
Psychoeducation for Fibromyalgia Syndrome: A Systematic Review of Emotional, Clinical and Functional Related-Outcomes



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis
3. Results
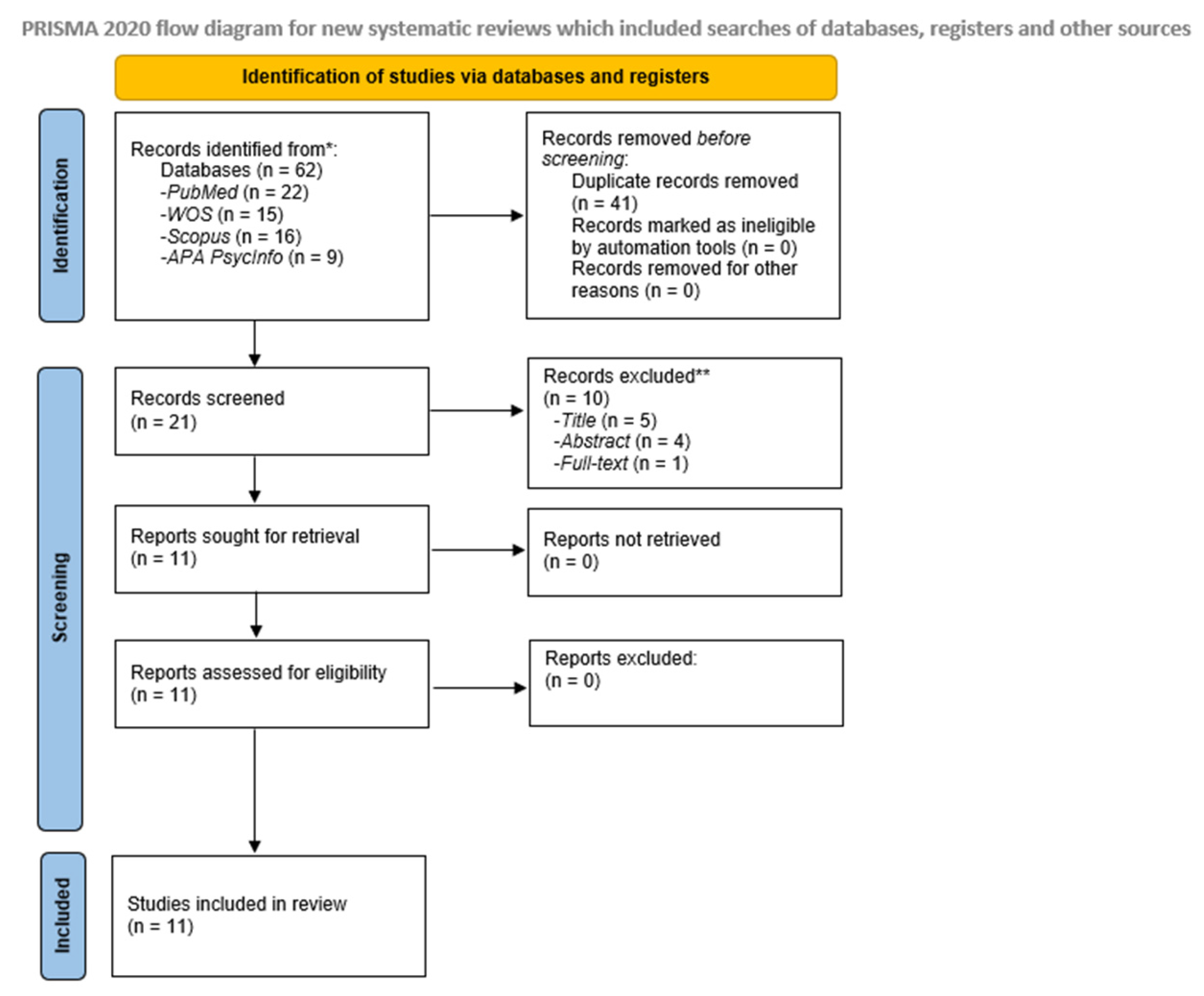
3.1. Literature Search and Study Characteristics


{kind=link}
| First Author (Publication Year), Study Name, Country | Objectives | Study Design/Procedure | Sample Size [Mean ± Age (SD)] | FMS Diagnostic Criteria | Instruments and Variables | Results |
|---|---|---|---|---|---|---|
| Antunes et al. (2022). Amigos de Fibro (Fibro Friends): Validation of an Educational Program to Promote Health in Fibromyalgia. Brazil. [97]. | To validate a multidisciplinary educational health promotion program for individuals with FMS. | Delphi technique. Procedure: Phases: (1) Development of Amigos de Fibro; (2) Content validation of Amigos de Fibro; (3) Adjusting the Amigos de Fibro; (4) Final assessment of Amigos de Fibro; and (5) Final version of Amigos de Fibro. | N = 23 health professionals (expert judges). 10 males (43.5%) and 13 females (56.5%). Aged between 31 and 40 years old (39.2%). N = 45 individuals with FMS (target audience). 4 males (9%) and 41 females (91%). Aged between 31 and 40 years old (38%). | 2016 ACR, revised version. | Groups of professionals and individuals with FMS listed their demands through the focus group. Evaluation of Amigos de Fibro, built with the information and results obtained from the first round, regarding the objectives, proposed themes and initiatives, relevance, writing style, and structure of the program (with specialists and individuals with FMS). Final evaluation of the material after the corrections are made, based on the judges’ suggestions. | Content validity index (CVI) ≤ 0.78 and coefficient kappa ≤ 0.61. All 25 items evaluated in both groups presented considerable minimum CVI by CVI and the kappa coefficient. Global CVI of Amigos de Fibro, by the specialist judges, was 0.90; and 0.95 by the target audience judges. The kappa coefficient of the expert judges was 0.90 and that of the target audience judges was 0.85. Amigos de Fibro was considered with adequate content validity and internal consistency. |
| Pérez-Aranda et al. (2021). Do humor styles predict clinical response to the MINDSET (MINDfulneSs & EducaTion) program? A pilot study in patients with fibromyalgia. Spain. [98]. | To explore the role of humor styles in predicting clinical changes after the multicomponent intervention (MINDSET) that combines mindfulness and psychoeducation for FMS patients. | Pilot Study. * Procedure: MINDSET intervention: 4 psychoeducation sessions about FMS, based on a previously validated program, and 4 sessions of mindfulness training, based on the Mindfulness-Based Stress Reduction curriculum. Psychoeducation Sessions: 2 h, twice per week, run by health psychologists in a group setting of 8–10 patients. Intervention added on to the patient’s usual care (i.e., medication). No additional active treatments. | N = 35 FMS patients. N = 34 (97.1%) FMS female patients [54.97 ± 8.65]. | 1990 ACR. | FFMQ-15. FIQR. HSQ. PGIC. | FMS patients: affiliative humor and positive/negative ratio humor styles had a unique predictive effect on self-reported clinical changes. Association between humor styles with functional impact and mindfulness facets. Some humor styles may imply a better disposition in patients to learn and implement the concepts and resources that the intervention offered. |
| Melin et al. (2018). Psychoeducation against depression, anxiety, alexithymia, and fibromyalgia: a pilot study in primary care for patients on sick leave. Sweden. [99]. | (1) To try the feasibility of ASSA in a Swedish primary care setting; (2) to explore associations between symptoms of depression, anxiety, alexithymia, and MUPS. | Pilot Study. * ¤ Procedure: ASSA began with 8 group sessions—‘the Affect School’, which were followed directly by 10 individual sessions—‘the Script Analysis’. All 27 respondents one-week post-intervention terminated ASSA within 20 weeks from the start. Script Analysis sessions were performed with one instructor, either the physiotherapist, the GP, or one social counselor. Affect School comprised 8 weekly, 2-h sessions, of a 5–7 participant group, led by the same instructors (one psychotherapist, one physiotherapist, and one GP) during all sessions. Psychoeducation Sessions: 8 weekly 2-h sessions with a 5–7 participant group led by two instructors followed by 10 individual hour-long sessions. Follow-up: 18 months. | N = 36 patients. 29 female patients (81%). Median age 39, range 27–60 years. (N FMS patients: 2 [6%]). | Not specified. | TAS-20. SASB. SCI-93. EuroQol ‘health barometer’ (100 mm—VAS). | Patients: one-week post-intervention median test score changes were significantly favorable for 9 of 11 measures (depression, anxiety, alexithymia, MUPS, general health, self-affirmation, self-love, self-blame, and self-hate); at 18 months post-intervention the results remained significantly favorable for 15 respondents for 7 of 11 measures (depression, alexithymia, MUPS, general health, self-affirmation, self-love, and self-hate). |
| Feliu-Soler et al. (2016). Cost-utility and biological underpinnings of Mindfulness-Based Stress Reduction (MBSR) versus a psychoeducational program (FibroQoL) for fibromyalgia: a 12-month randomized controlled trial (EUDAIMON study). Spain [102]. | (1) To examine the effectiveness and cost-utility for FMS patients of MBSR as an add-on to treatment as usual (TAU) versus TAU + the psychoeducational program FibroQoL, and versus TAU only; (2) to examine pre-post differences in brain structure and function, as well as levels of specific inflammatory markers in the three study arms; and (3) to analyze the role of some psychological variables as mediators of 12-month clinical outcomes. | 12-month randomized controlled trial. * ¤ Procedure: Protocol in progress. Psychoeducation Sessions (FibroQoL): 8, 2-h sessions. Three treatment arms: (1) TAU + MBSR; (2) TAU + FibroQoL; (3) TAU. Control Group: TAU (pharmacologic treatment + counselling about aerobic exercise adjusted to patients’ physical limitations). Active control group: TAU + FibroQoL. FibroQoL: a psycho-educational program for FMS patients based on a consensus document drawn up by the Health Department of Catalonia. Planned follow-up: 12 months. | N = 180 FMS female patients. N = 60 FMS female patients per group. | 1990 ACR. | Sociodemographic-clinical questionnaire. Structured Clinical Interview for DSM Axis I Disorders (SCID-I). Screening measures: MMSE. Primary Outcome: FIQR. Secondary Outcomes: CSRI. EQ-5D-5L. FFMQ. FSDC. HADS. MISCI. PCS. PIPS. PSS. SCS. Other measures: CEQ. PGIC. PSIC. Log of out-session for MBSR and psychotherapeutic practices. Adverse events of the interventions. Neuroimaging MRI. Brain structure: VBM. Inflammatory markers: Blood samples. | Protocol in progress. |
| Bourgault et al. (2015). Multicomponent interdisciplinary group intervention for self-management of fibromyalgia: a mixed-methods randomized controlled trial. Canada [104]. | To evaluate, quantitatively and qualitatively, the efficacy of the PASSAGE Program—a multicomponent interdisciplinary group intervention for the self-management of FMS. | A mixed-methods randomized controlled trial. * ¤ Intervention (INT) vs. waitlist (WL). Qualitative group interviews with a subset of patients were also conducted. Procedure: Intervention: PASSAGE Program (a structured multicomponent interdisciplinary group intervention aimed at reducing FMS symptoms and maintaining optimal function through the use of self-management strategies and patient education). 9 group sessions with 8 participants lasting 2.5 h each. Each session involved 3 major components: (1) psycho-educational tools; (2) CBT-related techniques; and (3) patient-tailored exercise activities. Follow-up: 3 months. | N = 28 INT Group. 26 females (92.9%). [49.98 ± 9.23]. N = 28 WL Group. 26 females (92.9%). [46.74 ± 11.42]. | 1990 ACR. | Primary outcomes: Change in pain intensity (0–10). Secondary outcomes: Fibromyalgia severity. Pain interference. Sleep quality. Pain coping strategies. Depression. Health-related quality of life. PGIC. Perceived pain relief. | FMS patients: the intervention had a statistically significant impact on the three PGIC measures. At the end of the PASSAGE Program, the percentages of patients who reported pain relief and perceived overall improvement on their pain levels, functioning, and quality of life were significantly higher in the INT Group than in the WL Group. The same differences were observed 3 months post-intervention. The results of the qualitative analysis were in line with the quantitative findings regarding the efficacy of the intervention. The improvement, however, was not reflected in the primary and secondary outcomes. |
| Dowd et al. (2015). Comparison of an Online Mindfulness-based Cognitive Therapy Intervention With Online Pain Management Psychoeducation: A Randomized Controlled Study. Ireland, the UK, North America, and other countries [103]. | To test the effectiveness of a computerized mindfulness-based cognitive therapy intervention (MIA) compared to computerized pain management psychoeducation (PE) in a randomized study. | A randomized controlled study. * ¤ Procedure: Participants in each condition received 12 sessions of treatment, twice per week for 6 weeks. MIA intervention was based on established mindfulness meditation and emotional regulation programs shown to be effective for chronic pain. Psychoeducation Sessions: based on many of the common elements found within pain management programs. The PE program was presented in a series of twice-weekly emails containing written information about chronic pain self-management. Follow-up: 6 months. | N = 124 chronic pain patients. 112 females (90.3%) and 12 males). [44.53 ± 12.25]. N MIA group = 62 participants (N FMS patients: 15). N PE group = 62 participants. (N FMS patients: 18). | Not specified. | Primary Outcomes: Pain interference (BPI). Psychological Distress (HADS). Secondary Outcomes: Pain Intensity: 2 NRS from BPI. PCS. SWL. Average Pain Pain Right Now. CPAQ. MAAS. PGIC. | FMS patients: both groups showed improvements in pain interference, pain acceptance, and catastrophizing from pre-treatment to post-treatment and at follow-up. Reduced average pain intensity from baseline to post-treatment for both groups, but not at follow-up. Increases in subjective well-being, were more pronounced in the MIA than in the PE group. MIA group: greater reduction in pain ‘right now’, and increases in their ability to manage emotions, manage stress and enjoy pleasant events on completion of the intervention. |
| Luciano et al. (2013). Cost-Utility of a Psychoeducational Intervention in Fibromyalgia Patients Compared With Usual Care. An Economic Evaluation Alongside a 12-Month Randomized Controlled Trial. Spain. [101]. | (1) To determine the effectiveness of adding psychoeducational treatment implemented in general practice to usual care for patients with fibromyalgia; (2) to analyze the cost-utility of the intervention from health care and societal perspectives. | 12-month randomized controlled trial. * ¤ Procedure: See Luciano et al., 2011. | See Luciano et al., 2011. | 1990 ACR. | See Luciano et al., 2011. | FMS patients who received psychoeducation: greater improvement on global functional status, physical functioning, pain, morning fatigue, stiffness, and depression. It was confirmed the long-term clinical effectiveness of a psychoeducational treatment program for FMS implemented at the primary care level and the cost-utility from a healthcare and societal perspective. |
| Luciano et al. (2011). Effectiveness of a Psychoeducational Treatment Program Implemented in General Practice for Fibromyalgia Patients. A Randomized Controlled Trial. Spain. [100]. | To examine whether a psychoeducational intervention implemented in primary care is more effective than usual care for improving the functional status of patients with FMS. | Randomized Controlled Trial. * ¤ Procedure: The treatment program is based on a consensus document developed by an expert panel in 2005 and published in 2006 by the Catalan Health Department. Psychoeducation Sessions: 9, 2-h sessions (5 sessions of education and 4 sessions of autogenic relaxation), delivered over a 2-month period (1-afternoon session per week), run by GP and rheumatologist, with a maximum of 18 patients per group. Six separate intervention groups were performed. Intervention group: Usual care from their GP + psychoeducational program. Control group: Usual care from their GP. Usual care from their GP: pharmacologic treatment + counselling about aerobic exercise adjusted to patients’ physical limitations. Follow-up: 12 months. | N = 211 participants. N = 105 intervention group. FMS female patients (97.2%) [55.17 ± 8.58]. N = 106 control group. FMS female patients (98.1%) [55.42 ± 8.63]. | 1990 ACR. | Sociodemographic Questionnaire. Chronic Medical Conditions Checklist. Marlowe-Crowne Social Desirability Scale. FIQ. STAI. | FMS patients who received psychoeducation: a 2-month psychoeducational intervention improves the functional status to a greater extent than usual care, at least in the short-term. The social desirability bias did not explain the reported outcomes. Trait anxiety was associated with response to treatment. |
| Mannerkorpi et al. (2009). Pool exercise for patients with fibromyalgia or chronic widespread pain: a randomized controlled trial and subgroup analyses. Sweden [107]. | To evaluate the effects of pool exercise in patients with fibromyalgia and chronic widespread pain and to determine characteristics influencing the effects of treatment. | Randomized controlled trial. * ¤ Procedure: 20-session exercise programme combined with a standardized 6-session education programme based on self-efficacy principles with an active control group, which undertook the same education programme. Psychoeducation Sessions: The education programme, which was designed to introduce strategies to cope with FMS symptoms, consisted of 6 1-h sessions, conducted once a week for 6 weeks. The programme was led by a physiotherapist. The pedagogical approach was based on the active participation of the patients through discussions and practical exercises. The control group received the same education programme. Exercise programme: comprised 20 sessions of 45-min pool exercise once a week for 20 weeks in temperate (33 °C) water, supervised by a physiotherapist. The exercise was planned to permit individual progress, aiming to improve overall function and to motivate regular physical activity. Follow-up: 11–12 months after the baseline. | N = 166: 134 FMS female patients + 32 chronic widespread pain (CWP) female patients. N = 81 Exercise—Education Group. [44.60 ± 9.26]. Intervention group. N = 85 Education Group. [46.50 ± 8.30]. Control Group. | 1990 ACR. | Primary outcomes: FIQ total score. Body functions (6MWT). Secondary outcomes: Pain (the FIQ Pain). Fatigue (the FIQ Fatigue). Depression (HADS-D). Health-related quality of life (SF36). Amount of leisure time physical activity (LTPAI). Exploratory outcomes: Clinical manifestations of stress (SCI). Multiple dimensions of fatigue (MFI-20). Experience in physical activity (ITT and PP). Note: PP is defined as attendance at least 60% of the sessions. | FMS patients: The exercise-education programme showed significant, but small, improvement on health status in patients with fibromyalgia and chronic widespread pain, compared with education only. Patients with milder symptoms improved most with this treatment. |
| Rook et al. (2007). Group Exercise, Education, and Combination Self-management in Women With Fibromyalgia. United States [106]. | To evaluate and directly compare the effects of 4 common self-management interventions on well-established measures of functional status, symptom severity, and self-efficacy in women with fibromyalgia. | Randomized Controlled Trial. * ¤ Procedure: Both exercise programs involved approximately 60 min of activity per session. Each session began with a brief warm-up of walking on a treadmill at a comfortable pace and then progressed to a self-determined level of moderate effort for a predetermined amount of time. All participants, regardless of fitness level, began with 5 min of walking and increased a maximum of 2 to 4 min weekly following a predetermined progression. The AE group progressed to a total of 45 min of walking. The ST group reached a maximum of 20 min of treadmill walking followed by 25 min of strength training movements. Psychoeducation Sessions: The Fibromyalgia Self-Help Course (FSHC) is a 7-session program that teaches individuals with fibromyalgia about the condition and self-management skills. Sessions were 120 min long every 2 weeks. All FSHC instructors were certified by the Arthritis Foundation. Follow-up: 6 months. | N = 207 enrolled and randomized FMS female patients. N = 138 FMS female patients who completed the intervention. N = 35 Aerobic and flexibility exercise (AE) Group [48.00 ± 11.00]. N = 35 strength training, aerobic, and flexibility exercise (ST) Group. [50.00 ± 11.00]. N = 27 the Arthritis Foundation’s Fibromyalgia Self-Help Course (FSHC) Group. [51.00 ± 12.00]. N = 38 a combination of ST and FSHC (ST-FSHC) Group. [50.00 ± 11.00]. | 1990 ACR. | Primary outcomes: Change in physical function from baseline to completion of the intervention (FIQ and SF-36). Secondary outcomes: Social and emotional function, symptoms (FIQ, the bodily pain and vitality subscales of the SF-36, and BDI). Self-efficacy (adapted Arthritis Self-Efficacy Scale). | FMS patients: progressive walking, simple strength training movements, and stretching activities improve functional status, key symptoms, and self-efficacy in women with fibromyalgia actively being treated with medication. The benefits of exercise are enhanced when combined with targeted self-management education. Appropriate exercise and patient education be included in the treatment of fibromyalgia. |
| King et al. (2002). The effects of exercise and education, individually or combined, in women with fibromyalgia. Canada [105]. | To examine the effectiveness of a supervised aerobic exercise program, a self-management education program, and the combination of exercise and education for women with fibromyalgia (FMS). | Randomized controlled trial with repeated measures design. * ¤ Procedure: The intervention programs were based upon principles of self-management (Bandura’s social cognitive theory). Treatment programs ran simultaneously for 12 weeks. Due to the large number of subjects required, the programs were offered on 5 different occasions over a 2 year period (winter–spring once, fall–winter, and spring–summer twice each). Education Group: met once a week for one and a half to 2 h per session. Exercise and education group: combined exercise and education programs. The educational component was the same as for the education-only group. The exercise-only group met twice per week and on the third day met for education and then exercise. Control group: On the day of the initial assessment, they were given a page of instructions for basic stretches and 5 items related to general coping strategies. They were contacted once or twice throughout the 12-week period to ensure they were filling out their logbook and to answer any questions. Subjects from the control group were offered one of the intervention programs at the end of the follow-up period. Follow-up: 3 months. | N = 170 FMS female patients. N = 46 Exercise Group. [45.2 ± 9.4]. N = 48 Education Group. [44.9 ± 10.0]. N = 37 Exercise & Education Group. [47.4 ± 9.0]. N = 39 Control Group. [47.3 ± 7.3]. | 1990 ACR. | SE. SE Pain. SE Function. SE Coping with symptoms. FIQ. 6MW. Tender Point Count. Total Survey Site Score. | FMS patients: subjects receiving the combination of exercise and education and who complied with the treatment protocol improved their perceived ability to cope with other symptoms. A supervised exercise program increased walking distance at post-test, an increase that was maintained at follow-up in the exercise-only group. Results demonstrate the challenges with conducting exercise and education studies in persons with FMS. |
3.2. Psychoeducation and Emotional, Clinical, and Functional Related-Outcomes in Fibromyalgia Syndrome
3.3. Structure of the Fibromyalgia Syndrome Psychoeducation Programs
| Study (Author and Year) | Psychoeducation Program Content |
|---|---|
| Antunes et al. (2022) [97]. |
|
| Pérez-Aranda et al. (2021) [98]. |
|
| Melin et al. (2018). Affect School [99]. |
(1) Joy; (2) Fear; (3) Interest and surprise; (4) Shame; (5) Anger; (6) Distaste and dissmell; (7) Distress; (8) Pain.
(2) How we act in different situations and how we interpret experiences are depending on our scripts; (3) Scripts are formed by family rules and common cultural rules for how affects should be handled; (4) Intensity and expressions of emotion are controlled by scripts; (5) Affects can be completely suppressed and thereby unconscious.
(2) How do you know that you feel…? (3) Do you feel … in a particular place in your body? (4) Does it happen often that you feel…? (5) How do you know that someone else is…? (6) Can you understand and accept another person’s…? |
| Feliu-Soler et al. (2016). FibroQoL. [102]. |
|
| Bourgault et al. (2015) [104]. |
|
| Dowd et al. (2015) [103]. |
|
| Luciano et al. (2011) [100]. Luciano et al. (2013) [101]. |
|
| Mannerkorpi et al. (2009) [107]. |
|
| Rook et al. (2007) [106]. | The Fibromyalgia Self-Help Course (FSHC):
|
| King et al. (2002) [105]. |
|
3.4. Risk of Bias
| Study (Author and Year) | Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | General Assessment (Low, Medium, High) |
|---|---|---|---|---|---|---|---|---|
| Antunes et al. (2022) [97]. | H | L | H | L | L | L | Yes | Medium |
| Pérez-Aranda et al. (2021) [98]. | H | H | H | H | L | L | Yes | Low |
| Melin et al. (2018) [99]. | H | H | H | H | L | L | Yes | Low |
| Feliu-Soler et al. (2016) [102]. | L | L | L | L | L | L | Yes | High |
| Bourgault et al. (2015) [104]. | L | L | L | L | L | L | Yes | High |
| Dowd et al. (2015) [103]. | L | L | H | H | L | L | Yes | Medium |
| Luciano et al. (2013) [101]. | L | L | L | L | L | L | Yes | High |
| Luciano et al. (2011) [100]. | L | L | L | L | L | L | Yes | High |
| Mannerkorpi et al. (2009) [107]. | L | L | L | L | L | L | Yes | High |
| Rook et al. (2007) [106]. | L | L | L | L | L | L | Yes | High |
| King et al. (2002) [105]. | L | L | L | L | L | L | Yes | High |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Thieme, K.; Turk, D.C.; Flor, H. Comorbid depression and anxiety in fibromyalgia syndrome: Relationship to somatic and psychosocial variables. Psychosom. Med. 2004, 66, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.L.; Huang, C.J.; Fang, S.C.; Ko, L.H.; Tsai, P.S. Cognitive Impairment in Fibromyalgia: A Meta-Analysis of Case-Control Studies. Psychosom. Med. 2018, 80, 432–438. [Google Scholar] [CrossRef]
- Teodoro, T.; Edwards, M.J.; Isaacs, J.D. A unifying theory for cognitive abnormalities in functional neurological disorders, fibromyalgia and chronic fatigue syndrome: Systematic review. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1308–1319. [Google Scholar] [CrossRef]
- Galvez-Sanchez, C.M.; Reyes del Paso, G.A.; Duschek, S. Cognitive impairments in fibromyalgia syndrome: Associations with positive and negative affect, alexithymia, pain catastrophizing and self-esteem. Front. Psychol. 2018, 9, 377. [Google Scholar] [CrossRef]
- Reyes del Paso, G.A.; Pulgar, A.; Duschek, S.; Garrido, S. Cognitive impairment in fibromyalgia syndrome: The impact of pain, emotional disorders, medication, and cardiovascular regulation. Eur. J. Pain 2012, 16, 421–429. [Google Scholar] [CrossRef]
- Srinivasan, S.; Maloney, E.; Wright, B.; Kennedy, M.; Kallail, K.J.; Rasker, J.J.; Häuser, W.; Wolfe, F. The Problematic Nature of Fibromyalgia Diagnosis in the Community. ACR Open Rheumatol. 2019, 1, 43–51. [Google Scholar] [CrossRef]
- Wolfe, F.; Walitt, B.; Perrot, S.; Rasker, J.J.; Häuser, W. Fibromyalgia diagnosis and biased assessment: Sex, prevalence and bias. PLoS ONE 2018, 13, e0203755. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Duschek, S.; Del Paso, G.A.R. Pain catastrophizing mediates the negative influence of pain and trait-anxiety on health-related quality of life in fibromyalgia. Qual. Life Res. 2020, 29, 1871–1881. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Duschek, S.; Reyes del Paso, A. Depression and trait-anxiety mediate the influence of clinical pain on health-related quality of life in fibromyalgia. J. Affect. Disord. 2020, 265, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Perrot, S.; Vicaut, E.; Servant, D.; Ravaud, P. Prevalence of fibromyalgia in France: A multi-step study research combining national screening and clinical confirmation: The DEFI study (Determination of Epidemiology of FIbromyalgia). BMC Musculoskelet. Disord. 2011, 12, 224. [Google Scholar] [CrossRef]
- Lee, J.W.; Lee, K.E.; Park, D.J.; Kim, S.H.; Nah, S.S.; Lee, J.H.; Kim, S.K.; Lee, Y.A.; Hong, S.J.; Kim, H.S.; et al. Determinants of quality of life in patients with fibromyalgia: A structural equation modeling approach. PLoS ONE 2017, 12, e0171186. [Google Scholar] [CrossRef] [PubMed]
- Montoro, C.I.; Galvez-Sánchez, C.M. The Mediating Role of Depression and Pain Catastrophizing in the Relationship between Functional Capacity and Pain Intensity in Patients with Fibromyalgia. Behav. Neurol. 2022, 2022, 9770047. [Google Scholar] [CrossRef] [PubMed]
- Galvez-Sánchez, C.M.; Duschek, S.; Reyes Del Paso, G.A. Psychological impact of fibromyalgia: Current perspectives. Psychol. Res. Behav. Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef]
- Montoro, C.I.; Reyes del Paso, G.A.; Duschek, S. Alexithymia in fibromyalgia syndrome. Pers. Individ. Differ. 2016, 102, 170–179. [Google Scholar] [CrossRef]
- Castelli, L.; Tesio, V.; Colonna, F.; Molinaro, S.; Leombruni, P.; Bruzzone, M.; Fusaro, E.; Sarzi-Puttini, P.; Torta, R. Alexithymia and psychological distress in fibromyalgia: Prevalence and relation with quality of life. Clin. Exp. Rheumatol. 2012, 30 (Suppl. 74), 70–77. [Google Scholar]
- Vural, M.; Berkol, T.D.; Erdogdu, Z.; Kucukserat, B.; Aksoy, C. Evaluation of personality profile in patients with fibromyalgia syndrome and healthy controls. Mod. Rheumatol. 2014, 24, 823–828. [Google Scholar] [CrossRef]
- Montoro, C.I.; Duschek, S.; Muñoz Ladrón de Guevara, C.; Fernández-Serrano, M.J.; Reyes del Paso, G.A. Aberrant cerebral blood flow responses during cognition: Implications for the understanding of cognitive deficits in fibromyalgia. Neuropsychology 2015, 29, 173–182. [Google Scholar] [CrossRef]
- Malin, K.; Littlejohn, G.O. Personality and fibromyalgia syndrome. Open Rheumatol. J. 2012, 6, 273–285. [Google Scholar] [CrossRef]
- Uguz, F.; Ciçek, E.; Salli, A.; Karahan, A.Y.; Albayrak, I.; Kaya, N.; Uğurlu, H. Axis I and Axis II psychiatric disorders in patients with fibromyalgia. Gen. Hosp. Psychiatry 2010, 32, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Gumà-Uriel, L.; Peñarrubia-María, M.T.; Cerdà-Lafont, M.; Cunillera-Puertolas, O.; Almeda-Ortega, J.; Fernández-Vergel, R.; García-Campayo, J.; Luciano, J.V. Impact of IPDE-SQ personality disorders on the healthcare and societal costs of fibromyalgia patients: A cross-sectional study. BMC Fam. Pract. 2016, 17, 61. [Google Scholar] [CrossRef] [PubMed]
- van Middendorp, H.; Lumley, M.A.; Jacobs, J.W.; van Doornen, L.J.; Bijlsma, J.W.; Geenen, R. Emotions and emotional approach and avoidance strategies in fibromyalgia. J. Psychosom. Res. 2008, 64, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Denollet, J. DS14: Standard assessment of negative affectivity, social inhibition, and Type D personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Garaigordobil, M. Fibromialgia: Discapacidad funcional, autoestima y perfil de personalidad. Inf. Psicol. 2013, 106, 4–16. [Google Scholar] [CrossRef]
- Michielsen, H.J.; Van Houdenhove, B.; Leirs, I.; Vandenbroeck, A.; Onghena, P. Depression, attribution style and self-esteem in chronic fatigue syndrome and fibromyalgia patients: Is there a link? Clin. Rheumatol. 2006, 25, 183–188. [Google Scholar] [CrossRef]
- Vong, S.K.; Cheing, G.L.; Chan, C.C.; Chan, F.; Leung, A.S. Measurement structure of the Pain Self-Efficacy Questionnaire in a sample of Chinese patients with chronic pain. Clin. Rehabil. 2009, 23, 1034–1043. [Google Scholar] [CrossRef]
- Mannerkorpi, K.; Svantesson, U.; Broberg, C. Relationships between performance-based tests and patients’ ratings of activity limitations, self-efficacy, and pain in fibromyalgia. Arch. Phys. Med. Rehabil. 2006, 87, 259–264. [Google Scholar] [CrossRef]
- Baptista, A.S.; Villela, A.L.; Jones, A.; Natour, J. Effectiveness of dance in patients with fibromyalgia: A randomized, single-blind, controlled study. Clin. Exp. Rheumatol. 2012, 30 (Suppl. 74), 18–23. [Google Scholar]
- Van Overmeire, R.; Vesentini, L.; Vanclooster, S.; Muysewinkel, E.; Bilsen, J. Body Image, Medication Use, and Mental Health among Women with Fibromyalgia in Flanders, Belgium. Int. J. Environ. Res. Public Health 2022, 19, 1418. [Google Scholar] [CrossRef]
- Varallo, G.; Suso-Ribera, C.; Ghiggia, A.; Veneruso, M.; Cattivelli, R.; Guerrini Usubini, A.; Franceschini, C.; Musetti, A.; Plazzi, G.; Fontana, J.M.; et al. Catastrophizing, Kinesiophobia, and Acceptance as Mediators of the Relationship between Perceived Pain Severity, Self-Reported and Performance-Based Physical Function in Women with Fibromyalgia and Obesity. J. Pain Res. 2022, 15, 3017–3029. [Google Scholar] [CrossRef] [PubMed]
- Scarpina, F.; Ghiggia, A.; Vaioli, G.; Varallo, G.; Capodaglio, P.; Arreghini, M.; Castelli, L. Altered recognition of fearful and angry facial expressions in women with fibromyalgia syndrome: An experimental case-control study. Sci. Rep. 2022, 12, 21498. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Jbali, L.R.; Montoro, C.I.; Montoya, P.; Halder, W.; Duschek, S. Central nervous activity during implicit processing of emotional face expressions in fibromyalgia syndrome. Brain Res. 2021, 1758, 147333. [Google Scholar] [CrossRef]
- Fischer-Jbali, L.R.; Montoro, C.I.; Montoya, P.; Halder, W.; Duschek, S. Central nervous activity during a dot probe task with facial expressions in fibromyalgia. Biol. Psychol. 2022, 172, 108361. [Google Scholar] [CrossRef] [PubMed]
- Amaro-Díaz, L.; Montoro, C.I.; Fischer-Jbali, L.R.; Galvez-Sánchez, C.M. Chronic Pain and Emotional Stroop: A Systematic Review. J. Clin. Med. 2022, 11, 3259. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Jbali, L.R.; Montoro, C.I.; Montoya, P.; Halder, W.; Duschek, S. Central nervous activity during an emotional Stroop task in fibromyalgia syndrome. Int. J. Psychophysiol. 2022, 177, 133–144. [Google Scholar] [CrossRef]
- Choy, E.; Perrot, S.; Leon, T.; Kaplan, J.; Petersel, D.; Ginovker, A.; Kramer, E. A patient survey of the impact of fibromyalgia and the journey to diagnosis. BMC Health Serv. Res. 2010, 10, 102. [Google Scholar] [CrossRef]
- Hooten, W.M.; Timming, R.; Belgrade, M.; Gaul, J.; Goertz, M.; Haake, B.; Walker, N. Assessment and Management of Chronic Pain; Institute for Clinical Systems Improvement (ICSI): Bloomington, MN, USA, 2013. [Google Scholar]
- Moyano, S.; Kilstein, J.G.; de Miguel, C.A. Nuevos criterios diagnósticos de fibromialgia: ¿vinieron para quedarse? Reumatol. Clin. 2014, 3, 716–721. [Google Scholar] [CrossRef]
- Okifuji, A.; Turk, D.C.; Sinclair, J.D.; Starz, T.W.; Marcus, D.A. A standardized manual tender point survey. I. Development and determination of a threshold point for the identification of positive tender points in fibromyalgia syndrome. J. Rheumatol. 1997, 24, 377–383. [Google Scholar]
- Montoro, C.I.; Duschek, S.; de Guevara, C.M.; Reyes Del Paso, G.A. Patterns of Cerebral Blood Flow Modulation During Painful Stimulation in Fibromyalgia: A Transcranial Doppler Sonography Study. Pain Med. 2016, 17, 2256–2267. [Google Scholar] [CrossRef]
- de la Coba, P.; Montoro, C.I.; Reyes Del Paso, G.A.; Galvez-Sánchez, C.M. Algometry for the assessment of central sensitisation to pain in fibromyalgia patients: A systematic review. Ann. Med. 2022, 54, 1403–1422. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Muñoz Ladrón de Guevara, C.; Montoro, C.I.; Fernández-Serrano, M.J.; Duschek, S.; Reyes Del Paso, G.A. Cognitive deficits in fibromyalgia syndrome are associated with pain responses to low intensity pressure stimulation. PLoS ONE 2018, 13, e0201488. [Google Scholar] [CrossRef] [PubMed]
- de la Coba, P.; Bruehl, S.; Galvez-Sánchez, C.M.; Reyes Del Paso, G.A. Slowly Repeated Evoked Pain as a Marker of Central Sensitization in Fibromyalgia: Diagnostic Accuracy and Reliability in Comparison with Temporal Summation of Pain. Psychosom. Med. 2018, 80, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Gracely, R.H.; Geisser, M.E.; Giesecke, T.; Grant, M.A.; Petzke, F.; Williams, D.A.; Clauw, D.J. Pain catastrophizing and neural responses to pain among persons with fibromyalgia. Brain 2004, 127 Pt 4, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Millan, M.J. Descending control of pain. Prog. Neurobiol. 2002, 66, 355–474. [Google Scholar] [CrossRef]
- Julien, N.; Goffaux, P.; Arsenault, P.; Marchand, S. Widespread pain in fibromyalgia is related to a deficit of endogenous pain inhibition. Pain 2005, 114, 295–302. [Google Scholar] [CrossRef]
- Russell, I.J.; Orr, M.D.; Littman, B.; Vipraio, G.A.; Alboukrek, D.; Michalek, J.E.; Lopez, Y.; MacKillip, F. Elevated cerebrospinal fluid levels of substance P in patients with the fibromyalgia syndrome. Arthritis Rheum. 1994, 37, 1593–1601. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152 (Suppl. 3), S2–S15. [Google Scholar] [CrossRef]
- Scholz, J.; Woolf, C.J. Can we conquer pain? Nat. Neurosci. 2002, 5, 1062–1067. [Google Scholar] [CrossRef]
- Clauw, D.J. Diagnosing and treating chronic musculoskeletal pain based on the underlying mechanism(s). Best Pract. Res. Clin. Rheumatol. 2015, 29, 6–19. [Google Scholar] [CrossRef]
- Woolf, C.J.; Salter, M.W. Neuronal plasticity: Increasing the gain in pain. Science 2000, 288, 1765–1768. [Google Scholar] [CrossRef] [PubMed]
- Staud, R.; Koo, E.; Robinson, M.E.; Price, D.D. Spatial summation of mechanically evoked muscle pain and painful aftersensations in normal subjects and fibromyalgia patients. Pain 2007, 130, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Gebhart, G.F. Descending modulation of pain. Neurosci. Biobehav. Rev. 2004, 27, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Price, D.D.; Staud, R. Neurobiology of fibromyalgia syndrome. J. Rheumatol. 2005, 75, 22–28. [Google Scholar]
- Arnold, L.M.; Hudson, J.I.; Hess, E.V.; Ware, A.E.; Fritz, D.A.; Auchenbach, M.B.; Starck, L.O.; Keck, P.E., Jr. Family study of fibromyalgia. Arthritis Rheum. 2004, 50, 944–952. [Google Scholar] [CrossRef]
- Buskila, D.; Sarzi-Puttini, P. Biology and therapy of fibromyalgia. Genetic aspects of fibromyalgia syndrome. Arthritis Res. Ther. 2006, 8, 218. [Google Scholar] [CrossRef] [PubMed]
- Farhad, K.; Oaklander, A.L. Fibromyalgia and small-fiber polyneuropathy: What’s in a name? Muscle Nerve 2018, 58, 611–613. [Google Scholar] [CrossRef]
- Martínez-Lavín, M. Fibromyalgia and small fiber neuropathy: The plot thickens! Clin. Rheumatol. 2018, 37, 3167–3171. [Google Scholar] [CrossRef]
- Álvarez-Gallardo, I.C.; Bidonde, J.; Busch, A.; Westby, M.; Kenny, G.P.; Delgado-Fernández, M.; Carbonell-Baeza, A.; Rahman, P.; De Angelis, G.; Brosseau, L. Therapeutic validity of exercise interventions in the management of fibromyalgia. J. Sports Med. Phys. Fitness 2019, 59, 828–838. [Google Scholar] [CrossRef]
- Arnold, L.M.; Gebke, K.B.; Choy, E.H. Fibromyalgia: Management strategies for primary care providers. Int. J. Clin. Pract. 2016, 70, 99–112. [Google Scholar] [CrossRef]
- González, E.; Elorza, J.; Failde, I. Comorbilidad psiquiátrica y Fibromialgia. Su efecto sobre la calidad de vida de los pacientes [Psychiatric comorbidity and Fibromyalgia and Its effect on the quality of life of patients]. Actas Esp. Psiquiatr. 2010, 38, 295–300. [Google Scholar] [PubMed]
- Samami, E.; Shahhosseini, Z.; Elyasi, F. The Effect of Psychological Interventions on the Quality of Life in Women with Fibromyalgia: A Systematic Review. J. Clin. Psychol. Med. Settings 2021, 28, 503–517. [Google Scholar] [CrossRef] [PubMed]
- Sumpton, J.E.; Moulin, D.E. Fibromyalgia: Presentation and management with a focus on pharmacological treatment. Pain Res. Manag. 2008, 13, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Winkelmann, A.; Bork, H.; Brückle, W.; Dexl, C.; Heldmann, P.; Henningsen, P.; Krumbein, L.; Pullwitt, V.; Schiltenwolf, M.; Häuser, W. Physiotherapie, Ergotherapie und physikalische Verfahren beim Fibromyalgiesyndrom: Aktualisierte Leitlinie 2017 und Übersicht von systematischen Übersichtsarbeiten [Physiotherapy, occupational therapy and physical therapy in fibromyalgia syndrome: Updated guidelines 2017 and overview of systematic review articles]. Schmerz 2017, 31, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Pardos-Gascón, E.M.; Narambuena, L.; Leal-Costa, C.; van-der Hofstadt-Román, C.J. Differential efficacy between cognitive-behavioral therapy and mindfulness-based therapies for chronic pain: Systematic review. Int. J. Clin. Health Psychol. 2021, 21, 100197. [Google Scholar] [CrossRef]
- Hassett, A.L.; Gevirtz, R.N. Nonpharmacologic treatment for fibromyalgia: Patient education, cognitive-behavioral therapy, relaxation techniques, and complementary and alternative medicine. Rheum. Dis. Clin. N. Am. 2009, 35, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Haugmark, T.; Hagen, K.B.; Smedslund, G.; Zangi, H.A. Mindfulness- and acceptance-based interventions for patients with fibromyalgia—A systematic review and meta-analyses. PLoS ONE 2019, 14, e0221897. [Google Scholar] [CrossRef]
- Adler-Neal, A.L.; Zeidan, F. Mindfulness Meditation for Fibromyalgia: Mechanistic and Clinical Considerations. Curr. Rheumatol. Rep. 2017, 19, 59. [Google Scholar] [CrossRef]
- Bravo, C.; Skjaerven, L.H.; Guitard Sein-Echaluce, L.; Catalan-Matamoros, D. Effectiveness of movement and body awareness therapies in patients with fibromyalgia: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2019, 55, 646–657. [Google Scholar] [CrossRef]
- Simister, H.D.; Tkachuk, G.A.; Shay, B.L.; Vincent, N.; Pear, J.J.; Skrabek, R.Q. Randomized Controlled Trial of Online Acceptance and Commitment Therapy for Fibromyalgia. J. Pain 2018, 19, 741–753. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Moreno-Padilla, M.; Reyes Del Paso, G.A.; de la Coba, P. Effectiveness of Acceptance and Commitment Therapy in Central Pain Sensitization Syndromes: A Systematic Review. J. Clin. Med. 2021, 10, 2706. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association APA—División 12. Treatment Target: Fibromyalgia. 2023. APA. Available online: https://div12.org/diagnosis/fibromyalgia/ (accessed on 1 February 2023).
- Lumley, M.A.; Schubiner, H.; Lockhart, N.A.; Kidwell, K.M.; Harte, S.E.; Clauw, D.J.; Williams, D.A. Emotional awareness and expression therapy, cognitive behavioral therapy, and education for fibromyalgia: A cluster-randomized controlled trial. Pain 2017, 158, 2354–2363. [Google Scholar] [CrossRef] [PubMed]
- Thieme, K.; Turk, D.C. Cognitive-behavioral and operant-behavioral therapy for people with fibromyalgia. Reumatismo 2012, 64, 275–285. [Google Scholar] [CrossRef]
- García-Torres, F.; Alós, F.J.; Pérez-Dueñas, C.; Morina, J.A. Guía de Tratamientos Psicológicos Eficaces en Psiconcología. Alteraciones Psicológicas y Físicas; Pirámide Editorial: Madrid, Spain, 2016. [Google Scholar]
- Veehof, M.M.; Oskam, M.J.; Schreurs, K.M.G.; Bohlmeijer, E.T. Acceptance-based interventions for the treatment of chronic pain: A systematic review and meta-analysis. Pain 2011, 152, 533–542. [Google Scholar] [CrossRef]
- Ducasse, D.; Fond, G. Acceptance and commitment therapy. Encephale 2015, 41, 1–9. [Google Scholar] [CrossRef]
- Araújo, F.M.; DeSantana, J.M. Physical therapy modalities for treating fibromyalgia. F1000Res 2019, 8, 17176. [Google Scholar] [CrossRef]
- Assumpção, A.; Pagano, T.; Matsutani, L.A.; Ferreira, E.A.; Pereira, C.A.; Marques, A.P. Quality of life and discriminating power of two questionnaires in fibromyalgia patients: Fibromyalgia impact Questionnaire and medical outcomes study 36-Item short-form health survey. Rev. Bras. Fisioter. 2010, 14, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Okifuji, A.; Donaldson, G.W.; Barck, L.; Fine, P.G. Relationship between fibromyalgia and obesity in pain, function, mood, and sleep. J. Pain 2010, 11, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- Muñoz Ladrón de Guevara, C.; Reyes Del Paso, G.A.; Fernández Serrano, M.J.; Montoro, C.I. Fibromyalgia Syndrome and Cognitive Decline: The Role of Body Mass Index and Clinical Symptoms. J. Clin. Med. 2022, 11, 3404. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Morlion, B.; Kempke, S.; Luyten, P.; Coppens, E.; Van Wambeke, P. Multidisciplinary pain education program (MPEP) for chronic pain patients: Preliminary evidence for effectiveness and mechanisms of change. Curr. Med. Res. Opin. 2011, 27, 1595–1601. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, B.P.; Newman, A.K.; Moraís, C.A.; Burns, J.W.; Eyer, J.C.; Thorn, B.E. Heterogeneity of Treatment Effects in a Randomized Trial of Literacy-Adapted Group Cognitive-Behavioral Therapy, Pain Psychoeducation, and Usual Medical Care for Multiply Disadvantaged Patients with Chronic Pain. J. Pain 2019, 20, 1236–1248. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Poli, A.; Ciacchini, R.; Hitchcott, P.; Bazzichi, L.; Gemignani, A. A psychoeducational intervention is a treatment for fibromyalgia syndrome. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 116), 98–104. [Google Scholar] [PubMed]
- Daviet, J.C.; Bonan, I.; Caire, J.M.; Colle, F.; Damamme, L.; Froger, J.; Leblond, C.; Leger, A.; Muller, F.; Simon, O.; et al. Therapeutic patient education for stroke survivors: Non-pharmacological management. A literature review. Ann. Phys. Rehabil. Med. 2012, 55, 641–656. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K. Patient Education: A Practical Approach; Sage: Thousand Oaks, CA, USA, 2021. [Google Scholar]
- García-Ríos, M.C.; Navarro-Ledesma, S.; Tapia-Haro, R.M.; Toledano-Moreno, S.; Casas-Barragán, A.; Correa-Rodríguez, M.; Aguilar-Ferrándiz, M.E. Effectiveness of health education in patients with fibromyalgia: A systematic review. Eur. J. Phys. Rehabil. Med. 2019, 55, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Perrot, S.; Fitzcharles, M.A. Management of fibromyalgia: Practical guides from recent evidence-based guidelines. Pol. Arch. Intern. Med. 2017, 127, 47–56. [Google Scholar] [CrossRef]
- Häuser, W.; Thieme, K.; Turk, D.C. Guidelines on the management of fibromyalgia syndrome—A systematic review. Eur. J. Pain 2010, 14, 5–10. [Google Scholar] [CrossRef]
- Carville, S.F.; Arendt-Nielsen, L.; Bliddal, H.; Blotman, F.; Branco, J.C.; Buskila, D.; Da Silva, J.A.; Danneskiold-Samsøe, B.; Dincer, F.; Henriksson, C.; et al. EULAR evidence-based recommendations for the management of fibromyalgia syndrome. Ann. Rheum. Dis. 2008, 67, 536–541. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Giorgi, V.; Atzeni, F.; Gorla, R.; Kosek, E.; Choy, E.H.; Bazzichi, L.; Häuser, W.; Ablin, J.N.; Aloush, V.; et al. Diagnostic and therapeutic care pathway for fibromyalgia. Clin. Exp. Rheumatol. 2021, 39 (Suppl. 130), 120–127. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Giorgi, V.; Atzeni, F.; Gorla, R.; Kosek, E.; Choy, E.H.; Bazzichi, L.; Häuser, W.; Ablin, J.N.; Aloush, V.; et al. Fibromyalgia position paper. Clin. Exp. Rheumatol. 2021, 39 (Suppl. 130), 186–193. [Google Scholar] [CrossRef]
- Berard, A.A.; Smith, A.P. Post Your Journey: Instagram as a Support Community for People with Fibromyalgia. Qual. Health Res. 2019, 29, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Antunes, M.D.; Schmitt, A.C.B.; Marques, A.P. Amigos de Fibro (Fibro Friends): Validation of an Educational Program to Promote Health in Fibromyalgia. Int. J. Environ. Res. Public Health 2022, 19, 5297. [Google Scholar] [CrossRef]
- Pérez-Aranda, A.; Angarita-Osorio, N.; Feliu-Soler, A.; Andrés-Rodríguez, L.; Borràs, X.; Luciano, J.V. Do humor styles predict clinical response to the MINDSET (MINDfulneSs & EducaTion) program? A pilot study in patients with fibromyalgia. Reumatol. Clin. (Engl. Ed.) 2021, 17, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Melin, E.O.; Svensson, R.; Thulesius, H.O. Psychoeducation against depression, anxiety, alexithymia and fibromyalgia: A pilot study in primary care for patients on sick leave. Scand. J. Prim. Health Care 2008, 36, 123–133. [Google Scholar] [CrossRef]
- Luciano, J.V.; Martínez, N.; Peñarrubia-María, M.T.; Fernández-Vergel, R.; García-Campayo, J.; Verduras, C.; Blanco, M.E.; Jiménez, M.; Ruiz, J.M.; López del Hoyo, Y.; et al. Effectiveness of a psychoeducational treatment program implemented in general practice for fibromyalgia patients: A randomized controlled trial. Clin. J. Pain 2011, 27, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Luciano, J.V.; Sabes-Figuera, R.; Cardeñosa, E.T.; Peñarrubia-María, M.; Fernández-Vergel, R.; García-Campayo, J.; Knapp, M.; Serrano-Blanco, A. Cost-utility of a psychoeducational intervention in fibromyalgia patients compared with usual care: An economic evaluation alongside a 12-month randomized controlled trial. Clin. J. Pain 2013, 29, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Feliu-Soler, A.; Borràs, X.; Peñarrubia-María, M.T.; Rozadilla-Sacanell, A.; D’Amico, F.; Moss-Morris, R.; Howard, M.A.; Fayed, N.; Soriano-Mas, C.; Puebla-Guedea, M.; et al. Cost-utility and biological underpinnings of Mindfulness-Based Stress Reduction (MBSR) versus a psychoeducational programme (FibroQoL) for fibromyalgia: A 12-month randomized controlled trial (EUDAIMON study). BMC Complement. Altern. Med. 2016, 16, 81. [Google Scholar] [CrossRef]
- Dowd, H.; Hogan, M.J.; McGuire, B.E.; Davis, M.C.; Sarma, K.M.; Fish, R.A.; Zautra, A.J. Comparison of an Online Mindfulness-based Cognitive Therapy Intervention with Online Pain Management Psychoeducation: A Randomized Controlled Study. Clin. J. Pain 2015, 31, 517–527. [Google Scholar] [CrossRef]
- Bourgault, P.; Lacasse, A.; Marchand, S.; Courtemanche-Harel, R.; Charest, J.; Gaumond, I.; Barcellos de Souza, J.; Choinière, M. Multicomponent interdisciplinary group intervention for self-management of fibromyalgia: A mixed-methods randomized controlled trial. PLoS ONE 2015, 10, e0126324. [Google Scholar] [CrossRef]
- King, S.J.; Wessel, J.; Bhambhani, Y.; Sholter, D.; Maksymowych, W. The effects of exercise and education, individually or combined, in women with fibromyalgia. J. Rheumatol. 2002, 29, 2620–2627. [Google Scholar] [PubMed]
- Rooks, D.S.; Gautam, S.; Romeling, M.; Cross, M.L.; Stratigakis, D.; Evans, B.; Goldenberg, D.L.; Iversen, M.D.; Katz, J.N. Group exercise, education, and combination self-management in women with fibromyalgia: A randomized trial. Arch. Intern. Med. 2007, 167, 2192–2200. [Google Scholar] [CrossRef] [PubMed]
- Mannerkorpi, K.; Nordeman, L.; Ericsson, A.; Arndorw, M.; GAU Study Group. Pool exercise for patients with fibromyalgia or chronic widespread pain: A randomized controlled trial and subgroup analyses. J. Rehabil. Med. 2009, 41, 751–760. [Google Scholar] [CrossRef]
- Iannuccelli, C.; Lucchino, B.; Gioia, C.; Dolcini, G.; Favretti, M.; Franculli, D.; Di Franco, M. Mental health and well-being during the COVID-19 pandemic: Stress vulnerability, resilience and mood disturbances in fibromyalgia and rheumatoid arthritis. Clin. Exp. Rheumatol. 2021, 39 (Suppl. 130), 153–160. [Google Scholar] [CrossRef] [PubMed]
- Aloush, V.; Gurfinkel, A.; Shachar, N.; Ablin, J.N.; Elkana, O. Physical and mental impact of COVID-19 outbreak on fibromyalgia patients. Clin. Exp. Rheumatol. 2021, 39 (Suppl. 130), 108–114. [Google Scholar] [CrossRef]
- Davis, M.C.; Zautra, A.J. An online mindfulness intervention targeting socioemotional regulation in fibromyalgia: Results of a randomized controlled trial. Ann. Behav. Med. 2013, 46, 273–284. [Google Scholar] [CrossRef]
- Ljótsson, B.; Atterlöf, E.; Lagerlöf, M.; Andersson, E.; Jernelöv, S.; Hedman, E.; Kemani, M.; Wicksell, R.K. Internet-delivered acceptance and values-based exposure treatment for fibromyalgia: A pilot study. Cogn. Behav. Ther. 2014, 43, 93–104. [Google Scholar] [CrossRef]
- Lai, L.; Liu, Y.; McCracken, L.M.; Li, Y.; Ren, Z. The efficacy of acceptance and commitment therapy for chronic pain: A three-level meta-analysis and a trial sequential analysis of randomized controlled trials. Behav. Res. Ther. 2023, 165, 104308. [Google Scholar] [CrossRef]
- Gowans, S.E.; DeHueck, A.; Voss, S. A randomized, controlled trial of exercise and education for individuals with fibromyalgia. Arthritis Care Res. 1999, 12, 120–128. [Google Scholar] [CrossRef]
- Hammond, A.; Freeman, K. Community patient education and exercise for people with fibromyalgia: A parallel group randomized controlled trial. Clin. Rehabil. 2006, 20, 835–846. [Google Scholar] [CrossRef]
- Arfuch, V.M.; Caballol Angelats, R.; Aguilar Martín, C.; Carrasco-Querol, N.; Sancho Sol, M.C.; González Serra, G.; Fusté Anguera, I.; Gonçalves, A.Q.; Berenguera, A. Assessing the benefits on quality of life of a multicomponent intervention for fibromyalgia syndrome in primary care: Patients’ and health professionals’ appraisals: A qualitative study protocol. BMJ Open 2020, 10, e039873. [Google Scholar] [CrossRef]
- Serrat, M.; Sanabria-Mazo, J.P.; García-Troiteiro, E.; Fontcuberta, A.; Mateo-Canedo, C.; Almirall, M.; Feliu-Soler, A.; Méndez-Ulrich, J.L.; Sanz, A.; Luciano, J.V. Efficacy of a Multicomponent Intervention for Fibromyalgia Based on Pain Neuroscience Education, Exercise Therapy, Psychological Support, and Nature Exposure (NAT-FM): Study Protocol of a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 7, 634. [Google Scholar] [CrossRef] [PubMed]
- Bruce, B.K.; Allman, M.E.; Rivera, F.A.; Wang, B.; Berianu, F.; Butendieck, R.R.; Calamia, K.T.; Hines, S.L.; Rummans, T.A.; Niazi, S.K.; et al. Intensive Multicomponent Fibromyalgia Treatment: A Translational Study to Evaluate Effectiveness in Routine Care Delivery. J. Clin. Rheumatol. 2021, 27, e496–e500. [Google Scholar] [CrossRef] [PubMed]
- Arnold, B.; Häuser, W.; Arnold, M.; Bernateck, M.; Bernardy, K.; Brückle, W.; Friedel, E.; Hesselschwerdt, H.J.; Jäckel, W.; Köllner, V.; et al. Multimodale Therapie des Fibromyalgiesyndroms. Systematische Übersicht, Metaanalyse und Leitlinie [Multicomponent therapy of fibromyalgia syndrome. Systematic review, meta-analysis and guideline. Schmerz 2012, 26, 287–290. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galvez-Sánchez, C.M.; Montoro, C.I. Psychoeducation for Fibromyalgia Syndrome: A Systematic Review of Emotional, Clinical and Functional Related-Outcomes. Behav. Sci. 2023, 13, 415. https://doi.org/10.3390/bs13050415
Galvez-Sánchez CM, Montoro CI. Psychoeducation for Fibromyalgia Syndrome: A Systematic Review of Emotional, Clinical and Functional Related-Outcomes. Behavioral Sciences. 2023; 13(5):415. https://doi.org/10.3390/bs13050415
Chicago/Turabian StyleGalvez-Sánchez, Carmen M., and Casandra I. Montoro. 2023. "Psychoeducation for Fibromyalgia Syndrome: A Systematic Review of Emotional, Clinical and Functional Related-Outcomes" Behavioral Sciences 13, no. 5: 415. https://doi.org/10.3390/bs13050415
APA StyleGalvez-Sánchez, C. M., & Montoro, C. I. (2023). Psychoeducation for Fibromyalgia Syndrome: A Systematic Review of Emotional, Clinical and Functional Related-Outcomes. Behavioral Sciences, 13(5), 415. https://doi.org/10.3390/bs13050415