
The Influence of UI Design Attributes and Users’ Uncertainty Avoidance on Stickiness of the Young Elderly Toward mHealth Applications


Abstract
1. Introduction
- RQ1: How significantly do the UI design attributes of mHealth applications influence the stickiness of young elderly users?
- RQ2: Does the level of uncertainty avoidance influence the stickiness of young elderly users to mHealth applications?
- RQ3: In mHealth applications, do UI design attributes and uncertainty avoidance indirectly influence the stickiness of young elderly users through psychological engagement and internal experiences?
2. Theoretical Background and Research Hypotheses
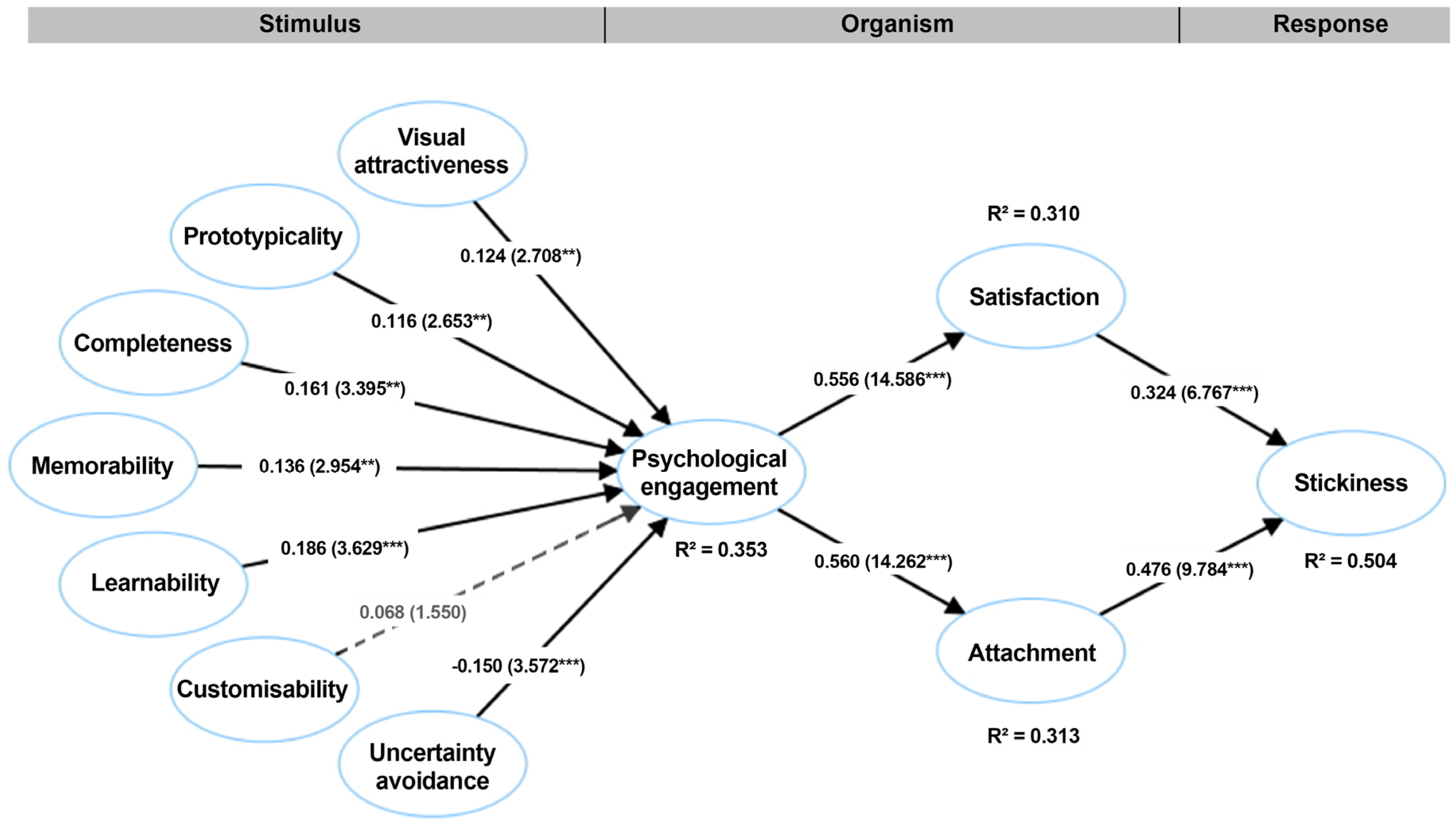
2.1. Stimulus–Organism–Response (S-O-R) Theory
2.2. Stimuli: UI Design Attributes and Uncertainty Avoidance
2.2.1. UI Aesthetic Attributes: Visual Attractiveness and Prototypicality
2.2.2. UI Usability Attributes: Completeness, Memorability, Learnability, and Customizability
2.2.3. Uncertainty Avoidance
2.3. Organism: Psychological Engagement and Internal Experience
2.4. Response: Stickiness
3. Methods
3.1. Sampling and Data Collection
3.2. Measurement
3.3. Preliminary Quality and Common Method Bias Checks
4. Data Analysis and Results
4.1. Measurement Model Assessment
4.2. Structural Model Assessment
4.2.1. Model Fit
4.2.2. Hypothesis Test Results
5. Discussion
5.1. Theoretical Implications
5.2. Practical Implications
- (1)
- Progressive disclosure: We recommend that developers of mHealth applications do not display all functionalities at once but gradually introduce more features based on the progress of elderly users to avoid information overload, leading to lower learnability and memorability.
- (2)
- Consistency within the interfaces of mHealth applications should be maintained, including the use of colors, fonts, layouts, and interactive elements, which helps elderly users learn and adapt to the application more quickly.
5.3. Limitations and Future Research Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Concept | Definition | Source |
|---|---|---|
| Completeness | The system can assist users in successfully completing tasks. This is usually measured objectively by system log files for the completion rate. | Brown et al. (2013, p. 1083) |
| Memorability | Users can easily remember how to perform tasks through the system. | |
| Learnability | Users are able to easily learn how to operate the system. | |
| Customizability | The system provides more than one way to accomplish tasks, which allows users to operate the system as preferred. |
Appendix B
| Construct | Measurement Items | Literature |
|---|---|---|
| Visual attractiveness (VA) | VA1: The user interface design of mobile health apps looks clean. | Fang et al. (2017) |
| VA2: The user interface design of mobile health apps is sophisticated. | ||
| VA3: The user interface design of mobile health apps is fascinating. | ||
| VA4: The user interface design of mobile health apps is aesthetically pleasing. | ||
| VA5: The user interface design of mobile health apps is visually appealing. | ||
| VA6: The interface layout of mobile health apps is attractive. | ||
| Prototypicality (PT) | PT1: This user interface looks very typical. | Miniukovich and Figl (2023); S. Lee et al. (2011) |
| PT2: This user interface looks very exemplary. | ||
| PT3: Compared to other existing user interfaces, it meets my general expectations for a mobile health app user interface. | ||
| Completeness (COM) | COM1: Provides me with complete information related to task management. | Tandon et al. (2024) |
| COM2: Adequate user support helps me to complete my tasks easily. | ||
| COM3: Timely notifications provided by mHealth app UI update me about my health status. | ||
| COM4: Comprehensive notifications provided by mHealth app UI update me about my health status. | ||
| Memorability (MEM) | MEM1: I can easily remember how to perform tasks using this UI. | Tandon et al. (2024) |
| MEM2: The messages provided by this UI are easy to memorize. | ||
| MEM3: It can help me recall important health information whenever I go to the doctor, such as tasks or details, that I might otherwise forget. | ||
| Learnability (LRN) | LRN1: I can easily learn how to use this user interface. | Tandon et al. (2024) |
| LRN2: The mobile health user interface is easy to operate. | ||
| LRN3: I am able to manage my health check-ups using this UI. | ||
| LRN4: It is easy to become proficient in using this user interface and its features. | ||
| Customizability (CTM) | CTM1: The user interface offers multiple methods to perform tasks. | Tandon et al. (2024) |
| CTM2: I can always log on and use the app by using multiple tabs. | ||
| CTM3: It allows me to generate reports about my health issues through multiple means. | ||
| CTM4: Navigational structure is simple, and related information is placed together. | ||
| Uncertainty avoidance (UA) | UA1: When starting a new job, I fear doing it. | Yoon (2009) |
| UA2: I fear uncertainty about the future. | ||
| UA3: I fear ambiguous situations and unfamiliar adventures. | ||
| UA4: It is risky to do something that has never been done before. | ||
| Psychological engagement (PEN) | PEN1: I feel strong and vigorous when I use mobile health apps. | Elsotouhy et al. (2024) |
| PEN2: I am enthusiastic about using mobile health apps. | ||
| PEN3: Using mobile health apps is absorbing and immersive. | ||
| Satisfaction (SAT) | STA1: I feel satisfied with using mobile health apps. | Elsotouhy et al. (2024) |
| STA2: I feel content with using mobile health apps. | ||
| STA3: I feel pleased with using mobile health apps. | ||
| STA4: I am delighted with my overall experience of using mobile health apps. | ||
| Attachment (ATT) | ATT1: I have a personal bond with mobile health apps. | Pedeliento et al. (2016) |
| ATT2: Mobile health apps have a special role in my life. | ||
| ATT3: Mobile health apps are very dear to me. | ||
| ATT4: Mobile health apps mean a lot to me. | ||
| ATT5: I am very attached to mobile health apps. | ||
| ATT6: I feel emotionally connected to mobile health apps. | ||
| Stickiness (ST) | SI1: I would stay for a long time while browsing mobile health apps. | M. Zhang et al. (2017) |
| SI2: I intend to prolong my stays on mobile health apps. | ||
| SI3: I would visit this app frequently. |
References
- Alam, M. Z., Hu, W., & Barua, Z. (2018). Using the UTAUT model to determine factors affecting acceptance and use of mobile health (mHealth) services in Bangladesh. Journal of Studies in Social Sciences, 17(2), 137–172. [Google Scholar]
- Alexander, R., Thompson, N., McGill, T., & Murray, D. (2021). The influence of user culture on website usability. International Journal of Human-Computer Studies, 154, 102688. [Google Scholar] [CrossRef]
- Ali, F., Terrah, A., Wu, C., Ali, L., & Wu, H. (2021). Antecedents and consequences of user engagement in smartphone travel apps. Journal of Hospitality and Tourism Technology, 12(2), 355–371. [Google Scholar] [CrossRef]
- Alipour, M., Dupuy-Chessa, S., & Céret, E. (2021, September 28–October 1). An emotion-oriented problem space for ui adaptation: From a literature review to a conceptual framework. 2021 9th International Conference on Affective Computing and Intelligent Interaction (ACII) (pp. 1–8), Nara, Japan. [Google Scholar]
- Al-Okaily, M., Lutfi, A., Alsaad, A., Taamneh, A., & Alsyouf, A. (2020). The determinants of digital payment systems’ acceptance under cultural orientation differences: The case of uncertainty avoidance. Technology in Society, 63, 101367. [Google Scholar] [CrossRef]
- Anderson, J. C., & Gerbing, D. W. (1988). Structural equation modeling in practice: A review and recommended two-step approach. Psychological Bulletin, 103(3), 411. [Google Scholar] [CrossRef]
- Ben Haobin, Y., Huiyue, Y., Peng, L., & Fong, L. H. N. (2021). The impact of hotel servicescape on customer mindfulness and brand experience: The moderating role of length of stay. Journal of Hospitality Marketing & Management, 30(5), 592–610. [Google Scholar]
- Beratarrechea, A., Lee, A. G., Willner, J. M., Jahangir, E., Ciapponi, A., & Rubinstein, A. (2014). The impact of mobile health interventions on chronic disease outcomes in developing countries: A systematic review. Telemedicine and e-Health, 20(1), 75–82. [Google Scholar] [CrossRef]
- Birkmeyer, S., Wirtz, B. W., & Langer, P. F. (2021). Determinants of mHealth success: An empirical investigation of the user perspective. International Journal of Information Management, 59, 102351. [Google Scholar] [CrossRef]
- Bonnardel, N., Piolat, A., & Le Bigot, L. (2011). The impact of colour on Website appeal and users’ cognitive processes. Displays, 32(2), 69–80. [Google Scholar] [CrossRef]
- Bowlby, J., & Bowlby, R. (2012). The making and breaking of affectional bonds. Routledge. [Google Scholar]
- Brown, W., III, Yen, P. Y., Rojas, M., & Schnall, R. (2013). Assessment of the Health IT Usability Evaluation Model (Health-ITUEM) for evaluating mobile health (mHealth) technology. Journal of Biomedical Informatics, 46(6), 1080–1087. [Google Scholar] [CrossRef]
- Bruce, H. (1998). User satisfaction with information seeking on the Internet. Journal of the American Society for Information Science, 49(6), 541–556. [Google Scholar] [CrossRef]
- Calvo-Porral, C., Faíña-Medín, A., & Nieto-Mengotti, M. (2017). Exploring technology satisfaction: An approach through the flow experience. Computers in Human Behavior, 66, 400–408. [Google Scholar] [CrossRef]
- Cao, Y., Qin, X., Li, J., Long, Q., & Hu, B. (2022). Exploring seniors’ continuance intention to use mobile social network sites in China: A cognitive-affective-conative model. Universal Access in the Information Society, 21, 71–92. [Google Scholar] [CrossRef]
- Carroll, B. A., & Ahuvia, A. C. (2006). Some antecedents and outcomes of brand love. Marketing Letters, 17, 79–89. [Google Scholar] [CrossRef]
- Celhay, F., & Trinquecoste, J. F. (2015). Package graphic design: Investigating the variables that moderate consumer response to atypical designs. Journal of Product Innovation Management, 32(6), 1014–1032. [Google Scholar] [CrossRef]
- Chang, H. J., Eckman, M., & Yan, R. N. (2011). Application of the Stimulus-Organism-Response model to the retail environment: The role of hedonic motivation in impulse buying behavior. The International Review of Retail, Distribution and Consumer Research, 21(3), 233–249. [Google Scholar] [CrossRef]
- Changizi, M., & Kaveh, M. H. (2017). Effectiveness of the mHealth technology in improvement of healthy behaviors in an elderly population—A systematic review. mHealth, 3, 51. [Google Scholar] [CrossRef]
- Chea, S., & Luo, M. M. (2008). Post-adoption behaviors of e-service customers: The interplay of cognition and emotion. International Journal of Electronic Commerce, 12(3), 29–56. [Google Scholar] [CrossRef]
- Chen, G., So, K. K. F., Hu, X., & Poomchaisuwan, M. (2022). Travel for affection: A stimulus-organism-response model of honeymoon tourism experiences. Journal of Hospitality & Tourism Research, 46(6), 1187–1219. [Google Scholar]
- Cheung, C. M., Shen, X. L., Lee, Z. W., & Chan, T. K. (2015). Promoting sales of online games through customer engagement. Electronic Commerce Research and Applications, 14(4), 241–250. [Google Scholar] [CrossRef]
- Chi, O. H., Chi, C. G., Gursoy, D., & Nunkoo, R. (2023). Customers’ acceptance of artificially intelligent service robots: The influence of trust and culture. International Journal of Information Management, 70, 102623. [Google Scholar] [CrossRef]
- Chin, W. W. (1998a). Commentary: Issues and opinion on structural equation modeling. MIS Quarterly, 22(1), vii–xvi. [Google Scholar]
- Chin, W. W. (1998b). The partial least squares approach to structural equation modeling. Modern Methods for Business Research, 295(2), 295–336. [Google Scholar]
- Cho, J. (2016). The impact of post-adoption beliefs on the continued use of health apps. International Journal of Medical Informatics, 87, 75–83. [Google Scholar] [CrossRef]
- Choi, H., & Kandampully, J. (2019). The effect of atmosphere on customer engagement in upscale hotels: An application of SOR paradigm. International Journal of Hospitality Management, 77, 40–50. [Google Scholar] [CrossRef]
- Chopdar, P. K., & Balakrishnan, J. (2020). Consumers response towards mobile commerce applications: SOR approach. International Journal of Information Management, 53, 102106. [Google Scholar] [CrossRef]
- Clemmensen, T., Shi, Q., Kumar, J., Li, H., Sun, X., & Yammiyavar, P. (2007). Cultural usability tests–How usability tests are not the same all over the world. In Usability and internationalization. HCI and Culture: Second international conference on usability and internationalization, UI-HCII 2007, held as part of HCI international 2007, Beijing, China, July 22–27, 2007, Proceedings, Part I 2 (pp. 281–290). Springer. [Google Scholar]
- Coursaris, C. K., & Van Osch, W. (2016). A Cognitive-Affective Model of Perceived User Satisfaction (CAMPUS): The complementary effects and interdependence of usability and aesthetics in IS design. Information & Management, 53(2), 252–264. [Google Scholar]
- Deka, P., Salahshurian, E., Ng, T., Buchholz, S. W., Klompstra, L., & Alonso, W. (2025). Use of mHealth technology for improving exercise adherence in patients with heart failure: Systematic review. Journal of Medical Internet Research, 27, e54524. [Google Scholar] [CrossRef]
- Deng, Z., Hong, Z., Ren, C., Zhang, W., & Xiang, F. (2018). What predicts patients’ adoption intention toward mHealth services in China: Empirical study. JMIR mHealth and uHealth, 6(8), e9316. [Google Scholar] [CrossRef]
- DIS, I. (2009). Ergonomics of human system interaction-Part 210: Human-centred design for interactive systems (ISO 9241-210:2010). International Standardization Organization (ISO). 2. [Google Scholar]
- Duarte, P., & Pinho, J. C. (2019). A mixed methods UTAUT2-based approach to assess mobile health adoption. Journal of Business Research, 102, 140–150. [Google Scholar] [CrossRef]
- Elguera Paez, L., & Zapata Del Río, C. (2019). Elderly users and their main challenges usability with mobile applications: A systematic review. In Design, user experience, and usability. Design philosophy and theory: 8th international conference, DUXU 2019, held as part of the 21st HCI international conference, HCII 2019, Orlando, FL, USA, July 26–31, 2019, Proceedings, Part I 21 (pp. 423–438). Springer International Publishing. [Google Scholar]
- Elsotouhy, M. M., Ghonim, M. A., Alasker, T. H., & Khashan, M. A. (2024). Investigating health and fitness app users’ stickiness, WOM, and continuance intention using SOR model: The moderating role of health consciousness. International Journal of Human–Computer Interaction, 40(5), 1235–1250. [Google Scholar] [CrossRef]
- Faisal, C. N., Gonzalez-Rodriguez, M., Fernandez-Lanvin, D., & de Andres-Suarez, J. (2016). Web design attributes in building user trust, satisfaction, and loyalty for a high uncertainty avoidance culture. IEEE Transactions on Human-Machine Systems, 47(6), 847–859. [Google Scholar] [CrossRef]
- Fang, J., Zhao, Z., Wen, C., & Wang, R. (2017). Design and performance attributes driving mobile travel application engagement. International Journal of Information Management, 37(4), 269–283. [Google Scholar] [CrossRef]
- Fornell, C., & Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research, 18(1), 39–50. [Google Scholar] [CrossRef]
- Free, C., Phillips, G., Galli, L., Watson, L., Felix, L., Edwards, P., Patel, V., & Haines, A. (2013). The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: A systematic review. PLoS Medicine, 10(1), e1001362. [Google Scholar] [CrossRef]
- Gao, X., Yee, C. L., & Choo, W. C. (2022). How attachment and community identification affect user stickiness in social commerce: A consumer engagement experience perspective. Sustainability, 14(20), 13633. [Google Scholar] [CrossRef]
- Gu, J. C., Lee, S. C., & Suh, Y. H. (2009). Determinants of behavioral intention to mobile banking. Expert Systems with Applications, 36(9), 11605–11616. [Google Scholar] [CrossRef]
- Guo, X., Chen, S., Zhang, X., Ju, X., & Wang, X. (2020). Exploring patients’ intentions for continuous usage of mHealth services: Elaboration-likelihood perspective study. JMIR mHealth and uHealth, 8(4), e17258. [Google Scholar] [CrossRef]
- Guru, R. R. D., Paulssen, M., & Japutra, A. (2024). Role of brand attachment and satisfaction in driving customer behaviors for durables: A longitudinal study. European Journal of Marketing, 58(1), 217–254. [Google Scholar] [CrossRef]
- Hage, P., & Miller, W. R. (1976). ‘eagle’=‘bird’: A note on the structure and evolution of Shoshoni ethnoornithological nomenclature. American Ethnologist, 3(3), 481–488. [Google Scholar] [CrossRef]
- Hair, J. F., Risher, J. J., Sarstedt, M., & Ringle, C. M. (2019). When to use and how to report the results of PLS-SEM. European Business Review, 31(1), 2–24. [Google Scholar] [CrossRef]
- Harman, H. H. (1976). Modern factor analysis. University of Chicago Press. [Google Scholar]
- Henseler, J., Ringle, C. M., & Sarstedt, M. (2015). A new criterion for assessing discriminant validity in variance-based structural equation modeling. Journal of the Academy of Marketing Science, 43, 115–135. [Google Scholar] [CrossRef]
- Higgins, E. T. (2006). Value from hedonic experience and engagement. Psychological Review, 113(3), 439–460. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J. P. (2016). Smartphone applications for patients’ health and fitness. The American Journal of Medicine, 129(1), 11–19. [Google Scholar] [CrossRef]
- Hoehle, H., Zhang, X., & Venkatesh, V. (2015). An espoused cultural perspective to understand continued intention to use mobile applications: A four-country study of mobile social media application usability. European Journal of Information Systems, 24(3), 337–359. [Google Scholar] [CrossRef]
- Hofstede, G., Hofstede, G. J., & Minkov, M. (2010). Cultures et organisations: Nos programmations mentales. Pearson Education France. [Google Scholar]
- Hsu, C. L., & Lin, J. C. C. (2016). Effect of perceived value and social influences on mobile app stickiness and in-app purchase intention. Technological Forecasting and Social Change, 108, 42–53. [Google Scholar] [CrossRef]
- Jacques, R. (1995). Engagement as a design concept for multimedia. Canadian Journal of Educational Communication, 24(1), 49–59. [Google Scholar] [CrossRef]
- Jung, W., & Yim, H. (2017). An empirical study on the relationship between user interface design attributes in smartphone applications and intention to use. In Advanced multimedia and ubiquitous engineering: MUE/FutureTech 2017 (pp. 81–84). Springer. [Google Scholar]
- Kim, H., Park, E., Lee, S., Kim, M., Park, E. J., & Hong, S. (2018). Self-management of chronic diseases among older Korean adults: An mHealth training, protocol, and feasibility study. JMIR mHealth and uHealth, 6(6), e9988. [Google Scholar] [CrossRef]
- Kim, S., Baek, T. H., Kim, Y. K., & Yoo, K. (2016). Factors affecting stickiness and word of mouth in mobile applications. Journal of Research in Interactive Marketing, 10(3), 177–192. [Google Scholar] [CrossRef]
- Kim, Y. H., Kim, D. J., & Wachter, K. (2013). A study of mobile user engagement (MoEN): Engagement motivations, perceived value, satisfaction, and continued engagement intention. Decision Support Systems, 56, 361–370. [Google Scholar] [CrossRef]
- Kirkman, B. L., Lowe, K. B., & Gibson, C. B. (2006). A quarter century of culture’s consequences: A review of empirical research incorporating Hofstede’s cultural values framework. Journal of International Business Studies, 37, 285–320. [Google Scholar] [CrossRef]
- Klasnja, P., & Pratt, W. (2012). Healthcare in the pocket: Mapping the space of mobile-phone health interventions. Journal of Biomedical Informatics, 45(1), 184–198. [Google Scholar] [CrossRef] [PubMed]
- Klaver, N. S., Van de Klundert, J., & Askari, M. (2021). Relationship between perceived risks of using mHealth applications and the intention to use them among older adults in the Netherlands: Cross-sectional study. JMIR mHealth and uHealth, 9(8), e26845. [Google Scholar] [CrossRef]
- Kumar, S., Dhir, A., Talwar, S., Chakraborty, D., & Kaur, P. (2021). What drives brand love for natural products? The moderating role of household size. Journal of Retailing and Consumer Services, 58, 102329. [Google Scholar] [CrossRef]
- Kumaran, R., Doshi, V. N., Chen, S. X., Nargund, A. A., Höllerer, T., & Sra, M. (2023, October 29–November 1). EChat: An emotion-aware adaptive UI for a messaging app. Adjunct Proceedings of the 36th Annual ACM Symposium on User Interface Software and Technology (pp. 1–3), San Francisco, CA, USA. [Google Scholar]
- Kühn, S. W., & Petzer, D. J. (2018). Fostering purchase intentions toward online retailer websites in an emerging market: An SOR perspective. Journal of Internet Commerce, 17(3), 255–282. [Google Scholar] [CrossRef]
- Lee, C. H., Chiang, H. S., & Hsiao, K. L. (2018). What drives stickiness in location-based AR games? An examination of flow and satisfaction. Telematics and Informatics, 35(7), 1958–1970. [Google Scholar] [CrossRef]
- Lee, S., Ha, S., & Widdows, R. (2011). Consumer responses to high-technology products: Product attributes, cognition, and emotions. Journal of Business Research, 64(11), 1195–1200. [Google Scholar] [CrossRef]
- Leung, L., & Chen, C. (2019). E-health/m-health adoption and lifestyle improvements: Exploring the roles of technology readiness, the expectation-confirmation model, and health-related information activities. Telecommunications Policy, 43(6), 563–575. [Google Scholar] [CrossRef]
- Li, D., Browne, G. J., & Wetherbe, J. C. (2006). Why do internet users stick with a specific web site? A relationship perspective. International Journal of Electronic Commerce, 10(4), 105–141. [Google Scholar] [CrossRef]
- Li, J., Zhang, C., Li, X., & Zhang, C. (2020). Patients’ emotional bonding with mHealth apps: An attachment perspective on patients’ use of mHealth applications. International Journal of Information Management, 51, 102054. [Google Scholar] [CrossRef]
- Li, L., & Kang, K. (2024). Effect of the social and cultural control on young eastern ethnic minority groups’ online-startup motivation. Entrepreneurship Research Journal, 14(2), 491–514. [Google Scholar] [CrossRef]
- Li, Y., Li, X., & Cai, J. (2021). How attachment affects user stickiness on live streaming platforms: A socio-technical approach perspective. Journal of Retailing and Consumer Services, 60, 102478. [Google Scholar] [CrossRef]
- Lien, C. H., Cao, Y., & Zhou, X. (2017). Service quality, satisfaction, stickiness, and usage intentions: An exploratory evaluation in the context of WeChat services. Computers in Human Behavior, 68, 403–410. [Google Scholar] [CrossRef]
- Lin, J., Li, T., & Guo, J. (2021). Factors influencing consumers’ continuous purchase intention on fresh food e-commerce platforms: An organic foods-centric empirical investigation. Electronic Commerce Research and Applications, 50, 101103. [Google Scholar] [CrossRef]
- Lin, J. C. C. (2007). Online stickiness: Its antecedents and effect on purchasing intention. Behaviour & Information Technology, 26(6), 507–516. [Google Scholar]
- Lindgaard, G. (2007). Aesthetics, visual appeal, usability, and user satisfaction. Australian Journal of Emerging Technologies and Society, 5(1), 1–25. [Google Scholar]
- Liu, N., Yin, J., Tan, S. S. L., Ngiam, K. Y., & Teo, H. H. (2021). Mobile health applications for older adults: A systematic review of interface and persuasive feature design. Journal of the American Medical Informatics Association, 28(11), 2483–2501. [Google Scholar] [CrossRef]
- Liu, Y., & Zhang, Q. (2019). Interface design aesthetics of interaction design. In Design, user experience, and usability. Design philosophy and theory: 8th international conference, DUXU 2019, held as part of the 21st HCI international conference, HCII 2019, Orlando, FL, USA, July 26–31, 2019, Proceedings, Part I 21 (pp. 279–290). Springer International Publishing. [Google Scholar]
- Loureiro, S. M. C., Gorgus, T., & Kaufmann, H. R. (2017). Antecedents and outcomes of online brand engagement: The role of brand love on enhancing electronic-word-of-mouth. Online Information Review, 41(7), 985–1005. [Google Scholar] [CrossRef]
- Löckenhoff, C. E., De Fruyt, F., Terracciano, A., McCrae, R. R., De Bolle, M., Costa, P. T., Aguilar-Vafaie, M. E., Ahn, C.-K., Ahn, H.-N., Alcalay, L., Allik, J., Avdeyeva, T. V., Barbaranelli, C., Benet-Martínez, V., Blatný, M., Bratko, D., Cain, T. R., Crawford, J. T., Lima, M. P., … Yik, M. (2009). Perceptions of aging across 26 cultures and their culture-level associates. Psychology and Aging, 24(4), 941. [Google Scholar] [CrossRef]
- Madina, S., & Kim, H. C. (2021). Exploring the Structural Relationship among Beauty Influencers’ Attractiveness and Homophily, Emotional Attachment, and Live Commerce Stickiness. International Journal of Advanced Smart Convergence, 10(4), 149–157. [Google Scholar]
- Maqableh, M., Abuhashesh, M., Dahabiyeh, L., Nawayseh, M., & Masadeh, R. (2021). The effect of Facebook users’ satisfaction and trust on stickiness: The role of perceived values. International Journal of Data and Network Science, 5(3), 245–256. [Google Scholar] [CrossRef]
- Marchand, D. A., & Davenport, T. H. (2000). Mastering information management. Taylor & Francis. [Google Scholar]
- Masrek, M. N., Razali, M. H., Ramli, I., & Andromeda, T. (2018). User engagement and satisfaction: The case of web digital library. International Journal of Engineering and Technology (UAE), 7(4), 19–24. [Google Scholar]
- McLean, G. (2018). Examining the determinants and outcomes of mobile app engagement-A longitudinal perspective. Computers in Human Behavior, 84, 392–403. [Google Scholar] [CrossRef]
- Mehrabian, A., & Russell, J. A. (1974). An approach to environmental psychology. The MIT Press. [Google Scholar]
- Miniukovich, A., & Figl, K. (2023). The effect of prototypicality on webpage aesthetics, usability, and trustworthiness. International Journal of Human-Computer Studies, 179, 103103. [Google Scholar] [CrossRef]
- O’Brien, H. L., & Toms, E. G. (2008). What is user engagement? A conceptual framework for defining user engagement with technology. Journal of the American society for Information Science and Technology, 59(6), 938–955. [Google Scholar] [CrossRef]
- Odushegun, L. (2023). Aesthetic semantics: Affect rating of atomic visual web aesthetics for use in affective user experience design. International Journal of Human-Computer Studies, 171, 102978. [Google Scholar] [CrossRef]
- Oh, S. S., Kim, K. A., Kim, M., Oh, J., Chu, S. H., & Choi, J. (2021). Measurement of digital literacy among older adults: Systematic review. Journal of Medical Internet Research, 23(2), e26145. [Google Scholar] [CrossRef]
- Oliver, R. L. (1999). Whence consumer loyalty? Journal of Marketing, 63(4_suppl1), 33–44. [Google Scholar] [CrossRef]
- Pan, J., & Dong, H. (2023). mHealth adoption among older chinese adults: A conceptual model with design suggestions. International Journal of Human–Computer Interaction, 39(5), 1072–1083. [Google Scholar] [CrossRef]
- Papa, A., Mital, M., Pisano, P., & Del Giudice, M. (2020). E-health and wellbeing monitoring using smart healthcare devices: An empirical investigation. Technological Forecasting and Social Change, 153, 119226. [Google Scholar] [CrossRef]
- Parboteeah, D. V., Valacich, J. S., & Wells, J. D. (2009). The influence of website characteristics on a consumer’s urge to buy impulsively. Information Systems Research, 20(1), 60–78. [Google Scholar] [CrossRef]
- Pedeliento, G., Andreini, D., Bergamaschi, M., & Salo, J. (2016). Brand and product attachment in an industrial context: The effects on brand loyalty. Industrial Marketing Management, 53, 194–206. [Google Scholar] [CrossRef]
- Peters, T., Işık, Ö., Tona, O., & Popovič, A. (2016). How system quality influences mobile BI use: The mediating role of engagement. International Journal of Information Management, 36(5), 773–783. [Google Scholar] [CrossRef]
- Podsakoff, P. M., & Organ, D. W. (1986). Self-reports in organizational research: Problems and prospects. Journal of Management, 12(4), 531–544. [Google Scholar] [CrossRef]
- Rahardja, U., Sigalingging, C. T., Putra, P. O. H., Nizar Hidayanto, A., & Phusavat, K. (2023). The impact of mobile payment application design and performance attributes on consumer emotions and continuance intention. Sage Open, 13(1), 21582440231151919. [Google Scholar] [CrossRef]
- Rizzo, L., Brick, J. M., & Park, I. (2004). A minimally intrusive method for sampling persons in random digit dial surveys. Public Opinion Quarterly, 68(2), 267–274. [Google Scholar] [CrossRef]
- Salcedo, E., & Gupta, M. (2021). The effects of individual-level espoused national cultural values on the willingness to use Bitcoin-like blockchain currencies. International Journal of Information Management, 60, 102388. [Google Scholar] [CrossRef]
- Schaffer, S., Ruß, A., & Gustke, O. (2022, November). User Experience of a Conversational User Interface in a Museum. In International conference on ArtsIT, interactivity and game creation (pp. 215–223). Springer Nature. [Google Scholar]
- Shao, Z., Zhang, L., Chen, K., & Zhang, C. (2020). Examining user satisfaction and stickiness in social networking sites from a technology affordance lens: Uncovering the moderating effect of user experience. Industrial Management & Data Systems, 120(7), 1331–1360. [Google Scholar]
- Sharma, R., Singh, G., & Sharma, S. (2020). Modelling internet banking adoption in Fiji: A developing country perspective. International Journal of Information Management, 53, 102116. [Google Scholar] [CrossRef]
- Shen, L., Zhang, Y., Fan, Y., Chen, Y., & Zhao, Y. (2022). Improving consumer stickiness in livestream e-commerce: A mixed-methods study. Frontiers in Psychology, 13, 962786. [Google Scholar] [CrossRef]
- Shin, H., Oh, C., Kim, N. Y., Choi, H., Kim, B., & Ji, Y. G. (2024). Evaluating and eliciting design requirements for an improved user experience in live-streaming commerce interfaces. Computers in Human Behavior, 150, 107990. [Google Scholar] [CrossRef]
- Soni, M., Jain, K., & Jajodia, I. (2021). Mobile health (mHealth) application loyalty in young consumers. Young Consumers, 22(3), 429–455. [Google Scholar] [CrossRef]
- Srite, M., & Karahanna, E. (2006). The role of espoused national cultural values in technology acceptance. MIS Quarterly, 30(3), 679–704. [Google Scholar] [CrossRef]
- Statista. (2025). Digital health: Market & data analysis. Available online: https://www.statista.com/study/116507/digital-health-report-2023/ (accessed on 8 April 2025).
- Sun, J., Guo, Y., Wang, X., & Zeng, Q. (2016). mHealth for aging China: Opportunities and challenges. Aging and Disease, 7(1), 53–67. [Google Scholar] [CrossRef]
- Sun, X., Chen, Z., & Jiang, Q. (2024). An empirical study on the willingness of young elderly to use elderly companion robot. International Journal of Human–Computer Interaction, 41(7), 4015–4036. [Google Scholar] [CrossRef]
- Tajudeen, F. P., Bahar, N., Maw Pin, T., & Saedon, N. I. (2022). Mobile technologies and healthy ageing: A bibliometric analysis on publication trends and knowledge structure of mHealth research for older adults. International Journal of Human–Computer Interaction, 38(2), 118–130. [Google Scholar] [CrossRef]
- Tandon, U., Ertz, M., & Shashi. (2024). Continued intention of mHealth care applications among the elderly: An enabler and inhibitor perspective. International Journal of Human–Computer Interaction, 40(18), 5026–5041. [Google Scholar] [CrossRef]
- Tang, J., Abraham, C., Stamp, E., & Greaves, C. (2015). How can weight-loss app designers’ best engage and support users? A qualitative investigation. British Journal of Health Psychology, 20(1), 151–171. [Google Scholar] [CrossRef]
- Tarute, A., Nikou, S., & Gatautis, R. (2017). Mobile application driven consumer engagement. Telematics and Informatics, 34(4), 145–156. [Google Scholar] [CrossRef]
- Tenenhaus, M., Vinzi, V. E., Chatelin, Y. M., & Lauro, C. (2005). PLS path modeling. Computational Statistics & Data Analysis, 48(1), 159–205. [Google Scholar]
- Thomson, M., MacInnis, D. J., & Whan Park, C. (2005). The ties that bind: Measuring the strength of consumers’ emotional attachments to brands. Journal of Consumer Psychology, 15(1), 77–91. [Google Scholar] [CrossRef]
- Tian, Z., Shi, Z., & Cheng, Q. (2021). Examining the antecedents and consequences of mobile travel app engagement. PLoS ONE, 16(3), e0248460. [Google Scholar] [CrossRef]
- Tu, W. J., Zeng, X., & Liu, Q. (2022). Aging tsunami coming: The main finding from China’s seventh national population census. Aging Clinical and Experimental Research, 34(5), 1159–1163. [Google Scholar] [CrossRef]
- Veryzer, R. W., Jr., & Hutchinson, J. W. (1998). The influence of unity and prototypicality on aesthetic responses to new product designs. Journal of Consumer Research, 24(4), 374–394. [Google Scholar] [CrossRef]
- Wallace, S., Reid, A., Clinciu, D., & Kang, J. S. (2013). Culture and the importance of usability attributes. Information Technology & People, 26(1), 77–93. [Google Scholar]
- Wang, W. T., Wang, Y. S., & Liu, E. R. (2016). The stickiness intention of group-buying websites: The integration of the commitment–trust theory and e-commerce success model. Information & Management, 53(5), 625–642. [Google Scholar]
- Wei, X., Jung, S., & Choi, T. M. (2022). Share it or buy it? Exploring the effects of product brand attachment on commercial sharing services. Journal of Business Research, 153, 115–127. [Google Scholar] [CrossRef]
- Westland, J. C. (2010). Lower bounds on sample size in structural equation modeling. Electronic Commerce Research and Applications, 9(6), 476–487. [Google Scholar] [CrossRef]
- Wilson, J., Heinsch, M., Betts, D., Booth, D., & Kay-Lambkin, F. (2021). Barriers and facilitators to the use of e-health by older adults: A scoping review. BMC Public Health, 21, 1556. [Google Scholar] [CrossRef]
- World Health Organization. (2011). mHealth: New horizons for health through mobile technologies: Based on the findings of the second global survey on eHealth. World Health Organization. [Google Scholar]
- Wu, Z., Zhou, J. Y., Feng, X. D., Fang, Y. R., Li, Y. S., & Wu, D. G. (1997). Dictionary of population science. Southwest University of Finance and Economics Press. [Google Scholar]
- Xia, Y., Deng, Y., Tao, X., Zhang, S., & Wang, C. (2024). Digital art exhibitions and psychological well-being in Chinese Generation Z: An analysis based on the SOR framework. Humanities and Social Sciences Communications, 11(1), 266. [Google Scholar] [CrossRef]
- Yin, M., Tayyab, S. M. U., Xu, X. Y., Jia, S. W., & Wu, C. L. (2021). The investigation of mobile health stickiness: The role of social support in a sustainable health approach. Sustainability, 13(4), 1693. [Google Scholar] [CrossRef]
- Yoo, B., Donthu, N., & Lenartowicz, T. (2011). Measuring Hofstede’s five dimensions of cultural values at the individual level: Development and validation of CVSCALE. Journal of International Consumer Marketing, 23(3–4), 193–210. [Google Scholar]
- Yoon, C. (2009). The effects of national culture values on consumer acceptance of e-commerce: Online shoppers in China. Information & Management, 46(5), 294–301. [Google Scholar]
- Zen, M., & Vanderdonckt, J. (2014, May 28–30). Towards an evaluation of graphical user interfaces aesthetics based on metrics. 2014 IEEE Eighth International Conference on Research Challenges in Information Science (RCIS) (pp. 1–12), Marrakesh, Morocco. [Google Scholar]
- Zhang, M., Guo, L., Hu, M., & Liu, W. (2017). Influence of customer engagement with company social networks on stickiness: Mediating effect of customer value creation. International Journal of Information Management, 37(3), 229–240. [Google Scholar] [CrossRef]
- Zhang, X. F., Guo, X., Ho, S. Y., Lai, K. H., & Vogel, D. (2021). Effects of emotional attachment on mobile health-monitoring service usage: An affect transfer perspective. Information & Management, 58(2), 103312. [Google Scholar]
- Zott, C., Amit, R., & Donlevy, J. (2000). Strategies for value creation in e-commerce:: Best practice in Europe. European Management Journal, 18(5), 463–475. [Google Scholar] [CrossRef]

| Socio-Demographic Variable | Frequency | Percentage (%) |
|---|---|---|
| Age | ||
| 50–54 | 210 | 42.7 |
| 55–60 | 161 | 32.7 |
| 61–65 | 112 | 22.8 |
| 66–69 | 9 | 1.8 |
| Gender | ||
| Male | 231 | 47.0 |
| Female | 261 | 53.0 |
| Education qualification | ||
| Primary school diploma | 75 | 15.2 |
| Middle school diploma | 235 | 47.8 |
| High school diploma | 97 | 19.7 |
| Bachelor’s degree | 47 | 9.6 |
| Master’s degree | 25 | 5.1 |
| Doctorate degree | 13 | 2.6 |
| Application usage | ||
| Less than 1 year | 186 | 37.8 |
| 1–3 year | 235 | 47.8 |
| More than 3 years | 71 | 14.4 |
| Preferred features | ||
| Health monitoring (e.g., body temperature, blood pressure, blood glucose, and heartbeat) | 104 | 21.1 |
| For emergency (e.g., calling for help automatically, providing vital medical information in an emergency like allergies and medical conditions) | 77 | 15.7 |
| Self-assessment or self-diagnose (e.g., checking health status with apps by yourself) | 26 | 5.3 |
| Finding suitable doctors and hospitals and making an appointment | 44 | 8.9 |
| Knowledge about health and health preservation information | 33 | 6.7 |
| Helping with healthy diet (e.g., healthy recipes, calories calculator, and food diary) | 56 | 11.4 |
| Fitness and exercises (step counter and exercise guide) | 75 | 15.2 |
| Communicating with a doctor online | 27 | 5.5 |
| Communicating with people who have the same health issue | 50 | 10.2 |
| Construct | Indicators | Factor Loading | Cronbach’s Alpha | CR | AVE |
|---|---|---|---|---|---|
| Visual attractiveness (VA) | VA1 | 0.821 | 0.916 | 0.924 | 0.706 |
| VA2 | 0.852 | ||||
| VA3 | 0.801 | ||||
| VA4 | 0.785 | ||||
| VA5 | 0.885 | ||||
| VA6 | 0.892 | ||||
| Prototypicality (PT) | PT1 | 0.866 | 0.887 | 0.910 | 0.814 |
| PT2 | 0.917 | ||||
| PT3 | 0.922 | ||||
| Completeness (COM) | COM1 | 0.902 | 0.889 | 0.908 | 0.768 |
| COM2 | 0.877 | ||||
| COM3 | 0.820 | ||||
| COM4 | 0.904 | ||||
| Memorability (MEM) | MEM1 | 0.923 | 0.919 | 0.920 | 0.861 |
| MEM2 | 0.929 | ||||
| MEM3 | 0.931 | ||||
| Learnability (LRN) | LRN1 | 0.904 | 0.930 | 0.931 | 0.827 |
| LRN2 | 0.917 | ||||
| LRN3 | 0.898 | ||||
| LRN4 | 0.919 | ||||
| Customizability (CTM) | CTM1 | 0.892 | 0.923 | 0.929 | 0.812 |
| CTM2 | 0.896 | ||||
| CTM3 | 0.903 | ||||
| CTM4 | 0.913 | ||||
| Uncertainty avoidance (UA) | UA1 | 0.887 | 0.919 | 0.919 | 0.804 |
| UA2 | 0.888 | ||||
| UA3 | 0.900 | ||||
| UA4 | 0.912 | ||||
| Psychological engagement (PEN) | PEN1 | 0.919 | 0.919 | 0.920 | 0.860 |
| PEN2 | 0.937 | ||||
| PEN3 | 0.926 | ||||
| Satisfaction (SAT) | SAT1 | 0.924 | 0.941 | 0.942 | 0.849 |
| SAT2 | 0.915 | ||||
| SAT3 | 0.917 | ||||
| SAT4 | 0.929 | ||||
| Attachment (ATT) | ATT1 | 0.914 | 0.959 | 0.960 | 0.831 |
| ATT2 | 0.908 | ||||
| ATT3 | 0.911 | ||||
| ATT4 | 0.917 | ||||
| ATT5 | 0.909 | ||||
| ATT6 | 0.909 | ||||
| Stickiness (ST) | ST1 | 0.934 | 0.928 | 0.929 | 0.875 |
| ST2 | 0.935 | ||||
| ST3 | 0.936 |
| ATT | COM | CTM | LRN | MEM | PT | PEN | SAT | ST | UA | VA | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| ATT | 0.912 | ||||||||||
| COM | 0.344 | 0.876 | |||||||||
| CTM | 0.273 | 0.203 | 0.901 | ||||||||
| LRN | 0.422 | 0.322 | 0.221 | 0.909 | |||||||
| MEM | 0.348 | 0.336 | 0.247 | 0.435 | 0.928 | ||||||
| PT | 0.321 | 0.323 | 0.225 | 0.269 | 0.247 | 0.902 | |||||
| PEN | 0.560 | 0.384 | 0.262 | 0.443 | 0.389 | 0.334 | 0.927 | ||||
| SAT | 0.558 | 0.255 | 0.223 | 0.351 | 0.279 | 0.359 | 0.556 | 0.921 | |||
| ST | 0.657 | 0.298 | 0.250 | 0.388 | 0.320 | 0.326 | 0.550 | 0.590 | 0.935 | ||
| UA | −0.321 | −0.260 | −0.227 | −0.418 | −0.265 | −0.234 | −0.384 | −0.286 | −0.293 | 0.897 | |
| VA | 0.272 | 0.216 | 0.21 | 0.294 | 0.261 | 0.254 | 0.335 | 0.216 | 0.254 | −0.283 | 0.840 |
| ATT | COM | CTM | LRN | MEM | PT | PEN | SAT | ST | UA | VA | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| ATT | |||||||||||
| COM | 0.364 | ||||||||||
| CTM | 0.289 | 0.221 | |||||||||
| LRN | 0.446 | 0.352 | 0.237 | ||||||||
| MEM | 0.370 | 0.366 | 0.265 | 0.471 | |||||||
| PT | 0.342 | 0.359 | 0.245 | 0.291 | 0.270 | ||||||
| PEN | 0.596 | 0.419 | 0.283 | 0.478 | 0.423 | 0.364 | |||||
| SAT | 0.586 | 0.276 | 0.238 | 0.375 | 0.299 | 0.389 | 0.597 | ||||
| ST | 0.696 | 0.321 | 0.269 | 0.417 | 0.345 | 0.352 | 0.595 | 0.630 | |||
| UA | 0.342 | 0.286 | 0.245 | 0.453 | 0.288 | 0.257 | 0.418 | 0.308 | 0.318 | ||
| VA | 0.287 | 0.237 | 0.222 | 0.318 | 0.284 | 0.283 | 0.361 | 0.230 | 0.274 | 0.308 |
| Hypotheses | Beta | t | p | Conclusion | |
|---|---|---|---|---|---|
| H1 | Visual attractiveness → psychological engagement | 0.124 | 2.708 | 0.007 ** | Supported |
| H2 | Prototypicality → psychological engagement | 0.116 | 2.653 | 0.008 ** | Supported |
| H3 | Completeness → psychological engagement | 0.161 | 3.395 | 0.001 ** | Supported |
| H4 | Memorability → psychological engagement | 0.136 | 2.954 | 0.003 ** | Supported |
| H5 | Learnability → psychological engagement | 0.186 | 3.629 | 0.000 *** | Supported |
| H6 | Customizability → psychological engagement | 0.068 | 1.550 | 0.121 | Rejected |
| H7 | Uncertainty avoidance → psychological engagement | −0.150 | 3.572 | 0.000 *** | Supported |
| H8 | Psychological engagement → satisfaction | 0.556 | 14.586 | 0.000 *** | Supported |
| H9 | Psychological engagement → attachment | 0.560 | 14.262 | 0.000 *** | Supported |
| H10 | Satisfaction → stickiness | 0.324 | 6.767 | 0.000 *** | Supported |
| H11 | Attachment → stickiness | 0.476 | 9.784 | 0.000 *** | Supported |
| Relationship | Total Effects | Specific Indirect Effects | |||
|---|---|---|---|---|---|
| β (t-Value) | Relationship | β (t-Value) | 2.5% | 97.5% | |
| VA → ST | 0.055 (2.649 **) | VA → PEN → SAT → ST | 0.022 (2.428 *) | 0.006 | 0.043 |
| VA → PEN → ATT → ST | 0.033 (2.523 *) | 0.010 | 0.061 | ||
| PT → ST | 0.052 (2.562 *) | PT → PEN → SAT → ST | 0.021 (2.367 *) | 0.005 | 0.040 |
| PT → PEN → ATT → ST | 0.031 (2.444 *) | 0.007 | 0.058 | ||
| COM → ST | 0.072 (3.269 **) | COM → PEN → SAT → ST | 0.029 (2.935 **) | 0.012 | 0.051 |
| COM → PEN → ATT → ST | 0.043 (3.011 **) | 0.018 | 0.074 | ||
| MEM → ST | 0.061 (2.941 **) | MEM → PEN → SAT → ST | 0.025 (2.679 **) | 0.008 | 0.044 |
| MEM → PEN → ATT → ST | 0.036 (2.772 **) | 0.012 | 0.063 | ||
| LRN → ST | 0.083 (3.373 **) | LRN → PEN → SAT → ST | 0.034 (2.995 **) | 0.014 | 0.058 |
| LRN → PEN → ATT → ST | 0.050 (3.111 **) | 0.021 | 0.084 | ||
| CTM → ST | 0.031 (1.523) | CTM → PEN → SAT → ST | 0.012 (1.450) | −0.003 | 0.031 |
| CTM → PEN → ATT → ST | 0.018 (1.502) | −0.005 | 0.043 | ||
| UA → ST | −0.067 (3.424 **) | UA → PEN → SAT → ST | −0.027 (2.007 **) | −0.047 | −0.011 |
| UA → PEN → ATT → ST | −0.040 (3.180 **) | −0.067 | −0.017 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Lee, J. The Influence of UI Design Attributes and Users’ Uncertainty Avoidance on Stickiness of the Young Elderly Toward mHealth Applications. Behav. Sci. 2025, 15, 581. https://doi.org/10.3390/bs15050581
Chen Z, Lee J. The Influence of UI Design Attributes and Users’ Uncertainty Avoidance on Stickiness of the Young Elderly Toward mHealth Applications. Behavioral Sciences. 2025; 15(5):581. https://doi.org/10.3390/bs15050581
Chicago/Turabian StyleChen, Zibin, and Jaehwan Lee. 2025. "The Influence of UI Design Attributes and Users’ Uncertainty Avoidance on Stickiness of the Young Elderly Toward mHealth Applications" Behavioral Sciences 15, no. 5: 581. https://doi.org/10.3390/bs15050581
APA StyleChen, Z., & Lee, J. (2025). The Influence of UI Design Attributes and Users’ Uncertainty Avoidance on Stickiness of the Young Elderly Toward mHealth Applications. Behavioral Sciences, 15(5), 581. https://doi.org/10.3390/bs15050581