
The Fibromyalgia Decomposition Phenomenon: A Reflexive Thematic Analysis

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Qualitative Approach and Research Paradigm
2.2. Researcher Characteristics and Reflexivity
2.3. Context
2.4. Sampling Strategy
2.5. Ethical Issues Pertaining to Human Subjects
2.6. Data Collection Methods
2.7. Data Collection Instruments and Technologies
2.8. Data Processing
2.9. Data Analysis
2.10. Techniques to Enhance Trustworthiness
3. Results
3.1. Description of Participants
3.2. Themes
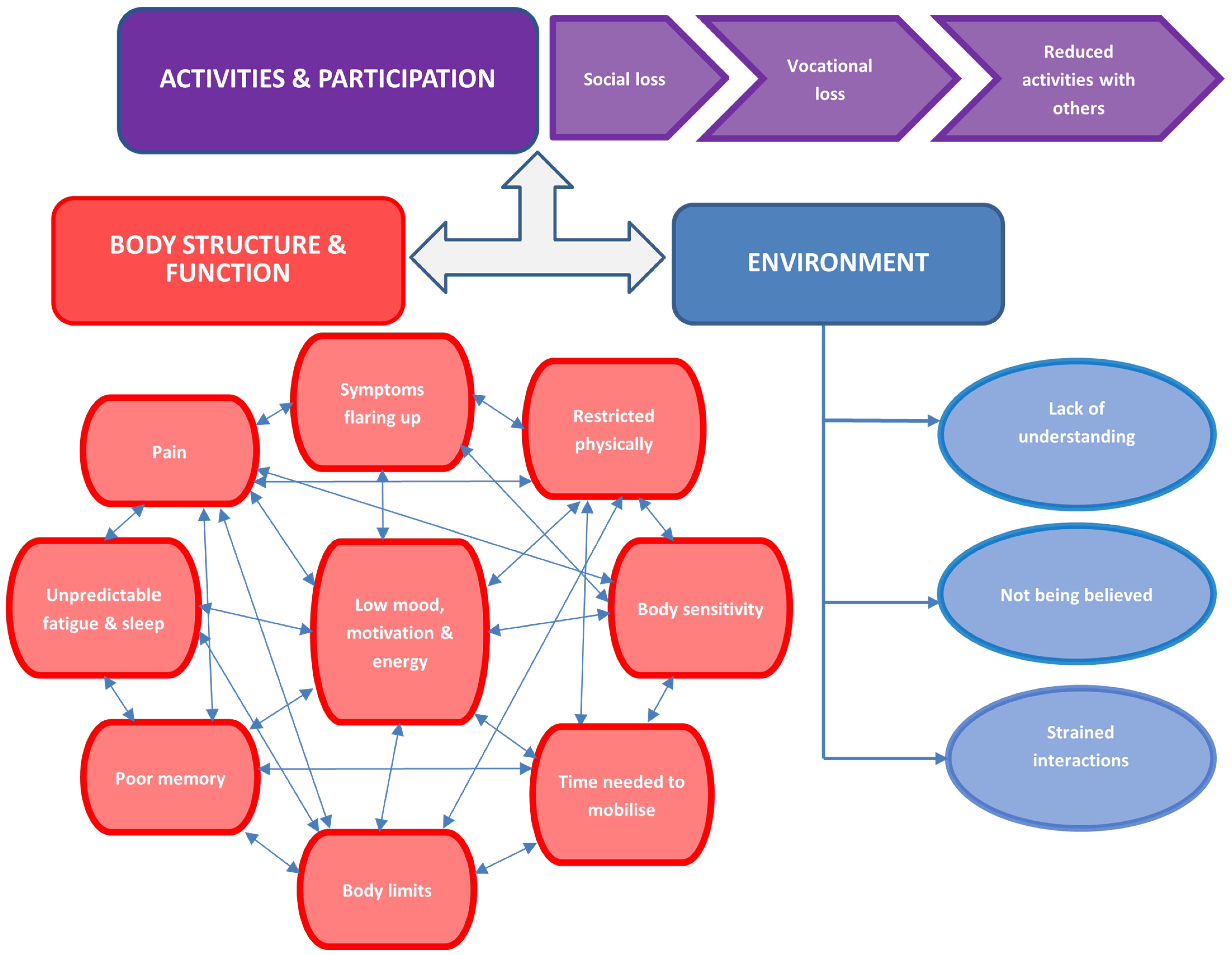
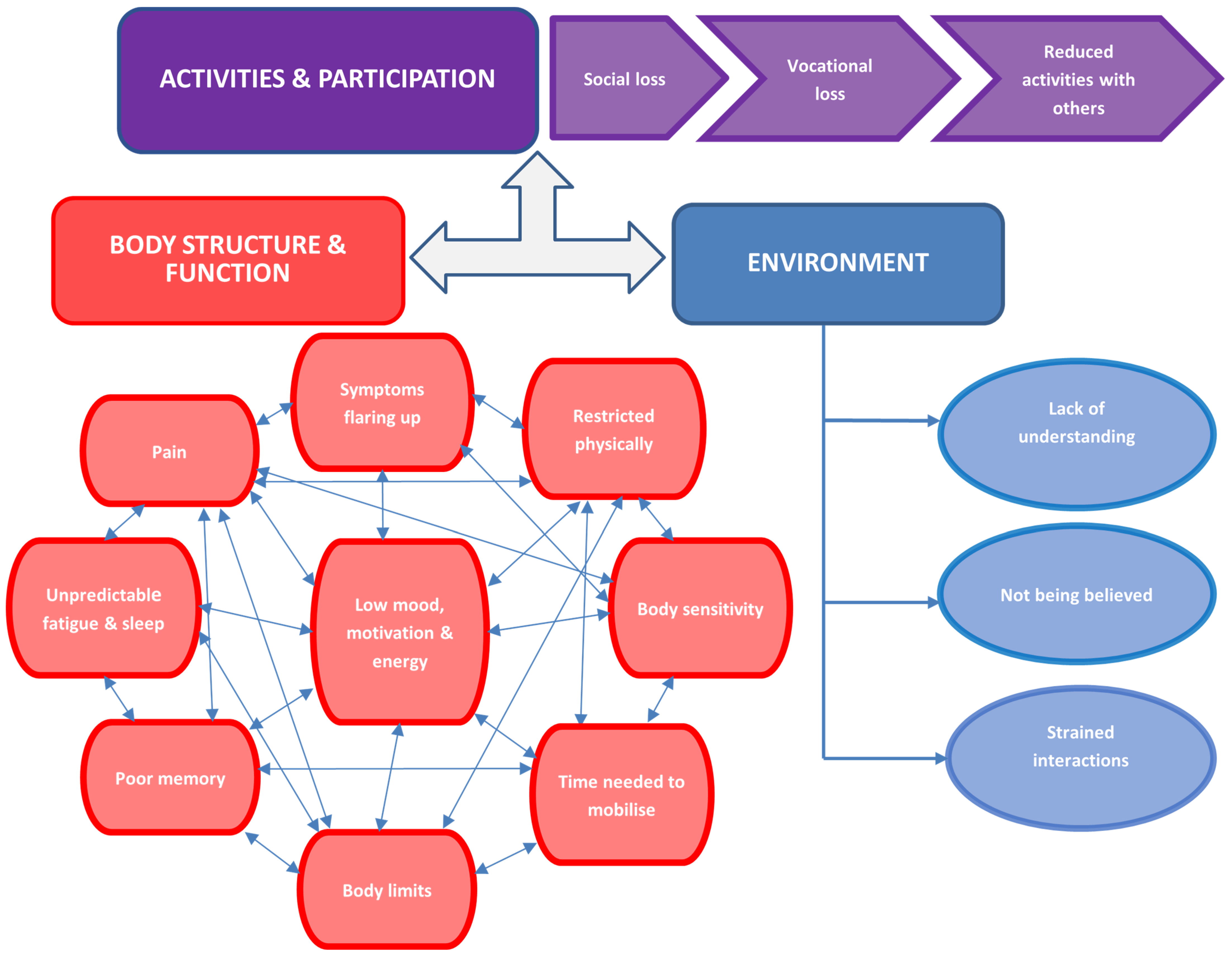
3.2.1. Body Structure and Function
“my pain’s that bad…I just think—no, I can’t be bothered”(Participant A)
“very tight and aching as if somebody needs to roll my body out with a rolling pin…it’s kinda like you’ve got the flu—heavy and achey…random spasms”(Participant D)
“the other pain is in my scapula and neck area where you feel like somebody using a chisel and digging down in my flesh, and other sensations—like a hot piece of iron on your flesh…my jawbone, my face is painful…I find it painful talking, eating, and if I like cough or yawn it hurts, it’s so painful”(Participant H)
“when I wake up there’s so much pain, it’s like someone’s been stepping on me—it’s crazy, crazy pain”(Participant L)
“the pain is just constantly there…it’s amazing that your arms hurt when you walk. Why do your arms hurt when you walk?!”(Participant P)
“Exhaustion, the pain’s a lot worse, can’t get out of bed. There’s no way I could make it to do any work even though I’ve just got to go downstairs…I’ve had to phone work and just say I can’t physically work”(Participant K)
“Sometimes I can’t get up the stairs. Sometimes I have to come down on my bottom…I can just walk sometimes and my legs give way”(Participant P)
“I used to walk my labrador quite a distance across the canal—don’t do it so much now because of the pain”(Participant A)
“I could be walking and I just get tightness from nowhere and muscle pain…I just can’t seem to identify exactly how it’s happening”(Participant B)
“I get support with some personal assistance, like to do housework, to cook and to shop”(Participant H)
“I can’t walk very much. I can maybe walk from my house to the corner shop…maybe 15 yards and that’s it I’ve had it”(Participant O)
“It’s really difficult for me to wipe my own backside”(Participant N)
“My skin literally burns like on fire. It crawls all over my body”(Participant H)
“It hurts even for a thin light quilt to rest on my feet”(Participant P)
“I just do what needs doing in little chunks because if I try to do too much in one go it’ll backfire on me”(Participant B)
“I’d feel as if I’d hit a brick wall…my body’s kind of on its brink”(Participant D)
“I can’t do anything to un-knot it”(Participant E)
“I lose the ability to walk…my knee will just jolt out and I’ll fall down”(Participant G)
“You know it’s like as if my body’s in control of me, not me in control of it”(Participant J)
“I ain’t there just yet to do it again (yoga)—I’m not motivated”(Participant A)
“I’ve got no interest in anything…if I haven’t got a reason to get up I’ll stay in bed all day…well because of the quality of my life, I just think you wouldn’t let an animal suffer like this. I welcome death because of the pain”(Participant F)
“it took me 3 days to clean up my bedroom and I didn’t wanna do it but I had to ‘cause it was a mess”(Participant G)
“I get really fed up and snappy…I snap at people for nothing…agitated at the least little thing”(Participant O)
“If you said to me like here’s a gun you can shoot yourself, I probably would—it’s not being able to cope with the pains”(Participant P)
“I get mixed up with words. I don’t open up in conversation because I feel ashamed”(Participant A)
“I just can’t stay engaged for that long, I can’t stay interested, my attention span’s gone”(Participant B)
“My reactions would feel as if they were a lot slower…I’d feel kinda too tired to answer straight away. I’d hear somebody saying something and I’d have to think it through”(Participant D)
“I can ask what drinks people want, walk into the next room, then I haven’t got a clue what they want…I’ll have to re-read a lot ‘cause I don’t remember the page I’m on…I forget the names of words a lot as well—my degree’s in Psychology and English—you’d think I’d know words”(Participant E)
“Grandchildren’s names? I’d never remember…I repeat myself a lot…I’ll tell them 3 or 4 times and not realise I’ve already told them…I used to love reading, that was my favourite thing, just get lost in a book—I can’t now I couldn’t even read a page, if I read a line I forgot what it says so I go back to the beginning”, ”I think I annoy people, and my speech comes out all jumbled up…so I think I’m saying the right thing but something else is coming out and I don’t realise”(Participant F)
“I mix up names of things but I don’t realise unless somebody points it out…like the other day I said I’m going to put my pizza in the fridge but I meant the oven—like it wouldn’t click in my head that I’d got the wrong word”(Participant I)
“I couldn’t string sentences together and I thought have I got dementia?”(Participant J)
“um what year are we in now? I was gonna say 1919, but it ain’t 1919 is it?(Participant P)
“By lunchtime I’m fatigued so I have to go home and have a nap”(Participant B)
“I think it was yesterday I didn’t wake up until 7 pm on the night-time. And I thought I was gonna be awake all night and I wasn’t. I fell asleep at 3 am and woke at 10 am today to get here so I’m actually shocked that I still feel exhausted. I feel like I’ve had no sleep for weeks”(Participant G)
“Tired, no energy I just feel dead, deflated…flat”(Participant H)
“The pain just from showering can exhaust me”(Participant I)
“I know I shouldn’t have but I just took another two co-codamol and another two gabapentin 600 mg, I think that’s about 1200 mg…don’t feel refreshed, don’t feel as if I’ve had a good enough sleep, I just feel like the soreness of my muscles is preventing me from completely relaxing”(Participant J)
“There have been nights where I have gone straight through without sleep”(Participant K)
“Sometimes I’m really really tired I say to myself I’m gonna go straight in bed when I leave work, the tiredness is crazy”(Participant L)
“I do nap in the day, my wife calls them cat naps ‘cause I’ll just be reading my phone…and the next thing I’m just asleep. There’s time when my wife says I’ve gone to sleep with my phone in my hand still pointing up at my face”(Participant M)
“I mean some nights I don’t even go to bed, I stop downstairs ‘cause I know I ain’t gonna go to sleep so it’s a waste of time…I feel like I’ve got no energy whatsoever”(Participant O)
3.2.2. Activities and Participation
“I put things off, I’ll make things up…I feel as though I’ll let people down before it’s even started…we’re supposed to be going out this Thursday and I’m dreading it even now ‘cause they’ll talk about something and my mind’ll just go”(Participant A)
“Some days it’s like I want to go, we book a table then I get to the night and it’s just like—I can’t. Sometimes I back out of it…sometimes I wonder whether it’s safe to drive the car…I get to the point where it’s just like I can’t function”(Participant B)
“I just wanna curl up into a ball and stay under my safety net”(Participant G)
“Church…I went yesterday…I came home and couldn’t eat, my body hurts all over. I was saying this is what happens when I go out on a social you know—I get this impact. Best not to make plans”(Participant H)
“Eventually they had to let me go…when I was off other people had to do my work…feeling guilty that I’m letting everybody down”(Participant B)
“Sometimes I just have to go to the toilet and lock myself in for a while and just cry. I have to force myself to stay because I know I’m on my last warning”(Participant F)
“sometime I just do hit a wall and I just have to close my eyes even if I’m working. You know my hands like doing this [hand action] moving the mouse so they think I’m working”(Participant K)
“My children…they say I’m gonna do something—then I don’t do it…I should be over the park with the kids and the dogs and I can’t do that…impossible…never”(Participant F)
“If I go out [e.g., shopping] it’s like I’ve walked up the highest mountain in the world and back in a day…I’m laid up in bed all the next day”(Participant G)
“My son, he wants to play football in the park and I say no to him like, but he doesn’t understand—he thinks I’m lazy”(Participant L)
“Me and my wife used to have a relatively good sex life…but not anymore, it’s just completely changed that side of the relationship…reduced libido, reduced urge, even pain…it just makes everything physically undesirable”(Participant M)
3.2.3. Environment
“I just feel I’m alone”(Participant A)
“Nobody can understand you know, ‘cause you look physically fine”(Participant B)
“My son says ‘I already told you mum and you’re just not listening to me’”(Participant K)
“Struggling with conversations…I haven’t got anything to say…I mean ‘cause they’re fed up of hearing it I think”(Participant N)
“People don’t wanna hear it and they think I’m making it up…other partners aren’t supportive because they don’t believe it’s a thing. They think it’s made up because you can’t be bothered”(Participant A)
“He can’t cope with me saying things like ‘I just can’t live like this anymore’—so it’s difficult for me to speak to him…it would hurt him and he’d worry all the time”(Participant P)
3.3. The Thematic Synthesis
“It’s absolutely changed my life because it feels like somebody pulled a rug from beneath my feet…it hasn’t allowed me to finish my degree that I wanted to finish in 2013”(Participant H)
“I used to be extremely fit…so to have to go where I am now—I’m like a shell of a person really”(Participant A)
“I used to do 25,000 steps a day…felt really refreshed, always up at the crack of dawn, out with the dog twice a day, the gym…my mood was good…we used to do quite a bit of walking like in the Yorkshire Dales…I’ve scaled that down now to little parks”(Participant C)
“I used to be so active…gym everyday, bike and swim, and very fitness and health-orientated. I used to love to do the garden…I don’t even go outside now”(Participant F)
“I used to really like walking over the fields with the dog but I’ve not done it in 4 years”(Participant I)
“My job…I was constantly up and down ladders…swimming twice a week, I used to cycle at least a couple of hundred miles a week, I used to do two martial arts—tai boxing and JKD…it’s just changed my life to be honest. I was quite a healthy weight. My weight has now rocketed to nearly 20 stone”(Participant M)
“I could do anything—if you spoke to my husband he’ll tell you he’s got a different wife now”(Participant P)
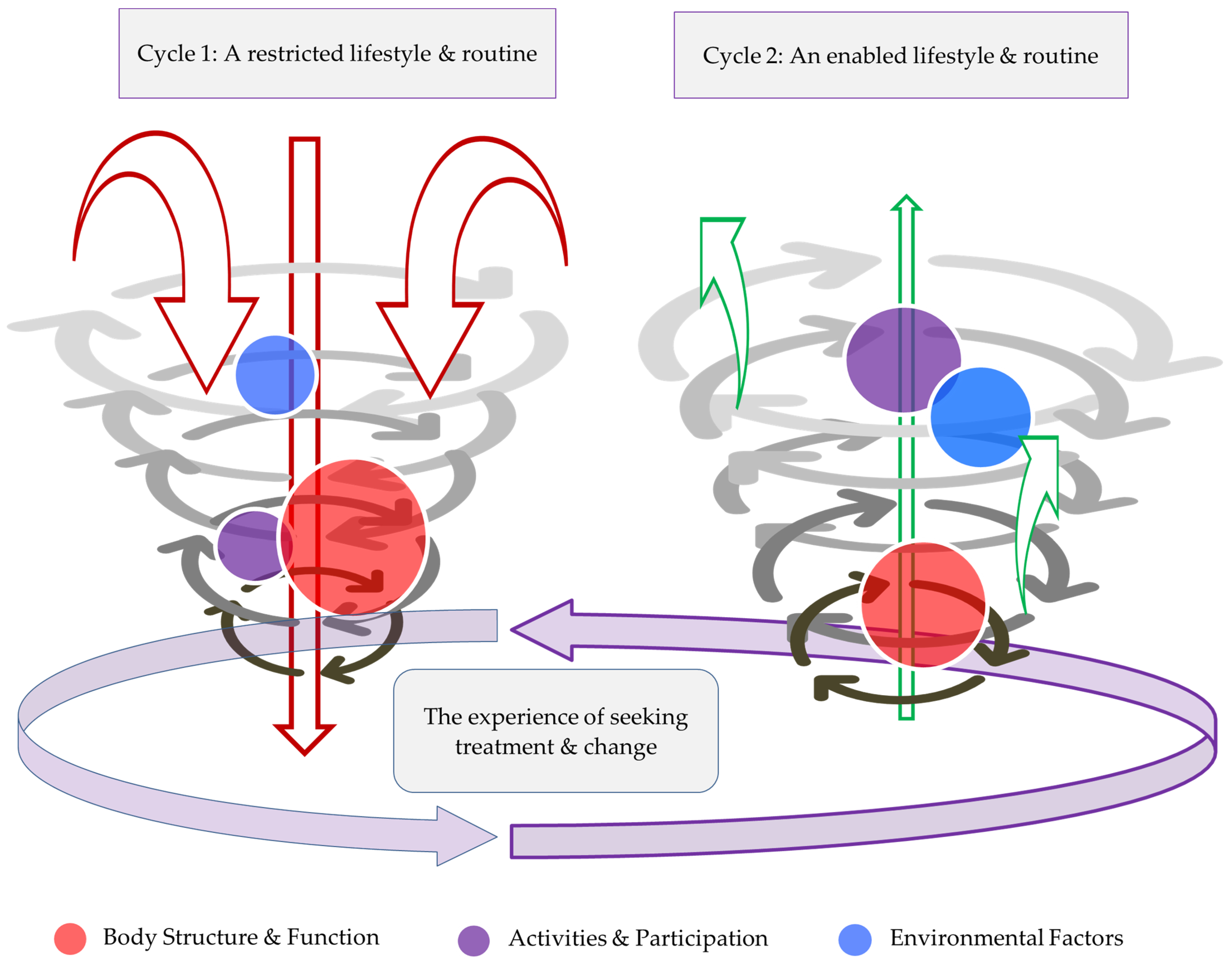
3.3.1. Established Phases of the Decomposition Reaction
Describing the Reaction
3.3.2. The Experiences of Seeking Treatment and Change
Problematic Experiences
“I was on so much medication I didn’t know where I was. I didn’t know this at the time because I was taking all the medication”(Participant A)
“The botox was the most painful thing I’ve ever had done in my life”(Participant B)
“I’ve tried a lot of drugs…felt constantly hungover—that’s not something I want in my system for no reason…I don’t want more toxins in my body. I wouldn’t drive because they make me drowsy, I don’t want to lose my driving license”(Participant D)
Ineffective Experiences
3.4. Potential for Recomposition Reaction
3.4.1. Describing the Reaction
3.4.2. Activities and Participation
3.4.3. Environment
4. Discussion
4.1. Cognition to Feature in the FM “Vicious Cycle”
4.2. The Fibromyalgia Decomposition Phenomenon
4.3. Potential for “Recomposition”
4.4. Requirement for a Widespread and Holistic Approach Not Only to Treatment, but in Patient and Clinician Treatment Evaluation
4.5. Limitations
4.6. Recommendations for Future Research and Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Primers 2015, 1, 15022. [Google Scholar] [CrossRef]
- Royal College of Physicians. The Diagnosis of Fibromyalgia Syndrome; UK Clinical Guidelines; Royal College of Physicians: London, UK, 2022. [Google Scholar]
- Wolfe, F. Criteria for fibromyalgia? What is fibromyalgia? Limitations to current concepts of fibromyalgia and fibromyalgia criteria. Clin. Exp. Rheumatol. 2017, 35, 3–5. [Google Scholar] [PubMed]
- World Health Organization. ICD-11 for Mortality and Morbidity Statistics. 2023. Available online: https://icd.who.int/browse11/l-m/en#! (accessed on 11 September 2023).
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Marques, A.P.; Santo, A.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reum. Engl. Ed. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- D’Onghia, M.; Ciaffi, J.; Ruscitti, P.; Cipriani, P.; Giacomelli, R.; Ablin, J.N.; Ursini, F. The economic burden of fibromyalgia: A systematic literature review. Semin. Arthritis Rheum. 2022, 56, 152060. [Google Scholar] [CrossRef] [PubMed]
- Offenbaecher, M.; Kohls, N.; Ewert, T.; Sigl, C.; Hieblinger, R.; Toussaint, L.L.; Sirois, F.; Hirsch, J.; Vallejo, M.A.; Kramer, S.; et al. Pain is not the major determinant of quality of life in fibromyalgia: Results from a retrospective “real world” data analysis of fibromyalgia patients. Rheumatol. Int. 2021, 41, 1995–2006. [Google Scholar] [CrossRef] [PubMed]
- Azzam, A.; Lamlom, M.; Khalifa, A. The Prevalence of Fibromyalgia in Patients with Rheumatoid Arthritis and its Impact on Disease Activity, Functional Level, and Psychological Status. Int. J. Med. Arts 2022, 4, 2514–2521. [Google Scholar] [CrossRef]
- Pincus, T.; Summey, J.A.; Soraci, S.A., Jr.; Wallston, K.A.; Hummon, N.P. Assessment of patient satisfaction in activities of daily living using a modified Stanford Health Assessment Questionnaire. Arthritis Rheum. 1983, 26, 1346–1353. [Google Scholar] [CrossRef]
- Hieblinger, R.; Coenen, M.; Stucki, G.; Winkelmann, A.; Cieza, A. Validation of the International Classification of Functioning, Disability and Health Core Set for chronic widespread pain from the perspective of fibromyalgia patients. Arthritis Res. Ther. 2009, 11, R67. [Google Scholar] [CrossRef]
- Prodinger, B.; Salzberger, T.; Stucki, G.; Stamm, T.; Cieza, A. Measuring functioning in people with fibromyalgia (FM) based on the international classification of functioning, disability and health (ICF)—A psychometric analysis. Pain Pract. 2012, 12, 255–265. [Google Scholar] [CrossRef]
- World Health Organization. How to Use the ICF: A practical Manual for Using the International Classification of Functioning, Disability and Health (ICF). Exposure Draft for Comment 2013. Available online: https://cdn.who.int/media/docs/default-source/classification/icf/drafticfpracticalmanual2.pdf?sfvrsn=8a214b01_4&download=true (accessed on 7 October 2023).
- Larsson, A.; Feldthusen, C.; Mannerkorpi, K. Factors promoting physical activity in women with fibromyalgia: A qualitative interview study. BMJ Open 2020, 10, e031693. [Google Scholar] [CrossRef] [PubMed]
- Fitzcharles, M.A.; Ste-Marie, P.A.; Rampakakis, E.; Sampalis, J.S.; Shir, Y. Disability in Fibromyalgia Associates with Symptom Severity and Occupation Characteristics. J. Rheumatol. 2016, 43, 931–936. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classfication of Functioning, Disability and Health (ICF). 2001. Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed on 30 June 2023).
- Armentor, J.L. Living With a Contested, Stigmatized Illness: Experiences of Managing Relationships among Women with Fibromyalgia. Qual. Health Res. 2017, 27, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Brown, N. The Social Course of Fibromyalgia: Resisting Processes of Marginalisation. Int. J. Environ. Res. Public Health 2022, 19, 333. [Google Scholar] [CrossRef]
- Quintner, J. Why Are Women with Fibromyalgia so Stigmatized? Pain Med. 2020, 21, 882–888. [Google Scholar] [CrossRef]
- Sabik, S. Fibromyalgia: Stigmatization and its Impact. J. Appl. Rehabil. Couns. 2010, 41, 30–36. [Google Scholar] [CrossRef]
- Van Alboom, M.; De Ruddere, L.; Kindt, S.; Loeys, T.; Van Ryckeghem, D.; Bracke, P.; Mittinty, M.M.; Goubert, L. Well-being and Perceived Stigma in Individuals with Rheumatoid Arthritis and Fibromyalgia: A Daily Diary Study. Clin. J. Pain 2021, 37, 349–358. [Google Scholar] [CrossRef]
- Qureshi, A.G.; Jha, S.K.; Iskander, J.; Avanthika, C.; Jhaveri, S.; Patel, V.H.; Rasagna Potini, B.; Talha Azam, A. Diagnostic Challenges and Management of Fibromyalgia. Cureus 2021, 13, e18692. [Google Scholar] [CrossRef]
- Ashe, S.C.; Furness, P.J.; Taylor, S.J.; Haywood-Small, S.; Lawson, K. A qualitative exploration of the experiences of living with and being treated for fibromyalgia. Health Psychol. Open 2017, 4, 2055102917724336. [Google Scholar] [CrossRef]
- Byrne, A.; Jones, K.; Backhouse, M.; Rose, F.; Moatt, E.; van der Feltz-Cornelis, C. Patient and primary care practitioners’ perspectives on consultations for fibromyalgia: A qualitative evidence synthesis. Prim. Health Care Res. Dev. 2023, 24, e58. [Google Scholar] [CrossRef]
- Rico-Villademoros, F.; Postigo-Martin, P.; Garcia-Leiva, J.M.; Ordoñez-Carrasco, J.L.; Calandre, E.P. Patterns of pharmacologic and non-pharmacologic treatment, treatment satisfaction and perceived tolerability in patients with fibromyalgia: A patients’ survey. Clin. Exp. Rheumatol. 2020, 38 (Suppl. S123), 72–78. [Google Scholar]
- Valentini, E.; Fetter, E.; Orbell, S. Treatment preferences in fibromyalgia patients: A cross-sectional web-based survey. Eur. J. Pain 2020, 24, 1290–1300. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Moshrif, A.; Mosallam, A.; Abu-Zaid, M.H.; Gouda, W. Evaluating the Effect of Delayed Diagnosis on Disease Outcome in Fibromyalgia: A Multi-Center Cross-Sectional Study. J. Pain Res. 2023, 16, 1355–1365. [Google Scholar] [CrossRef] [PubMed]
- Borg, C.; Chouchou, F.; Dayot-Gorlero, J.; Zimmerman, P.; Maudoux, D.; Laurent, B.; Michael, G.A. Pain and emotion as predictive factors of interoception in fibromyalgia. J. Pain Res. 2018, 11, 823–835. [Google Scholar] [CrossRef]
- Montoya, P.; Larbig, W.; Braun, C.; Preissl, H.; Birbaumer, N. Influence of social support and emotional context on pain processing and magnetic brain responses in fibromyalgia. Arthritis Rheum. 2004, 50, 4035–4044. [Google Scholar] [CrossRef] [PubMed]
- Rhudy, J.L.; DelVentura, J.L.; Terry, E.L.; Bartley, E.J.; Olech, E.; Palit, S.; Kerr, K.L. Emotional modulation of pain and spinal nociception in fibromyalgia. PAIN® 2013, 154, 1045–1056. [Google Scholar] [CrossRef] [PubMed]
- Trucharte, A.; Leon, L.; Castillo-Parra, G.; Magán, I.; Freites, D.; Redondo, M. Emotional regulation processes: Influence on pain and disability in fibromyalgia patients. Clin. Exp. Rheumatol. 2020, 38, 40–46. [Google Scholar]
- van Middendorp, H.; Lumley, M.A.; Moerbeek, M.; Jacobs, J.W.G.; Bijlsma, J.W.J.; Geenen, R. Effects of anger and anger regulation styles on pain in daily life of women with fibromyalgia: A diary study. Eur. J. Pain 2010, 14, 176–182. [Google Scholar] [CrossRef]
- Pinto, A.M.; Geenen, R.; Wager, T.D.; Lumley, M.A.; Häuser, W.; Kosek, E.; Ablin, J.N.; Amris, K.; Branco, J.; Buskila, D.; et al. Emotion regulation and the salience network: A hypothetical integrative model of fibromyalgia. Nat. Rev. Rheumatol. 2023, 19, 44–60. [Google Scholar] [CrossRef]
- Lineberger, M.D.; Means, M.K.; Edinger, J.D. Sleep Disturbance in Fibromyalgia. Sleep Med. Clin. 2007, 2, 31–39. [Google Scholar] [CrossRef]
- Serrano, P.V.; Zortea, M.; Alves, R.L.; Beltran, G.; Deliberali, C.B.; Maule, A.; Torres, I.L.S.; Fregni, F.; Caumo, W. Association between descending pain modulatory system and cognitive impairment in fibromyalgia: A cross-sectional exploratory study. Front. Behav. Neurosci. 2022, 16, 917554. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, V.; Ortega, F.; Carbonell-Baeza, A.; Cuevas-Toro, A.; Delgado-Fernández, M.; Ruiz, J. Anxiety, depression and fibromyalgia pain and severity. Behav. Psychol./Psicol. Conduct. 2013, 21, 192–381. [Google Scholar]
- Alvarez, M.C.; Albuquerque, M.L.L.; Neiva, H.P.; Cid, L.; Rodrigues, F.; Teixeira, D.S.; Matos, R.; Antunes, R.; Morales-Sánchez, V.; Monteiro, D. Exploring the Relationship between Fibromyalgia-Related Fatigue, Physical Activity, and Quality of Life. Int. J. Environ. Res. Public Health 2022, 19, 4870. [Google Scholar] [CrossRef] [PubMed]
- Lempp, H.K.; Hatch, S.L.; Carville, S.F.; Choy, E.H. Patients’ experiences of living with and receiving treatment for fibromyalgia syndrome: A qualitative study. BMC Musculoskelet. Disord. 2009, 10, 124. [Google Scholar] [CrossRef] [PubMed]
- Fitzcharles, M.A.; Perrot, S.; Häuser, W. Comorbid fibromyalgia: A qualitative review of prevalence and importance. Eur. J. Pain 2018, 22, 1565–1576. [Google Scholar] [CrossRef]
- Sanz-Baños, Y.; Pastor, M.; Velasco, L.; López-Roig, S.; Peñacoba, C.; Lledo, A.; Rodríguez, C. To walk or not to walk: Insights from a qualitative description study with women suffering from fibromyalgia. Rheumatol. Int. 2016, 36, 1135–1143. [Google Scholar] [CrossRef]
- Velasco-Furlong, L.; Gutiérrez-Hermoso, L.; Mateos-Pintado, B.; Castro, D.G.; Blanco-Rico, S.; Sanromán-Canelada, L.; López-Roig, S.; Pastor-Mira, M.; Peñacoba-Puente, C. The 4 U’s Rule of Fibromyalgia: A Proposed Model for Fatigue in a Sample of Women with Fibromyalgia: A Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 6224. [Google Scholar] [CrossRef]
- Reig-Garcia, G.; Bosch-Farré, C.; Suñer-Soler, R.; Juvinyà-Canal, D.; Pla-Vila, N.; Noell-Boix, R.; Boix-Roqueta, E.; Mantas-Jiménez, S. The Impact of a Peer Social Support Network from the Perspective of Women with Fibromyalgia: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 12801. [Google Scholar] [CrossRef]
- Wilson, N.; Beasley, M.J.; Pope, C.; Dulake, D.; Moir, L.J.; Hollick, R.J.; Macfarlane, G.J. UK healthcare services for people with fibromyalgia: Results from two web-based national surveys (the PACFiND study). BMC Health Serv. Res. 2022, 22, 989. [Google Scholar] [CrossRef]
- Charles, A. Integrated Care Systems Explained: Making Sense of Systems, Places and Neighbourhoods. 2022. Available online: https://www.kingsfund.org.uk/publications/integrated-care-systems-explained (accessed on 7 October 2023).
- Public Participant Team. NHS England Patient and Public Voice Partners Policy. 2017. Available online: https://www.england.nhs.uk/wp-content/uploads/2017/08/patient-and-public-voice-partners-policy-july-2017.pdf (accessed on 7 October 2023).
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Harding, G.; Gantley, M. Qualitative methods: Beyond the cookbook. Fam. Pract. 1998, 15, 76–79. [Google Scholar] [CrossRef]
- Fitzmaurice, B.C.; Heneghan, N.R.; Rayen, A.T.A.; Grenfell, R.L.; Soundy, A.A. Whole-Body Photobiomodulation Therapy for Fibromyalgia: A Feasibility Trial. Behav. Sci. 2023, 13, 717. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Byrne, D. A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Qual. Quant. 2022, 56, 1391–1412. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]
- Allemang, B.; Sitter, K.; Dimitropoulos, G. Pragmatism as a paradigm for patient-oriented research. Health Expect 2022, 25, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Moore, P.C.F. The Pain Toolkit. 2010. Available online: https://www.paintoolkit.org/ (accessed on 6 October 2023).
- Theodore, B.R.; Kishino, N.D.; Gatchel, R.J. Biopsychosocial Factors that Perpetuate Chronic Pain, Impairment, and Disability. Psychol. Inj. Law 2008, 1, 182–190. [Google Scholar] [CrossRef]
- Choy, E.H.S. The role of sleep in pain and fibromyalgia. Nat. Rev. Rheumatol. 2015, 11, 513–520. [Google Scholar] [CrossRef]
- Steiner, J.L.; Bigatti, S.M.; Slaven, J.E.; Ang, D.C. The Complex Relationship between Pain Intensity and Physical Functioning in Fibromyalgia: The Mediating Role of Depression. J. Appl. Biobehav. Res. 2017, 22, e12079. [Google Scholar] [CrossRef]
- Covich, A.P. Energy Flow and Ecosystems. In Encyclopedia of Biodiversity, 2nd ed.; Levin, S.A., Ed.; Academic Press: Waltham, MA, USA, 2013; pp. 237–249. [Google Scholar] [CrossRef]
- Berg, B.M.C.C. Decomposition as a Process. In Plant Litter, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar] [CrossRef]
- Bitesize, B. Computational Thinking. 2023. Available online: https://www.bbc.co.uk/bitesize/guides/zp92mp3/revision/1 (accessed on 9 October 2023).
- Gessner, M.O.; Swan, C.M.; Dang, C.K.; McKie, B.G.; Bardgett, R.D.; Wall, D.H.; Hättenschwiler, S. Diversity meets decomposition. Trends Ecol. Evol. 2010, 25, 372–380. [Google Scholar] [CrossRef] [PubMed]
- The Free Dictionary. Available online: https://www.thefreedictionary.com/recompose (accessed on 9 October 2023).
- Barakat, C.; Pearson, J.; Escalante, G.; Campbell, B.; De Souza, E.O. Body Recomposition: Can Trained Individuals Build Muscle and Lose Fat at the Same Time? Strength Cond. J. 2020, 42, 7–21. [Google Scholar] [CrossRef]
- Romadona, M.R.; Setiawan, S. Researchers’ View on R&D Organizational Change Using the Grief Cycle. STI Policy Manag. J. 2021, 6, 157–171. [Google Scholar] [CrossRef]
- Galosi, E.; Truini, A.; Di Stefano, G. A Systematic Review and Meta-Analysis of the Prevalence of Small Fibre Impairment in Patients with Fibromyalgia. Diagnostics 2022, 12, 1135. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef]
- Huber, F.A.; Toledo, T.A.; Newsom, G.; Rhudy, J.L. The relationship between sleep quality and emotional modulation of spinal, supraspinal, and perceptual measures of pain. Biol. Psychol. 2022, 171, 108352. [Google Scholar] [CrossRef]
- Estévez-López, F.; Álvarez-Gallardo, I.C.; Segura-Jiménez, V.; Soriano-Maldonado, A.; Borges-Cosic, M.; Pulido-Martos, M.; Aparicio, V.A.; Carbonell-Baeza, A.; Delgado-Fernández, M.; Geenen, R. The discordance between subjectively and objectively measured physical function in women with fibromyalgia: Association with catastrophizing and self-efficacy cognitions. The al-Ándalus project. Disabil. Rehabil. 2018, 40, 329–337. [Google Scholar] [CrossRef]
- Kay, L.; Lanyon, P.; MacGregor, A. Rheumatomogy GIRFT Programme National Speciality Report. 2021. Available online: https://www.gettingitrightfirsttime.co.uk/wp-content/uploads/2021/09/Rheumatology-Jul21h-NEW.pdf (accessed on 7 October 2023).
- Faculty of Pain Medicine of the Royal College of Anaesthetists. Core Standards for Pain Management Services in the UK. 2021. Available online: https://www.britishpainsociety.org/static/uploads/resources/files/FPM-Core-Standards-2021.pdf (accessed on 26 October 2023).
- Davies, A.W.P. Conducting Quality Consultations in Pain Medicine. 2022. Available online: https://fpm.ac.uk/sites/fpm/files/documents/2022-04/Conducting%20a%20Quality%20Consultation%202022_0.pdf (accessed on 26 October 2023).
- Falvo, D.; Holland, B.E. Medical and Psychosocial Aspects of Chronic Illness and Disability, 6th ed.; Jones & Bartlett Learning: Burlington, NJ, USA, 2018. [Google Scholar]
- Zinboonyahgoon, N.; Luansritisakul, C.; Eiamtanasate, S.; Duangburong, S.; Sanansilp, V.; Korwisi, B.; Barke, A.; Rief, W.; Treede, R.-D. Comparing the ICD-11 chronic pain classification with ICD-10: How can the new coding system make chronic pain visible? A study in a tertiary care pain clinic setting. Pain 2021, 162, 1995–2001. [Google Scholar] [CrossRef]
- Societal Impact of Pain. The WHO Internation Classification of Functioning, Disability and Health (ICF). Ed. 2022, pp. 1–8. Available online: https://europeanpainfederation.eu/sip/icd-11 (accessed on 5 October 2023).
- Taylor, S.J.; Steer, M.; Ashe, S.C.; Furness, P.J.; Haywood-Small, S.; Lawson, K. Patients’ perspective of the effectiveness and acceptability of pharmacological and non-pharmacological treatments of fibromyalgia. Scand. J. Pain 2019, 19, 167–181. [Google Scholar] [CrossRef]
- Pinto, A.M.; Geenen, R.; Castilho, P.; da Silva, J.A.P. Progress towards improved non-pharmacological management of fibromyalgia. Jt. Bone Spine 2020, 87, 377–379. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Participant ID | Gender | Age (Years) | Symptoms (Years) | Marital Status | Employment | Education Level | Ethnicity | BMI Category (kg/m2) |
|---|---|---|---|---|---|---|---|---|
| A | Female | 51–55 | 27 | Married | Unemployed (looking for work) | Further education (sixth form) | White British | 30.0 to <35 |
| B | Male | 46–50 | 6 | Single | Self-employed | Higher education | Asian/Asian British | 18.5 to <25 |
| C | Male | 41–45 | 6 | Civil Partnership | Self-employed | Higher education | White British | 25.0 to <30 |
| D | Female | 31–35 | 10 | Single | Sick leave | Higher education | White British | 18.5 to <25 |
| E | Female | 36–40 | 26 | Single | Unemployed (not looking for work) | Higher education | White British | 25.0 to <30 |
| F | Female | 51–55 | 10 | Married | Employed full-time | Higher education | White British | 35.0 to <40 |
| G | Female | 31–35 | 24 | Single | Unemployed (not looking for work) | Higher education | White British | 35.0 to <40 |
| H | Female | 46–50 | 10 | Single | Unemployed (not looking for work) | Higher education | Black British-Caribbean | >40 |
| I | Female | 26–30 | 4 | Co-habiting | Unemployed (not looking for work) | Higher education | White British | 25.0 to <30 |
| J | Female | 61–65 | 31 | Divorced | Retired | Higher education | White British | 25.0 to <30 |
| K | Female | 51–55 | 17 | Married | Employed full-time | Secondary school | White British | 25.0 to <30 |
| L | Male | 36–40 | 24 | Married | Employed full-time | Higher education | Asian/Asian British | 25.0 to <30 |
| M | Male | 46–50 | 11 | Married | Retired | Higher education | White British | >40 |
| N | Male | 66–70 | 15 | Married | Retired | Secondary school | White British | 35.0 to <40 |
| O | Female | 66–70 | 15 | Married | Retired | Some secondary school | White British | 35.0 to <40 |
| P | Female | 51–55 | 10 | Married | Employed full-time | Higher education | White British | 35.0 to <40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fitzmaurice, B.C.; Grenfell, R.L.; Heneghan, N.R.; Rayen, A.T.A.; Soundy, A.A. The Fibromyalgia Decomposition Phenomenon: A Reflexive Thematic Analysis. Behav. Sci. 2024, 14, 47. https://doi.org/10.3390/bs14010047
Fitzmaurice BC, Grenfell RL, Heneghan NR, Rayen ATA, Soundy AA. The Fibromyalgia Decomposition Phenomenon: A Reflexive Thematic Analysis. Behavioral Sciences. 2024; 14(1):47. https://doi.org/10.3390/bs14010047
Chicago/Turabian StyleFitzmaurice, Bethany C., Rebecca L. Grenfell, Nicola R. Heneghan, Asius T. A. Rayen, and Andrew A. Soundy. 2024. "The Fibromyalgia Decomposition Phenomenon: A Reflexive Thematic Analysis" Behavioral Sciences 14, no. 1: 47. https://doi.org/10.3390/bs14010047
APA StyleFitzmaurice, B. C., Grenfell, R. L., Heneghan, N. R., Rayen, A. T. A., & Soundy, A. A. (2024). The Fibromyalgia Decomposition Phenomenon: A Reflexive Thematic Analysis. Behavioral Sciences, 14(1), 47. https://doi.org/10.3390/bs14010047