
How Does Individual Psychotherapy Promote Recovery for Persons with Psychosis? A Systematic Review of Qualitative Studies to Understand the Patient’s Experience


Abstract
1. Introduction
1.1. Psychosis and Treatment
1.2. Recovery after Psychosis
1.3. The Importance of Qualitative Research in Understanding Recovery
1.4. Aims and Scope
2. Method
2.1. Approach and Design
2.2. Study Eligibility and Exclusion Criteria
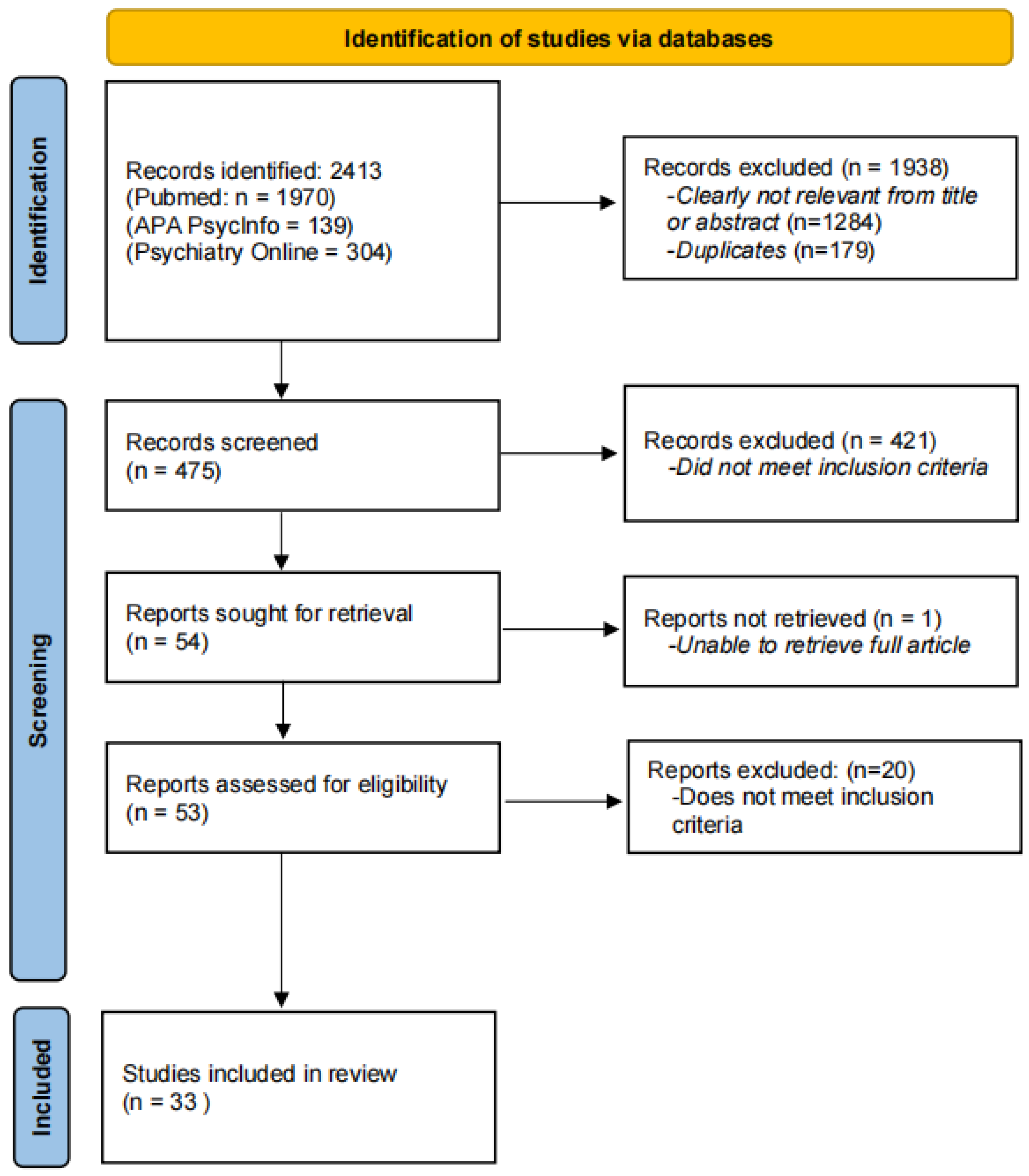
2.3. Search Strategy and Article Selection
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis
3. Results
3.1. Study Characteristics
3.2. Aim 1: Perception of Benefit, Impact on Recovery, and Mechanisms of Change
3.3. Aim 2: The Experience of Psychotherapy
3.4. Aim 3: Critiques of Therapy
4. Discussion
4.1. Psychotherapy Benefit on Objective and Subjective Recovery, and Mechanisms of Change
4.2. Therapeutic Relationship
4.3. Challenges/Barriers and Critiques of Psychotherapy
4.4. Unexpected Findings: Unique Impact of Music Therapy and Similarities to Other Approaches
4.5. Limitations
4.6. Summary and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuipers, E.; Yesufu-Udechuku, A.; Taylor, C.; Kendall, T. Management of psychosis and schizophrenia in adults: Summary of updated NICE guidance. BMJ 2014, 348, g1173. [Google Scholar] [CrossRef]
- NICE. Core Interventions in the Treatment and Management of Schizophrenia in Primary and Secondary Care; NICE: London, UK, 2009. [Google Scholar]
- Morrison, A.P. Should people with psychosis be supported in choosing cognitive therapy as an alternative to antipsychotic medication: A commentary on current evidence. Schizophr. Res. 2019, 203, 94–98. [Google Scholar] [CrossRef]
- Morrison, A.P.; Law, H.; Carter, L.; Sellers, R.; Emsley, R.; Pyle, M.; French, P.; Shiers, D.; Yung, A.; Murphy, E.K.; et al. Antipsychotic drugs versus cognitive behavioural therapy versus a combination of both in people with psychosis: A randomised controlled pilot and feasibility study. Lancet Psychiatry 2018, 5, 411–423. [Google Scholar] [CrossRef]
- Bergström, T.; Gauffin, T. The association of antipsychotic postponement with 5-year outcomes of adolescent first-episode psychosis. Schizophr. Bull. Open 2023, 4, sgad032. [Google Scholar] [CrossRef]
- Leonhardt, B.L.; Huling, K.; Hamm, J.A.; Roe, D.; Hasson-Ohayon, I.; McLeod, H.J.; Lysaker, P.H. Recovery and serious mental illness: A review of current clinical and research paradigms and future directions. Expert Rev. Neurother. 2017, 17, 1117–1130. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.; White, W. The concept of recovery as an organizing principle for integrating mental health and addiction services. J. Behav. Health Serv. Res. 2007, 34, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Anthony, W.A. Recovery from mental illness: The guiding vision of the mental health service system in the 1990s. Psychosoc. Rehabil. J. 1993, 16, 11–23. [Google Scholar] [CrossRef]
- Hamm, J.A.; Hasson-Ohayon, I.; Kukla, M.; Lysaker, P.H. Individual psychotherapy for schizophrenia: Trends and developments in the wake of the recovery movement. Psychol. Res. Behav. Manag. 2013, 6, 45–54. [Google Scholar] [CrossRef]
- Hazell, C.M.; Hayward, M.; Cavanagh, K.; Strauss, C. A systematic review and meta-analysis of low intensity CBT for psychosis. Clin. Psychol. Rev. 2016, 45, 183–192. [Google Scholar] [CrossRef]
- Naeem, F.; Khoury, B.; Munshi, T.; Ayub, M.; Lecomte, T.; Kingdon, D.; Farooq, S. Brief cognitive behavioral therapy for psychosis (CBTp) for schizophrenia: Literature review and meta-analysis. Int. J. Cogn. Ther. 2016, 9, 73–86. [Google Scholar] [CrossRef]
- Heriot-Maitland, C.; Gumley, A.; Wykes, T.; Longden, E.; Irons, C.; Gilbert, P.; Peters, E. A case series study of compassion-focused therapy for distressing experiences in psychosis. Br. J. Clin. Psychol. 2023, 62, 762–781. [Google Scholar] [CrossRef] [PubMed]
- Yıldız, E. The effects of acceptance and commitment therapy in psychosis treatment: A systematic review of randomized controlled trials. Perspect. Psychiatr. Care 2020, 56, 149–167. [Google Scholar] [CrossRef]
- Lysaker, P.H.; Klion, R.E. Recovery, Meaning-Making, and Severe Mental Illness: A Comprehensive Guide to Metacognitive Reflection and Insight Therapy; Routledge: New York, NY, USA, 2017. [Google Scholar]
- Lysaker, P.H.; Gagen, E.; Klion, R.; Zalzala, A.; Vohs, J.; Faith, L.A.; Leonhardt, B.; Hamm, J.; Hasson-Ohayon, I. Metacognitive reflection and insight therapy: A recovery-oriented treatment approach for psychosis. Psychol. Res. Behav. Manag. 2020, 13, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.; Woods-Giscombe, C. Influence of dosage and type of music therapy in symptom management and rehabilitation for individuals with schizophrenia. Issues Ment. Health Nurs. 2016, 37, 631–641. [Google Scholar] [CrossRef]
- Hardy, A.; Keen, N.; van den Berg, D.; Varese, F.; Longden, E.; Ward, T.; Brand, R.M. Trauma therapies for psychosis: A state-of-the-art review. Psychol. Psychother. Theory Res. Pract. 2023, 97, 74–90. [Google Scholar] [CrossRef]
- Palinkas, L.A. Qualitative and mixed methods in mental health services and implementation research. J. Clin. Child Adolesc. Psychol. 2014, 43, 851–861. [Google Scholar] [CrossRef]
- Bedi, R.; Hayes, S. Clients’ perspectives on, experiences of, and contributions to the working alliance. In Working Alliance Skills for Mental Health Professionals; Oxford University Press: New York, NY, USA, 2019; p. 111. [Google Scholar]
- Bachelor, A. Clients’ and therapists’ views of the therapeutic alliance: Similarities, differences and relationship to therapy outcome. Clin. Psychol. Psychother. 2013, 20, 118–135. [Google Scholar] [CrossRef] [PubMed]
- Renjith, V.; Yesodharan, R.; Noronha, J.A.; Ladd, E.; George, A. Qualitative Methods in Health Care Research. Int. J. Prev. Med. 2021, 12, 20. [Google Scholar] [CrossRef]
- Munson, M.R.; Jaccard, J.; Scott, L.D., Jr.; Moore, K.L.; Narendorf, S.C.; Cole, A.R.; Shimizu, R.; Rodwin, A.H.; Jenefsky, N.; Davis, M.; et al. Outcomes of a metaintervention to improve treatment engagement among young adults with serious mental illnesses: Application of a pilot randomized explanatory design. J. Adolesc. Health 2021, 69, 790–796. [Google Scholar] [CrossRef]
- Delsignore, A.; Schnyder, U. Control expectancies as predictors of psychotherapy outcome: A systematic review. Br. J. Clin. Psychol. 2007, 46, 467–483. [Google Scholar] [CrossRef]
- Harris, M.; Blanco, E.; Howie, H.; Rempfer, M. The discrepancy between subjective and objective evaluations of cognitive and functional ability among people with schizophrenia: A systematic review. Behav. Sci. 2023, 14, 30. [Google Scholar] [CrossRef] [PubMed]
- Holding, J.C.; Gregg, L.; Haddock, G. Individuals’ experiences and opinions of psychological therapies for psychosis: A narrative synthesis. Clin. Psychol. Rev. 2016, 43, 142–161. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.; Burke, E.; Morrison, A. Individual cognitive behavioural therapy for psychosis (CBTp): A systematic review of qualitative literature. Behav. Cogn. Psychother. 2015, 43, 285–297. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. APA Dictionary of Psychology 2024; American Psychological Association: Washington, DC, USA, 2024. [Google Scholar]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Ansdell, G.; Meehan, J. Some light at the end of the tunnel: ’Exploring users’ evidence for the effectiveness of music therapy in adult mental health settings. Music Med. 2010, 2, 29. [Google Scholar] [CrossRef]
- Bacon, T.; Farhall, J.; Fossey, E. The active therapeutic processes of acceptance and commitment therapy for persistent symptoms of psychosis: Clients’ perspectives. Behav. Cogn. Psychother. 2014, 42, 402–420. [Google Scholar] [CrossRef] [PubMed]
- Birchwood, M.; Mohan, L.; Meaden, A.; Tarrier, N.; Lewis, S.; Wykes, T.; Davies, L.M.; Dunn, G.; Peters, E.; Michail, M. The COMMAND trial of cognitive therapy for harmful compliance with command hallucinations (CTCH): A qualitative study of acceptability and tolerability in the UK. BMJ Open 2018, 8, e021657. [Google Scholar] [CrossRef]
- Bjornestad, J.; Veseth, M.; Davidson, L.; Joa, I.; Johannessen, J.O.; Larsen, T.K.; Melle, I.; Hegelstad, W.T.V. Psychotherapy in psychosis: Experiences of fully recovered service users. Front. Psychol. 2018, 9, 1675. [Google Scholar] [CrossRef]
- Bond, J.; Kenny, A.; Mesaric, A.; Wilson, N.; Pinfold, V.; Kabir, T.; Freeman, D.; Waite, F.; Larkin, M.; Robotham, D.J. A life more ordinary: A peer research method qualitative study of the Feeling Safe Programme for persecutory delusions. Psychol. Psychother. Theory Res. Pract. 2022, 95, 1108–1125. [Google Scholar] [CrossRef] [PubMed]
- Bornheimer, L.A.; Verdugo, J.L.; Krasnick, J.; Jeffers, N.; Storey, F.; King, C.A.; Taylor, S.F.; Florence, T.; Himle, J.A. A cognitive-behavioral suicide prevention treatment for adults with schizophrenia spectrum disorders in community mental health: Preliminary findings of an open pilot study. Soc. Work. Ment. Health 2023, 21, 538–560. [Google Scholar] [CrossRef] [PubMed]
- Bouws, J.; Henrard, A.; de Koning, M.; Schirmbeck, F.; van Ghesel Grothe, S.; van Aubel, E.; Reininghaus, U.; Myin-Germeys, I. Acceptance and Commitment Therapy for individuals at risk for psychosis or with a first psychotic episode: A qualitative study on patients’ perspectives. Early Interv. Psychiatry 2023, 18, 122–131. [Google Scholar] [CrossRef]
- Cella, M.; Tomlin, P.; Robotham, D.; Green, P.; Griffiths, H.; Stahl, D.; Valmaggia, L. Virtual reality therapy for the negative symptoms of schizophrenia (V-NeST): A pilot randomised feasibility trial. Schizophr. Res. 2022, 248, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Davies, B.E.; Morgan, S.; John-Evans, H.; Deere, E. ‘Monsters don’t bother me anymore’ forensic mental health service users’ experiences of acceptance and commitment therapy for psychosis. J. Forens. Psychiatry Psychol. 2019, 30, 594–613. [Google Scholar] [CrossRef]
- de Jong, S.; Hasson-Ohayon, I.; van Donkersgoed, R.; Aleman, A.; Pijnenborg, G.H.M. A qualitative evaluation of the effects of Metacognitive Reflection and Insight Therapy: ‘Living more consciously’. Psychol. Psychother. Theory Res. Pract. 2020, 93, 223–240. [Google Scholar] [CrossRef]
- Every-Palmer, S.; Ross, B.; Flewett, T.; Rutledge, E.; Hansby, O.; Bell, E. Eye movement desensitisation and reprocessing (EMDR) therapy in prison and forensic services: A qualitative study of lived experience. Eur. J. Psychotraumatol. 2023, 14, 2282029. [Google Scholar] [CrossRef]
- Feary, N.; Brand, R.; Williams, A.; Thomas, N. ‘Like jumping off a ledge into the water’: A qualitative study of trauma-focussed imaginal exposure for hearing voices. Psychol. Psychother. Theory Res. Pract. 2022, 95, 277–294. [Google Scholar] [CrossRef] [PubMed]
- Forkert, A.; Brown, P.; Freeman, D.; Waite, F. A compassionate imagery intervention for patients with persecutory delusions. Behav. Cogn. Psychother. 2022, 50, 15–27. [Google Scholar] [CrossRef]
- Gee, B.; Berry, C.; Hodgekins, J.; Greenwood, K.; Fitzsimmons, M.; Lavis, A.; Notley, C.; Pugh, K.; Birchwood, M.; Fowler, D. A qualitative process evaluation of social recovery therapy for enhancement of social recovery in first-episode psychosis (SUPEREDEN3). Behav. Cogn. Psychother. 2023, 51, 133–145. [Google Scholar] [CrossRef]
- Greenwood, K.E.; Gurnani, M.; Ward, T.; Vogel, E.; Vella, C.; McGourty, A.; Robertson, S.; Sacadura, C.; Hardy, A.; Rus-Calafell, M.; et al. The service user experience of SlowMo therapy: A co-produced thematic analysis of service users’ subjective experience. Psychol. Psychother. Theory Res. Pract. 2022, 95, 680–700. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, R.; Mansell, W.; Edge, D.; Carey, T.A.; Peel, H.; Tai, S.J. ‘It was me answering my own questions’: Experiences of method of levels therapy amongst people with first-episode psychosis. Int. J. Ment. Health Nurs. 2019, 28, 721–734. [Google Scholar] [CrossRef] [PubMed]
- Grubaugh, A.L.; Veronee, K.; Ellis, C.; Brown, W.; Knapp, R.G. Feasibility and efficacy of prolonged exposure for PTSD among individuals with a psychotic spectrum disorder. Front. Psychol. 2017, 8, 977. [Google Scholar] [CrossRef] [PubMed]
- Hardy, A.; Good, S.; Dix, J.; Longden, E. “It hurt but it helped”: A mixed methods audit of the implementation of trauma-focused cognitive-behavioral therapy for psychosis. Front. Psychiatry 2022, 13, 946615. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.; Gooding, P.A.; Awenat, Y.; Haddock, G.; Cook, L.; Huggett, C.; Jones, S.; Lobban, F.; Peeney, E.; Pratt, D.; et al. Acceptability of a novel suicide prevention psychological therapy for people who experience non-affective psychosis. Psychol. Psychother. Theory Res. Pract. 2023, 96, 560–576. [Google Scholar] [CrossRef] [PubMed]
- Hayward, M.; Bogen-Johnston, L.; Deamer, F. Relating Therapy for distressing voices: Who, or what, is changing? Psychosis 2018, 10, 132–141. [Google Scholar] [CrossRef]
- Kilbride, M.; Byrne, R.; Price, J.; Wood, L.; Barratt, S.; Welford, M.; Morrison, A.P. Exploring service users’ perceptions of cognitive behavioural therapy for psychosis: A user led study. Behav. Cogn. Psychother. 2013, 41, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Kukla, M.; Arellano-Bravo, C.; Lysaker, P.H. “I’d be a completely different person if I hadn’t gone to therapy”: A qualitative study of metacognitive therapy and recovery outcomes in adults with schizophrenia. Psychiatry 2022, 85, 259–269. [Google Scholar] [CrossRef]
- Longden, E.; Branitsky, A.; Jones, W.; Peters, S. When therapists talk to voices: Perspectives from service-users who experience auditory hallucinations. Psychol. Psychother. Theory Res. Pract. 2023, 96, 967–981. [Google Scholar] [CrossRef]
- Lysaker, P.H.; Kukla, M.; Belanger, E.; White, D.A.; Buck, K.D.; Luther, L.; Firmin, R.L.; Leonhardt, B. Individual psychotherapy and changes in self-experience in schizophrenia: A qualitative comparison of patients in metacognitively focused and supportive psychotherapy. Psychiatry 2015, 78, 305–316. [Google Scholar] [CrossRef]
- Mauritz, M.; Goossens, P.; Jongedijk, R.; Vermeulen, H.; van Gaal, B. Investigating the efficacy and experiences with narrative exposure therapy in severe mentally ill patients with comorbid post-traumatic stress disorder receiving flexible assertive community treatment: A mixed methods study. Front. Psychiatry 2022, 13, 804491. [Google Scholar] [CrossRef] [PubMed]
- Messari, S.; Hallam, R. CBT for psychosis: A qualitative analysis of clients’ experiences. Br. J. Clin. Psychol. 2003, 42, 171–188. [Google Scholar] [CrossRef] [PubMed]
- Paul, N.; Lotter, C.; van Staden, W. Patient reflections on individual music therapy for a major depressive disorder or acute phase schizophrenia spectrum disorder. J. Music Ther. 2020, 57, 168–192. [Google Scholar] [CrossRef] [PubMed]
- Schnackenberg, J.; Fleming, M.; Martin, C.R. Experience focused counselling with voice hearers as a recovery-focused approach: A qualitative thematic inquiry. Am. J. Psychiatr. Rehabil. 2019, 22, 125–146. [Google Scholar]
- Solli, H.P.; Rolvsjord, R. “The opposite of treatment”: A qualitative study of how patients diagnosed with psychosis experience music therapy. Nord. J. Music Ther. 2015, 24, 67–92. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.J.; Perry, A.; Hutton, P.; Tan, R.; Fisher, N.; Focone, C.; Griffiths, D.; Seddon, C. Cognitive analytic therapy for psychosis: A case series. Psychol. Psychother. Theory Res. Pract. 2019, 92, 359–378. [Google Scholar] [CrossRef] [PubMed]
- Tong, J.; Simpson, K.; Alvarez-Jimenez, M.; Bendall, S. Distress, psychotic symptom exacerbation, and relief in reaction to talking about trauma in the context of beneficial trauma therapy: Perspectives from young people with post-traumatic stress disorder and first episode psychosis. Behav. Cogn. Psychother. 2017, 45, 561–576. [Google Scholar] [CrossRef] [PubMed]
- Tong, J.; Simpson, K.; Alvarez-Jimenez, M.; Bendall, S. Talking about trauma in therapy: Perspectives from young people with post-traumatic stress symptoms and first episode psychosis. Early Interv. Psychiatry 2019, 13, 1236–1244. [Google Scholar] [CrossRef]
- Waller, H.; Garety, P.; Jolley, S.; Fornells-Ambrojo, M.; Kuipers, E.; Onwumere, J.; Woodall, A.; Craig, T. Training frontline mental health staff to deliver “low intensity” psychological therapy for psychosis: A qualitative analysis of therapist and service user views on the therapy and its future implementation. Behav. Cogn. Psychother. 2015, 43, 298–313. [Google Scholar] [CrossRef] [PubMed]
- Lysaker, P.H.; Holm, T.; Kukla, M.; Wiesepape, C.; Faith, L.; Musselman, A.; Lysaker, J.T. Psychosis and the challenges to narrative identity and the good life: Advances from research on the integrated model of metacognition. J. Res. Pers. 2022, 100, 104267. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I.; Arnon-Ribenfeld, N.; Hamm, J.A.; Lysaker, P.H. Agency before action: The application of behavioral activation in psychotherapy with persons with psychosis. Psychotherapy 2017, 54, 245. [Google Scholar] [CrossRef] [PubMed]
- Ruchlewska, A.; Kamperman, A.M.; van der Gaag, M.; Wierdsma, A.I.; Mulder, N.C. Working alliance in patients with severe mental illness who need a crisis intervention plan. Commun. Ment. Health J. 2016, 52, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Igra, L.; Lavidor, M.; Atzil-Slonim, D.; Arnon-Ribenfeld, N.; de Jong, S.; Hasson-Ohayon, I. A meta-analysis of client-therapist perspectives on the therapeutic alliance: Examining the moderating role of type of measurement and diagnosis. Eur. Psychiatry 2020, 63, e67. [Google Scholar] [CrossRef] [PubMed]
- Richards, M.; Bedi, R.P. Gaining perspective: How men describe incidents damaging the therapeutic alliance. Psychol. Men. Masc. 2015, 16, 170. [Google Scholar] [CrossRef]
- Lavi-Rotenberg, A.; Bar-Kalifa, E.; de Jong, S.; Igra, L.; Lysaker, P.H.; Hasson-Ohayon, I. Elements that enhance therapeutic alliance and short-term outcomes in metacognitive reflection and insight therapy: A session-by-session assessment. Psychiatr. Rehabil. J. 2020, 43, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Timulak, L.; Keogh, D. The client’s perspective on (experiences of) psychotherapy: A practice friendly review. J. Clin. Psychol. 2017, 73, 1556–1567. [Google Scholar] [CrossRef] [PubMed]
- Gold, C.; Solli, H.P.; Krüger, V.; Lie, S.A. Dose–response relationship in music therapy for people with serious mental disorders: Systematic review and meta-analysis. Clin. Psychol. Rev. 2009, 29, 193–207. [Google Scholar] [CrossRef]
- Lincoln, T.M.; Jung, E.; Wiesjahn, M.; Schlier, B. What is the minimal dose of cognitive behavior therapy for psychosis? An approximation using repeated assessments over 45 sessions. Eur. Psychiatry 2016, 38, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Lecomte, T.; Lecomte, C. Are we there yet? Commentary on special issue on psychotherapy integration for individuals with psychosis. J. Psychother. Integr. 2012, 22, 375–381. [Google Scholar] [CrossRef]
- Lysaker, P.H.; Roe, D. The processes of recovery from schizophrenia: The emergent role of integrative psychotherapy, recent developments, and new directions. J. Psychother. Integr. 2012, 22, 287–297. [Google Scholar] [CrossRef]
- Gumley, A.; Clark, S. Risk of arrested recovery following first episode psychosis: An integrative approach to psychotherapy. J. Psychother. Integr. 2012, 22, 298. [Google Scholar] [CrossRef]
- Harder, S.; Folke, S. Affect regulation and metacognition in psychotherapy of psychosis: An integrative approach. J. Psychother. Integr. 2012, 22, 330. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I. Integrating cognitive behavioral-based therapy with an intersubjective approach: Addressing metacognitive deficits among people with schizophrenia. J. Psychother. Integr. 2012, 22, 356. [Google Scholar] [CrossRef]
- Salvatore, G.; Russo, B.; Russo, M.; Popolo, R.; Dimaggio, G. Metacognition-oriented therapy for psychosis: The case of a woman with delusional disorder and paranoid personality disorder. J. Psychother. Integr. 2012, 22, 314. [Google Scholar] [CrossRef]
- Lysaker, P.H.; Buck, K.D.; Carcione, A.; Procacci, M.; Salvatore, G.; Nicolò, G.; Dimaggio, G. Addressing metacognitive capacity for self reflection in the psychotherapy for schizophrenia: A conceptual model of the key tasks and processes. Psychol. Psychother. Theory Res. Pract. 2011, 84, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Hillecke, T.; Nickel, A.; Bolay, H.V. Scientific perspectives on music therapy. Ann. N. Y. Acad. Sci. 2005, 1060, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Hamm, J.A.; Ridenour, J.M.; Hillis, J.D.; Neal, D.W.; Lysaker, P.H. Fostering intersubjectivity in the psychotherapy of psychosis: Accepting and challenging fragmentation. J. Psychother. Integr. 2022, 32, 377. [Google Scholar] [CrossRef]
- Winnicott, D.W. Playing and Reality, 2nd ed.; Routledge: New York, USA, 1971. [Google Scholar]
- Roe, D.; Lysaker, P.H. Meaning, recovery, and psychotherapy in light of the art of jazz. Psychiatr. Rehabil. J. 2023, 46, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.; Shahar, G.; Lawless, M.S.; Sells, D.; Tondora, J. Play, pleasure, and other positive life events: “Non-Specific” factors in recovery from mental illness. Psychiatry 2006, 69, 151–163. [Google Scholar] [CrossRef]
- Lambert, M.J.; Ogles, B.M. Common factors: Post hoc explanation or empirically based therapy approach? Psychotherapy 2014, 51, 500–504. [Google Scholar] [CrossRef]
- Wampold, B.E. How important are the common factors in psychotherapy? An update. World Psychiatry 2015, 14, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Lysaker, P.; Yanos, P.T.; Roe, D. The role of insight in the process of recovery from schizophrenia: A review of three views. Psychosis 2009, 1, 113–121. [Google Scholar] [CrossRef]
- Newman-Taylor, K.; Bentall, R. Cognitive behavioural therapy for psychosis: The end of the line or time for a new approach? Psychol. Psychother. Theory Res. Pract. 2023, 97, 4–18. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| First Author (Year of Publication) | Country | Type of Therapy (# of Sessions) | Participants & Setting | Aims | Analysis | Results/Themes (Subthemes) |
|---|---|---|---|---|---|---|
| Ansdell & Meehan (2010) [31] | UK | Music therapy (at least 10 sessions) | N = 19 adults aged 24–69 with chronic MH problems | To explore experiences of music therapy and its benefits and effectiveness. | Interpretive phenomenological analysis | Benefit goes beyond symptoms; reconnecting with music; working with music-health-illness narrative; therapeutic aspects of music are unified; musical processes are distinct; therapist as equal “musical companion”; music therapy is distinct from other therapies; benefits are compensatory or alleviatory; reinvigorated hope. |
| Bacon et al. (2014) [32] | AUS | Acceptance and Commitment Therapy (ACT) (8 sessions) | N = 9 people aged 16–65 diagnosed with psychosis in an OP setting | To investigate perspectives of therapeutic processes. | Thematic analysis | Usefulness of therapy; changes attributed to ACT; understanding of therapy; non-specific therapy factors. |
| Birchwood et al. (2018) [33] | UK | Cognitive therapy for harmful compliance with command hallucinations (CTCH) (25 sessions) | N = 25 adults aged 18–67 with psychosis from inpatient and OP settings | To explore service user experiences in the context of a randomized controlled trial to measure acceptability and tolerability. | Grounded theory, thematic analysis | Helpful aspects included gaining control over the voices, challenging the power/omniscience of the voices, the structured approach, normalization of hearing voices, and peer support. Concerns included anxiety about completing tasks, fear of talking to voices, need for follow-up/ongoing support and concerns with adaptability. |
| Bjornestad et al. (2018) [34] | Norway | Various approaches including CBT and psychodynamic frameworks (Average # of sessions was 76.3, range 2–416) | N = 20 fully recovered people aged 17–58 with diagnosis of psychosis or affective disorder with mood incongruent delusions | To explore the working ingredients of psychotherapy in the recovery process after psychosis. | Thematic analysis | Help with the basics; having a companion through chaotic turf; creating a common language; putting psychosis in brackets and cultivating wellness; building a bridge from psychosis to the world. |
| Bond et al. (2022) [35] | UK | Feeling Safe Programme (approximately 20 sessions) | N = 6 adults aged 22–62 with non-affective psychosis | To understand experiences of the intervention to inform future development using peer research methods. | Interpretive Phenological Analysis | Engaging with everyday life; openness, engagement, and personal responsibility; the therapist as a professional friend; gaining new knowledge and alternative perspectives; having the right pace in therapy; flexibility and fitting. |
| Bornheimer et al. (2023) [36] | US | Cognitive-behavioral suicide prevention (10 sessions) | N = 5 adults with mean age 44.7 with psychosis in community MH | To explore experience of receiving treatment (part of an open pilot study). | Grounded theory | Treatment experience; engagement enhancers; barriers to this treatment within community MH; and suggestions to improve CBSPp delivery in CMH. |
| Bouws et al. (2023) [37] | The Netherlands and Belgium | Acceptance and Commitment Therapy (ACT) (8 sessions) | N = 19 individuals aged 21–40 with clinical high risk or early psychosis from secondary MH services | To explore treatment perspectives for early psychosis. | Thematic analysis | Participants understood and connected with ACT, noticing more awareness and acceptance of their thoughts and feelings, and living more in line with their personal values. Suggestions included comments on personalization or not being psychosis specific enough and difficultly understanding material with active psychosis. |
| Cella et al. (2022) [38] | UK | Virtual Reality Therapy for the Negative Symptoms of Schizophrenia (V-NeST) (12 sessions) | N = 9 adults with mean age 37.1 with psychosis from community MH | To understand acceptability (part of a feasibility study). | Thematic analysis | Therapy goals; impact of the pandemic; issues with symptoms; using virtual reality; relevance of virtual reality; therapy procedures; suggestions for improvement. |
| Davies et al. (2019) [39] | UK | Acceptance and Commitment Therapy for Psychosis (ACTp) | N = 10 male service users aged 21–60 from a medium secure MH service with mixed MH diagnoses | To gain an understanding of experiences and changes. | Thematic analysis | Recovery (hope, helpful, improved relationships/support), insight (developing insight, normalization, reflective), developing skills (coping strategies, mindfulness, acceptance, and defusion, values and committed action), and accessibility (metaphors/visual prompts, format) |
| de Jong et al. (2020) [40] | The Netherlands | Metacognitive Reflection and Insight Therapy (MERIT) (40 sessions) | N = 14 adults with psychosis with mean age 46 in post-acute phase of treatment | To investigate experiences, effectiveness and related processes, similarities/differences from other interventions, and non-desirable factors/outcomes. | Grounded Theory | Clear changes including self, coping, interpersonal, cognitive, and affective. Factors contributing to change included: positive alliance, concrete problems, venting/self-expression, adherence/active role, and putting therapy into practice. |
| Every-Palmer et al. (2023) [41] | New Zealand | Eye movement desensitization and reprocessing (EMDR) therapy (maximum 8 sessions) | N = 10 adults aged 20–59 with PTSD and psychotic disorders who had received EMDR as part of a clinical trial, either in prison or in a hospital | To understand patient experiences of EMDR therapy while receiving forensic care. | Thematic analysis | Severe trauma was ubiquitous and greatly affected participants; participants initially reacted to EMDR with early skepticism; the therapy was initially emotionally taxing, but participants generally felt safe and persevered; they were pleasantly surprised by results (e.g., symptom reduction and personal transformation); EMDR fit with the forensic setting (empowerment in a disempowering place). |
| Feary et al. (2022) [42] | AUS | Trauma-focused imaginal exposure for hearing voices (6 sessions) | N = 10 people (age not reported) experiencing voices with mixed SMI diagnoses | To explore the experience of participants. | Thematic analysis | Benefits from the intervention (e.g., sense of self, decreased distress, wellness, understanding of symptoms/trauma); therapy was intense with later benefits; changes in relationship with the world; this therapy was a different approach with positives and negatives. |
| Forkert et al. (2022) [43] | UK | Compassionate imagery intervention (4 sessions) | N = 12 adults aged 18–65 non-affective psychosis and persecutory delusions from secondary MH services | To explore experiences of the treatment (as part of a feasibility study). | Thematic analysis | Effortful learning; seeing change (increased calm, clarity, and acceptance); taking it forward. |
| Gee et al. (2023) [44] | UK | Social Recovery Therapy (average 19.29 sessions) compared with treatment as usual | N = 19 people aged 16–35 participating in psychosis early intervention services | To explore how SRT was implemented and therapeutic processes. | Thematic analysis | Increased self-knowledge; relationship with therapist; facing your fears; pushing oneself, sense of achievement; increased agency; positivity, hope, optimism. |
| Greenwood et al. (2022) [45] | UK | SlowMo blended (therapist delivered and technology enhanced) digital therapy (8 sessions) | N = 22 adults aged 29–79 with psychosis and persistent distressing paranoia | To explore the experience of the therapy content and design. | Thematic analysis | Starting the SlowMo journey; the role of the therapist; slowing things down; value and learning from social connections; approaches and challenges of technology; improvements in paranoia and well-being. |
| Griffiths et al. (2019) [46] | UK | Transdiagnostic Cognitive Therapy: Method of Levels (MOL) (1–10 sessions) | N = 12 adults aged 19–62 with first-episode psychosis and mixed diagnostic presentation | To understand how people experienced the intervention (part of a feasibility randomized controlled trial). | Thematic analysis | The therapist’s approach; being in control; thinking and talking; gaining a different perspective about problems. |
| Grubaugh et al. (2017) [47] | US | Prolonged Exposure (PE) (10–15 sessions) | N = 14 adults with mean age 46.8 with a psychosis and PTSD | To understand patient reactions and responses to PE (part of a feasibility study). | Grounded theory | History of PTSD symptoms without previous treatment; initial hesitation of therapy and ability to manage difficult thoughts/emotions; treatment credibility; treatment benefits; intervention difficulties. |
| Hardy et al. (2022) [48] | UK | Trauma-focused CBT for psychosis | N = 6 adults aged 20–59 under the care of psychosis community MH teams | To understand experiences of therapy as part of a mixed methods study. | Inductive thematic analysis | Perseverance; establishing safety; the challenges of therapy; rebuilding one’s life after trauma. |
| Harris et al. (2023) [49] | UK | Cognitive Behavioral Suicide Prevention for psychosis (CBSPp) (maximum 24 sessions) | N = 20 adults with mean age 38 with non-affective psychosis from community MH | To investigate the views on the therapy (part of a randomized controlled trial). | Inductive thematic analysis | Affective attitude; burden; alliance; intervention coherence; perceived effectiveness; self-efficacy. |
| Hayward et al. (2018) [50] | UK | Relating Therapy (maximum 16 sessions) | N = 9 adults aged 24–61 years with psychosis | To explore the experience of participants. | Inductive Thematic analysis | Changes in me (feeling stronger, standing up for myself, connecting with others); changes in voices; and role plays. |
| Kilbride et al. (2013) [51] | UK | CBTp (# sessions not specified) | N = 9 adults aged 21–65 from either early psychosis intervention services or community MH team | To inform user-oriented perspectives on psychosis treatment. | Interpretive Phenomenological Analysis | Person-centered engagement; active process of structured learning; improvement of personal understanding; therapy is hard work; recovery and outcomes. |
| Kukla et al. (2022) [52] | US | Metacognitive Reflection and Insight Therapy (MERIT) (approximately 48 sessions) | N = 13 adults with mean age 44 with psychosis in an OP setting | To understand experiences of recovery outcomes. | Inductive thematic analysis | Improvements in real world functioning; increased formation of life pursuits; enhanced social connections; self compassion; improved quality of life and wellness. |
| Longden et al. (2023) [53] | UK | Talking with Voices (TwV) (12–39 sessions) | N = 13 individuals with psychosis | To investigate patient experiences of the treatment (part of a randomized controlled trial). | Inductive thematic analysis | Desire for appropriate help (motivation to reduce voice-related distress, limitation of other treatment options); engaging with voices (challenges, support/safety, exploration/revelation); contemplating the future (aftermath of adversity, living well with voices, resources). |
| Lysaker et al. (2015) [54] | US | Metacognitive Reflection and Insight Therapy (MERIT) compared with supportive therapy (approximately 48 sessions) | N = 25 adults with mean age 44 with psychosis from an OP VA Medical Center | To explore whether treatment can affect self-experience. | Thematic analysis | Both groups: improved confidence, self-esteem, clarity of thought, and goal setting. MERIT group: improved narrative coherence and personal agency. |
| Mauritz et al. (2022) [55] | The Netherlands | Narrative Exposure Therapy (NET) (5–16 sessions) | N = 23 adults aged 21–65 with mixed SMI diagnoses and comorbid PTSD from an OP setting | To understand patients’ experiences of NET concerning changes in symptoms, care needs, quality of life, and functioning. | Grounded theory | Increased awareness/worsening of symptoms during therapy with eventual improvement; improved self-knowledge, quality of life, and functioning; professional and informal support as helpful and needed during and after therapy (some reported this as adequate and others needed more); a few reported no improvements after treatment. |
| Messari, S. & Hallam (2003) [56] | UK | CBT for psychosis | N = 5 adults aged 28–48 with psychosis from inpatient and OP programs | To involve users in the planning and delivery of MH services. | Discourse analysis | This is truly happening; I am ill; CBT as an educational process; CBT as a respectful relationship between equals; CBT as a healing process; CBT participation as compliance with the powerful medical establishment. |
| Paul et al. (2020) [57] | South Africa | Music therapy (8 sessions) | N = 15 adults aged 18–57 with major depressive disorder (MDD) or an acute phase of psychosis from an inpatient psychiatric hospital | To explore patient reflections of music therapy. | Thematic analysis | Praise for music therapy; distress before/during therapy; opening up and emotionally dealing with old wounds; new perspectives; growing strong; emotional fulfillment; social closeness and more adept; liberation and creativity. |
| Schnakenberg et al. (2018) [58] | Germany | Experience-Focused Counselling (Making Sense of Voices) compared with treatment as usual | N = 9 adults aged 18–65 with psychosis or personality disorder | To explore whether Experience Focused Counselling could be considered trauma-sensitive. | Thematic Analysis | Trauma related; dealing with emotions; process of working with voices; intra- and interpersonal life; and coping related. |
| Solli & Rolvsjord (2015) [59] | Norway | Music therapy (14–55 sessions) | N = 9 adults aged 21–41 with psychosis or PTSD from an inpatient setting | To explore how patients experienced music therapy. | Interpretative phenomenological analysis | Freedom; contact; wellbeing; symptom reduction. |
| Taylor et al. (2019) [60] | UK | Cognitive Analytic Therapy (CAT) (4–28 sessions) | N = 4 adults aged 19–34 with psychosis from secondary care MH services | To understand the experience of receiving CAT (part of a case series study). | Thematic analysis | Insight into experiences; building a therapeutic relationship; the usefulness of CAT tools; making positive changes. |
| Tong et al. (2017) [61] | AUS | Trauma-integrated psychotherapy for psychosis (TRIPP) (unspecified # of sessions) | N = 8 adults aged 18–27 with comorbid first-episode psychosis and PTSD from an early psychosis intensive OP program | To explore young people’s reactions to a trauma-focused treatment for PTSD in FEP. | Interpretive phenological approach | Distress in session; relief in and out of session; symptom exacerbation out of session. |
| Tong et al. (2019) [62] | AUS | Trauma-integrated psychotherapy for psychosis (TRIPP) (unspecified # of sessions) | N = 11 adults aged 18–27 with comorbid first-episode psychosis and PTSD | To gain an understanding experiences of treatment and how experiences related to trauma-informed/specific treatment. | Interpretive phenological approach | Reluctance to approach the trauma memory (not wanting to talk about trauma, difficulty acknowledging the trauma, not wanting to re-experience trauma-related emotions); factors aiding the process (desire for change, not being pressured to talk, therapeutic relationship, time). |
| Waller et al. (2015) [63] | UK | “Low intensity” psychological therapy (8 weekly sessions with 1 booster at 1 month) | N = 17 adults average age 41.17 with psychosis who were in adult MH services | To evaluate the acceptability of the training protocol and the therapy, and to examine the factors promoting and restraining implementation. | Thematic analysis | Benefits of the intervention: learning new skills, achieving their goals, and therapeutic relationship. Barriers: interference of physical/MH problems and not crediting achievements. Suggestions for improvement: difficulty understanding material, not a good fit, and need for more sessions. |
| Theme | Subtheme |
|---|---|
| Improvements in objective recovery | Symptom reduction |
| Functional improvements | |
| Achievement of goals | |
| Improvements in subjective recovery | Sense of oneself |
| Self-confidence/self-compassion | |
| Quality of life/wellness | |
| Engagement with the world | |
| Mechanisms of change | Insight (understanding oneself/illness/symptoms) |
| New/improved way of thinking | |
| Autonomy/agency | |
| Learning skills | |
| Emotional expression | |
| Therapeutic relationship as an important part of psychotherapy | Equal/collaborative relationship |
| Resembled a friendship/companionship | |
| Supportive and nonjudgmental | |
| Trust | |
| Respect and Understanding | |
| Flexible & Personal | |
| Challenging | |
| Challenges/Barriers of psychotherapy | Problems with therapeutic alliance (e.g., lack of trust) |
| Early skepticism of therapy | |
| Intense/emotionally burdensome | |
| Increased distress/symptoms | |
| Critiques of psychotherapy | Need for personalization/flexibility |
| Desire for more time | |
| Difficulty understanding topics | |
| Technical issues | |
| Treatment not a good fit (e.g., too structured) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faith, L.A.; Hillis-Mascia, J.D.; Wiesepape, C.N. How Does Individual Psychotherapy Promote Recovery for Persons with Psychosis? A Systematic Review of Qualitative Studies to Understand the Patient’s Experience. Behav. Sci. 2024, 14, 460. https://doi.org/10.3390/bs14060460
Faith LA, Hillis-Mascia JD, Wiesepape CN. How Does Individual Psychotherapy Promote Recovery for Persons with Psychosis? A Systematic Review of Qualitative Studies to Understand the Patient’s Experience. Behavioral Sciences. 2024; 14(6):460. https://doi.org/10.3390/bs14060460
Chicago/Turabian StyleFaith, Laura A., Jaclyn D. Hillis-Mascia, and Courtney N. Wiesepape. 2024. "How Does Individual Psychotherapy Promote Recovery for Persons with Psychosis? A Systematic Review of Qualitative Studies to Understand the Patient’s Experience" Behavioral Sciences 14, no. 6: 460. https://doi.org/10.3390/bs14060460
APA StyleFaith, L. A., Hillis-Mascia, J. D., & Wiesepape, C. N. (2024). How Does Individual Psychotherapy Promote Recovery for Persons with Psychosis? A Systematic Review of Qualitative Studies to Understand the Patient’s Experience. Behavioral Sciences, 14(6), 460. https://doi.org/10.3390/bs14060460