
Perceived Parenting Stress Is Related to Cardiac Flexibility in Mothers: Data from the NorBaby Study

 , , and
, , and
Abstract
1. Introduction
1.1. Heart Rate Variability
1.2. Parental Stress and Well-Being
1.3. Maternal Mental States and Infant Heart Rate Variability
1.4. Maternal and Infant Heart Rate Variability
1.5. Study Aims
Research question 1: Are parenting stress or depressive symptoms related to cardiac autonomic flexibility? Would maternal bonding mediate the relationship?
We hypothesized that the higher the perceived parenting stress and/or postnatal depressive symptoms the lower the HRV in mothers. Maternal bonding might mediate the relationship between parenting stress/depressive symptoms and HRV.
Research question 2: Do antenatal factors affect the infant’s cardiac autonomic flexibility? We investigated if pregnancy-related anxiety, antenatal depressive symptoms, and recurrent negative thoughts during pregnancy have an effect on the 6-month-old infant’s HRV. We hypothesized that the higher the load of maternal adverse factors during pregnancy, the lower the infant’s HRV.
Research question 3: Is there a relationship between the mother and infant’s cardiac autonomic flexibility? To address this, we correlated maternal and infant HRV.
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.2.1. Demographic and Health Information
2.2.2. Pregnancy-Related Anxiety
2.2.3. Depressive Symptoms
2.2.4. Repetitive Negative Thinking
2.2.5. Parenting Stress
2.2.6. Postnatal Bonding
2.2.7. Cardiac Data
2.3. Data Analysis
3. Results
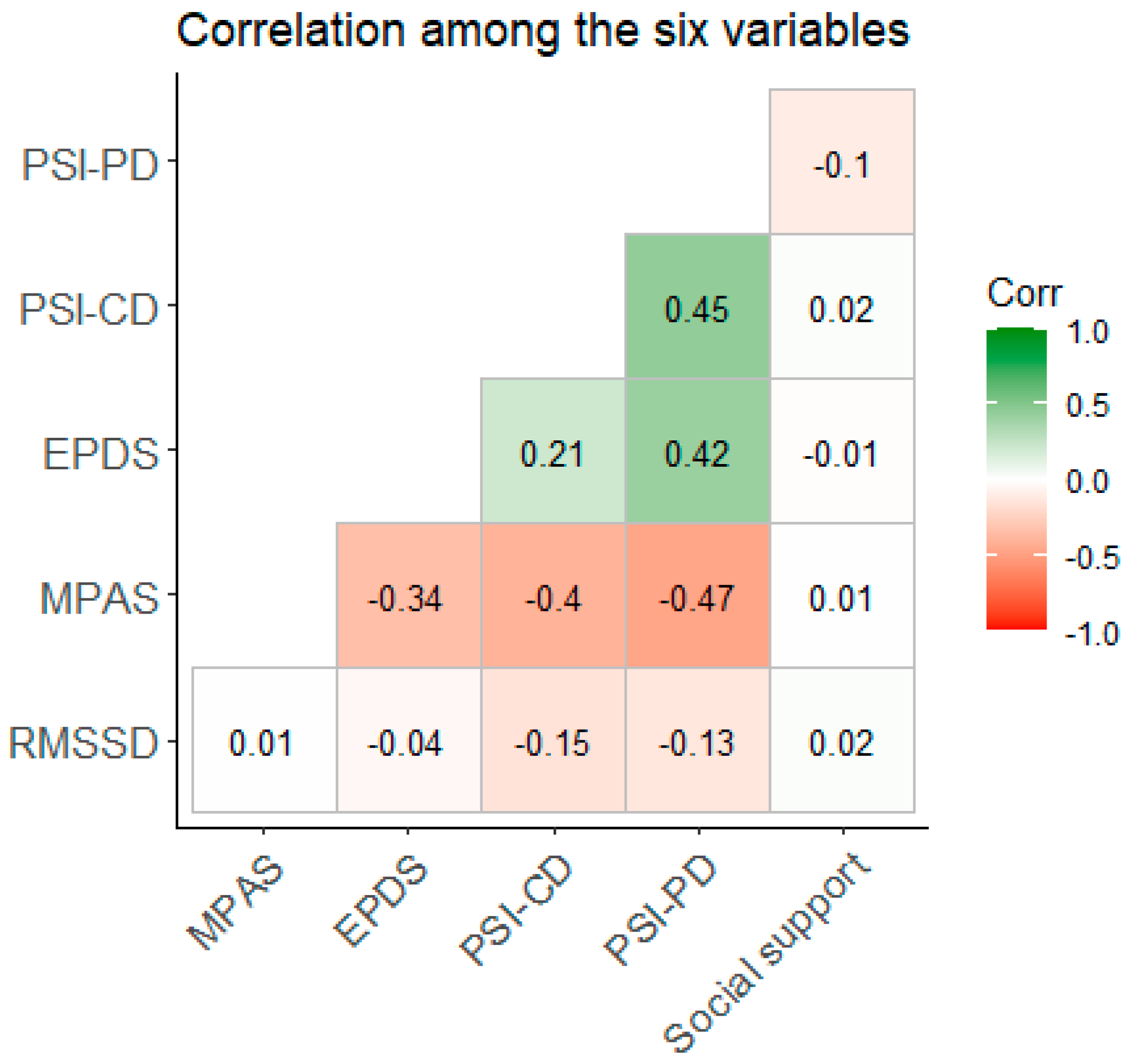
3.1. Research Question 1: Are Perceived Parenting Stress and/or Depressive Symptoms Related to Maternal HRV? If So, Does Maternal Bonding Mediate the Relationship?
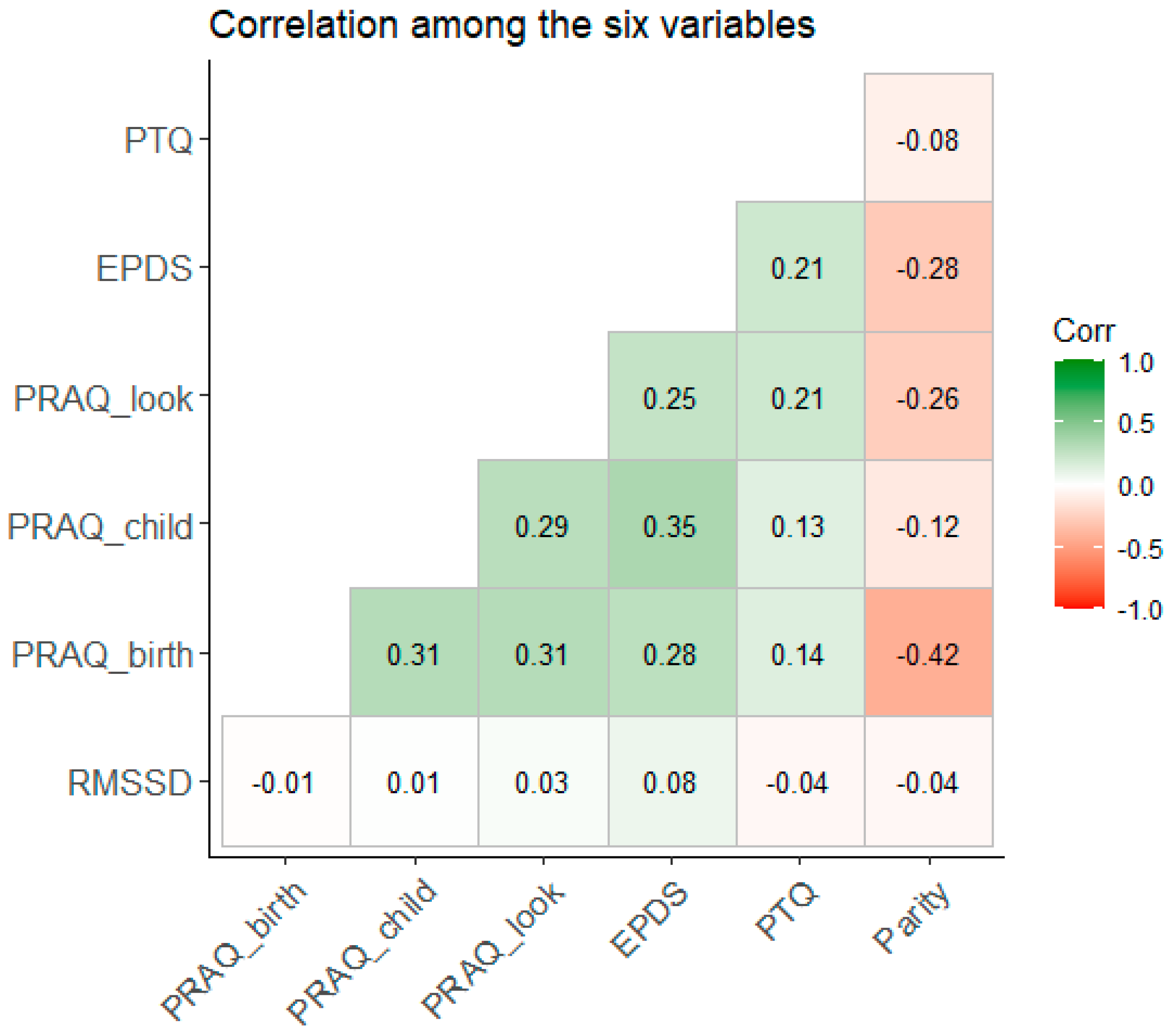
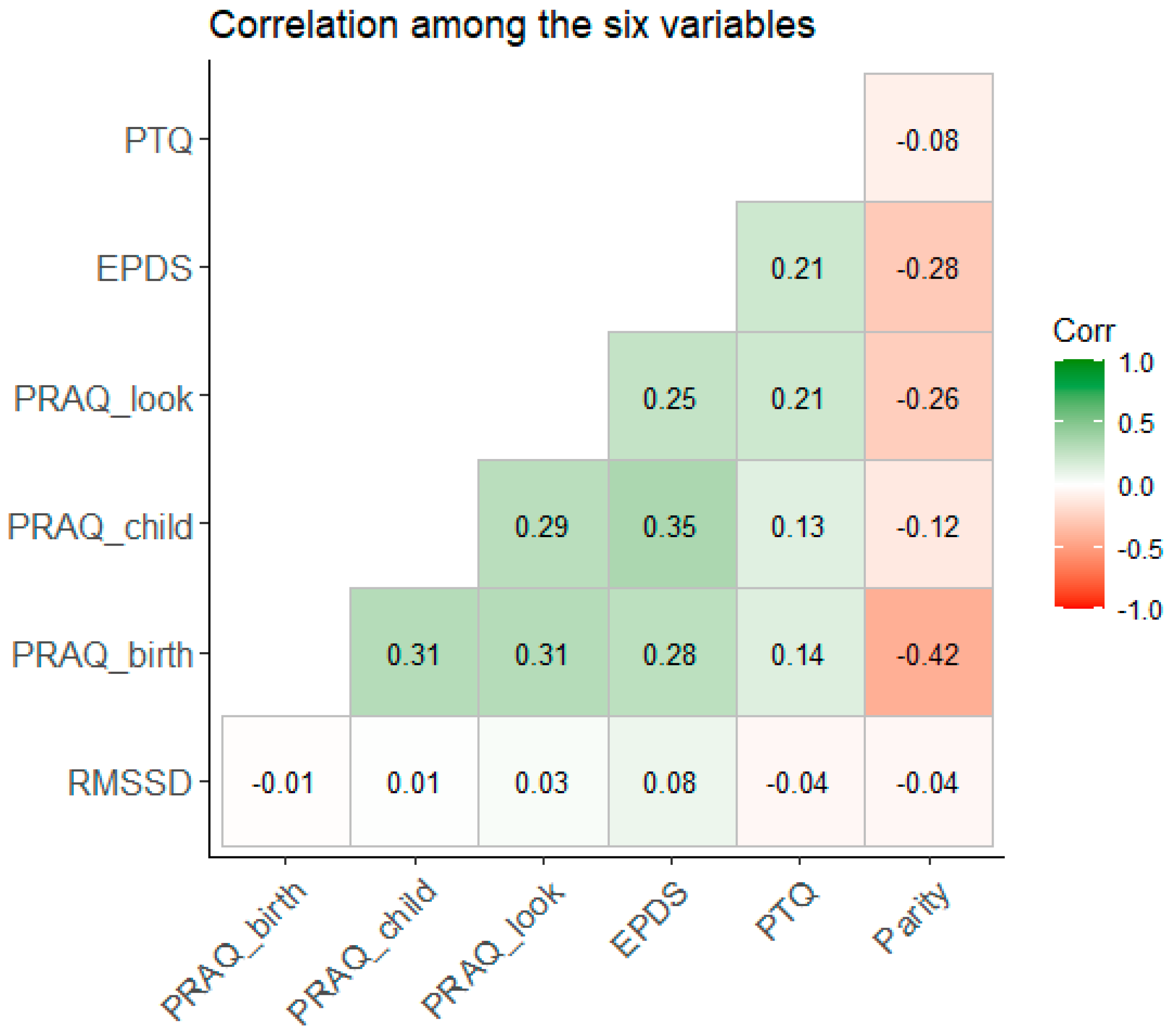
3.2. Research Question 2: Are Antenatal Factors Related to the HRV of the Infant?
3.3. Research Question 3: Are Maternal and Infant HRV Associated?
4. Discussion
4.1. Strengths and Limitations
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- DiPietro, J.A.; Ghera, M.M.; Costigan, K.; Hawkins, M. Measuring the ups and downs of pregnancy stress. J. Psychosom. Obstet. Gynecol. 2004, 25, 189–201. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, J.A.; Goldshore, M.A.; Kivlighan, K.T.; Pater, H.A.; Costigan, K.A. The ups and downs of early mothering. J. Psychosom. Obstet. Gynaecol. 2015, 36, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Galatzer-Levy, I.R.; Mazursky, H.; Mancini, A.D.; Bonanno, G.A. What we don’t expect when expecting: Evidence for heterogeneity in subjective well-being in response to parenthood. J. Fam. Psychol. JFP J. Div. Fam. Psychol. Am. Psychol. Assoc. Div. 2011, 25, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.K.; Kushlev, K.; English, T.; Dunn, E.W.; Lyubomirsky, S. In defense of parenthood: Children are associated with more joy than misery. Psychol. Sci. 2013, 24, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Browne, P.D.; Bossenbroek, R.; Kluft, A.; van Tetering, E.M.A.; de Weerth, C. Prenatal Anxiety and Depression: Treatment Uptake, Barriers, and Facilitators in Midwifery Care. J. Womens Health 2021, 30, 1116–1126. [Google Scholar] [CrossRef]
- Fontein-Kuipers, Y.; Ausems, M.; Budé, L.; Van Limbeek, E.; De Vries, R.; Nieuwenhuijze, M. Factors influencing maternal distress among Dutch women with a healthy pregnancy. Women Birth 2015, 28, e36–e43. [Google Scholar] [CrossRef]
- Loomans, E.M.; van Dijk, A.E.; Vrijkotte, T.G.M.; van Eijsden, M.; Stronks, K.; Gemke, R.J.; van Den Bergh, B.R. Psychosocial stress during pregnancy is related to adverse birth outcomes: Results from a large multi-ethnic community-based birth cohort. Eur. J. Public Health 2013, 23, 485–491. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Mapping global prevalence of depression among postpartum women. Transl. Psychiatry 2021, 11, 543. [Google Scholar] [CrossRef]
- Bartels, R.; Peçanha, T. HRV: A Pythonic package for Heart Rate Variability Analysis. J. Open Source Softw. 2020, 5, 1867. [Google Scholar] [CrossRef]
- Malik, M.; Camm, A.J. Heart rate variability. Clin. Cardiol. 1990, 13, 570–576. [Google Scholar] [CrossRef]
- Wang, Y.; Wei, S.; Zhang, S.; Zhang, Y.; Zhao, L.; Liu, C.; Murray, A. Comparison of time-domain, frequency-domain and non-linear analysis for distinguishing congestive heart failure patients from normal sinus rhythm subjects. Biomed. Signal Process. Control 2018, 42, 30–36. [Google Scholar] [CrossRef]
- Burton, A.R.; Rahman, K.; Kadota, Y.; Lloyd, A.; Vollmer-Conna, U. Reduced heart rate variability predicts poor sleep quality in a case-control study of chronic fatigue syndrome. Exp. Brain Res. 2010, 204, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Sajadieh, A.; Nielsen, O.W.; Rasmussen, V.; Hein, H.O.; Abedini, S.; Hansen, J.F. Increased heart rate and reduced heart-rate variability are associated with subclinical inflammation in middle-aged and elderly subjects with no apparent heart disease. Eur. Heart J. 2004, 25, 363–370. [Google Scholar] [CrossRef]
- Kim, H.G.; Cheon, E.J.; Bai, D.S.; Lee, Y.H.; Koo, B.H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, B.R.H. Maternal Anxiety, Mindfulness, and Heart Rate Variability During Pregnancy Influence Fetal and Infant Development. In Fetal Development: Research on Brain and Behavior, Environmental Influences, and Emerging Technologies [Internet]; Reissland, N., Kisilevsky, B.S., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 267–292. [Google Scholar] [CrossRef]
- Blood, J.D.; Wu, J.; Chaplin, T.M.; Hommer, R.; Vazquez, L.; Rutherford, H.J.V.; Mayes, L.C.; Crowley, M.J. The variable heart: High frequency and very low frequency correlates of depressive symptoms in children and adolescents. J. Affect Disord. 2015, 186, 119–126. [Google Scholar] [CrossRef]
- Kemp, A.H.; Quintana, D.S.; Gray, M.A.; Felmingham, K.L.; Brown, K.; Gatt, J.M. Impact of Depression and Antidepressant Treatment on Heart Rate Variability: A Review and Meta-Analysis. Biol. Psychiatry 2010, 67, 1067–1074. [Google Scholar] [CrossRef]
- Kemp, A.H.; Quintana, D.S.; Felmingham, K.L.; Matthews, S.; Jelinek, H.F. Depression, Comorbid Anxiety Disorders, and Heart Rate Variability in Physically Healthy, Unmedicated Patients: Implications for Cardiovascular Risk. PLoS ONE 2012, 7, e30777. [Google Scholar] [CrossRef]
- Kidwell, M.; Ellenbroek, B.A. Heart and soul: Heart rate variability and major depression. Behav. Pharmacol. 2018, 29, 152. [Google Scholar] [CrossRef]
- Sgoifo, A.; Carnevali, L.; de los Angeles Pico Alfonso, M.; Amore, M. Autonomic dysfunction and heart rate variability in depression. Stress 2015, 18, 343–352. [Google Scholar] [CrossRef]
- Yeh, M.L.; Chung, Y.C.; Hsu, L.C.; Hung, S.H. Effect of Transcutaneous Acupoint Electrical Stimulation on Post-Hemorrhoidectomy-Associated Pain, Anxiety, and Heart Rate Variability: A Randomized-Controlled Study. Clin. Nurs. Res. 2018, 27, 450–466. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Luecken, L.J. Heart Rate Variability as an Index of Regulated Emotional Responding. Rev. Gen. Psychol. 2006, 10, 229–240. [Google Scholar] [CrossRef]
- Bach, D.; Groesbeck, G.; Stapleton, P.; Sims, R.; Blickheuser, K.; Church, D. Clinical EFT (Emotional Freedom Techniques) Improves Multiple Physiological Markers of Health. J. Evid.-Based Integr. Med. 2019, 24, 2515690X18823691. [Google Scholar] [CrossRef] [PubMed]
- Liu, I.; Ni, S.; Peng, K. Happiness at Your Fingertips: Assessing Mental Health with Smartphone Photoplethysmogram-Based Heart Rate Variability Analysis. Telemed. e-Health 2020, 26, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.H.; Quintana, D.S. The relationship between mental and physical health: Insights from the study of heart rate variability. Int. J. Psychophysiol. 2013, 89, 288–296. [Google Scholar] [CrossRef]
- Porges, S.W. Cardiac vagal tone: A physiological index of stress. Neurosci. Biobehav. Rev. 1995, 19, 225–233. [Google Scholar] [CrossRef]
- Taylor, S.E.; Klein, L.C.; Lewis, B.P.; Gruenewald, T.L.; Gurung, R.A.R.; Updegraff, J.A. Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychol. Rev. 2000, 107, 411–429. [Google Scholar] [CrossRef]
- Taylor, A.F.; Kuo, F.E.; Sullivan, W.C. Views of Nature and Self-Discipline: Evidence from Inner City Children. J. Environ. Psychol. 2002, 22, 49–63. [Google Scholar] [CrossRef]
- Lampert, R.; Tuit, K.; Hong, K.I.; Donovan, T.; Lee, F.; Sinha, R. Cumulative stress and autonomic dysregulation in a community sample. Stress 2016, 19, 269–279. [Google Scholar] [CrossRef]
- Sin, N.L.; Sloan, R.P.; McKinley, P.S.; Almeida, D.M. Linking Daily Stress Processes and Laboratory-Based Heart Rate Variability in a National Sample of Midlife and Older Adults. Psychosom. Med. 2016, 78, 573. [Google Scholar] [CrossRef] [PubMed]
- Fogelman, N.; Schwartz, J.; Chaplin, T.M.; Jastreboff, A.M.; Silverman, W.K.; Sinha, R. Parent Stress and Trauma, Autonomic Responses, and Negative Child Behaviors. Child Psychiatry Hum. Dev. 2022, 54, 1779–1788. [Google Scholar] [CrossRef]
- Rådmark, L.; Osika, W.; Wallén, M.B.; Nissen, E.; Lönnberg, G.; Bränström, R.; Henje, E.; Gardner, R.; Fransson, E.; Karlsson, H.; et al. Autonomic function and inflammation in pregnant women participating in a randomized controlled study of Mindfulness Based Childbirth and Parenting. BMC Pregnancy Childbirth 2023, 23, 237. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Nakamura, Y.; Garcia, M.E.; Thompson, R.W.; Dunn, A.L.; Blair, S.N. Heart rate variability, trait anxiety, and perceived stress among physically fit men and women. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2000, 37, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Endukuru, C.; Tripathi, S. Evaluation of cardiac responses to Stress in healthy individuals A Non invasive evaluation by Heart Rate Variability and Stroop test. Int. J. Sci. Res. 2016, 5, 286–289. [Google Scholar]
- Uusitalo, A.; Mets, T.; Martinmäki, K.; Mauno, S.; Kinnunen, U.; Rusko, H. Heart rate variability related to effort at work. Appl. Ergon. 2011, 42, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Belsky, J. The determinants of parenting: A process model. Child Dev. 1984, 55, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, D.V.; Canavarro, M.C.; Moreira, H. The Mediating Role of Parenting Stress in the Relationship Between Anxious and Depressive Symptomatology, Mothers’ Perception of Infant Temperament, and Mindful Parenting During the Postpartum Period. Mindfulness 2021, 12, 275–290. [Google Scholar] [CrossRef]
- Oddi, K.B.; Murdock, K.W.; Vadnais, S.; Bridgett, D.J.; Gartstein, M.A. Maternal and Infant Temperament Characteristics as Contributors to Parenting Stress in the First Year Postpartum. Infant Child Dev. 2013, 22, 553–579. [Google Scholar] [CrossRef]
- Gregory, A.M.; Moffitt, T.E.; Ambler, A.; Arseneault, L.; Houts, R.M.; Caspi, A. Maternal insomnia and children’s family socialization environments. Sleep 2012, 35, 579–582. [Google Scholar] [CrossRef]
- McQuillan, M.E.; Bates, J.E.; Staples, A.D.; Deater Deckard, K. Maternal Stress, Sleep, and Parenting. J. Fam. Psychol. JFP J. Div. Fam. Psychol. Am. Psychol. Assoc. Div. 2019, 33, 349–359. [Google Scholar] [CrossRef]
- Yap, Y.; Slavish, D.C.; Taylor, D.J.; Bei, B.; Wiley, J.F. Bi-directional relations between stress and self-reported and actigraphy-assessed sleep: A daily intensive longitudinal study. Sleep 2020, 43, zsz250. [Google Scholar] [CrossRef]
- Farmer, A.Y.; Lee, S.K. The Effects of Parenting Stress, Perceived Mastery, and Maternal Depression on Parent–Child Interaction. J. Soc. Serv. Res. 2011, 37, 516–525. [Google Scholar] [CrossRef]
- Leigh, B.; Milgrom, J. Risk factors for antenatal depression, postnatal depression and parenting stress. BMC Psychiatry 2008, 8, 24. [Google Scholar] [CrossRef]
- Roberti, E.; Giacchero, R.; Grumi, S.; Biasucci, G.; Cuzzani, L.; Decembrino, L.; Magnani, M.L.; Motta, M.; Nacinovich, R.; Pisoni, C.; et al. Post-partum Women’s Anxiety and Parenting Stress: Home-Visiting Protective Effect During the COVID-19 Pandemic. Matern. Child Health J. 2022, 26, 2308–2317. [Google Scholar] [CrossRef]
- Krieg, D.B. Does Motherhood Get Easier the Second-Time Around? Examining Parenting Stress and Marital Quality Among Mothers Having Their First or Second Child. Parent. Sci. Pract. 2007, 7, 149–175. [Google Scholar] [CrossRef]
- Iwata, H.; Mori, E.; Sakajo, A.; Aoki, K.; Maehara, K.; Tamakoshi, K. Prevalence of postpartum depressive symptoms during the first 6 months postpartum: Association with maternal age and parity. J. Affect Disord. 2016, 203, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Bohne, A.; Nordahl, D.; Høifødt, R.S.; Moe, V.; Landsem, I.P.; Wang, C.E.A.; Pfuhl, G. Do parental cognitions during pregnancy predict bonding after birth in a low-risk sample? Front. Psychol. 2022, 13, 986757. [Google Scholar] [CrossRef]
- Spinhoven, P.; van Hemert, A.M.; Penninx, B.W. Repetitive negative thinking as a predictor of depression and anxiety: A longitudinal cohort study. J. Affect Disord. 2018, 241, 216–225. [Google Scholar] [CrossRef]
- Wahl, K.; Ehring, T.; Kley, H.; Lieb, R.; Meyer, A.; Kordon, A.; Heinzel, C.V.; Mazanec, M.; Schönfeld, S. Is repetitive negative thinking a transdiagnostic process? A comparison of key processes of RNT in depression, generalized anxiety disorder, obsessive-compulsive disorder, and community controls. J. Behav. Ther. Exp. Psychiatry 2019, 64, 45–53. [Google Scholar] [CrossRef]
- de Cock, E.S.A.; Henrichs, J.; Klimstra, T.A.; Maas, A.J.B.M.; Vreeswijk, C.M.J.M.; Meeus, W.H.J.; van Bakel, H.J.A. Longitudinal Associations Between Parental Bonding, Parenting Stress, and Executive Functioning in Toddlerhood. J. Child Fam. Stud. 2017, 26, 1723–1733. [Google Scholar] [CrossRef]
- Willinger, U.; Diendorfer-Radner, G.; Willnauer, R.; Jörgl, G.; Hager, V. Parenting stress and parental bonding. Parent. Stress Parent. Bonding. Behav. Med. 2005, 31, 63–69. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, J.A.; Bornstein, M.H.; Hahn, C.S.; Costigan, K.; Achy-Brou, A. Fetal heart rate and variability: Stability and prediction to developmental outcomes in early childhood. Child Dev. 2007, 78, 1788–1798. [Google Scholar] [CrossRef] [PubMed]
- Begum, M.; Ven Den Bergh, B.; Khan, M. Stress during pregnancy and its influence on the offspring’s heart rate: A physiological study. Int. J. Pharm. Biol. Sci. 2013, 3, 327–333. [Google Scholar]
- Eykens, H.; Widjaja, D.; Vanderperren, K.; Taelman, J.; Braeken, M.; Otte, R.A.; Van den Bergh, B.R.H.; Van Huffel, S. Phase-rectified signal averaging for the quantification of the influence of prenatal anxiety on heart rate variability of babies. In Proceedings of the International Conference on Bio-Inspired Systems and Signal Processing; SciTe Press: Setúbal, Portugal, 2012; pp. 163–168. [Google Scholar]
- Jacob, S.; Byrne, M.; Keenan, K. Neonatal physiological regulation is associated with perinatal factors: A study of neonates born to healthy African American women living in poverty. Infant Ment. Health J. 2009, 30, 82–94. [Google Scholar] [CrossRef]
- Braeken, M.A.K.A.; Kemp, A.H.; Outhred, T.; Otte, R.A.; Monsieur, G.J.Y.J.; Jones, A.; Van den Bergh, B.R. Pregnant Mothers with Resolved Anxiety Disorders and Their Offspring Have Reduced Heart Rate Variability: Implications for the Health of Children. PLoS ONE 2013, 8, e83186. [Google Scholar] [CrossRef]
- Huizink, A.C.; Mulder, E.J.H.; Robles de Medina, P.G.; Visser, G.H.A.; Buitelaar, J.K. Is pregnancy anxiety a distinctive syndrome? Early Hum. Dev. 2004, 79, 81–91. [Google Scholar] [CrossRef]
- Dunkel Schetter, C.; Tanner, L. Anxiety, depression and stress in pregnancy: Implications for mothers, children, research, and practice. Curr. Opin. Psychiatry 2012, 25, 141. [Google Scholar] [CrossRef]
- Dierckx, B.; Tulen, J.H.M.; van den Berg, M.P.; Tharner, A.; Jaddoe, V.W.; Moll, H.A.; Hofman, A.; Verhulst, F.C.; Tiemeier, H. Maternal Psychopathology Influences Infant Heart Rate Variability: Generation R Study. Psychosom. Med. 2009, 71, 313. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L.A.; Evans, L.; Monk, C. Effects of mothers’ prenatal psychiatric status and postnatal caregiving on infant biobehavioral regulation: Can prenatal programming be modified? Early Hum. Dev. 2008, 84, 249–256. [Google Scholar] [CrossRef]
- Jones, N.A.; Field, T.; Fox, N.A.; Davalos, M.; Lundy, B.; Hart, S. Newborns of mothers with depressive symptoms are physiologically less developed. Infant Behav. Dev. 1998, 21, 537–541. [Google Scholar] [CrossRef]
- De Meersman, R.E.; Stein, P.K. Vagal modulation and aging. Biol. Psychol. 2007, 74, 165–173. [Google Scholar] [CrossRef]
- Høifødt, R.S.; Nordahl, D.; Pfuhl, G.; Landsem, I.P.; Thimm, J.C.; Ilstad, L.K.K.; Wang, C.E.A. Protocol for the Northern babies longitudinal study: Predicting postpartum depression and improving parent–infant interaction with The Newborn Behavioral Observation. BMJ Open 2017, 7, e016005. [Google Scholar] [CrossRef]
- Bayley, N. Bayley Scales of Infant and Toddler Development. In Administration Manual; Psychorp: Washington, DC, USA, 2006. [Google Scholar]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Eberhard-Gran, M.; Eskild, A.; Tambs, K.; Schei, B.; Opjordsmoen, S. The Edinburgh Postnatal Depression Scale: Validation in a Norwegian community sample. Nord. J. Psychiatry 2001, 55, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Ehring, T.; Zetsche, U.; Weidacker, K.; Wahl, K.; Schönfeld, S.; Ehlers, A. The Perseverative Thinking Questionnaire (PTQ): Validation of a content-independent measure of repetitive negative thinking. J. Behav. Ther. Exp. Psychiatry 2011, 42, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Abidin, R.R. Parenting Stress Index: Manual, Administration Booklet, [and] Research Update; Pediatric Psychology Press: Charlottesville, VA, USA, 1983. [Google Scholar]
- Condon, J.T.; Corkindale, C.J. The assessment of parent-to-infant attachment: Development of a self-report questionnaire instrument. J. Reprod. Infant Psychol. 1998, 16, 57–76. [Google Scholar] [CrossRef]
- Urdal, J.; Engan, K.; Eftestøl, T.; Haaland, S.H.; Kamala, B.; Mdoe, P.; Kidanto, H.; Ersdal, H. Fetal heart rate development during labour. BioMedical Eng. OnLine 2021, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Brysbaert, M. How Many Participants Do We Have to Include in Properly Powered Experiments? A Tutorial of Power Analysis with Reference Tables. J. Cogn. 2019, 2, 16. [Google Scholar] [CrossRef]
- Ehring, T.; Ehlers, A. Does rumination mediate the relationship between emotion regulation ability and posttraumatic stress disorder? Eur. J. Psychotraumatology 2014, 5, 23547. [Google Scholar] [CrossRef]
- Brosschot, J.F.; Gerin, W.; Thayer, J.F. The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. J. Psychosom. Res. 2006, 60, 113–124. [Google Scholar] [CrossRef]
- Hummel, K.V.; Trautmann, S.; Venz, J.; Thomas, S.; Schäfer, J. Repetitive negative thinking: Transdiagnostic correlate and risk factor for mental disorders? A proof-of-concept study in German soldiers before and after deployment to Afghanistan. BMC Psychol. 2021, 9, 198. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S.; Wisco, B.E.; Lyubomirsky, S. Rethinking Rumination. Perspect. Psychol. Sci. 2008, 3, 400–424. [Google Scholar] [CrossRef] [PubMed]
- Watkins, E.R. Constructive and Unconstructive Repetitive Thought. Psychol. Bull. 2008, 134, 163–206. [Google Scholar] [CrossRef] [PubMed]
- Bohne, A.; Nordahl, D.; Lindahl, Å.; Ulvenes, P.; Wang, C.; Pfuhl, G. Emotional Infant Face Processing in Women with Major Depression and Expecting Parents with Depressive Symptoms. Front. Psychol. 2021, 12, 657269. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables (Timepoint) | n | Mean | SD | Min | Max | Median |
|---|---|---|---|---|---|---|
| Age | 111 | 30.93 | 4.01 | 20 | 40 | 31 |
| Marital status married/cohabiting /other | 111 32/78/1 | |||||
| Parity nulliparous/multiparous | 111 58/53 | |||||
| Education high school/BA/MA or higher | 111 13/35/63 | |||||
| Social support | 96 | 1.85 | 0.38 | 0 | 2 | 2 |
| PRAQ—fear of birth | 111 | 6.92 | 3.17 | 3 | 15 | 7.0 |
| PRAQ—fear for child | 111 | 10.89 | 3.98 | 4 | 20 | 11 |
| PRAQ—looks | 111 | 6.1 | 3.37 | 3 | 15 | 5 |
| PTQ | 111 | 17.72 | 9.60 | 0 | 47 | 17 |
| EPDS (T1) | 111 | 4.55 | 3.32 | 0 | 16 | 4 |
| EPDS (T5) | 96 | 3.65 | 3.39 | 0 | 13 | 3 |
| PSI-PD (T5) | 96 | 2.17 | 0.41 | 1.41 | 3.5 | 2.15 |
| PSI-CD (T5) | 96 | 1.84 | 0.33 | 1.21 | 3.26 | 1.83 |
| MPAS (T5) | 94 | 4.34 | 0.43 | 2.23 | 4.95 | 4.44 |
| HRV mother (sec) | 107 | 0.04 | 0.03 | 0.01 | 0.24 | 0.03 |
| HRV infant (sec) | 109 | 0.011 | 0.004 | 0.004 | 0.024 | 0.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parisi, F.; Høifødt, R.S.; Bohne, A.; Wang, C.E.A.; Pfuhl, G. Perceived Parenting Stress Is Related to Cardiac Flexibility in Mothers: Data from the NorBaby Study. Behav. Sci. 2024, 14, 117. https://doi.org/10.3390/bs14020117
Parisi F, Høifødt RS, Bohne A, Wang CEA, Pfuhl G. Perceived Parenting Stress Is Related to Cardiac Flexibility in Mothers: Data from the NorBaby Study. Behavioral Sciences. 2024; 14(2):117. https://doi.org/10.3390/bs14020117
Chicago/Turabian StyleParisi, Francesca, Ragnhild Sørensen Høifødt, Agnes Bohne, Catharina Elisabeth Arfwedson Wang, and Gerit Pfuhl. 2024. "Perceived Parenting Stress Is Related to Cardiac Flexibility in Mothers: Data from the NorBaby Study" Behavioral Sciences 14, no. 2: 117. https://doi.org/10.3390/bs14020117
APA StyleParisi, F., Høifødt, R. S., Bohne, A., Wang, C. E. A., & Pfuhl, G. (2024). Perceived Parenting Stress Is Related to Cardiac Flexibility in Mothers: Data from the NorBaby Study. Behavioral Sciences, 14(2), 117. https://doi.org/10.3390/bs14020117