
Increasing Prevention of Mother to Child Transmission (PMTCT) Uptake through Facility-Based Health Promotion: Intervention Development
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
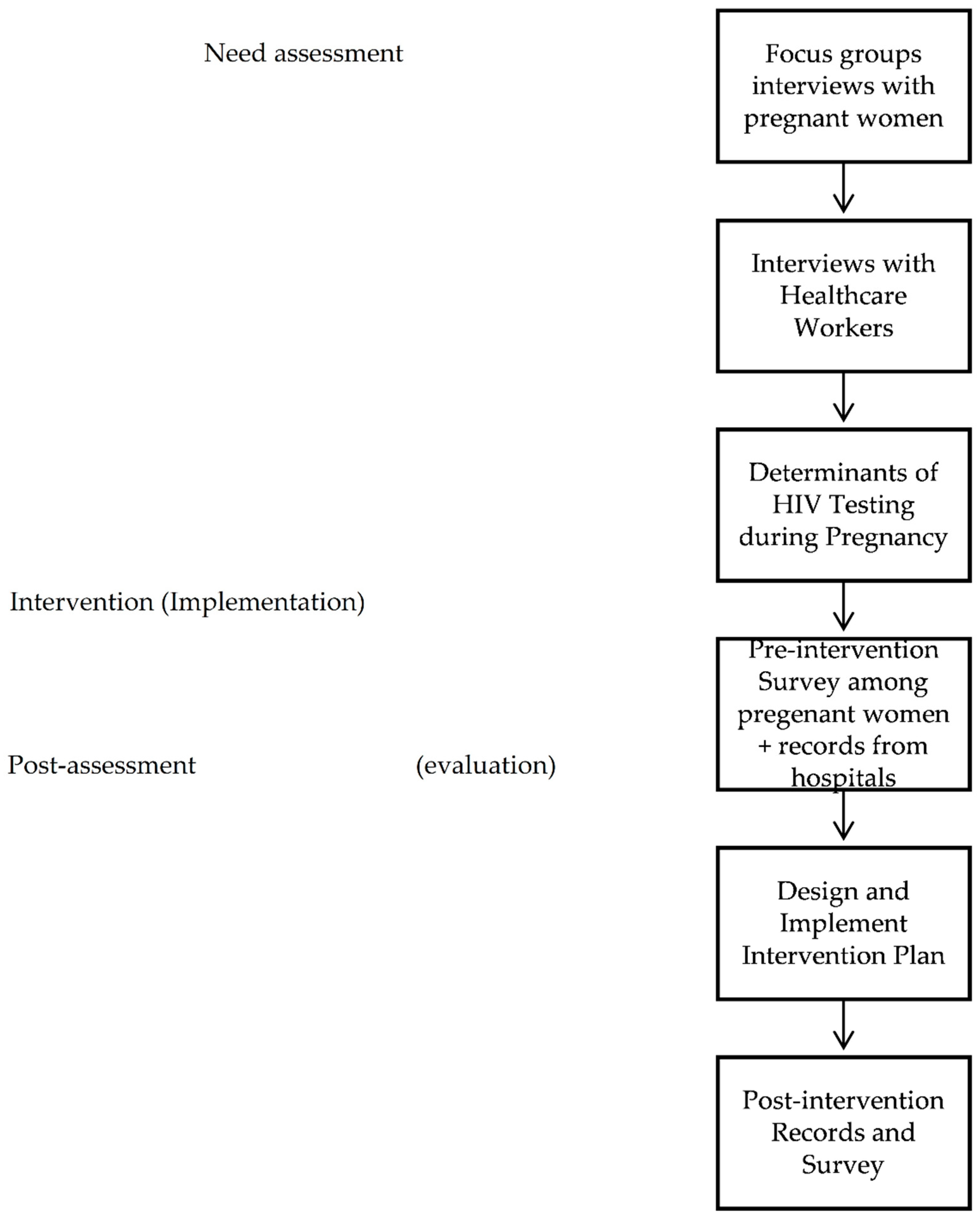
2.1. Step 1: Need Assessment
2.2. Step 2: Program Outcomes and Objectives
2.3. Step 3: Program Design
2.4. Step 4: Developing Intervention Components and Program Production
2.5. Step 5: Implementation Plan
2.6. Step 6: Evaluation Plan
3. Results
3.1. Step 1: Need Assessment
3.2. Steps 2 and 3: Program Outcomes, Objectives and Design
3.3. Steps 4 and 5: Developing Intervention Components and Implementation Plan
- Sensitization of hospital management to prioritize PMTCT. The technical advisory group that was formed from the Sudan National AIDS program (SNAP), the representative of obstetrics and genecology specialists, and the senior management in hospitals all supported this. It was agreed that the HIV test will be added to the lab prescription that has ANC routine tests. They ensured that at least twice a week a quick orientation on PMTCT is done to the doctors in the hospital. This was included as a discussion point in their monthly meetings.
- Ensuring HIV testing kits are available and no stock-out during the intervention period. This was done in collaboration with SNAP, who confirmed supplies will be provided and no stock out will happen during the intervention period. The research team followed up on a monthly basis with the PMTCT team to ensure supplies are pre-positioned.
- Orientation of doctors with reminders to offer HIV tests during ANC visits. The senior genecologists in maternity hospitals were asked to facilitate this at least twice a week. The technical advisory group was assigned to monitor this.
- Incentivizing counsellors to increase group and individual awareness and counselling for pregnant women during waiting time as well as individual counselling. The research team provided technical and supportive supervision to the counsellors in the hospitals. A limited financial incentive was also secured for the counsellors.
- Work with the lab technicians to expect an increase in HIV test requests. The research team followed up with the lab teams in the hospitals who also received orientation from the hospital management on the expected increase in the number of HIV tests.
- Mother-to-mother peer support group. We considered the educational level of pregnant women and their exposure to PMTCT and created effective awareness and counselling sessions. A group of pregnant women volunteered to support PMTCT awareness. They were trained on interpersonal communication skills and developed awareness schedules targeting their peers during the ANC visits.
- Supported aid materials. Print and audio-visual Information, Education, and Communication (IEC) materials are available and clearly visible in the waiting areas. A set of IEC materials that address the knowledge gap in relation to the individual level determinants was drafted and pre-tested among the pregnant women. These materials were then produced and placed in the waiting areas of the PMTCT sites and small leaflets were also handed to pregnant women who joins the group awareness and counselling sessions.
- Reporting: The research team worked with the PMTCT teams in the hospitals to ensure that the routine reporting systems are strengthened to capture the intervention components. For example, the number of counselling sessions conducted, the number of pregnant women that participated, and the number of pregnant women tested. As described in the evaluation section that follows, these were captured before, during, and after the intervention.
3.4. Step 6: Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Global HIV & AIDS Statistics—Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 2 February 2023).
- Reece, M.; Hollub, A.; Nangami, M.; Lane, K. Assessing male spousal engagement with prevention of mother-to-child transmission (pMTCT) programs in western Kenya. AIDS Care 2010, 6, 743–750. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. 2013 UNAIDS Report on the Global AIDS Epidemic. Available online: https://www.unaids.org/en/resources/documents/2013/20130923_UNAIDS_Global_Report_2013 (accessed on 5 January 2022).
- Eide, M.; Myhre, M.; Lindbæk, M.; Sundby, J.; Arimi, P.; Thior, I. Social consequences of HIV-positive women’s participation in prevention of mother-to-child transmission programmes. Patient Educ. Couns. 2006, 60, 148–151. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants: Recommendations for a Public Health Approach–2010 Version. Available online: https://apps.who.int/iris/handle/10665/75236 (accessed on 4 March 2022).
- Babiker, Z.O.; Mohammed, A.A.; Herieka, E.A. The current status of maternal HIV infection in Sudan: Time for action? Sudan Med. J. 2010, 46, 112–120. [Google Scholar]
- Barigye, H.; Levin, J.; Maher, D.; Tindiwegi, G.; Atuhumuza, E.; Nakibinge, S.; Grosskurth, H. Operational evaluation of a service for prevention of mother-to-child transmission of HIV in rural Uganda: Barriers to uptake of single-dose nevirapine and the role of birth reporting. Trop. Med. Int. Health 2010, 15, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- FMoH. Sudan National HIV Updated Strategic Framework. Available online: http://www.fmoh.gov.sd/ (accessed on 5 January 2015).
- SNACP. Sudan National Guidelines on PMTCT. Available online: http://www.fmoh.gov.sd/ (accessed on 4 March 2015).
- Bwirire, L.D.; Fitzgerald, M.; Zachariah, R.; Chikafa, V.; Massaquoi, M.; Moens, M.; Kamoto, K.; Schouten, E.J. Reasons for loss to follow-up among mothers registered in a prevention-of-mother-to-child transmission program in rural Malawi. R. Soc. Trop. Med. Hyg. 2008, 102, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Colvin, C.; Konopka, S.; Chalker, J.C.; Jonas, E.; Albertini, J.; Amzel, A.; Fogg, K. A Systematic Review of Health System Barriers and Enablers for Antiretroviral Therapy (ART) for HIV-Infected Pregnant and Postpartum Women. PLoS ONE 2014, 9, e108150. [Google Scholar] [CrossRef] [PubMed]
- Shroufi, A.; Mafara, E.; Sauveur, S.F.J.; Taziwa, F.; Viñoles, C.M. Mother to Mother (M2M) Peer Support for Women in Prevention of Mother to Child Transmission (PMTCT) Programmes: A Qualitative Study. PLoS ONE 2013, 8, e64717. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, L.; Grant, D.L.; Watson, J.D.; Kahawita, T.; Ong’ech, J.O.; David, R.A. Linking women who test HIV-positive in pregnancy-related services to long-term HIV care and treatment services: A systematic review. Trop. Med. Int. Health 2012, 17, 564–580. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, M.M.; Nasr, A.M.; Gassmelseed, D.E.A.; Abdalelhafiz, M.A.; Elsheikh, M.A.; Adam, I. Knowledge and Attitude Toward HIV Voluntary Counseling and Testing Services Among Pregnant Women Attending an Antenatal Clinic in Sudan. J. Med. Virol. 2007, 79, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Elsheikh, I.E.; Crutzen, R.; van den Borne, H.W. Perceptions of Sudanesewomen of reproductive age toward HIV/AIDS and services for Prevention of Mother-to-Child Transmission of HIV. BMC 2015, 15, 674. [Google Scholar] [CrossRef]
- Elsheikh, I.E.; Crutzen, R.; Adam, I.; Abdelraheem, S.I.; van den Borne, H.W. Determinants of HIV Testing during Pregnancy among Pregnant Sudanese Women: A Cross-Sectional Study. Behav. Sci. 2022, 12, 150. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, L.K.B.; Markham, C.M.; Ruiter, R.A.C.; Fernández, M.E.; Kok, G.; Parcel, G.S. Planning Health Promotion Programs: An Intervention Mapping Approach, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2016. [Google Scholar]
- Berninger, N.M.; Hoor, G.A.; Plasqui, G.; Kok, G.; Peters, G.Y.; Ruiter, R.A.C. Sedentary Work in Desk-Dominated Environments: A Data-Driven Intervention Using Intervention Mapping. JMIR Form. Res. 2020, 4, e14951. [Google Scholar] [CrossRef] [PubMed]
- Alemu, Y.; Ambaw, F.; Smith, A.W. Utilization of HIV testing services among pregnant mothers in low income primary care settings in northern Ethiopia: A cross sectional study. BMC Pregnancy Childbirth 2017, 17, 199. [Google Scholar] [CrossRef] [PubMed]
- Abtew, S.; Awoke, W.; Asrat, A. Knowledge of pregnant women on mother-to-child transmission of HIV, its prevention, and associated factors in Assosa town, Northwest Ethiopia. HIV/AIDS Res. Palliat. Care 2016, 8, 101–107. [Google Scholar] [CrossRef] [PubMed]
- De Paoli, M.M.; Manongi, R.; Klepp, K.I. Factors influencing acceptability of voluntary counselling and HIV-testing among pregnant women in Northern Tanzania. AIDS Care 2010, 16, 411–425. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.; Haidar, J. Applicability of the theory of planned behavior in predicting intended use of Voluntary HIV Counseling and Testing services among teachers of Harari Region, Ethiopia. Ethiop. J. Health Dev. 2010, 24, 96–102. [Google Scholar] [CrossRef]
- Reevesa, B.C.; Gaus, W. Guidelines for Reporting Non-Randomised Studies. Komplementärmed Kl. Nat. 2004, 11, 46–52. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Name of Hospital | Sample Size (Number of Pregnant Women) | Type of Group |
|---|---|---|
| Omdurman Maternity Hospital | 126 | Experimental (intervention) |
| Al Suadi Maternity Hospital | 115 | Control (no intervention) |
| Bahri Teaching Hospital | 77 | Control (no intervention) |
| Al Turki Naternity Hospital | 67 | Experimental (intervention) |
| Total | 385 |
| Existing Practices/Behaviours According to the Assessment | Determinants | Performance Objective | Proposed Interventions | Expected Effect |
|---|---|---|---|---|
| Strong coordination and advocacy with hospitals to support the intervention plan is needed | Willingness and support of the senior management in hospitals | Establish a technical advisory group to strengthen the coordination and ensure buy-in | Regular meetings, sensitization | Improved coordination and accountability to support the PMTCT intervention |
| Doctors are not offering the HIV test for the pregnant women | No clear policy directive. Very busy schedule and a lot of pregnant women coming, time-consuming Not a priority compared to other aspects of health care | Doctors offer HIV tests to pregnant women during their ANC visits | 1. Sensitization of doctors, including the issuance of a clear policy directive from the director of the hospital 2. Key reminders and follow up with doctors | Increase in percent of pregnant women tested for HIV |
| Lab technicians/staff are not prepared for an additional number of HIV tests | Perceived as an additional burden | Ensure that testing kits for HIV tests are available Lab technicians are aware and committed to the expected increase in HIV tests | 1. Provision of adequate testing kits 2. Reminders for the lab technicians | Quick and fast HIV tests are performed for pregnant women |
| Counsellors are not used to additional counselling sessions (pre and post-test sessions) | Perceived as an additional burden | Counsellors are prepared for additional counselling sessions following the expected increase of number of women who will be tested | 1. Provision of supportive aid, e.g., IEC materials 2. Reminders and financial incentives for counsellors | Quality counselling sessions with more pregnant women involved |
| Existing Practices/Behaviours According to the Assessment | Determinants | Performance Objective | Proposed Interventions | Expected Effect |
|---|---|---|---|---|
| Pregnant women (PW) are not aware about the benefits of PMTCT | Limited knowledge about the PMTCT services and benefits Limited and poor public counselling sessions at PMTCT site | Ensure that 85% of pregnant women attending the ANC are exposed to HIV awareness Refresher training of the counsellors to ensure quality sessions | Awareness-raising sessions through counsellors and IEC materials (Print + TV screen) Mass-media short messages about importance of HIV test during pregnancy Peer education groups from PW themselves | Increase in knowledge among PW |
| Pregnant women are scared when they hear about HIV and AIDS | Scared of being positive and the consequences Believe that it is a chronic killing disease Lack of in-depth discussion on PMTCT | Ensure that 75% of pregnant women attending the ANC are exposed to quality HIV counselling | Counselling sessions targeting MTCT knowledge gaps Improved counselling by ensuring sessions are well-designed and tailored to the issues identified in our assessment Stigma reduction through giving examples of successful delivery of HIV positive women and the fact that with the ARV people with HIV lives productive life | Pregnant women are better prepared to accept HIV tests during pregnancy |
| Pregnant women are not convinced to undergo HIV test | Low self-efficacy Absence of high-quality counselling sessions | Ensure that 65% of pregnant women attending the ANC are exposed to HIV peer education and high-quality individual counselling sessions | Establishment of pregnant women peer groups to do peer education sessions | Increase in percent of women who accept HIV test |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elsheikh, I.E.; Crutzen, R.; Adam, I.; Abdelraheem, S.I.; Van den Borne, H.W. Increasing Prevention of Mother to Child Transmission (PMTCT) Uptake through Facility-Based Health Promotion: Intervention Development. Behav. Sci. 2023, 13, 317. https://doi.org/10.3390/bs13040317
Elsheikh IE, Crutzen R, Adam I, Abdelraheem SI, Van den Borne HW. Increasing Prevention of Mother to Child Transmission (PMTCT) Uptake through Facility-Based Health Promotion: Intervention Development. Behavioral Sciences. 2023; 13(4):317. https://doi.org/10.3390/bs13040317
Chicago/Turabian StyleElsheikh, Ibrahim Elsiddig, Rik Crutzen, Ishag Adam, Salah Ibrahim Abdelraheem, and Hubertus W. Van den Borne. 2023. "Increasing Prevention of Mother to Child Transmission (PMTCT) Uptake through Facility-Based Health Promotion: Intervention Development" Behavioral Sciences 13, no. 4: 317. https://doi.org/10.3390/bs13040317
APA StyleElsheikh, I. E., Crutzen, R., Adam, I., Abdelraheem, S. I., & Van den Borne, H. W. (2023). Increasing Prevention of Mother to Child Transmission (PMTCT) Uptake through Facility-Based Health Promotion: Intervention Development. Behavioral Sciences, 13(4), 317. https://doi.org/10.3390/bs13040317