process: Toward a reconceptualization. Journal of Experimental Social Psychology, 13, 89–111. [Google Scholar] [CrossRef]
- Moshman, D. (2013). Adolescent rationality. Advances in Child Development and Behavior, 45, 155–183. [Google Scholar] [CrossRef]
- Mörtberg, E., Jansson-Fröjmark, M., Pettersson, A., & Hennlid-Oredsson, T. (2018). Psychometric properties of the personal report of public speaking anxiety (PRPSA) in a sample of university students in Sweden. International Journal of Cognitive Therapy, 11, 421–433. [Google Scholar] [CrossRef]
- Mulac, A., & Sherman, A. R. (1974). Behavioral assessment of speech anxiety. Quarterly Journal of Speech, 60, 134–143. [Google Scholar] [CrossRef]
- Muris, P., & Field, A. P. (2008). Distorted cognition and pathological anxiety in children and adolescents. Cognition and Emotion, 22(3), 395–421. [Google Scholar] [CrossRef]
- Nicolson, D., & Ayers, H. (2004). Adolescent problems. A practical guide for parents, teachers and counsellors (rev. ed.). David Fulton Publishers. [Google Scholar]
- Niles, A. N., & Craske, M. G. (2019). Incidental emotion regulation deficits in public speaking anxiety. Cognitive Therapy and Research, 43, 419–426. [Google Scholar] [CrossRef]
- Paulus, F. W., Ohmann, S., Möhler, E., Plener, P., & Popow, C. (2021). Emotional dysregulation in children and adolescents with psychiatric disorders. A narrative review. Frontiers in Psychiatry, 12, 628252. [Google Scholar] [CrossRef]
- Pertaub, D. P., Slater, M., & Barker, C. (2002). An experiment on public speaking anxiety in response to three different types of virtual audience. Presence, 11(1), 68–78. [Google Scholar] [CrossRef]
- Philips, K. F. V., & Power, M. J. (2007). A new selfreport measure of emotion regulation in adolescents: The Regulation of Emotions Questionnaire. Clinical Psychology and Psychotherapy, 14, 145–156. [Google Scholar] [CrossRef]
- Predatu, R., David, D. O., & Maffei, A. (2020). The effects of irrational, rational, and acceptance beliefs about emotions on the emotional response and perceived control of emotions. Personality and Individual Differences, 155, 109712. [Google Scholar] [CrossRef]
- Rice, F., Davidovich, S., & Dunsmuir, S. (2017). Emotion regulation and depression: Maintaining equilibrium between positive and negative affect. In C. A. Essau, S. Leblanc, & T. H. Ollendick (Eds.), Emotion regulation and psychopathology in children and adolescents (pp. 171–195). Oxford University Press. [Google Scholar]
- Roiser, J. P., Elliott, R., & Sahakian, B. J. (2012). Cognitive mechanisms of treatment in depression. Neuropsychopharmacology, 37(1), 117–136. [Google Scholar] [CrossRef]
- Rutter, M., Pickles, A., Murray, R., & Eaves, L. (2001). Testing hypotheses on specific environmental causal effects on behavior. Psychological Bulletin, 127(3), 291–324. [Google Scholar] [CrossRef]
- Sackl-Pammer, P., Jahn, R., Özlü-Erkilic, Z., Pollak, E., Ohmann, S., Schwarzenberg, J., Plener, P., & Akkaya-Kalayci, T. (2019). Social anxiety disorder and emotion regulation problems in adolescents. Child and Adolescent Psychiatry and Mental Health, 13, 37. [Google Scholar] [CrossRef] [PubMed]
- Santrock, J. W. (1987). Adolescence: An introduction. Wm C Brown Publishers. [Google Scholar]
- Schoemann, A. M., Boulton, A. J., & Short, S. D. (2017). Determining power and sample size for simple and complex mediation models. Social Psychological and Personality Science, 8(4), 379–386. [Google Scholar] [CrossRef]
- Schweizer, S., Gotlib, I. H., & Blakemore, S. J. (2020). The role of affective control in emotion regulation during adolescence. Emotion, 20(1), 80. [Google Scholar] [CrossRef] [PubMed]
- Sevim, O. (2012). Öğretmen adaylarına yönelik Konuşma Kaygısı Ölçeği: Bir geçerlik ve güvenirlik çalışması. Electronic Turkish Studies, 7(2), 927–936. [Google Scholar]
- Smetana, J. G., Campione-Barr, N., & Metzger, A. (2006). Adolescent development in interpersonal and societal contexts. Annual Review of Psychology, 57, 255–284. [Google Scholar] [CrossRef] [PubMed]
- Stein, M. B., Walker, J. R., & Forde, D. R. (1996). Public speaking fears in a community sample: Prevalence, impact on functioning, and diagnostic classification. Archives of General Psychiatry, 53, 169–174. [Google Scholar] [CrossRef]
- Steinberg, L., & Morris, A. S. (2001). Adolescent development. Annual Review of Psychology, 52(1), 83–110. [Google Scholar] [CrossRef]
- Sypher, H. E. (1980). Illusory correlation in communication research. Human Communication Research, 7, 83–87. [Google Scholar] [CrossRef]
- Şahan, B., & Kahtali, B. D. (2021). The role of parental attıtudes, irrational beliefs, need for social approval and self-esteem in speech anxiety. European Journal of Alternative Education Studies, 6(1), 96–115. [Google Scholar] [CrossRef]
- Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Allyn & Bacon/Pearson Education. [Google Scholar]
- Thompson, R. A. (1994). Emotion regulation: A theme in search of definition. Monographs of the Society for Research in Child Development, 59(2/3), 25–52. [Google Scholar] [CrossRef]
- Tovilović, S. (2004). Latent structure of the social anxiety scale and relations between social anxiety and irrational beliefs. Psihologija, 37(1), 63–88. Available online: https://scindeks.ceon.rs/article.aspx?artid=0048-57050401063T (accessed on 3 January 2025.). [CrossRef]
- Trincas, R., Bilotta, E., & Mancini, F. (2016). Specific beliefs about emotions are associated with different emotion-regulation strategies. Psychology, 7, 1682–1699. [Google Scholar] [CrossRef]
- Türküm, A. S. (2003). Akılcı Olmayan İnanç Ölçeğinin geliştirilmesi ve kısaltma çalışmaları. Türk Psikolojik Danışma ve Rehberlik Dergisi. Cilt II 19, 41–47. [Google Scholar]
- Türküm, A. S., Balkaya, A., & ve Karaca, E. (2005). Akılcı Olmayan İnanç Ölçeğinin lise öğrencilerine uyarlanması: Geçerlik ve güvenirlik çalışmaları. Türk Psikolojik Danışma ve Rehberlik Dergisi, 3(23), 77–85. [Google Scholar]
- Urbán, D. J., García-Fernández, J. M., & Inglés, C. J. (2024). Risk profiles of social anxiety for interpersonal difficulties in a sample of Spanish adolescents. Revista de Psicodidáctica, 29(1), 9–18. [Google Scholar] [CrossRef]
- Urfa, O., & Aşçı, F. H. (2023). The direct and indirect effects of irrational beliefs on perceived performance: The mediation role of emotions and automatic thoughts. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 41(2), 432–453. [Google Scholar] [CrossRef]
- Vacca, M., Cerolini, S., Zegretti, A., Zagaria, A., & Lombardo, C. (2023). Bullying victimization and adolescent depression, anxiety and stress: The mediation of cognitive emotion regulation. Children, 10(12), 1897. [Google Scholar] [CrossRef]
- Viner, R. M., Ross, D., Hardy, R., Kuh, D., Power, C., Johnson, A., Wellings, K., McCambridge, J., Cole, T. J., Kelly, Y., & Batty, G. D. (2015). Life course epidemiology: Recognising the importance of adolescence. Journal of Epidemiology and Community Health, 69(8), 719–720. [Google Scholar] [CrossRef] [PubMed]
- Yaman, H., & Sofu, M. S. (2014). Öğretmen adaylarına yönelik Konuşma Kaygısı Ölçeğinin geliştirilmesi. Türkiye Sosyal Araştırmalar Dergisi, 173, 41–50. [Google Scholar]
- Yıldız, M. A., Baytemir, K., & Demirtaş, A. S. (2018). Irrational beliefs and perceived stress in adolescents: The role of self-esteem. Journal of Educational Sciences & Psychology, 1(8), 79–89. [Google Scholar]
- Young, K. S., Sandman, C. F., & Craske, M. G. (2019). Positive and negative emotion regulation in adolescence: Links to anxiety and depression. Brain Sciences, 9(4), 76. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Last Item No | First Item No | Factor Loadings | Item Total Test Correlation |
|---|---|---|---|
| 1 | 2 | 0.610 | 0.758 |
| 2 | 5 | 0.640 | 0.774 |
| 3 | 7 | 0.665 | 0.698 |
| 4 | 8 | 0.643 | 0.682 |
| 5 | 9 | 0.599 | 0.774 |
| 6 | 11 | 0.732 | 0.750 |
| 7 | 14 | 0.689 | 0.678 |
| 8 | 16 | 0.664 | 0.779 |
| 9 | 17 | 0.599 | 0.626 |
| 10 | 18 | 0.767 | 0.776 |
| 11 | 20 | 0.510 | 0.702 |
| 12 | 21 | 0.696 | 0.601 |
| 13 | 22 | 0.612 | 0.713 |
| 14 | 23 | 0.614 | 0.725 |
| 15 | 24 | 0.644 | 0.733 |
| 16 | 27 | 0.722 | 0.803 |
| 17 | 28 | 0.517 | 0.704 |
| 18 | 29 | 0.683 | 0.795 |
| Eigenvalue | 11.686 | ||
| Variance explained | 64.922 | ||
| Number of Items | Cronbach’s Alpha | Guttman Split-Half | McDonald’s Omega-ω | |
|---|---|---|---|---|
| PSAS | 18 | 0.957 | 0.964 | 0.957 |
| Variables | 1 | 2 | 3 | 4 | Tol | VIF |
|---|---|---|---|---|---|---|
| 1-Public speaking anxiety | 1 | |||||
| 2-Irrational beliefs | 0.42 ** | 1 | 0.783 | 1.277 | ||
| 3-Regulation of internal dysfunctional emotions | 0.46 ** | 0.51 ** | 1 | 0.748 | 1.336 | |
| 4-Regulation of external dysfunctional emotions | 0.19 ** | 0.07 * | 0.28 ** | 1 | 0.916 | 1.092 |
| α | 0.96 | 0.82 | 0.86 | 0.76 | ||
| Skewness | 0.242 | −0.219 | 0.181 | 1.341 | ||
| Kurtosis | −0.926 | −0.424 | −0.607 | 1.936 | ||
| Average | 54.73 | 55.99 | 13.70 | 10.01 | ||
| Sd. | 20.72 | 10.82 | 4.59 | 4.25 |
| Types | Total Effect (% 95 CI) | Direct Effects (% 95 CI) | Indirect Effect (% 95 CI) | Decision | ||
|---|---|---|---|---|---|---|
| Irrational Beliefs | → | Public Speaking Anxiety | −0.43 ** (0.32 **, 0.54 **) | 0.25 ** (0.22 **, 0.42 *) | −0.17 ** (0.13 **, 0.21 **) | Partial Mediation |
| Irrational Beliefs | → | Regulation of Internal Dysfunctional Emotions | 0.42 ** (0.52 **, 0.36 **) | |||
| Regulation of Internal Dysfunctional Emotions | → | Public Speaking Anxiety | 0.40 ** (0.30 **, 0.52 **) | |||
| Irrational Beliefs | → | Regulation of External Dysfunctional Emotions | 0.19 ** (0.32 **, 0.06 **) | No intermediation was observed. | ||
| Regulation of External Dysfunctional Emotions | → | Irrational Beliefs | 0.09 (p; 0.168 > 0.01) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demir, S.; Kan, M.O. Developing the Public Speaking Anxiety Scale (PSAS) for Adolescents: The Mediating Role of Dysfunctional Emotion Regulation in the Effect of Irrational Beliefs on Public Speaking Anxiety. Behav. Sci. 2025, 15, 825. https://doi.org/10.3390/bs15060825
Demir S, Kan MO. Developing the Public Speaking Anxiety Scale (PSAS) for Adolescents: The Mediating Role of Dysfunctional Emotion Regulation in the Effect of Irrational Beliefs on Public Speaking Anxiety. Behavioral Sciences. 2025; 15(6):825. https://doi.org/10.3390/bs15060825
Chicago/Turabian StyleDemir, Sezai, and Mustafa Onur Kan. 2025. "Developing the Public Speaking Anxiety Scale (PSAS) for Adolescents: The Mediating Role of Dysfunctional Emotion Regulation in the Effect of Irrational Beliefs on Public Speaking Anxiety" Behavioral Sciences 15, no. 6: 825. https://doi.org/10.3390/bs15060825
APA StyleDemir, S., & Kan, M. O. (2025). Developing the Public Speaking Anxiety Scale (PSAS) for Adolescents: The Mediating Role of Dysfunctional Emotion Regulation in the Effect of Irrational Beliefs on Public Speaking Anxiety. Behavioral Sciences, 15(6), 825. https://doi.org/10.3390/bs15060825