




Exploring Attention Bias Mechanisms in Sub-Threshold Depression: ERP Insights into Biased Orientation and Disengagement

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
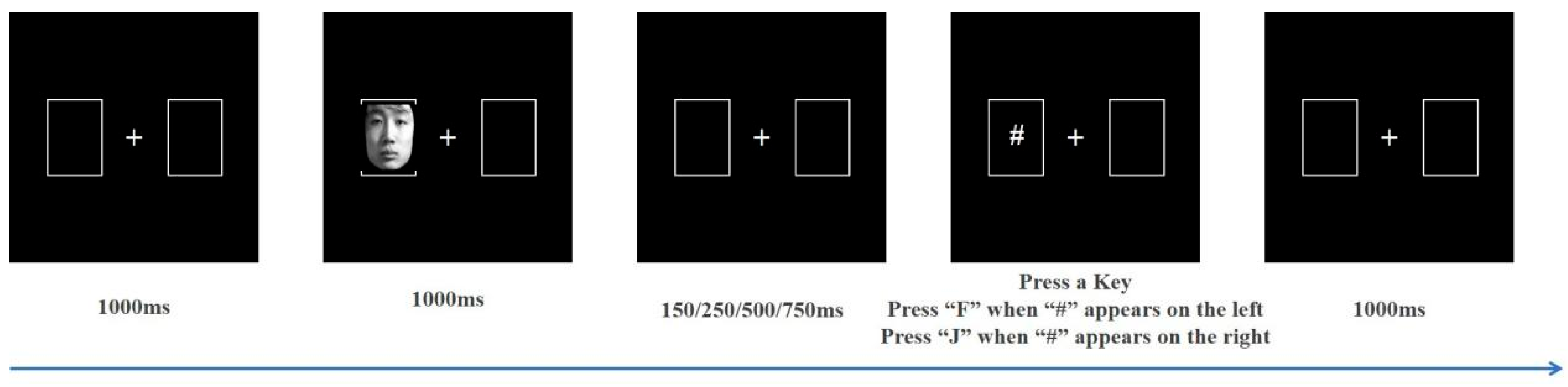
2.2. Experimental Task and Stimuli
2.3. Electroencephalogram (EEG) Recording
2.4. Statistical Analysis
3. Results
3.1. Behavioral Data
3.1.1. Participant Characteristics
3.1.2. RT
3.1.3. IOR
3.2. ERP Data
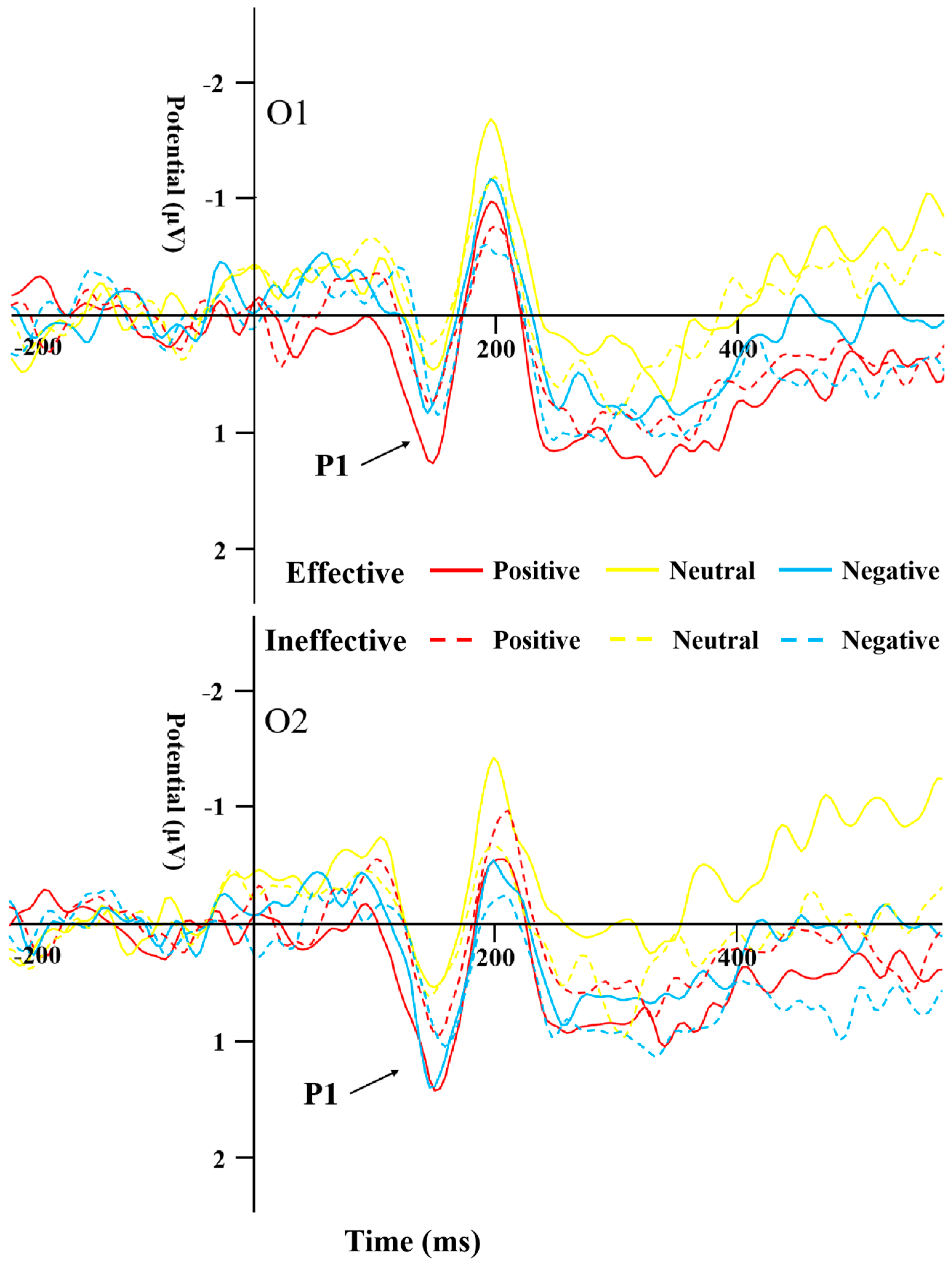
3.2.1. P1
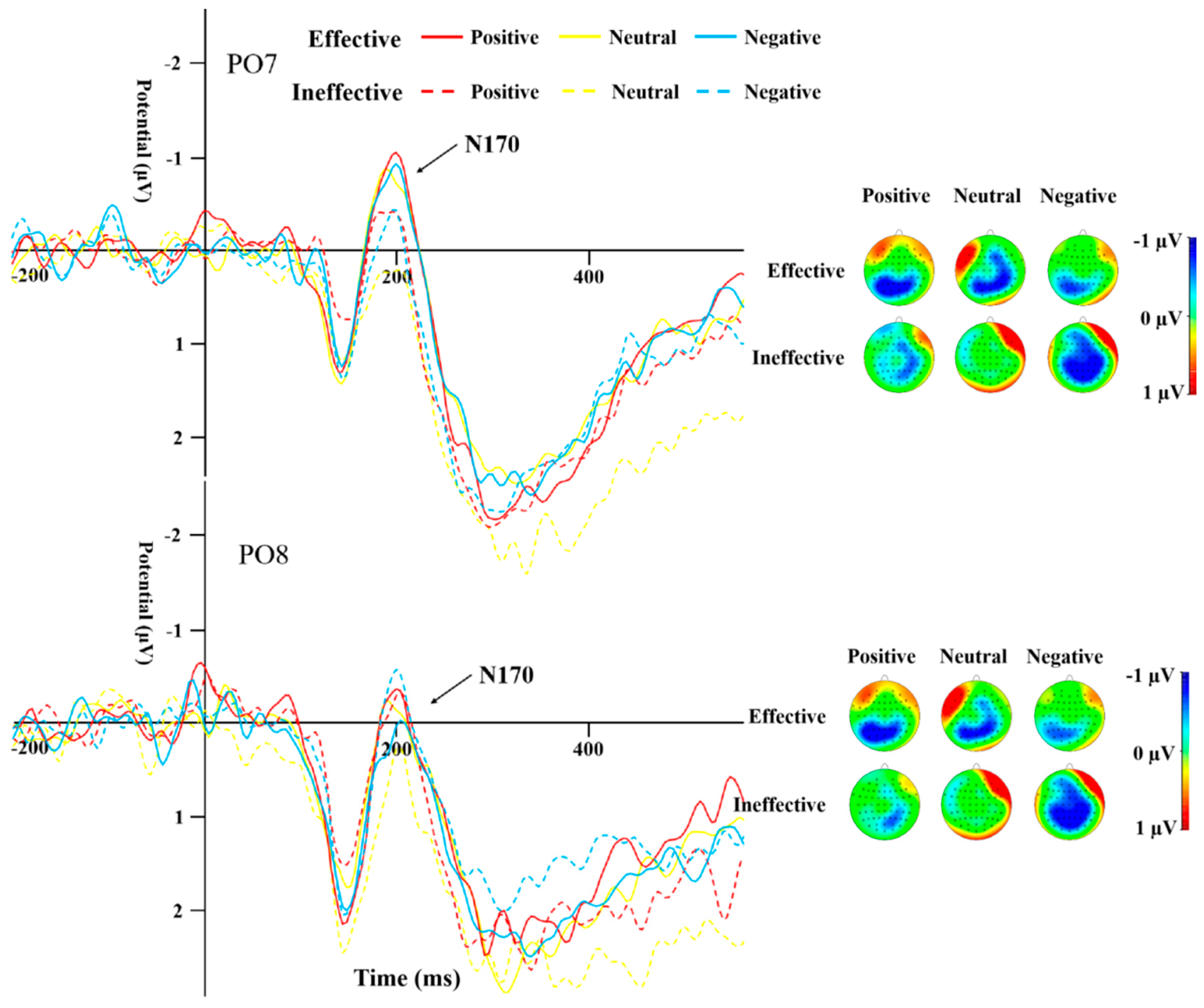
3.2.2. N170
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Murray, C.J. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wang, Y.; Wang, H.; Liu, Z.; Yu, X.; Yan, J.; Wu, Y. Prevalence of Mental Disorders in China: A Cross-Sectional Epidemiological Study. Lancet Psychiatry 2019, 6, 211–224. [Google Scholar] [CrossRef]
- Angst, J.; Sellar, R.; Merikangas, K.R. Depressive Spectrum Diagnoses. Compr. Psychiatry 2000, 41, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Judd, L.L.; Rapaport, M.H.; Paulus, M.P.; Brown, J.L. Subsyndromal Symptomatic Depression: A New Mood Disorder? J. Clin. Psychiatry 1994, 55, 17–28. [Google Scholar] [CrossRef]
- Naber, D.; Bullinger, M. Should Antidepressants Be Used in Minor Depression? Dialogues Clin. Neurosci. 2018, 20, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Sadek, N.; Bona, J. Subsyndromal Symptomatic Depression: A New Concept. Depress. Anxiety 2000, 12, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Gotlib, I.H.; Lewinsohn, P.M.; Seeley, J.R. Symptoms versus a Diagnosis of Depression: Differences in Psychosocial Functioning. J. Consult. Clin. Psychol. 1995, 63, 90–100. [Google Scholar] [CrossRef]
- da Silva Lima, A.F.; de Almeida Fleck, M.P. Subsyndromal Depression: An Impact on Quality of Life? J. Affect. Disord. 2007, 100, 163–169. [Google Scholar] [CrossRef]
- Cuijpers, P.; Smit, F.; Oostenbrink, J.; de Graaf, R.; Ten Have, M.; Beekman, A. Economic Costs of Minor Depression: A Population-Based Study. Acta Psychiatr. Scand. 2007, 115, 229–236. [Google Scholar] [CrossRef]
- Judd, L.L.; Schettler, P.J.; Akiskal, H.S. The Prevalence, Clinical Relevance, and Public Health Significance of Subthreshold Depressions. Psychiatr. Clin. N. Am. 2002, 25, 685–698. [Google Scholar] [CrossRef]
- Fogel, J.; Eaton, W.W.; Ford, D.E. Minor Depression as a Predictor of the First Onset of Major Depressive Disorder over a 15-Year Follow-Up. Acta Psychiatr. Scand. 2006, 113, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Feng, Z.Z.; Jiang, J. Effect of Strengthened or Weakened Emotional Processing on Cognitive Control in Individuals with Subthreshold Depression: An Event-Related Potential Study. J. Army Med. Univ. 2016, 38, 1991–1996. [Google Scholar]
- Cuijpers, P.; Smit, F.; van Straten, A. Psychological Treatments of Subthreshold Depression: A Meta-Analytic Review. Acta Psychiatr. Scand. 2007, 115, 434–441. [Google Scholar] [CrossRef]
- Li, H.J.; Lu, J.M.; Zhang, Q.L.; Qiu, J. Difficulty in Disengaging Attention from Emotionally Negative Stimuli among Individuals with Sub-threshold Depression. Psychol. Dev. Educ. 2016, 32, 513–520. [Google Scholar]
- Dai, Q.; Feng, Z.Z. Attentional Bias in Major Depressive Disorder. Adv. Psychol. Sci. 2008, 02, 260–265. [Google Scholar]
- Bar-Haim, Y.; Lamy, D.; Pergamin, L.; Bakermans-Kranenburg, M.J.; van IJzendoorn, M.H. Threat-Related Attentional Bias in Anxious and Non-Anxious Individuals: A Meta-Analytic Study. Psychol. Bull. 2007, 133, 1–24. [Google Scholar] [CrossRef]
- Petersen, S.E.; Posner, M.I. The Attention System of the Human Brain: 20 Years After. Annu. Rev. Neurosci. 2012, 35, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Cisler, J.M.; Koster, E. Mechanisms of Attentional Biases Towards Threat in Anxiety Disorders: An Integrative Review. Clin. Psychol. Rev. 2010, 30, 203–216. [Google Scholar] [CrossRef]
- Jongen, E.; Smulders, F.; Ranson, S.; Arts, B.; Krabbendam, L. Attentional Bias and General Orienting Processes in Bipolar Disorder. J. Behav. Ther. Exp. Psychiatry 2007, 38, 168–183. [Google Scholar] [CrossRef]
- Kellough, J.L.; Beevers, C.G.; Ellis, A.J.; Wells, T.T. Time Course of Selective Attention in Clinically Depressed Young Adults: An Eye Tracking Study. Behav. Res. Ther. 2008, 46, 1238–1243. [Google Scholar] [CrossRef]
- Gotlib, I.H.; Joormann, J. Cognition and Depression: Current Status and Future Directions. Annu. Rev. Clin. Psychol. 2010, 6, 285–312. [Google Scholar] [CrossRef] [PubMed]
- Koster, E.H.; De Raedt, R.; Goeleven, E.; Franck, E.; Crombez, G. Mood-Congruent Attentional Bias in Dysphoria: Maintained Attention to and Impaired Disengagement from Negative Information. Emotion 2005, 5, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Koster, E.H.; Crombez, G.; Van Damme, S.; Verschuere, B.; De Houwer, J. Does Imminent Threat Capture and Hold Attention? Emotion 2004, 4, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Bishop, S. Trait Anxiety and Impoverished Prefrontal Control of Attention. Nat. Neurosci. 2009, 12, 92–98. [Google Scholar] [CrossRef]
- Spek, V.; Nyklicek, I.; Smits, N.; Cuijpers, P.; Riper, H.; Keyzer, J.; Pop, V. Internet-Based Cognitive Behavioral Therapy for Subthreshold Depression in People over 50 Years Old: A Randomized Controlled Clinical Trial. Psychol. Med. 2007, 37, 1797–1806. [Google Scholar] [CrossRef]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B. Structured Clinical Interview for DSM-IV-TR Axis I Disorders—Patient Edition (SCID-I/P.2/2001 Revision); Biometrics Research Department, New York State Psychiatric Institute: New York, NY, USA, 2001. [Google Scholar]
- Vuilleumier, P.; Patrik, P. Facial Expression and Selective Attention. Curr. Opin. Psychiatry 2002, 15, 291–300. [Google Scholar] [CrossRef]
- Gong, X.; Huang, Y.X.; Wang, Y.; Luo, Y.J. Revision of the Chinese Facial Affective Picture System. Chin. Ment. Health J. 2011, 25, 40–46. [Google Scholar]
- Liu, Z.X.; Zhang, X.C.; Zheng, K.L.; Chu, J.; Peng, W.R.; Yi, J.Y. The Frontal Alpha Asymmetry in Patients with First-Episode Drug-Naive Major Depressive Disorder. Chin. J. Clin. Psychol. 2022, 30, 499–504. [Google Scholar]
- Gibson, B.S.; Amelio, J. Inhibition of Return and Attentional Control Settings. Percept. Psychophys. 2000, 62, 496–504. [Google Scholar] [CrossRef]
- Pierce, A.M.; McDonald, J.J.; Green, J.J. Electrophysiological Evidence of an Attentional Bias in Crossmodal Inhibition of Return. Neuropsychologia 2018, 114, 11–18. [Google Scholar] [CrossRef]
- Batty, M.; Taylor, M.J. Early Processing of the Six Basic Facial Emotional Expressions. Brain Res. Cogn. Brain Res. 2003, 17, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Holmes, A.; Nielsen, M.K.; Green, S. Effects of Anxiety on the Processing of Fearful and Happy Faces: An Event-Related Potential Study. Biol. Psychol. 2008, 77, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Bentin, S.; Allison, T.; Puce, A.; Perez, E.; McCarthy, G. Electrophysiological Studies of Face Perception in Humans. J. Cogn. Neurosci. 1996, 8, 551–565. [Google Scholar] [CrossRef]
- Eimer, M. Event-related brain potentials distinguish processing stages involved in face perception and recognition. Clin. Neurophysiol. 2000, 111, 694–705. [Google Scholar] [CrossRef]
- Santesso, D.L.; Meuret, A.E.; Hofmann, S.G.; Mueller, E.M.; Ratner, K.G.; Roesch, E.B.; Pizzagalli, D.A. Electrophysiological Correlates of Spatial Orienting Towards Angry Faces: A Source Localization Study. Neuropsychologia 2008, 46, 1338–1348. [Google Scholar] [CrossRef] [PubMed]
- Deldin, P.J.; Keller, J.; Gergen, J.A.; Miller, G.A. Right-Posterior Face Processing Anomaly in Depression. J. Abnorm. Psychol. 2000, 109, 116–121. [Google Scholar] [CrossRef]
- Shi, Y.M.; Luo, Y.J. Attentional Bias to Affective Information in College Students with Optimistic and Pessimistic Attributional Style. Chin. Ment. Health J. 2017, 31, 395–399. [Google Scholar]
- Zhang, Y.; Peng, C.H.; Sun, Y.; Zhang, M. Cognitive Mechanism of Visual Inhibition of Return. Adv. Psychol. Sci. 2013, 21, 1913–1926. [Google Scholar] [CrossRef]
- Posner, M.I.; Cohen, Y. Components of Visual Orienting. Atten. Perform. 1984, 32, 531–556. [Google Scholar]
- Klein, R.M. Inhibition of Return. Trends Cogn. Sci. 2000, 4, 138–147. [Google Scholar] [CrossRef]
- Allison, T.; Puce, A.; Spencer, D.D.; McCarthy, G. Electrophysiological Studies of Human Face Perception. I: Potentials Generated in Occipitotemporal Cortex by Face and Non-Face Stimuli. Cereb. Cortex 1999, 9, 415–430. [Google Scholar] [CrossRef] [PubMed]
- Eldar, S.; Yankelevitch, R.; Lamy, D.; Bar-Haim, Y. Enhanced Neural Reactivity and Selective Attention to Threat in Anxiety. Biol. Psychol. 2010, 85, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Tang, Y.; Chen, S.; Lyu, Y.; Curtin, A.; Wang, J.; Sun, J.; Tong, S. Early Perceptual Anomaly of Negative Facial Expression in Depression: An Event-Related Potential Study. Neurophysiol. Clin. /Clin. Neurophysiol. 2015, 45, 435–443. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SD | HC | t | p | |
|---|---|---|---|---|
| Male:Female | 11:14 | 12:9 | ||
| Age | 21.12 ± 2.297 | 22.38 ± 2.783 | −1.684 | 0.099 |
| BDI-Ⅱ | 30.48 ± 6.035 | 1.76 ± 1.7 | 22.741 | *** |
| SDS | 64.08 ± 7 | 32.54 ± 4.08 | 39.576 | *** |
| T-AI | 31.28 ± 9.26 | 28.76 ± 4.5 | 1.201 | 0.238 |
| SOA (ms) | Emotion | Effective | Ineffective | IOR | |
|---|---|---|---|---|---|
| SD | 150 | Positive | 442.49 ± 78.17 | 434.83 ± 87.71 | −7.67 ± 42.43 |
| Neutral | 430.95 ± 71.06 | 431.23 ± 77.10 | 0.28 ± 33.39 | ||
| Negative | 437.78 ± 82.15 | 426.37 ± 80.77 | −11.40 ± 38.96 | ||
| 250 | Positive | 426.91 ± 80.32 | 432.96 ± 83.09 | 6.04 ± 31.84 | |
| Neutral | 425.95 ± 95.07 | 426.32 ± 79.19 | 0.36 ± 42.46 | ||
| Negative | 425.65 ± 90.65 | 427.31 ± 84.00 | 1.66 ± 44.62 | ||
| 500 | Positive | 407.34 ± 93.62 | 401.90 ± 86.07 | −5.44 ± 48.31 | |
| Neutral | 385.13 ± 74.27 | 394.70 ± 83.48 | −0.43 ± 30.63 | ||
| Negative | 399.47 ± 77.01 | 391.95 ± 80.20 | −7.52 ± 46.74 | ||
| 750 | Positive | 384.64 ± 66.35 | 377.52 ± 61.19 | −7.12 ± 26.43 | |
| Neutral | 391.47 ± 79.10 | 382.61 ± 65.02 | −8.85 ± 39.71 | ||
| Negative | 385.42 ± 67.78 | 379.68 ± 64.69 | −5.74 ± 26.60 | ||
| HC | 150 | Positive | 429.16 ± 74.33 | 442.33 ± 62.65 | 13.17 ± 36.74 |
| Neutral | 424.28 ± 57.40 | 443.78 ± 74.04 | 19.51 ± 37.71 | ||
| Negative | 436.54 ± 75.03 | 429.41 ± 55.76 | −7.14 ± 60.07 | ||
| 250 | Positive | 399.61 ± 55.19 | 421.04 ± 67.69 | 21.43 ± 39.30 | |
| Neutral | 415.03 ± 67.17 | 425.21 ± 71.55 | 10.18 ± 40.47 | ||
| Negative | 415.30 ± 66.09 | 418.06 ± 59.45 | 2.77 ± 36.99 | ||
| 500 | Positive | 397.84 ± 61.82 | 387.98 ± 56.70 | −9.86 ± 30.92 | |
| Neutral | 388.97 ± 65.59 | 387.16 ± 56.38 | −1.80 ± 42.80 | ||
| Negative | 391.96 ± 54.41 | 392.94 ± 54.55 | 0.98 ± 43.98 | ||
| 750 | Positive | 388.34 ± 57.43 | 380.71 ± 60.19 | −7.62 ± 27.91 | |
| Neutral | 382.23 ± 55.40 | 384.73 ± 68.42 | 2.50 ± 32.92 | ||
| Negative | 374.24 ± 60.20 | 379.09 ± 55.44 | 4.85 ± 37.50 |
| Positive | Neutral | Negative | ||||||
|---|---|---|---|---|---|---|---|---|
| Effective | Ineffective | Effective | Ineffective | Effective | Ineffective | |||
| Peak | SD | O1 | 1.51 ± 1.37 | 0.95 ± 1.42 | 0.74 ± 2.08 | 0.58 ± 1.65 | 1.15 ±1.81 | 1.0 ± 1.55 |
| O2 | 1.69 ± 1.32 | 1.19 ± 1.20 | 0.93 ± 2.21 | 0.95 ± 1.64 | 1.66 ± 1.31 | 1.36 ± 1.43 | ||
| HC | O1 | 1.70 ± 0.88 | 1.46 ± 1.49 | 1.88 ± 1.12 | 1.89 ± 1.11 | 1.63 ± 1.01 | 1.73 ± 1.22 | |
| O2 | 1.89 ± 1.25 | 1.31 ± 1.10 | 1.78 ± 1.43 | 2.17 ± 1.39 | 1.98 ± 1.23 | 1.86 ± 1.23 | ||
| latency | SD | O1 | 145.92 ± 10.34 | 149.60 ± 12.22 | 147.52 ± 12.18 | 149.12 ± 13.64 | 149.76 ± 11.78 | 152.00 ± 10.52 |
| O2 | 146.88 ± 11.58 | 151.52 ± 12.35 | 147.36 ± 13.15 | 148.48 ± 13.08 | 150.56 ± 10.45 | 156.32 ± 12.16 | ||
| HC | O1 | 149.33 ± 10.76 | 152.95 ± 11.52 | 148.95 ± 11.38 | 152.19 ± 12.55 | 152.00 ± 11.59 | 150.29 ± 10.85 | |
| O2 | 150.48 ± 11.49 | 149.90 ± 11.29 | 148.57 ± 12.28 | 154.10 ± 8.26 | 154.67 ± 10.15 | 152.95 ± 9.03 | ||
| Positive | Neutral | Negative | ||||||
|---|---|---|---|---|---|---|---|---|
| Effective | Ineffective | Effective | Ineffective | Effective | Ineffective | |||
| Peak | SD | PO7 | −1.59 ± 1.72 | −0.64 ± 1.47 | −1.73 ± 1.98 | −1.40 ± 1.56 | −1.62 ± 1.94 | −0.86 ± 1.93 |
| PO8 | −0.78 ± 1.80 | −1.10 ± 1.53 | −1.58 ± 2.55 | −0.88 ± 1.35 | −0.76 ± 1.96 | −0.81 ± 1.83 | ||
| HC | PO7 | −1.52 ± 1.40 | −1.00 ± 1.72 | −1.29 ± 1.76 | −0.42 ± 1.97 | −1.27 ± 1.61 | −0.67 ± 1.22 | |
| PO8 | −0.96 ± 1.94 | −0.77 ± 1.67 | −0.74 ± 1.87 | −0.03 ± 2.01 | −0.47 ± 1.82 | −0.81 ± 1.59 | ||
| latency | SD | PO7 | 192.48 ± 13.73 | 192.00 ± 14.51 | 194.08 ± 13.62 | 194.40 ± 14.79 | 192.64 ± 13.84 | 194.40 ± 13.95 |
| PO8 | 196.80 ± 15.83 | 196.80 ± 13.76 | 194.72 ± 12.95 | 194.08 ± 13.32 | 197.28 ± 15.13 | 192.32 ± 15.01 | ||
| HC | PO7 | 197.71 ± 13.36 | 190.29 ± 13.95 | 194.48 ± 12.99 | 195.62 ± 15.79 | 195.43 ± 13.82 | 192.19 ± 13.53 | |
| PO8 | 200.95 ± 13.38 | 193.33 ± 11.62 | 200.19 ± 13.65 | 196.95 ± 11.66 | 197.71 ± 15.26 | 200.00 ± 10.73 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Jia, H.; Wang, E. Exploring Attention Bias Mechanisms in Sub-Threshold Depression: ERP Insights into Biased Orientation and Disengagement. Behav. Sci. 2024, 14, 821. https://doi.org/10.3390/bs14090821
Zhang X, Jia H, Wang E. Exploring Attention Bias Mechanisms in Sub-Threshold Depression: ERP Insights into Biased Orientation and Disengagement. Behavioral Sciences. 2024; 14(9):821. https://doi.org/10.3390/bs14090821
Chicago/Turabian StyleZhang, Xin, Huibin Jia, and Enguo Wang. 2024. "Exploring Attention Bias Mechanisms in Sub-Threshold Depression: ERP Insights into Biased Orientation and Disengagement" Behavioral Sciences 14, no. 9: 821. https://doi.org/10.3390/bs14090821
APA StyleZhang, X., Jia, H., & Wang, E. (2024). Exploring Attention Bias Mechanisms in Sub-Threshold Depression: ERP Insights into Biased Orientation and Disengagement. Behavioral Sciences, 14(9), 821. https://doi.org/10.3390/bs14090821