
Outcome Expectations on Physical Activity: The Roles of Body Appreciation and Health Status

Abstract
1. Introduction
1.1. Outcome Expectation and Physical Activity
1.2. The Mediating Role of Body Appreciation
1.3. The Moderating Role of Health Status
2. Method
2.1. Participants and Research Design
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics, Correlation Analysis, and Common Method Bias Test
3.2. The Mediation Effect of Body Appreciation
3.3. The Moderation Effects of Health Status
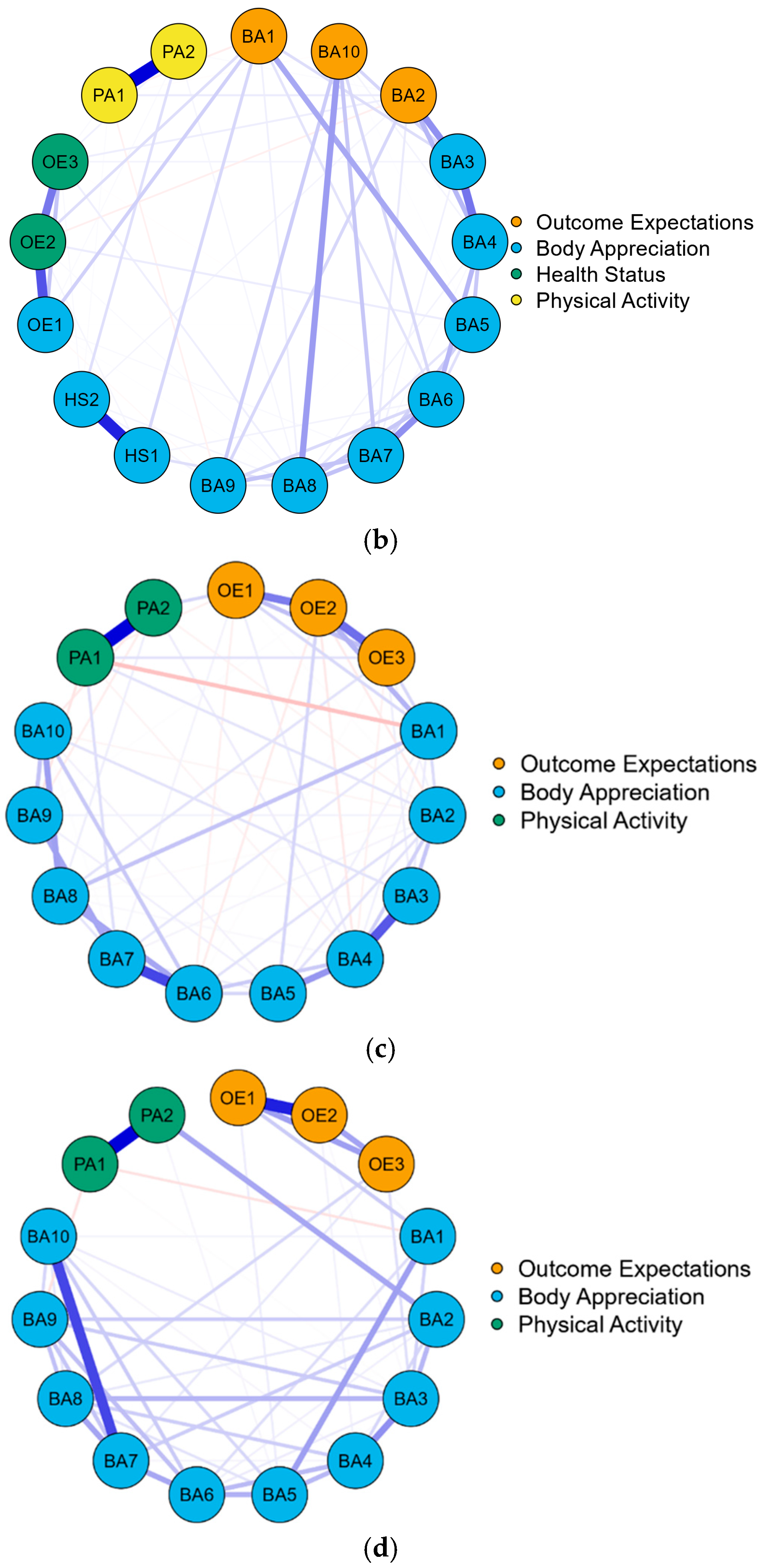
3.4. Network Structure
3.5. Centrality Indices
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| a. Weight matrix of outcome expectations, body appreciation, and physical activity for total samples. | |||||||||||||||||
| Items | OE1 | OE2 | OE3 | BA1 | BA2 | BA3 | BA4 | BA5 | BA6 | BA7 | BA8 | BA9 | BA10 | PA1 | PA2 | ||
| OE1 | 0 | 0.519 | 0.17 | 0.155 | 0 | 0 | −0.021 | 0.014 | −0.019 | 0.049 | 0.024 | −0.070 | 0 | 0 | 0.023 | ||
| OE2 | 0.519 | 0 | 0.424 | 0.105 | −0.110 | 0.01 | 0.022 | 0.054 | 0 | 0 | 0.003 | 0.059 | 0 | −0.013 | 0.014 | ||
| OE3 | 0.17 | 0.424 | 0 | 0 | 0.108 | 0.028 | 0 | 0 | −0.046 | 0 | 0.075 | −0.028 | 0.002 | 0.032 | 0.031 | ||
| BA1 | 0.155 | 0.105 | 0 | 0 | 0 | 0.126 | −0.046 | 0.276 | 0.122 | 0 | 0.068 | 0 | 0 | −0.059 | 0 | ||
| BA2 | 0 | −0.110 | 0.108 | 0 | 0 | 0.337 | 0.223 | 0 | 0 | 0.068 | 0 | 0.134 | 0 | 0.092 | 0 | ||
| BA3 | 0 | 0.01 | 0.028 | 0.126 | 0.337 | 0 | 0.431 | 0 | 0 | 0.023 | 0 | 0 | 0.123 | 0 | 0 | ||
| BA4 | −0.021 | 0.022 | 0 | −0.046 | 0.223 | 0.431 | 0 | 0.177 | 0.229 | 0.018 | 0.026 | 0 | 0.032 | −0.046 | 0.039 | ||
| BA5 | 0.014 | 0.054 | 0 | 0.276 | 0 | 0 | 0.177 | 0 | 0.097 | 0.133 | 0.073 | 0 | 0 | −0.005 | 0.014 | ||
| BA6 | −0.019 | 0 | −0.046 | 0.122 | 0 | 0 | 0.229 | 0.097 | 0 | 0.355 | 0.194 | 0.112 | 0.113 | −0.005 | 0 | ||
| BA7 | 0.049 | 0 | 0 | 0 | 0.068 | 0.023 | 0.018 | 0.133 | 0.355 | 0 | 0.181 | 0.189 | 0.175 | 0.008 | 0 | ||
| BA8 | 0.024 | 0.003 | 0.075 | 0.068 | 0 | 0 | 0.026 | 0.073 | 0.194 | 0.181 | 0 | 0.078 | 0.316 | 0.019 | 0.051 | ||
| BA9 | −0.070 | 0.059 | −0.028 | 0 | 0.134 | 0 | 0 | 0 | 0.112 | 0.189 | 0.078 | 0 | 0.151 | −0.047 | 0 | ||
| BA10 | 0 | 0 | 0.002 | 0 | 0 | 0.123 | 0.032 | 0 | 0.113 | 0.175 | 0.316 | 0.151 | 0 | −0.006 | −0.027 | ||
| PA1 | 0 | −0.013 | 0.032 | −0.059 | 0.092 | 0 | −0.046 | −0.005 | −0.005 | 0.008 | 0.019 | −0.047 | −0.006 | 0 | 0.78 | ||
| PA2 | 0.023 | 0.014 | 0.031 | 0 | 0 | 0 | 0.039 | 0.014 | 0 | 0 | 0.051 | 0 | −0.027 | 0.78 | 0 | ||
| b. Weight matrix of outcome expectations, body appreciation, health status, and physical activity for total samples. | |||||||||||||||||
| Items | OE1 | OE2 | OE3 | BA1 | BA2 | BA3 | BA4 | BA5 | BA6 | BA7 | BA8 | BA9 | BA10 | PA1 | PA2 | HS1 | HS2 |
| OE1 | 0 | 0 | 0 | 0.103 | 0 | 0.266 | 0.087 | 0 | 0.046 | 0 | 0.123 | 0 | 0.143 | 0.1 | 0 | −0.057 | 0 |
| OE2 | 0 | 0 | 0 | 0.126 | 0.033 | 0.005 | 0.119 | 0.172 | 0.3 | 0.153 | 0 | 0 | 0 | 0 | 0 | −0.010 | 0 |
| OE3 | 0 | 0 | 0 | 0.333 | 0.219 | 0 | 0 | 0.065 | 0 | 0.123 | 0 | 0.029 | 0 | −0.048 | 0.052 | 0.06 | 0.011 |
| BA1 | 0.103 | 0.126 | 0.333 | 0 | 0.416 | 0 | 0 | 0.041 | 0 | 0 | 0 | 0 | 0 | 0 | 0.031 | 0 | 0 |
| BA2 | 0 | 0.033 | 0.219 | 0.416 | 0 | 0.167 | 0.218 | 0.019 | 0.032 | 0.004 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| BA3 | 0.266 | 0.005 | 0 | 0 | 0.167 | 0 | 0.099 | 0.141 | 0.08 | 0 | 0 | 0 | 0.003 | 0.06 | 0 | 0 | 0 |
| BA4 | 0.087 | 0.119 | 0 | 0 | 0.218 | 0.099 | 0 | 0.337 | 0.172 | 0.117 | 0.037 | 0 | 0 | 0 | −0.005 | 0 | 0 |
| BA5 | 0 | 0.172 | 0.065 | 0.041 | 0.019 | 0.141 | 0.337 | 0 | 0.187 | 0.183 | 0 | 0 | 0.019 | 0 | 0 | 0 | 0 |
| BA6 | 0.046 | 0.3 | 0 | 0 | 0.032 | 0.08 | 0.172 | 0.187 | 0 | 0.067 | 0.1 | 0.032 | 0.005 | 0.016 | 0.05 | 0 | 0.028 |
| BA7 | 0 | 0.153 | 0.123 | 0 | 0.004 | 0 | 0.117 | 0.183 | 0.067 | 0 | 0.003 | 0.038 | −0.019 | 0 | 0 | −0.042 | 0 |
| BA8 | 0.123 | 0 | 0 | 0 | 0 | 0 | 0.037 | 0 | 0.1 | 0.003 | 0 | 0.649 | 0 | 0.027 | 0 | 0 | 0 |
| BA9 | 0 | 0 | 0.029 | 0 | 0 | 0 | 0 | 0 | 0.032 | 0.038 | 0.649 | 0 | 0 | 0 | 0.017 | 0.013 | 0.098 |
| BA10 | 0.143 | 0 | 0 | 0 | 0 | 0.003 | 0 | 0.019 | 0.005 | −0.019 | 0 | 0 | 0 | 0.511 | 0.176 | 0 | 0.016 |
| PA1 | 0.1 | 0 | −0.048 | 0 | 0 | 0.06 | 0 | 0 | 0.016 | 0 | 0.027 | 0 | 0.511 | 0 | 0.407 | 0 | 0 |
| PA2 | 0 | 0 | 0.052 | 0.031 | 0 | 0 | −0.005 | 0 | 0.05 | 0 | 0 | 0.017 | 0.176 | 0.407 | 0 | 0.015 | 0.045 |
| HS1 | −0.057 | −0.010 | 0.06 | 0 | 0 | 0 | 0 | 0 | 0 | −0.042 | 0 | 0.013 | 0 | 0 | 0.015 | 0 | 0.759 |
| HS2 | 0 | 0 | 0.011 | 0 | 0 | 0 | 0 | 0 | 0.028 | 0 | 0 | 0.098 | 0.016 | 0 | 0.045 | 0.759 | 0 |
| c. Weight matrix of outcome expectations, body appreciation, and physical activity for high health status group. | |||||||||||||||||
| Items | OE1 | OE2 | OE3 | BA1 | BA2 | BA3 | BA4 | BA5 | BA6 | BA7 | BA8 | BA9 | BA10 | PA1 | PA2 | ||
| OE1 | 0 | 0.409 | 0.201 | 0.117 | −0.009 | 0 | 0.055 | 0 | −0.051 | 0.038 | 0 | 0 | 0 | −0.050 | 0.131 | ||
| OE2 | 0.409 | 0 | 0.449 | 0.24 | −0.065 | 0 | −0.071 | 0.132 | −0.062 | 0 | 0 | 0.007 | 0 | 0 | 0 | ||
| OE3 | 0.201 | 0.449 | 0 | 0.125 | 0.038 | 0.053 | −0.042 | 0 | −0.009 | 0 | 0.09 | 0 | 0 | 0.093 | 0 | ||
| BA1 | 0.117 | 0.24 | 0.125 | 0 | 0.113 | 0.062 | 0.044 | 0.045 | 0 | 0.076 | 0.186 | 0 | 0 | −0.189 | 0 | ||
| BA2 | −0.009 | −0.065 | 0.038 | 0.113 | 0 | 0.178 | 0.146 | 0.093 | 0.092 | 0.034 | −0.012 | 0.039 | −0.031 | 0.086 | −0.038 | ||
| BA3 | 0 | 0 | 0.053 | 0.062 | 0.178 | 0 | 0.518 | 0 | 0 | 0 | 0.011 | 0 | 0.089 | 0 | 0 | ||
| BA4 | 0.055 | −0.071 | −0.042 | 0.044 | 0.146 | 0.518 | 0 | 0.328 | 0.166 | 0 | 0.02 | 0 | 0 | −0.034 | 0.055 | ||
| BA5 | 0 | 0.132 | 0 | 0.045 | 0.093 | 0 | 0.328 | 0 | 0.13 | 0.059 | 0 | 0.045 | 0.039 | 0 | 0 | ||
| BA6 | −0.051 | −0.062 | −0.009 | 0 | 0.092 | 0 | 0.166 | 0.13 | 0 | 0.569 | 0.28 | 0 | 0.171 | 0 | 0 | ||
| BA7 | 0.038 | 0 | 0 | 0.076 | 0.034 | 0 | 0 | 0.059 | 0.569 | 0 | 0.082 | 0.28 | 0.007 | 0.103 | 0 | ||
| BA8 | 0 | 0 | 0.09 | 0.186 | −0.012 | 0.011 | 0.02 | 0 | 0.28 | 0.082 | 0 | 0 | 0.299 | 0 | 0.052 | ||
| BA9 | 0 | 0.007 | 0 | 0 | 0.039 | 0 | 0 | 0.045 | 0 | 0.28 | 0 | 0 | 0.19 | −0.084 | −0.055 | ||
| BA10 | 0 | 0 | 0 | 0 | −0.031 | 0.089 | 0 | 0.039 | 0.171 | 0.007 | 0.299 | 0.19 | 0 | 0 | −0.067 | ||
| PA1 | −0.050 | 0 | 0.093 | −0.189 | 0.086 | 0 | −0.034 | 0 | 0 | 0.103 | 0 | −0.084 | 0 | 0 | 0.79 | ||
| PA2 | 0.131 | 0 | 0 | 0 | −0.038 | 0 | 0.055 | 0 | 0 | 0 | 0.052 | −0.055 | −0.067 | 0.79 | 0 | ||
| d. Weight matrix of outcome expectations, body appreciation, and physical activity for low health status group. | |||||||||||||||||
| Items | OE1 | OE2 | OE3 | BA1 | BA2 | BA3 | BA4 | BA5 | BA6 | BA7 | BA8 | BA9 | BA10 | PA1 | PA2 | ||
| OE1 | 0 | 0.544 | 0.241 | 0.13 | 0 | 0 | 0 | 0.047 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| OE2 | 0.544 | 0 | 0.231 | 0.007 | 0 | 0.014 | 0.032 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| OE3 | 0.241 | 0.231 | 0 | 0 | 0 | 0.079 | 0 | 0 | 0 | 0.058 | 0.1 | 0 | 0 | 0 | 0 | ||
| BA1 | 0.13 | 0.007 | 0 | 0 | 0 | 0.112 | 0 | 0.241 | 0.084 | 0 | 0 | 0 | 0.029 | −0.076 | 0 | ||
| BA2 | 0 | 0 | 0 | 0 | 0 | 0.182 | 0.101 | 0 | 0.036 | 0.126 | 0.058 | 0.128 | 0 | 0 | 0.223 | ||
| BA3 | 0 | 0.014 | 0.079 | 0.112 | 0.182 | 0 | 0.279 | 0.014 | 0.049 | 0 | 0.187 | 0.131 | 0.049 | −0.007 | 0 | ||
| BA4 | 0 | 0.032 | 0 | 0 | 0.101 | 0.279 | 0 | 0.179 | 0.175 | 0.028 | 0.123 | 0 | 0.024 | 0 | 0 | ||
| BA5 | 0.047 | 0 | 0 | 0.241 | 0 | 0.014 | 0.179 | 0 | 0.2 | 0 | 0.072 | 0 | 0.101 | 0 | 0.024 | ||
| BA6 | 0 | 0 | 0 | 0.084 | 0.036 | 0.049 | 0.175 | 0.2 | 0 | 0.221 | 0 | 0.163 | 0.133 | 0 | 0 | ||
| BA7 | 0 | 0 | 0.058 | 0 | 0.126 | 0 | 0.028 | 0 | 0.221 | 0 | 0.228 | 0.146 | 0.458 | 0 | 0 | ||
| BA8 | 0 | 0 | 0.1 | 0 | 0.058 | 0.187 | 0.123 | 0.072 | 0 | 0.228 | 0 | 0.156 | 0.066 | 0 | 0 | ||
| BA9 | 0 | 0 | 0 | 0 | 0.128 | 0.131 | 0 | 0 | 0.163 | 0.146 | 0.156 | 0 | 0.104 | −0.078 | 0 | ||
| BA10 | 0 | 0 | 0 | 0.029 | 0 | 0.049 | 0.024 | 0.101 | 0.133 | 0.458 | 0.066 | 0.104 | 0 | 0 | 0 | ||
| PA1 | 0 | 0 | 0 | −0.076 | 0 | −0.007 | 0 | 0 | 0 | 0 | 0 | −0.078 | 0 | 0 | 0.635 | ||
| PA2 | 0 | 0 | 0 | 0 | 0.223 | 0 | 0 | 0.024 | 0 | 0 | 0 | 0 | 0 | 0.635 | 0 | ||
| Items | Total Samples | High Health Status Group | Low Health Status Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Betweenness | Closeness | Strength | Expected Influence | Betweenness | Closeness | Strength | Expected Influence | Betweenness | Closeness | Strength | Expected Influence | |
| OE1 | −0.059 | −0.628 | −0.049 | −0.460 | −0.780 | −0.822 | −0.304 | −0.270 | −0.034 | −1.331 | 0.268 | 0.404 |
| OE2 | 0.236 | −0.479 | 1.671 | 0.894 | 1.560 | 0.533 | 1.186 | 0.570 | −1.409 | −1.619 | −0.624 | −0.247 |
| OE3 | −0.649 | −0.609 | −0.839 | −0.735 | −1.040 | −0.861 | −0.147 | 0.396 | 0.309 | −1.093 | −1.417 | −0.826 |
| BA1 | 0.236 | 0.466 | −0.744 | −0.996 | 1.430 | 1.574 | 0.241 | −0.367 | 1.168 | 0.457 | −1.612 | −1.702 |
| BA2 | 2.891 | 1.517 | −0.009 | −0.413 | −0.650 | −1.082 | −0.650 | −1.030 | 1.168 | 0.234 | −0.443 | −0.115 |
| BA3 | −0.354 | 1.491 | 0.020 | 0.831 | −1.040 | −0.532 | −0.899 | 0.029 | 1.340 | 1.560 | 1.220 | 1.027 |
| BA4 | 0.826 | 1.213 | 1.507 | 0.863 | 0.130 | 0.217 | 1.363 | 1.195 | −0.722 | 0.612 | 0.138 | 0.310 |
| BA5 | −0.944 | 0.265 | −1.478 | −0.523 | −0.130 | 0.157 | −1.058 | −0.142 | 0.137 | 0.460 | −0.279 | 0.005 |
| BA6 | 0.678 | 0.668 | 1.402 | 1.238 | 1.690 | 1.664 | 1.573 | 1.632 | −0.378 | 0.582 | 0.926 | 0.885 |
| BA7 | −0.354 | 0.090 | 0.803 | 1.508 | 0.000 | 0.730 | 0.450 | 1.476 | 1.340 | 1.095 | 2.285 | 1.876 |
| BA8 | −0.354 | −0.038 | 0.213 | 0.998 | 1.170 | 1.457 | −0.413 | 0.445 | 0.653 | 0.988 | 0.459 | 0.544 |
| BA9 | −0.944 | −0.079 | −1.314 | −1.932 | −1.040 | −1.248 | −1.740 | −2.067 | −1.409 | 0.297 | −0.105 | −0.626 |
| BA10 | −0.796 | −0.387 | −0.825 | −0.274 | −0.390 | −0.362 | −0.970 | −0.892 | −1.409 | 0.001 | 0.284 | 0.416 |
| PA1 | 0.531 | −1.644 | 0.248 | −0.983 | 0.000 | −0.422 | 1.164 | −0.817 | −0.722 | −1.210 | −0.839 | −1.967 |
| PA2 | −0.944 | −1.847 | −0.606 | −0.015 | −0.910 | −1.003 | 0.204 | −0.158 | −0.034 | −1.032 | −0.264 | 0.016 |
| Items | Betweenness | Closeness | Strength | Expected Influence |
|---|---|---|---|---|
| OE1 | 0.765 | −0.672 | −0.614 | −0.493 |
| OE2 | −0.210 | −1.035 | 1.434 | 0.886 |
| OE3 | −0.861 | −1.251 | −1.295 | −0.895 |
| BA1 | 3.151 | 1.540 | −0.363 | −0.757 |
| BA2 | −0.21 | 0.360 | −0.264 | −0.550 |
| BA3 | −0.427 | 0.928 | 0.559 | 0.740 |
| BA4 | −0.319 | 0.898 | 0.983 | 1.098 |
| BA5 | 0.874 | 1.436 | −1.135 | −0.693 |
| BA6 | −0.753 | 0.575 | 1.609 | 1.560 |
| BA7 | 0.223 | 0.615 | 1.394 | 1.445 |
| BA8 | 0.115 | 0.416 | 1.026 | 1.134 |
| BA9 | −1.186 | −0.487 | −1.651 | −1.894 |
| BA10 | −0.644 | 0.027 | −0.412 | −0.207 |
| PA1 | −0.319 | −1.643 | −0.135 | −1.214 |
| PA2 | −0.536 | −1.664 | −0.142 | 0.147 |
| HS1 | 0.765 | 0.194 | −0.261 | 0.046 |
| HS2 | −0.427 | −0.238 | −0.732 | −0.352 |
References
- Adler, N. E., Epel, E. S., Castellazzo, G., & Ickovics, J. R. (2000). Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, white women. Health Psychology, 19(6), 586–592. [Google Scholar] [CrossRef] [PubMed]
- American College Health Association (ACHA). (2019). Spring 2019 reference group executive summary. National College Health Assessment. Available online: https://www.acha.org/wp-content/uploads/2024/07/NCHA-II_SPRING_2019_US_REFERENCE_GROUP_EXECUTIVE_SUMMARY.pdf (accessed on 2 March 2025).
- Anderson, L. L., MapelLentz, S., & Larson, S. A. (2019). Physical disability and health disparities. In D. Hollar (Ed.), Advances in exercise and health for people with mobility limitations (pp. 41–59). Springer International Publishing. [Google Scholar]
- Andrew, R., Tiggemann, M., & Clark, L. (2016). Predictors and health-related outcomes of positive body image in adolescent girls: A prospective study. Developmental Psychology, 52(3), 463–474. [Google Scholar] [CrossRef]
- August, K. J., Malik, D., Markey, C. H., Woods, K., & Gerwitz, G. C. (2023). Additive and interactive associations among body appreciation, self-compassion, and gender in understanding college students’ health behaviors. Body Image, 47, 101634. [Google Scholar] [CrossRef] [PubMed]
- Avalos, L., Tylka, T. L., & Wood-Barcalow, N. (2005). The body appreciation scale: Development and psychometric evaluation. Body Image, 2(3), 285–297. [Google Scholar] [CrossRef] [PubMed]
- Bakalım, O. (2016). Self-confident approach in coping with stress and social appearance anxiety of turkish university students: The mediating role of body appreciation. International Journal of Higher Education, 5, 134–143. [Google Scholar] [CrossRef]
- Bandura, A. (1986). The explanatory and predictive scope of self-efficacy theory. Journal of Social and Clinical Psychology, 4(3), 359–373. [Google Scholar] [CrossRef]
- Bandura, A. (1997). The anatomy of stages of change. American Journal of Health Promotion: AJHP, 12(1), 8–10. [Google Scholar] [CrossRef]
- Bandura, A. (2004). Health promotion by social cognitive means. Health Education & Behavior, 31(2), 143–164. [Google Scholar]
- Becker, C. B., Verzijl, C. L., Kilpela, L. S., Wilfred, S. A., & Stewart, T. (2019). Body image in adult women: Associations with health behaviors, quality of life, and functional impairment. Journal of Health Psychology, 24(11), 1536–1547. [Google Scholar] [CrossRef]
- Borsboom, D., Cramer, A. O., Schmittmann, V. D., Epskamp, S., & Waldorp, L. J. (2011). The small world of psychopathology. PLoS ONE, 6(11), e27407. [Google Scholar] [CrossRef] [PubMed Central]
- Caldwell, A. E., Masters, K. S., Peters, J. C., Bryan, A. D., Grigsby, J., Hooker, S. A., Wyatt, H. R., & Hill, J. O. (2018). Harnessing centred identity transformation to reduce executive function burden for maintenance of health behaviour change: The Maintain IT model. Health Psychology Review, 12(3), 231–253. [Google Scholar] [CrossRef] [PubMed]
- Conceição, E. M., de Lourdes, M., Moreira, L., Pinto-Bastos, A., & Félix, S. (2020). Weight loss expectations and weight loss after surgery: The mediating role of body image and weight concerns. Surgery for Obesity and Related Diseases, 16(7), 932–939. [Google Scholar] [CrossRef]
- Cox, A. E., Ullrich-French, S., Tylka, T. L., & McMahon, A. K. (2019). The roles of self-compassion, body surveillance, and body appreciation in predicting intrinsic motivation for physical activity: Cross-sectional associations, and prospective changes within a yoga context. Body Image, 29, 110–117. [Google Scholar] [CrossRef]
- Deci, E. L., & Ryan, R. M. (2000). The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychological Inquiry, 11(4), 227–268. [Google Scholar] [CrossRef]
- Deng, J. X., Wang, M. C., Shou, Y. Y., & Gao, Y. (2021). Core features of callous-unemotional traits: Network analysis of the inventory of callous-unemotional traits in offender and community samples. Journal of Clinical Psychology, 77(6), 1487–1498. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, N., Arnaoutis, G., Chrysohoou, C., Barkas, F., Liberopoulos, E., Sfikakis, P. P., Pitsavos, C., Tsioufis, C., Tambalis, K. D., & Panagiotakos, D. (2025). Assessment of long-term engagement in aerobic versus resistance exercise on 20-year cardiovascular disease incidence (2002–2024): The ATTICA epidemiological cohort study. Journal of Clinical Medicine, 14(2), 522. [Google Scholar] [CrossRef]
- Epskamp, S., Cramer, A. O. J., Waldorp, L. J., Schmittmann, V. D., & Borsboom, D. (2012). qgraph: Network visualizations of relationships in psychometric data. Journal of Statistical Software, 48(4), 1–18. [Google Scholar] [CrossRef]
- Ferraro, K. F., & Farmer, M. M. (1999). Utility of health data from social surveys: Is there a gold standard for measuring morbidity? American Sociological Review, 64(2), 303–315. [Google Scholar] [CrossRef]
- Gillen, M. M. (2015). Associations between positive body image and indicators of men’s and women’s mental and physical health. Body Image, 13, 67–74. [Google Scholar] [CrossRef]
- Gomer, B., Jiang, G., & Yuan, K.-H. (2019). New effect size measures for structural equation modeling. Structural Equation Modeling: A Multidisciplinary Journal, 26(3), 371–389. [Google Scholar] [CrossRef]
- Guerriero, M. A., Dipace, A., Monda, A., De Maria, A., Polito, R., Messina, G., Monda, M., di Padova, M., Basta, A., Ruberto, M., Capasso, E., Moscatelli, F., & Limone, P. (2025). Relationship between sedentary lifestyle, physical activity and stress in university students and their life habits: A scoping review with PRISMA checklist (PRISMA-ScR). Brain Sciences, 15(1), 78. [Google Scholar] [CrossRef]
- Halliwell, E., Dawson, K., & Burkey, S. (2019). A randomized experimental evaluation of a yoga-based body image intervention. Body Image, 28, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Press. [Google Scholar]
- Heinrich, K. M., Maddock, J., & Bauman, A. (2011). Exploring the relationship between physical activity knowledge, health outcomes expectancies, and behavior. Journal of Physical Activity and Health, 8(3), 404–409. [Google Scholar] [CrossRef] [PubMed]
- Hevey, D. (2018). Network analysis: A brief overview and tutorial. Health Psychology and Behavioral Medicine, 6(1), 301–328. [Google Scholar] [CrossRef]
- Jones, B. T., Corbin, W., & Fromme, K. (2001). A review of expectancy theory and alcohol consumption. Addiction, 96(1), 57–72. [Google Scholar]
- Karvinen, K., & Vallance, J. (2015). Breast and colon cancer survivors’ expectations about physical activity for improving survival. Oncology Nursing Forum, 42(5), 527–533. [Google Scholar] [CrossRef]
- Kawaji, T., Hasegawa, T., & Uchiyama, Y. (2022). Dyspnea and outcome expectations are associated with physical activity in persons with pneumoconiosis: A cross-sectional study. BMC Pulmonary Medicine, 22(1), 335. [Google Scholar] [CrossRef]
- Li, B., Jiang, W., Han, S.-S., Ye, Y.-P., Li, Y.-X., Lou, H., & Zhang, J.-Y. (2024). Influence of moderate-to-high intensity physical activity on depression levels: A study based on a health survey of Chinese university students. BMC Public Health, 24(1), 1023. [Google Scholar] [CrossRef]
- Lyon, B. (2005). Getting back on track: Nursing’s autonomous scope of practice. Clinical Nurse Specialist, 19(1), 28–33. [Google Scholar] [CrossRef]
- Maddux, J. E., Sherer, M., & Rogers, R. W. (1982). Self-efficacy expectancy and outcome expectancy: Their relationship and their effects on behavioral intentions. Cognitive Therapy and Research, 6(2), 207–211. [Google Scholar] [CrossRef]
- Medrano-Ureña, M. D. R., Ortega-Ruiz, R., & Benítez-Sillero, J. D. (2020). Physical fitness, exercise self-efficacy, and quality of life in adulthood: A systematic review. International Journal of Environmental Research and Public Health, 17(17), 6343. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mootoo, C., Fountain, C., & Rasmussen, A. (2019). Formative psychosocial evaluation using dynamic networks: Trauma, stressors, and distress among Darfur refugees living in Chad. Conflict and Health, 13, 30. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D., Watts, A. W., & Rydell, S. (2018). Yoga and body image: How do young adults practicing yoga describe its impact on their body image? Body Image, 27, 156–168. [Google Scholar] [CrossRef] [PubMed Central]
- Nolen, E., & Panisch, L. S. (2022). The relationship between body appreciation and health behaviors among women and adolescent girls: A scoping review. Health & Social Work, 47(2), 113–122. [Google Scholar] [CrossRef]
- Opsahl, T., Agneessens, F., & Skvoretz, J. (2010). Node centrality in weighted networks: Generalizing degree and shortest paths. Social Networks, 32(3), 245–251. [Google Scholar] [CrossRef]
- Pender, N. J., Murdaugh, C. L., & Parsons, M. A. (2011). Health promotion in nursing practice. Health Promotion in Nursing Practice. [Google Scholar]
- Penedo, F. J., & Dahn, J. R. (2005). Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Current Opinion in Psychiatry, 18(2), 189–193. [Google Scholar] [CrossRef]
- Perkins, H. Y., Waters, A. J., Baum, G. P., & Basen-Engquist, K. M. (2009). Outcome expectations, expectancy accessibility, and exercise in endometrial cancer survivors. Journal of Sport and Exercise Psychology, 31(6), 776–785. [Google Scholar] [CrossRef]
- Phillips, W. J., & Hine, D. W. (2021). Self-compassion, physical health, and health behaviour: A meta-analysis. Health Psychology Review, 15(1), 113–139. [Google Scholar] [CrossRef] [PubMed]
- Podsakoff, P. M., MacKenzie, S. B., & Podsakoff, N. P. (2012). Sources of method bias in social science research and recommendations on how to control it. Annual Review of Psychology, 63(1), 539–569. [Google Scholar] [CrossRef]
- Robinaugh, D. J., Millner, A. J., & McNally, R. J. (2016). Identifying highly influential nodes in the complicated grief network. Journal of Abnormal Psychology, 125(6), 747–757. [Google Scholar] [CrossRef]
- Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist, 55(1), 68–78. [Google Scholar] [CrossRef] [PubMed]
- Saracci, R. (1997). The World Health Organisation needs to reconsider its definition of health. Bmj, 314(7091), 1409–1410. [Google Scholar] [CrossRef] [PubMed Central]
- Schwarzer, R. (2008). Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Applied Psychology: An International Review, 57(1), 1–29. [Google Scholar] [CrossRef]
- Schwarzer, R. (2016). Health action process approach (HAPA) as a theoretical framework to understand behavior change. [El Modelo Procesual de Acción en Salud como un marco de referencia teórico para entender el cambio de conducta]. Actualidades en Psicología, 30(121), 119–130. [Google Scholar] [CrossRef]
- Schwarzer, R., Lippke, S., & Luszczynska, A. (2011). Mechanisms of health behavior change in persons with chronic illness or disability: The Health Action Process Approach (HAPA). Rehabilitation Psychology, 56(3), 161. [Google Scholar]
- Shi, L., Jiang, L., Zhou, S., Zhou, W., & Yang, H. (2024). Self-appreciation is not enough: Exercise identity mediates body appreciation and physical activity and the role of perceived stress. Frontiers in Psychology, 15, 1377772. [Google Scholar] [CrossRef]
- Speed-Andrews, A. E., McGowan, E. L., Rhodes, R. E., Blanchard, C. M., Culos-Reed, S. N., Friedenreich, C. M., & Courneya, K. S. (2014). Identification and evaluation of the salient physical activity beliefs of colorectal cancer survivors. Cancer Nursing, 37(1), 14–22. [Google Scholar] [CrossRef]
- Stathopoulou, G., Powers, M. B., Berry, A. C., Smits, J. A. J., & Otto, M. W. (2006). Exercise interventions for mental health: A quantitative and qualitative review. Clinical Psychology: Science and Practice, 13(2), 179–193. [Google Scholar] [CrossRef]
- Swami, V., Ng, S. K., & Barron, D. (2016). Translation and psychometric evaluation of a Standard Chinese version of the Body Appreciation Scale-2. Body Image, 18, 23–26. [Google Scholar] [CrossRef]
- Tylka, T. L., & Homan, K. J. (2015). Exercise motives and positive body image in physically active college women and men: Exploring an expanded acceptance model of intuitive eating. Body Image, 15, 90–97. [Google Scholar] [CrossRef]
- Tylka, T. L., & Wood-Barcalow, N. L. (2015a). The Body Appreciation Scale-2: Item refinement and psychometric evaluation. Body Image, 12, 53–67. [Google Scholar] [CrossRef] [PubMed]
- Tylka, T. L., & Wood-Barcalow, N. L. (2015b). What is and what is not positive body image? Conceptual foundations and construct definition. Body Image, 14, 118–129. [Google Scholar] [CrossRef] [PubMed]
- van Borkulo, C. D., van Bork, R., Boschloo, L., Kossakowski, J. J., Tio, P., Schoevers, R. A., Borsboom, D., & Waldorp, L. J. (2023). Comparing network structures on three aspects: A permutation test. Psychological Methods, 28(6), 1273–1285. [Google Scholar] [CrossRef] [PubMed]
- Vroom, V. H. (1964). Work and motivation. Wiley. [Google Scholar]
- Warburton, D. E. R., & Bredin, S. S. D. (2017). Health benefits of physical activity: A systematic review of current systematic reviews. Current Opinion in Cardiology, 32(5), 541–556. [Google Scholar] [CrossRef]
- Weinstein, N. D. (1987). Unrealistic optimism about susceptibility to health problems: Conclusions from a community-wide sample. Journal of Behavioral Medicine, 10(5), 481–500. [Google Scholar] [CrossRef]
- Wójcicki, T. R., White, S. M., & McAuley, E. (2009). Assessing outcome expectations in older adults: The multidimensional outcome expectations for exercise scale. The Journals of Gerontology: Series B, 64B(1), 33–40. [Google Scholar] [CrossRef]
- Xiang, J. J., Peng, F., Jiao, J. Y., Tan, T., Liu, L., Chen, M. W., Wang, J. T., Luo, D., & Liu, S. (2025). Health risk behaviors, depressive symptoms and suicidal ideation among college students: A latent class analysis in middle China. Journal of Affective Disorders, 375, 205–213. [Google Scholar] [CrossRef]
- Zhang, G., Feng, W., Zhao, L., Zhao, X., & Li, T. (2024). The association between physical activity, self-efficacy, stress self-management and mental health among adolescents. Scientific Reports, 14(1), 5488. [Google Scholar] [CrossRef]
- Zheng, L., Miao, M., & Gan, Y. Q. (2020). Perceived control buffers the effects of the COVID-19 pandemic on general health and life satisfaction: The mediating role of psychological distance. Applied Psychology-Health and Well Being, 12(4), 1095–1114. [Google Scholar] [CrossRef]
- Zhou, S., Li, L. Q., Zhao, Y., Cao, Y. H., Peng, B. Z., & Zheng, L. (2021). Physical activity under stress: A perspective of HAPA and individual differences. International Journal of Environmental Research and Public Health, 18(22), 12144. [Google Scholar] [CrossRef]
| M | SD | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|---|
| 1. Age | 19.42 | 1.51 | - | ||||
| 2. Subjective Social Class | 4.85 | 1.56 | 0.02 | - | |||
| 3. Outcome Expectation | 3.67 | 0.85 | 0.04 | 0.14 ** | - | ||
| 4. Body Appreciation | 3.74 | 0.81 | 0.01 | 0.26 *** | 0.53 *** | - | |
| 5. Health Status | 3.65 | 0.77 | 0.01 | 0.23 *** | 0.39 *** | 0.56 *** | - |
| 6. Physical Activity | 2.80 | 0.85 | 0.04 | 0.09 ** | 0.20 *** | 0.20 *** | 0.27 *** |
| Effect | Effect Size | SE | LLCI | ULCI | Relative Effect |
|---|---|---|---|---|---|
| Total effect | 0.18 | 0.03 | 0.14 | 0.23 | |
| Direct effect | 0.10 | 0.03 | 0.04 | 0.16 | 55.56% |
| Indirect effect | 0.08 | 0.02 | 0.04 | 0.16 | 44.44% |
| Regression Equation | Regression Coefficient | Overall Fit Index | ||||||
|---|---|---|---|---|---|---|---|---|
| Outcome Variables | Predictive Variables | β | SE | LLCI | ULCI | t | R2 | F |
| BA | OE | 0.50 | 0.03 | 0.46 | 0.55 | 22.147 *** | 0.32 | 157.733 |
| Gender | 0.18 | 0.05 | 0.09 | 0.28 | 3.751 *** | |||
| Age | −0.01 | 0.02 | −0.04 | 0.02 | −0.475 | |||
| Subjective Social Class | 0.11 | 0.02 | 0.08 | 0.14 | 7.711 *** | |||
| PA | OE | 0.07 | 0.03 | 0.02 | 0.13 | 2.608 ** | 0.22 | 55.249 |
| BA | 0.09 | 0.03 | 0.03 | 0.15 | 2.789 ** | |||
| HS | 0.18 | 0.03 | 0.12 | 0.24 | 6.082 *** | |||
| BA × HS | 0.06 | 0.02 | 0.02 | 0.10 | 3.132 ** | |||
| Gender | −0.80 | 0.05 | −0.90 | −0.69 | −15.059 *** | |||
| Age | 0.03 | 0.02 | −0.01 | 0.06 | 1.581 | |||
| Subjective Social Class | 0.03 | 0.02 | −0.01 | 0.06 | 1.793 | |||
| Moderator | Effect Size | SE | LLCI | ULCI |
|---|---|---|---|---|
| HS (M − 1SD) | 0.02 | 0.02 | −0.02 | 0.06 |
| HS (M) | 0.05 | 0.02 | 0.01 | 0.08 |
| HS (M + SD) | 0.08 | 0.02 | 0.03 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, N.; Guan, Q.; Yin, Z.; Zhou, S.; Zhou, W. Outcome Expectations on Physical Activity: The Roles of Body Appreciation and Health Status. Behav. Sci. 2025, 15, 394. https://doi.org/10.3390/bs15030394
Wang N, Guan Q, Yin Z, Zhou S, Zhou W. Outcome Expectations on Physical Activity: The Roles of Body Appreciation and Health Status. Behavioral Sciences. 2025; 15(3):394. https://doi.org/10.3390/bs15030394
Chicago/Turabian StyleWang, Nanbo, Qingli Guan, Zihan Yin, Song Zhou, and Wenbo Zhou. 2025. "Outcome Expectations on Physical Activity: The Roles of Body Appreciation and Health Status" Behavioral Sciences 15, no. 3: 394. https://doi.org/10.3390/bs15030394
APA StyleWang, N., Guan, Q., Yin, Z., Zhou, S., & Zhou, W. (2025). Outcome Expectations on Physical Activity: The Roles of Body Appreciation and Health Status. Behavioral Sciences, 15(3), 394. https://doi.org/10.3390/bs15030394