
Thriving Beyond Adversity: A Prospective Longitudinal Cohort Study Using a Strength-Based Approach Depicts Indigenous Adolescents with Less Adverse Childhood Experiences (ACEs) Had Fewer Neurodevelopmental Disorders (NDDs)
 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Data Source and Study Design
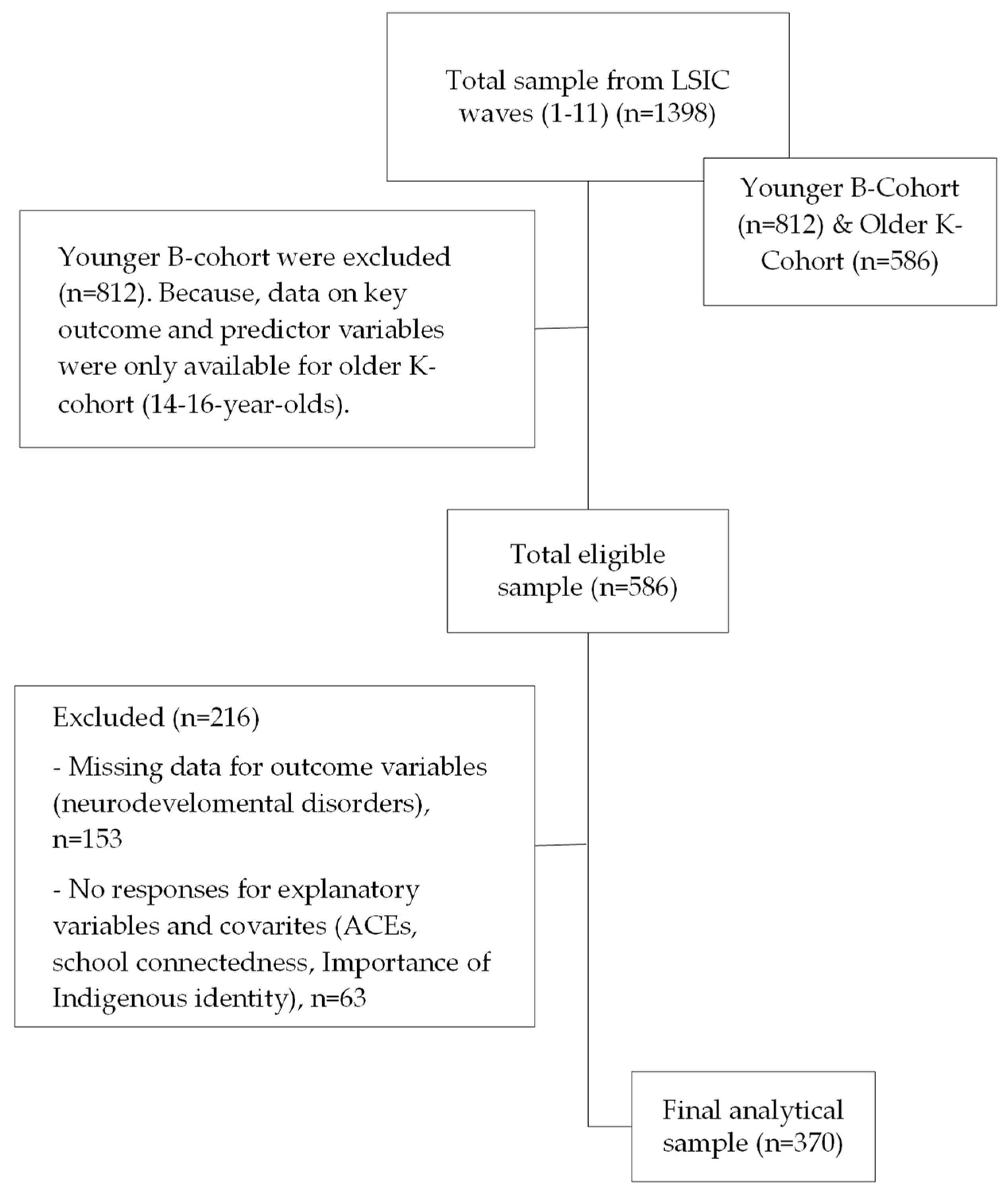
2.2. Participants and Sample Selection
2.3. Measures
2.4. Cultural Integrity
2.5. Statistical Analysis
2.6. Ethics Approval
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Commonwealth of Australia. National Strategic Framework for Aboriginal and Torres Strait Islander Peoples’ Mental Health and Social and Emotional Wellbeing; Commonwealth of Australia: Canberra, Australia, 2017; pp. 1–52. [Google Scholar]
- Islam, M.I.; Sharwood, L.; Chadwick, V.; Esgin, T.; Martiniuk, A. Protective Factors against Self-Harm and Suicidality among Australian Indigenous Adolescents: A Strengths-Based Analysis of the Longitudinal Study of Indigenous Children. Int. J. Environ. Res. Public Health 2022, 19, 9131. [Google Scholar] [CrossRef] [PubMed]
- Radford, A.; Toombs, E.; Zugic, K.; Boles, K.; Lund, J.; Mushquash, C.J. Examining Adverse Childhood Experiences (ACEs) within Indigenous Populations: A Systematic Review. J. Child Adolesc. Trauma 2022, 15, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Maegan Rides at the Door; Shaw, S. The Other Side of the ACEs Pyramid: A Healing Framework for Indigenous Communities. Int. J. Environ. Res. Public Health 2023, 20, 4108. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander Health Survey. In Aboriginal and Torres Strait Islander Peoples; ABS, Ed.; Australian Bureau of Statistics: Canberra, Australia, 2018–2019. [Google Scholar]
- Australian Institute of Health and Welfare. Australian Burden of Disease Study 2018: Interactive Data on Risk Factor Burden Among Aboriginal and Torres Strait Islander People; AIHW: Canberra, Australia, 2022.
- Coalition of Peaks. National Agreement on Closing the Gap; Coalition of Peaks, Ed.; Coalition of Peaks: Canberra, Australia, 2020. [Google Scholar]
- Australian Government Department of Health. National Aboriginal and Torres Strait Islander Health Plan 2021–2031; Australian Government Department of Health, Ed.; Commonwealth of Australia as Represented by the Department of Health: Canberra, Australia, 2021.
- Darwin, L.; Vervoort, S.; Vollert, E.; Blustein, S. Intergenerational Trauma and Mental Health; Australian Institute of Health and Welfare, Ed.; Australian Institute of Health and Welfare: Canberra, Australia, 2023.
- Hopkins, K.D.; Taylor, C.L.; Zubrick, S.R. Psychosocial resilience and vulnerability in Western Australian Aboriginal youth. Child Abus. Negl. 2018, 78, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Australia’s Children; AIHW: Canberra, Australia, 2022.
- Paul, J.; McQuaid, R.J.; Hopkins, C.; Perri, A.; Stewart, S.; Matheson, K.; Anisman, H.; Bombay, A. Relations between bullying and distress among youth living in First Nations communities: Assessing direct and moderating effects of culture-related variables. Transcult. Psychiatry 2024, 61, 429–439. [Google Scholar] [CrossRef]
- Luke, C.R.; Benfer, K.; Mick-Ramsamy, L.; Ware, R.S.; Reid, N.; Bos, A.F.; Bosanquet, M.; Boyd, R.N. Early detection of Australian Aboriginal and Torres Strait Islander infants at high risk of adverse neurodevelopmental outcomes at 12 months corrected age: LEAP-CP prospective cohort study protocol. BMJ Open 2022, 12, e053646. [Google Scholar] [CrossRef]
- Mullin, A.P.; Gokhale, A.; Moreno-De-Luca, A.; Sanyal, S.; Waddington, J.L.; Faundez, V. Neurodevelopmental disorders: Mechanisms and boundary definitions from genomes, interactomes and proteomes. Transl. Psychiatry 2013, 3, e329. [Google Scholar] [CrossRef]
- Zubrick, S.; Lawrence, D.; Silburn, S.; Blair, E.; Milroy, H.; Wilkes, T.; Eades, S.; D’Antoine, H.; Read, A.; Ishiguchi, P.; et al. The Western Australian Aboriginal Child Health Survey: The Health of Aboriginal Children and Young People; Telethon Institute for Child Health Research: Perth, Australia, 2004; Volume 1. [Google Scholar]
- Bourke, J.; Nembhard, W.N.; Wong, K.; Leonard, H. Twenty-Five Year Survival of Children with Intellectual Disability in Western Australia. J. Pediatr. 2017, 188, 232–239.e232. [Google Scholar] [CrossRef]
- Blair, E.; Watson, L.; O’Kearney, E.; D’Antoine, H.; Delacy, M.J.; Group, T.A.C.P.R. Comparing risks of cerebral palsy in births between Australian Indigenous and non-Indigenous mothers. Dev. Med. Child Neurol. 2016, 58, 36–42. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. America’s Children and the Environment, 3rd ed.; U.S. Environmental Protection Agency: Washington, DC, USA, 2015.
- Productivity Commission. Closing the Gap Annual Data Compilation Report July 2023; Australian Government Productivity Commission: Canberra, Australia, 2023.
- Bailey, B.; Arciuli, J. Indigenous Australians with autism: A scoping review. Autism 2020, 24, 1031–1046. [Google Scholar] [CrossRef]
- Lau, S.; Czuczman, N.; Dennett, L.; Hicks, M.; Ospina, M. 72 Prevalence of Neurodevelopmental Disorder among Indigenous Children: A Systematic Review. Paediatr. Child Health 2022, 27, e34. [Google Scholar] [CrossRef]
- Australian Medical Association. Aboriginal and Torres Strait Islander Health Report Card 2012–2013: The Healthy Early Years—Getting the Right Start in Life; Australian Medical Association: Canberra, Australia, 2013. [Google Scholar]
- Bourgeron, T. What Do We Know about Early Onset Neurodevelopmental Disorders? In Translational Neuroscience: Toward New Therapies [Internet]; Nikolich, K., Hyman, S.E., Eds.; MIT Press: Cambridge, MA, USA, 2015. [Google Scholar]
- Van Hus, J.W.; Potharst, E.S.; Jeukens-Visser, M.; Kok, J.H.; van Wassenaer-Leemhuis, A.G. Motor impairment in very preterm-born children: Links with other developmental deficits at 5 years of age. Dev. Med. Child Neurol. 2014, 56, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, T.; Molander, F.; Taylor, M.J.; Jonsson, U.; Bölte, S. Early environmental risk factors for neurodevelopmental disorders—A systematic review of twin and sibling studies. Dev. Psychopathol. 2021, 33, 1448–1495. [Google Scholar] [CrossRef] [PubMed]
- Gibberd, A.J.; Simpson, J.M.; Jones, J.; Williams, R.; Stanley, F.; Eades, S.J. A large proportion of poor birth outcomes among Aboriginal Western Australians are attributable to smoking, alcohol and substance misuse, and assault. BMC Pregnancy Childbirth 2019, 19, 110. [Google Scholar] [CrossRef] [PubMed]
- Westrupp, E.M.; D’Esposito, F.; Freemantle, J.; Mensah, F.K.; Nicholson, J.M. Health outcomes for Australian Aboriginal and Torres Strait Islander children born preterm, low birthweight or small for gestational age: A nationwide cohort study. PLoS ONE 2019, 14, e0212130. [Google Scholar] [CrossRef] [PubMed]
- Kildea, S.; Tracy, S.; Sherwood, J.; Magick-Dennis, F.; Barclay, L. Improving maternity services for Indigenous women in Australia: Moving from policy to practice. Med. J. Aust. 2016, 205, 374–379. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Adverse Childhood Experiences International Questionnaire (ACE-IQ). Available online: https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq) (accessed on 27 September 2023).
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- CDC. Adverse Childhood Experiences (ACEs) Preventing Early Trauma to Improve Adult Health. Available online: https://www.cdc.gov/vitalsigns/aces/index.html (accessed on 23 April 2024).
- Boullier, M.; Blair, M. Adverse childhood experiences. Paediatr. Child Health 2018, 28, 132–137. [Google Scholar] [CrossRef]
- Twizeyemariya, A.; Guy, S.; Furber, G.; Segal, L. Risks for Mental Illness in Indigenous Australian Children: A Descriptive Study Demonstrating High Levels of Vulnerability. Milbank Q. 2017, 95, 319–357. [Google Scholar] [CrossRef]
- Zhang, N.; Gao, M.; Yu, J.; Zhang, Q.; Wang, W.; Zhou, C.; Liu, L.; Sun, T.; Liao, X.; Wang, J. Understanding the association between adverse childhood experiences and subsequent attention deficit hyperactivity disorder: A systematic review and meta-analysis of observational studies. Brain Behav. 2022, 12, e32748. [Google Scholar] [CrossRef]
- Minnis, H. Abuse, neglect and neurodevelopment across the life course: What can paediatricians and child psychiatrists do about this together? The Illingworth-Rees keynote lecture 2023. Arch. Dis. Child. 2024, 109, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Isaacs, A.N. Profile of transcultural patients in a regional Child and Adolescent Mental Health Service in Gippsland, Australia: The need for a multidimensional understanding of the complexities. Int. J. Soc. Psychiatry 2019, 65, 217–224. [Google Scholar] [CrossRef] [PubMed]
- D’Antoine, M.; Malvaso, C.; Delfabbro, P.; O’Connor, J. Suicidal behaviour in Aboriginal and non-Aboriginal young men under custodial youth justice supervision: Understanding the role of adverse childhood experiences. Psychiatry Psychol. Law 2022, 29, 953–975. [Google Scholar] [CrossRef] [PubMed]
- Zarei, K.; Xu, G.; Zimmerman, B.; Giannotti, M.; Strathearn, L. Adverse Childhood Experiences Predict Common Neurodevelopmental and Behavioral Health Conditions among U.S. Children. Children 2021, 8, 761. [Google Scholar] [CrossRef] [PubMed]
- Gajwani, R.; Minnis, H. Double jeopardy: Implications of neurodevelopmental conditions and adverse childhood experiences for child health. Eur. Child Adolesc. Psychiatry 2023, 32, 1–4. [Google Scholar] [CrossRef]
- Lacey, R.E.; Minnis, H. Practitioner Review: Twenty years of research with adverse childhood experience scores—Advantages, disadvantages and applications to practice. J. Child Psychol. Psychiatry 2020, 61, 116–130. [Google Scholar] [CrossRef]
- Brown, D.W.; Anda, R.F.; Felitti, V.J.; Edwards, V.J.; Malarcher, A.M.; Croft, J.B.; Giles, W.H. Adverse childhood experiences are associated with the risk of lung cancer: A prospective cohort study. BMC Public Health 2010, 10, 20. [Google Scholar] [CrossRef]
- Chanlongbutra, A.; Singh, G.K.; Mueller, C.D. Adverse Childhood Experiences, Health-Related Quality of Life, and Chronic Disease Risks in Rural Areas of the United States. J. Environ. Public Health 2018, 2018, 7151297. [Google Scholar] [CrossRef]
- Gilbert, L.K.; Breiding, M.J.; Merrick, M.T.; Thompson, W.W.; Ford, D.C.; Dhingra, S.S.; Parks, S.E. Childhood adversity and adult chronic disease: An update from ten states and the District of Columbia, 2010. Am. J. Prev. Med. 2015, 48, 345–349. [Google Scholar] [CrossRef]
- Li, L.; Manor, O.; Power, C. Early environment and child-to-adult growth trajectories in the 1958 British birth cohort. Am. J. Clin. Nutr. 2004, 80, 185–192. [Google Scholar] [CrossRef]
- Oh, D.L.; Jerman, P.; Silvério Marques, S.; Koita, K.; Purewal Boparai, S.K.; Burke Harris, N.; Bucci, M. Systematic review of pediatric health outcomes associated with childhood adversity. BMC Pediatr. 2018, 18, 83. [Google Scholar] [CrossRef] [PubMed]
- Prehn, J.; Baltra-Ulloa, J.; Canty, J.; Williamson, M. What Is the Best Thing About Being an Indigenous Father in Australia? Aust. Soc. Work 2022, 75, 358–371. [Google Scholar] [CrossRef]
- Thurber, K.A.; Thandrayen, J.; Banks, E.; Doery, K.; Sedgwick, M.; Lovett, R. Strengths-based approaches for quantitative data analysis: A case study using the Australian Longitudinal Study of Indigenous Children. SSM-Popul. Health 2020, 12, 100637. [Google Scholar] [CrossRef] [PubMed]
- Thurber, K.A.; Banks, E.; Banwell, C. Cohort Profile: Footprints in Time, the Australian Longitudinal Study of Indigenous Children. Int. J. Epidemiol. 2015, 44, 789–800. [Google Scholar] [CrossRef] [PubMed]
- Department of Social Services. Footprints in Time: The Longitudinal Study of Indigenous Children—Data User Guide; Department of Social Services, Australian Government: Canberra, Australia, 2022.
- Hewitt, B. The Longitudinal Study of Indigenous Children: Implications of the Study Design for Analysis and Results; The University of Queensland, Institute for Social Science Research: St. Lucia, Australia, 2012. [Google Scholar]
- Hunt, T.K.A.; Slack, K.S.; Berger, L.M. Adverse childhood experiences and behavioral problems in middle childhood. Child Abus. Negl. 2017, 67, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, G.; Anme, T. Adverse Childhood Experiences, Resilience, and Emotional Problems in Young Chinese Children. Int. J. Environ. Res. Public Health 2023, 20, 3028. [Google Scholar] [CrossRef] [PubMed]
- Harfield, S.; Pearson, O.; Morey, K.; Kite, E.; Canuto, K.; Glover, K.; Gomersall, J.S.; Carter, D.; Davy, C.; Aromataris, E.; et al. Assessing the quality of health research from an Indigenous perspective: The Aboriginal and Torres Strait Islander quality appraisal tool. BMC Med. Res. Methodol. 2020, 20, 79. [Google Scholar] [CrossRef]
- Cohen, G.L.; Sherman, D.K. The Psychology of Change: Self-Affirmation and Social Psychological Intervention. Annu. Rev. Psychol. 2014, 65, 333–371. [Google Scholar] [CrossRef]
- Fuller-Thomson, E.; Hooper, S.R. The Association Between Childhood Physical Abuse and Dyslexia:Findings From a Population-Based Study. J. Interpers. Violence 2015, 30, 1583–1592. [Google Scholar] [CrossRef]
- Kenney, M.K.; Singh, G.K. Adverse Childhood Experiences among American Indian/Alaska Native Children: The 2011-2012 National Survey of Children’s Health. Scientifica 2016, 2016, 7424239. [Google Scholar] [CrossRef]
- Koponen, A.M.; Nissinen, N.-M.; Gissler, M.; Autti-Rämö, I.; Kahila, H.; Sarkola, T. Adverse childhood experiences and neurodevelopmental disorders among youth with and without prenatal substance exposure: A longitudinal matched register-based cohort study. Nord. Stud. Alcohol Drugs 2023, 40, 176–198. [Google Scholar] [CrossRef] [PubMed]
- Ketheesan, S.; Rinaudo, M.; Berger, M.; Wenitong, M.; Juster, R.P.; McEwen, B.S.; Sarnyai, Z. Stress, allostatic load and mental health in Indigenous Australians. Stress 2020, 23, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Sarnyai, Z.; Berger, M.; Jawan, I. Allostatic load mediates the impact of stress and trauma on physical and mental health in Indigenous Australians. Australas. Psychiatry 2016, 24, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Macedo, D.M.; Smithers, L.G.; Roberts, R.M.; Paradies, Y.; Jamieson, L.M. Effects of racism on the socio-emotional wellbeing of Aboriginal Australian children. Int. J. Equity Health 2019, 18, 132. [Google Scholar] [CrossRef] [PubMed]
- Currie, C.L.; Copeland, J.L.; Metz, G.A. Childhood racial discrimination and adult allostatic load: The role of Indigenous cultural continuity in allostatic resiliency. Soc. Sci. Med. 2019, 241, 112564. [Google Scholar] [CrossRef] [PubMed]
- Strathearn, L.; Giannotti, M.; Mills, R.; Kisely, S.; Najman, J.; Abajobir, A. Long-term Cognitive, Psychological, and Health Outcomes Associated With Child Abuse and Neglect. Pediatrics 2020, 146, e20200438. [Google Scholar] [CrossRef]
- Child Welfare Information Gateway. Protective Factors Approaches in Child Welfare; U.S. Department of Health and Human Services: Washington, DC, USA, 2020.
- Ortiz, R. Building Resilience Against the Sequelae of Adverse Childhood Experiences: Rise Up, Change Your Life, and Reform Health Care. Am. J. Lifestyle Med. 2019, 13, 470–479. [Google Scholar] [CrossRef]
- Conching, A.K.S.; Thayer, Z. Biological pathways for historical trauma to affect health: A conceptual model focusing on epigenetic modifications. Soc. Sci. Med. 2019, 230, 74–82. [Google Scholar] [CrossRef]
- Haque, A.; Tasnim, A.; Islam, S.; Towhid, M.; Sultana, S.; Salwa, M.; Barman, N.; Siddique, S. Mother’s Adverse Childhood Experiences and Elevated Risk of Neuro-developmental Disorders in Offspring: A Case-Control Study. Advers. Resil. Sci. 2021, 2, 1–10. [Google Scholar] [CrossRef]
- Roberts, A.L.; Liew, Z.; Lyall, K.; Ascherio, A.; Weisskopf, M.G. Association of Maternal Exposure to Childhood Abuse With Elevated Risk for Attention Deficit Hyperactivity Disorder in Offspring. Am. J. Epidemiol. 2018, 187, 1896–1906. [Google Scholar] [CrossRef]
- Mehari, K.; Iyengar, S.; Schneider, M.; Berg, K.; Bennett, A. Adverse Childhood Experiences Among Children with Neurodevelopmental Delays: Relations to Diagnoses, Behavioral Health, and Clinical Severity. J. Clin. Psychol. Med. Settings 2021, 28, 808–814. [Google Scholar] [CrossRef] [PubMed]
- De Giambattista, C.; Ventura, P.; Trerotoli, P.; Margari, F.; Margari, L. Sex Differences in Autism Spectrum Disorder: Focus on High Functioning Children and Adolescents. Front. Psychiatry 2021, 12, 539835. [Google Scholar] [CrossRef] [PubMed]
- National Center on Birth Defects and Developmental Disabilities, Centres for Disease Control and Prevention. Data & Statistics on Autism Spectrum Disorder; U.S. Department of Health and Human Services, Ed.; National Center on Birth Defects and Developmental Disabilities, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2023.
- Crouch, E.; Radcliff, E.; Bennett, K.J.; Brown, M.J.; Hung, P. Examining the Relationship Between Adverse Childhood Experiences and ADHD Diagnosis and Severity. Acad. Pediatr. 2021, 21, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Baidawi, S.; Piquero, A.R. Neurodisability among Children at the Nexus of the Child Welfare and Youth Justice System. J. Youth Adolesc. 2021, 50, 803–819. [Google Scholar] [CrossRef]
- Bath, K.G. Synthesizing Views to Understand Sex Differences in Response to Early Life Adversity. Trends Neurosci. 2020, 43, 300–310. [Google Scholar] [CrossRef]
- Hull, L.; Mandy, W. Protective effect or missed diagnosis? Females with autism spectrum disorder. Future Neurol. 2017, 12, 159–169. [Google Scholar] [CrossRef]
- Lai, M.-C.; Lin, H.-Y.; Ameis, S.H. Towards equitable diagnoses for autism and attention-deficit/hyperactivity disorder across sexes and genders. Curr. Opin. Psychiatry 2022, 35, 90–100. [Google Scholar] [CrossRef]
- Fatima, Y.; Cleary, A.; King, S.; Solomon, S.; McDaid, L.; Hasan, M.M.; Al Mamun, A.; Baxter, J. Cultural Identity and Social and Emotional Wellbeing in Aboriginal and Torres Strait Islander Children. In Family Dynamics over the Life Course: Foundations, Turning Points and Outcomes; Baxter, J., Lam, J., Povey, J., Lee, R., Zubrick, S.R., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 57–70. [Google Scholar]
- Barker, B.; Goodman, A.; DeBeck, K. Reclaiming Indigenous identities: Culture as strength against suicide among Indigenous youth in Canada. Can. J. Public Health 2017, 108, e208–e210. [Google Scholar] [CrossRef]
- Shepherd, S.M.; Delgado, R.H.; Sherwood, J.; Paradies, Y. The impact of indigenous cultural identity and cultural engagement on violent offending. BMC Public Health 2017, 18, 50. [Google Scholar] [CrossRef]
- MacLean, S.; Ritte, R.; Thorpe, A.; Ewen, S.; Arabena, K. Health and wellbeing outcomes of programs for Indigenous Australians that include strategies to enable the expression of cultural identities: A systematic review. Aust. J. Prim. Health 2017, 23, 309–318. [Google Scholar] [CrossRef]
- Khanlou, N.; Bender, A.; Mill, C.; Vazquez, L.M.; Rojas, L. Youth Experiences of Cultural Identity and Migration: A Systems Perspective. In Today’s Youth and Mental Health; Springer International Publishing: Cham, Switzerland; Toronto, ON, Canada, 2018; pp. 57–76. [Google Scholar]
- Martin, K.L. Culture and Identity: LSIC Parents’ Beliefs and Values and Raising Young Indigenous Children in the Twenty-First Century. In Indigenous Children Growing up Strong: A Longitudinal Study of Aboriginal and Torres Strait Islander Families; Walter, M., Martin, K.L., Bodkin-Andrews, G., Eds.; Palgrave Macmillan: London, UK, 2017; pp. 79–99. [Google Scholar]
- Kirmayer, L.J.; Brass, G.M.; Tait, C.L. The mental health of Aboriginal peoples: Transformations of identity and community. Can. J. Psychiatry 2000, 45, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Loh, P.-R.; Hayden, G.; Vicary, D.; Mancini, V.; Martin, N.; Piek, J.P. Attention Deficit Hyperactivity Disorder: An Aboriginal perspective on diagnosis and intervention. J. Trop. Psychol. 2017, 7, e2. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables 1 | Description of Variables |
|---|---|
| Outcome variables | |
| Neurodevelopmental disorders | Whether the study child was diagnosed with any neurodevelopmental disorders such as autism, ADHD, intellectual, neurological, psychiatric, and specific learning disabilities. Response options were categorised as ‘Yes’ (coded 0) and ‘No’ (coded 1). |
| Main explanatory variable | |
| Adverse childhood experiences (ACEs) | We created a composite score from five types of ACEs (highest score 5 and lowest score 0) and then categorised them into two: study children experienced 3–5 ACEs termed as ‘multiple ACEs’ (coded 0), while children with zero/one ACE termed as ‘No/Limited ACE’ (coded 1). The included ACEs were: biological parents had split up, family violence, parents/close family members mugged/robbed/assaulted, parents/close family members arrested/jailed, and study child bullied because of Indigeneity. |
| Covariates | |
| Age | Age was used as a continuous variable |
| Sex | The sex of the adolescents was categorised into ‘Boys’ (coded as 0) and ‘Girls’ (coded as 1). |
| Area of residence | The Australian Statistical Geography Standard (ASGS) classifies Remoteness Areas into five categories of relative remoteness across the country: Major Cities of Australia, Inner Regional Australia, Outer Regional Australia, Remote Australia, and Very Remote Australia [37]. From the responses, we created a binary variable, ‘Area of Residence’: ‘major cities’ were coded as ‘1’, and ‘inner regional’, ‘outer regional’, ‘remote’, and ‘very remote’ were combined as ‘regional/remote’ (coded as 0). |
| IRSEO index | The Indigenous Relative Socioeconomic Outcomes (IRSEO) index is comprised of socioeconomic outcomes (i.e., employment, education, income, and housing) and is used to estimate the socioeconomic status of Indigenous Australians living in each Indigenous area in Australia. The lowest IRSEO index (Quintile 1, 0–20%) signifies the most disadvantaged, and the highest IRSEO index (Quintile 5, 80–100%) indicates the most advantaged at the Indigenous area level. In this study, we categorised the IRSEO index into three: disadvantaged (quintile 1 + 2), average (quintile 3), and advantaged group (quintile 3 + 4). |
| School connectedness | Categorised into two categories: ‘Not much connected’ (coded as 0) and ‘Strongly connected’ (coded as 1). School connectedness was measured by whether the study child was good at school, made friends easily at school, did schoolwork, felt strong at school, and knew where/when to go at school. |
| Indigenous identity | Categorised into ‘Not so important’ (coded as 0) and ‘Important’ (coded as 1). According to the National Strategic Framework of Health for Indigenous Australians, Indigenous identity is one of the vital components of SEWB. |
| n (370) | % | |
|---|---|---|
| Age 1 | Mean = 15.05, SD = 0.44 | |
| Gender | ||
| Boys | 190 | 51.4 |
| Girls | 180 | 48.7 |
| Area of residence | ||
| Regional/Remote | 267 | 72.2 |
| Urban | 103 | 27.8 |
| Indigenous socioeconomic status | ||
| Disadvantaged | 111 | 30.0 |
| Average | 96 | 26.0 |
| Advantaged | 163 | 44.1 |
| School connectedness | ||
| Not much connected | 109 | 29.5 |
| Strongly connected | 261 | 70.5 |
| Indigenous cultural identity | ||
| Not important | 99 | 26.8 |
| Important | 271 | 73.2 |
| Main explanatory variable | ||
| ACEs | ||
| Multiple (2 or more ACEs) | 267 | 72.2 |
| Limited (0 to 1 ACE) | 103 | 27.8 |
| Outcome variable | ||
| Neurodevelopmental disorders (NDDs) | ||
| Yes | 26 | 7.0 |
| No | 344 | 93.0 |
| Neurodevelopmental Disorders (NDDs) | ||
|---|---|---|
| Unadjusted OR (95% CI) | Adjusted # OR (95% CI) | |
| ACEs | ||
| Multiple (2 or more ACEs) | Ref. | Ref. |
| Limited (0 to 1 ACE) | 5.22 * (1.18, 23.09) | 6.01 * (1.26, 28.61) |
| Age | ||
| Mean | 1.07 (0.36, 3.20) | - |
| Gender | ||
| Boys | Ref. | Ref. |
| Girls | 12.99 ** (2.99, 56.31) | 13.88 ** (3.06, 62.84) |
| Area of residence | ||
| Regional/Remote | Ref. | - |
| Urban | 0.97 (0.32, 2.95) | - |
| Indigenous socioeconomic status | ||
| Disadvantaged | Ref. | - |
| Average | 0.58 (0.12, 2.74) | - |
| Advantaged | 1.28 (0.27, 6.03) | - |
| School connectedness | ||
| Not much connected | Ref. | - |
| Strongly connected | 2.78 (0.95, 8.10) | - |
| Indigenous cultural identity | ||
| Not important | Ref. | Ref. |
| Important | 2.80 * (1.16, 6.75) | 2.81 * (1.06, 7.39) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.I.; Lam, B.Y.Y.; Esgin, T.; Martiniuk, A. Thriving Beyond Adversity: A Prospective Longitudinal Cohort Study Using a Strength-Based Approach Depicts Indigenous Adolescents with Less Adverse Childhood Experiences (ACEs) Had Fewer Neurodevelopmental Disorders (NDDs). Behav. Sci. 2024, 14, 1047. https://doi.org/10.3390/bs14111047
Islam MI, Lam BYY, Esgin T, Martiniuk A. Thriving Beyond Adversity: A Prospective Longitudinal Cohort Study Using a Strength-Based Approach Depicts Indigenous Adolescents with Less Adverse Childhood Experiences (ACEs) Had Fewer Neurodevelopmental Disorders (NDDs). Behavioral Sciences. 2024; 14(11):1047. https://doi.org/10.3390/bs14111047
Chicago/Turabian StyleIslam, Md Irteja, Bernadette Yan Yue Lam, Tuguy Esgin, and Alexandra Martiniuk. 2024. "Thriving Beyond Adversity: A Prospective Longitudinal Cohort Study Using a Strength-Based Approach Depicts Indigenous Adolescents with Less Adverse Childhood Experiences (ACEs) Had Fewer Neurodevelopmental Disorders (NDDs)" Behavioral Sciences 14, no. 11: 1047. https://doi.org/10.3390/bs14111047
APA StyleIslam, M. I., Lam, B. Y. Y., Esgin, T., & Martiniuk, A. (2024). Thriving Beyond Adversity: A Prospective Longitudinal Cohort Study Using a Strength-Based Approach Depicts Indigenous Adolescents with Less Adverse Childhood Experiences (ACEs) Had Fewer Neurodevelopmental Disorders (NDDs). Behavioral Sciences, 14(11), 1047. https://doi.org/10.3390/bs14111047