

Factors Affecting Physical Activity in People with Dementia: A Systematic Review and Narrative Synthesis

Abstract
:1. Introduction
2. Materials and Methods
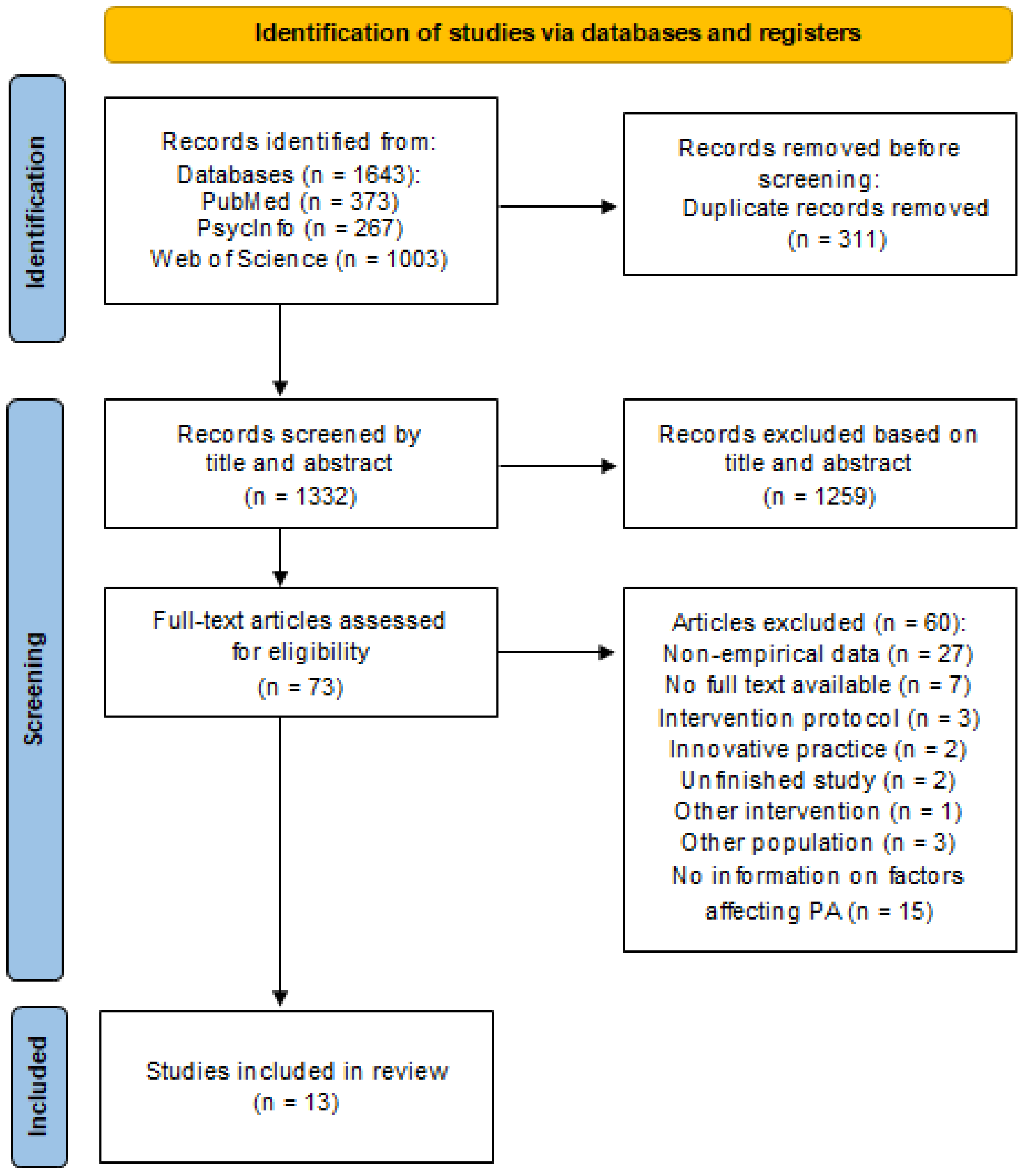
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Processing
2.4. Methodological Quality Assessment
3. Results
3.1. Methodological Quality of Studies

{kind=link}
| Reference | Study Design | Method | Results | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Barrado-Martín et al. [54] | + | + | − | + | + | ? | + | + | + | + |
| Barrado-Martín et al. [55] | + | + | + | + | + | ? | + | + | + | + |
| Donkers, van der Veen, Vernooij-Dassen, Nijhuis-van der Sanden and Graff [50] | + | + | + | − | + | ? | + | − | − | − |
| Hancox et al. [56] | + | + | + | − | + | ? | + | + | + | + |
| MacAndrew et al. [57] | + | + | + | + | + | ? | + | − | + | + |
| Reference | A | B | C | D | E | F |
|---|---|---|---|---|---|---|
| Dawson, Judge and Gerhart [53] | + | + | + | +/− | +/− | +/− |
| Henskens et al. [58] | + | +/− | + | − | + | + |
| Henwood et al. [59] | +/− | +/− | +/− | − | − | +/− |
| Kruse et al. [60] | +/− | − | − | − | +/− | +/− |
| Sondell, Rosendahl, Gustafson, Lindelöf and Littbrand [51] | + | + | − | − | − | + |
| Tak, van Uffelen, Paw, van Mechelen and Hopman-Rock [52] | + | + | − | − | − | + |
| Teri et al. [61] | + | + | + | − | − | + |
| Yu and Kolanowski [62] | +/− | − | − | − | +/− | − |
3.2. Study Characteristics
3.3. Participant Characteristics
3.4. Characteristics of PA Interventions
3.5. Success of Implementation of PA Interventions
3.6. Barriers, Facilitators and Motivators for Physical Activity
4. Discussion
4.1. Complementary Findings
4.2. New Findings on the Intrapersonal Level
4.2.1. Physical or Mental Health
4.2.2. Individual Preferences
4.3. New Findings on the Interpersonal Level
4.3.1. General Support from Informal Care, Family or Health Professional
4.3.2. Support for Staff in Nursing Homes
4.4. New Findings on the Community Level
4.4.1. Structural and Organizational (Intervention) Factors: Content of the Intervention
4.4.2. Structural and Organizational (Intervention) Factors: Organization of the Intervention
4.5. Success Rates of PA Implementations
4.6. Theoretical Framework Integration
4.7. Limitations of Underlying Studies and Limitations of This Review
4.8. Clinical and Practical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- WHO. Global Status Report on the Public Health Response to Dementia; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Breitner, J.C.S. Dementia—Epidemiological Considerations, Nomenclature, and a Tacit Consensus Definition. J. Geriatr. Psychiatry Neurol. 2006, 19, 129–136. [Google Scholar] [CrossRef]
- WHO. Global Action Plan on the Public Health Response to Dementia 2017–2025; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Sachdev, P.S.; Blacker, D.; Blazer, D.G.; Ganguli, M.; Jeste, D.V.; Paulsen, J.S.; Petersen, R.C. Classifying neurocognitive disorders: The DSM-5 approach. Nat. Rev. Neurol. 2014, 10, 634–642. [Google Scholar] [CrossRef]
- Sverdrup, K.; Selbæk, G.; Bergh, S.; Strand, B.H.; Thingstad, P.; Skjellegrind, H.K.; Skjerve, K.N.; Tangen, G.G. Physical performance across the cognitive spectrum and between dementia subtypes in a population-based sample of older adults: The HUNT study. Arch. Gerontol. Geriatr. 2021, 95, 104400. [Google Scholar] [CrossRef]
- Cipriani, G.; Danti, S.; Picchi, L.; Nuti, A.; Fiorino, M.D. Daily functioning and dementia. Dement. Neuropsychol. 2020, 14, 93–102. [Google Scholar] [CrossRef]
- Brodaty, H.; Breteler, M.M.B.; Dekosky, S.T.; Dorenlot, P.; Fratiglioni, L.; Hock, C.; Kenigsberg, P.-A.; Scheltens, P.; De Strooper, B. The World of Dementia Beyond 2020. J. Am. Geriatr. Soc. 2011, 59, 923–927. [Google Scholar] [CrossRef]
- George, E.K.; Reddy, P.H. Can Healthy Diets, Regular Exercise, and Better Lifestyle Delay the Progression of Dementia in Elderly Individuals? J. Alzheimer’s Dis. 2019, 72, S37–S58. [Google Scholar] [CrossRef]
- Scales, K.; Zimmerman, S.; Miller, S.J. Evidence-Based Nonpharmacological Practices to Address Behavioral and Psychological Symptoms of Dementia. Gerontologist 2018, 58, S88–S102. [Google Scholar] [CrossRef]
- Anand, A.; Khurana, P.; Chawla, J.; Sharma, N.; Khurana, N. Emerging treatments for the behavioral and psychological symptoms of dementia. CNS Spectr. 2018, 23, 361–369. [Google Scholar] [CrossRef]
- Ringman, J.M.; Cummings, J.L. Current and emerging pharmacological treatment options for dementia. Behav. Neurol. 2006, 17, 5–16. [Google Scholar] [CrossRef]
- Douglas, S.; James, I.; Ballard, C. Non-pharmacological interventions in dementia. Adv. Psychiatr. Treat. 2004, 10, 171–177. [Google Scholar] [CrossRef]
- Takeda, M.; Tanaka, T.; Okochi, M.; Kazui, H. Non-pharmacological intervention for dementia patients. Psychiatry Clin. Neurosci. 2012, 66, 1–7. [Google Scholar] [CrossRef]
- Shaji, K.; Sivakumar, P.; Rao, G.; Paul, N. Clinical practice guidelines for management of dementia. Indian J. Psychiatry 2018, 60, 312–328. [Google Scholar] [CrossRef]
- Marques-Aleixo, I.; Beleza, J.; Sampaio, A.; Stevanović, J.; Coxito, P.; Gonçalves, I.; Ascensão, A.; Magalhães, J. Preventive and Therapeutic Potential of Physical Exercise in Neurodegenerative Diseases. Antioxid. Redox Signal. 2021, 34, 674–693. [Google Scholar] [CrossRef]
- Pitkälä, K.; Savikko, N.; Poysti, M.; Strandberg, T.; Laakkonen, M.-L. Efficacy of physical exercise intervention on mobility and physical functioning in older people with dementia: A systematic review. Exp. Gerontol. 2013, 48, 85–93. [Google Scholar] [CrossRef]
- Sanders, L.M.J.; Hortobagyi, T.; Karssemeijer, E.G.A.; van der Zee, E.A.; Scherder, E.J.A.; van Heuvelen, M.J.G. Effects of low- and high-intensity physical exercise on physical and cognitive function in older persons with dementia: A randomized controlled trial. Alzheimer’s Res. Ther. 2020, 12, 28. [Google Scholar] [CrossRef]
- Lam, F.M.; Huang, M.Z.; Liao, L.R.; Chung, R.C.; Kwok, T.C.; Pang, M.Y. Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia: A systematic review. J. Physiother. 2018, 64, 4–15. [Google Scholar] [CrossRef]
- De Souto Barreto, P.; Maltais, M.; Rosendahl, E.; Vellas, B.; Bourdel-Marchasson, I.; Lamb, S.E.; Pitkala, K.; Rolland, Y. Exercise Effects on Falls, Fractures, Hospitalizations, and Mortality in Older Adults with Dementia: An Individual-Level Patient Data Meta-analysis. J. Gerontol. Ser. A 2021, 76, e203–e212. [Google Scholar] [CrossRef]
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst. Rev. 2015, 2015, CD006489. [Google Scholar] [CrossRef]
- Toots, A.; Littbrand, H.; Lindelöf, N.; Wiklund, R.; Holmberg, H.; Nordström, P.; Lundin-Olsson, L.; Gustafson, Y.; Rosendahl, E. Effects of a High-Intensity Functional Exercise Program on Dependence in Activities of Daily Living and Balance in Older Adults with Dementia. J. Am. Geriatr. Soc. 2016, 64, 55–64. [Google Scholar] [CrossRef]
- Blankevoort, C.G.; Van Heuvelen, M.J.G.; Boersma, F.; Luning, H.; De Jong, J.; Scherder, E.J.A. Review of Effects of Physical Activity on Strength, Balance, Mobility and ADL Performance in Elderly Subjects with Dementia. Dement. Geriatr. Cogn. Disord. 2010, 30, 392–402. [Google Scholar] [CrossRef]
- Nuzum, H.; Stickel, A.; Corona, M.; Zeller, M.; Melrose, R.J.; Wilkins, S.S. Potential Benefits of Physical Activity in MCI and Dementia. Behav. Neurol. 2020, 2020, 7807856. [Google Scholar] [CrossRef] [PubMed]
- Demurtas, J.; Schoene, D.; Torbahn, G.; Marengoni, A.; Grande, G.; Zou, L.; Petrovic, M.; Maggi, S.; Cesari, M.; Lamb, S.; et al. Physical Activity and Exercise in Mild Cognitive Impairment and Dementia: An Umbrella Review of Intervention and Observational Studies. J. Am. Med. Dir. Assoc. 2020, 21, 1415–1422.e1416. [Google Scholar] [CrossRef] [PubMed]
- Groot, C.; Hooghiemstra, A.M.; Raijmakers, P.G.; van Berckel, B.N.; Scheltens, P.; Scherder, E.J.; van der Flier, W.M.; Ossenkoppele, R. The effect of physical activity on cognitive function in patients with dementia: A meta-analysis of randomized control trials. Ageing Res. Rev. 2016, 25, 13–23. [Google Scholar] [CrossRef]
- Jia, R.-X.; Liang, J.-H.; Xu, Y.; Wang, Y.-Q. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: A meta-analysis. BMC Geriatr. 2019, 19, 181. [Google Scholar] [CrossRef] [PubMed]
- Law, C.-K.; Lam, F.M.; Chung, R.C.; Pang, M.Y. Physical exercise attenuates cognitive decline and reduces behavioural problems in people with mild cognitive impairment and dementia: A systematic review. J. Physiother. 2020, 66, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Guitar, N.A.; Connelly, D.M.; Nagamatsu, L.S.; Orange, J.B.; Muir-Hunter, S.W. The effects of physical exercise on executive function in community-dwelling older adults living with Alzheimer’s-type dementia: A systematic review. Ageing Res. Rev. 2018, 47, 159–167. [Google Scholar] [CrossRef]
- Venegas-Sanabria, L.C.; Martínez-Vizcaino, V.; Cavero-Redondo, I.; Chavarro-Carvajal, D.A.; Cano-Gutierrez, C.A.; Álvarez-Bueno, C. Effect of physical activity on cognitive domains in dementia and mild cognitive impairment: Overview of systematic reviews and meta-analyses. Aging Ment. Health 2021, 25, 1977–1985. [Google Scholar] [CrossRef]
- Zeng, Y.; Wang, J.; Cai, X.; Zhang, X.; Zhang, J.; Peng, M.; Xiao, D.; Ouyang, H.; Yan, F. Effects of physical activity interventions on executive function in older adults with dementia: A meta-analysis of randomized controlled trials. Geriatr. Nurs. 2023, 51, 369–377. [Google Scholar] [CrossRef]
- Van Alphen, H.J.M.; Volkers, K.M.; Blankevoort, C.G.; Scherder, E.J.A.; Hortobágyi, T.; Van Heuvelen, M.J.G. Older Adults with Dementia Are Sedentary for Most of the Day. PLoS ONE 2016, 11, e0152457. [Google Scholar] [CrossRef]
- Hartman, Y.A.W.; Karssemeijer, E.G.A.; Van Diepen, L.A.M.; Olde Rikkert, M.G.M.; Thijssen, D.H.J. Dementia Patients Are More Sedentary and Less Physically Active than Age- and Sex-Matched Cognitively Healthy Older Adults. Dement. Geriatr. Cogn. Disord. 2018, 46, 81–89. [Google Scholar] [CrossRef]
- Taylor, M.E.; Brodie, M.A.; van Schooten, K.S.; Delbaere, K.; Close, J.C.T.; Payne, N.; Webster, L.; Chow, J.; McInerney, G.; Kurrle, S.E.; et al. Older People with Dementia Have Reduced Daily-Life Activity and Impaired Daily-Life Gait When Compared to Age-Sex Matched Controls. J. Alzheimer’s Dis. 2019, 71, S125–S135. [Google Scholar] [CrossRef] [PubMed]
- Van der Wardt, V.; Hancox, J.; Pollock, K.; Logan, P.; Vedhara, K.; Harwood, R.H. Physical activity engagement strategies in people with mild cognitive impairment or dementia-a focus group study. Aging Ment. Health 2020, 24, 1326–1333. [Google Scholar] [CrossRef] [PubMed]
- Cedervall, Y.; Aberg, A.C. Physical activity and implications on well-being in mild Alzheimer’s disease: A qualitative case study on two men with dementia and their spouses. Physiother. Theory Pract. 2010, 26, 226–239. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Eggermont, L.; Soundy, A.; Probst, M.; Vandenbulcke, M.; Vancampfort, D. What are the factors associated with physical activity (PA) participation in community dwelling adults with dementia? A systematic review of PA correlates. Arch. Gerontol. Geriatr. 2014, 59, 195–203. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef]
- Telenius, E.W.; Tangen, G.G.; Eriksen, S.; Rokstad, A.M.M. Fun and a meaningful routine: The experience of physical activity in people with dementia. BMC Geriatr. 2022, 22, 500. [Google Scholar] [CrossRef]
- Gebhard, D.; Mess, F. Feasibility and Effectiveness of a Biography-Based Physical Activity Intervention in Institutionalized People with Dementia: Quantitative and Qualitative Results from a Randomized Controlled Trial. J. Aging Phys. Act. 2022, 30, 237–251. [Google Scholar] [CrossRef]
- Van Alphen, H.J.M.; Hortobágyi, T.; van Heuvelen, M.J.G. Barriers, motivators, and facilitators of physical activity in dementia patients: A systematic review. Arch. Gerontol. Geriatr. 2016, 66, 109–118. [Google Scholar] [CrossRef]
- Vseteckova, J.; Dadova, K.; Gracia, R.; Ryan, G.; Borgstrom, E.; Abington, J.; Gopinath, M.; Pappas, Y. Barriers and facilitators to adherence to walking group exercise in older people living with dementia in the community: A systematic review. Eur. Rev. Aging Phys. Act. 2020, 17, 15. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- CASP. CASP Qualitative Studies Checklist. Critical Appraisal Skills Programme; CASP: Sacramento, CA, USA, 2018. [Google Scholar]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Groot Kormelinck, C.M.; Janus, S.I.M.; Smalbrugge, M.; Gerritsen, D.L.; Zuidema, S.U. Systematic review on barriers and facilitators of complex interventions for residents with dementia in long-term care. Int. Psychogeriatr. 2021, 33, 873–889. [Google Scholar] [CrossRef] [PubMed]
- EPHPP. Quality Assessment Tool for Quantitative Studies. Effective Public Health Practice Project; EPHPP: Hamilton, ON, Canada, 2009. [Google Scholar]
- Gheysen, F.; Poppe, L.; Desmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Donkers, H.W.; van der Veen, D.J.; Vernooij-Dassen, M.J.; Nijhuis-van der Sanden, M.W.G.; Graff, M.J.L. Social participation of people with cognitive problems and their caregivers: A feasibility evaluation of the Social Fitness Programme. Int. J. Geriatr. Psychiatry 2017, 32, e50–e63. [Google Scholar] [CrossRef]
- Sondell, A.; Rosendahl, E.; Gustafson, Y.; Lindelöf, N.; Littbrand, H. The Applicability of a High-Intensity Functional Exercise Program Among Older People with Dementia Living in Nursing Homes. J. Geriatr. Phys. Ther. 2019, 42, E16–E24. [Google Scholar] [CrossRef]
- Tak, E.C.P.M.; van Uffelen, J.G.Z.; Paw, M.; van Mechelen, W.; Hopman-Rock, M. Adherence to Exercise Programs and Determinants of Maintenance in Older Adults with Mild Cognitive Impairment. J. Aging Phys. Act. 2012, 20, 32–46. [Google Scholar] [CrossRef]
- Dawson, N.; Judge, K.S.; Gerhart, H. Improved Functional Performance in Individuals with Dementia After a Moderate-Intensity Home-Based Exercise Program: A Randomized Controlled Trial. J. Geriatr. Phys. Ther. 2019, 42, 18–27. [Google Scholar] [CrossRef]
- Barrado-Martín, Y.; Heward, M.; Polman, R.; Nyman, S.R. People living with dementia and their family carers’ adherence to home-based Tai Chi practice. Dement.-Int. J. Soc. Res. Pract. 2020, 20, 1586–1603. [Google Scholar] [CrossRef]
- Barrado-Martín, Y.; Heward, M.; Polman, R.; Nyman, S.R. Acceptability of a dyadic Tai Chi intervention for older people living with dementia and their informal carers. J. Aging Phys. Act. 2019, 27, 166–183. [Google Scholar] [CrossRef] [PubMed]
- Hancox, J.E.; Van Der Wardt, V.; Pollock, K.; Booth, V.; Vedhara, K.; Harwood, R.H. Factors influencing adherence to home-based strength and balance exercises among older adults with mild cognitive impairment and early dementia: Promoting Activity, Independence and Stability in Early Dementia (PrAISED). PLoS ONE 2019, 14, e0217387. [Google Scholar] [CrossRef] [PubMed]
- MacAndrew, M.; Kolanowski, A.; Fielding, E.; Kerr, G.; McMaster, M.; Wyles, K.; Beattie, E. “Would you like to join me for a walk?” The feasibility of a supervised walking programme for people with dementia who wander. Int. J. Older People Nurs. 2019, 14, e12244. [Google Scholar] [CrossRef] [PubMed]
- Henskens, M.; Nauta, I.M.; Scherder, E.J.A.; Oosterveld, F.G.J.; Vrijkotte, S. Implementation and effects of Movement-oriented Restorative Care in a nursing home-a quasi-experimental study. BMC Geriatr. 2017, 17, 243. [Google Scholar] [CrossRef]
- Henwood, T.; Neville, C.; Baguley, C.; Beattie, E. Aquatic exercise for residential aged care adults with dementia: Benefits and barriers to participation. Int. Psychogeriatr. 2017, 29, 1439–1449. [Google Scholar] [CrossRef]
- Kruse, A.; Cordes, T.; Schulz, S.; Wollesen, B. Feasibility of Multicomponent Training for People with Moderate to Severe Dementia Living in a Long-Term Care Home: A Social Ethical Approach. Int. J. Environ. Res. Public Health 2021, 18, 7631. [Google Scholar] [CrossRef]
- Teri, L.; Logsdon, R.G.; McCurry, S.M.; Pike, K.C.; McGough, E.L. Translating an Evidence-based Multicomponent Intervention for Older Adults with Dementia and Caregivers. Gerontologist 2020, 60, 548–557. [Google Scholar] [CrossRef]
- Yu, F.; Kolanowski, A. Facilitating Aerobic Exercise Training in Older Adults with Alzheimer’s Disease. Geriatr. Nurs. 2009, 30, 250–259. [Google Scholar] [CrossRef]
- Cedervall, Y.; Torres, S.; Åberg, A.C. Maintaining well-being and selfhood through physical activity: Experiences of people with mild Alzheimer’s disease. Aging Ment. Health 2015, 19, 679–688. [Google Scholar] [CrossRef]
- Malthouse, R.; Fox, F. Exploring experiences of physical activity among people with Alzheimer’s disease and their spouse carers: A qualitative study. Physiotherapy 2014, 100, 169–175. [Google Scholar] [CrossRef]
- Suttanon, P.; Hill, K.D.; Said, C.M.; Byrne, K.N.; Dodd, K.J. Factors influencing commencement and adherence to a home-based balance exercise program for reducing risk of falls: Perceptions of people with Alzheimer’s disease and their caregivers. Int. Psychogeriatr. 2012, 24, 1172–1182. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Leon, A.S.; Bliss, D.; Dysken, M.; Savik, K.; Wyman, J.F. Aerobic training for older men with Alzheimer’s disease: Individual examples of progression. Res. Gerontol. Nurs. 2011, 4, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Dal Bello-Haas, V.P.; O’Connell, M.E.; Morgan, D.G.; Crossley, M. Lessons learned: Feasibility and acceptability of a telehealth-delivered exercise intervention for rural-dwelling individuals with dementia and their caregivers. Rural Remote Health 2014, 14, 2715. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.F.; Telenius, E.W.; Engedal, K.; Bergland, A. Increased self-efficacy: The experience of high-intensity exercise of nursing home residents with dementia—A qualitative study. BMC Health Serv. Res. 2015, 15, 379. [Google Scholar] [CrossRef] [PubMed]
- Sobol, N.A.; Hoffmann, K.; Frederiksen, K.S.; Vogel, A.; Vestergaard, K.; Brændgaard, H.; Gottrup, H.; Lolk, A.; Wermuth, L.; Jakobsen, S.; et al. Effect of aerobic exercise on physical performance in patients with Alzheimer’s disease. Alzheimer’s Dement. 2016, 12, 1207–1215. [Google Scholar] [CrossRef]
- Cox, K.L.; Flicker, L.; Almeida, O.P.; Xiao, J.; Greenop, K.R.; Hendriks, J.; Phillips, M.; Lautenschlager, N.T. The FABS trial: A randomised control trial of the effects of a 6-month physical activity intervention on adherence and long-term physical activity and self-efficacy in older adults with memory complaints. Prev. Med. 2013, 57, 824–830. [Google Scholar] [CrossRef]
- Teri, L.; Logsdon, R.G.; McCurry, S.M. Exercise interventions for dementia and cognitive impairment: The Seattle Protocols. J. Nutr. Health Aging 2008, 12, 391–394. [Google Scholar] [CrossRef]
- Yu, F.; Greimel, S.; Kelly, K.; Wyman, J.F. Strategies to engage older adults with behavioral and psychological symptoms of dementia in exercise: A multiple case study. Appl. Nurs. Res. 2017, 36, 77–80. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J. Nonpharmacologic Treatment of Behavioral Disorders in Dementia. Curr. Treat. Options Neurol. 2013, 15, 765–785. [Google Scholar] [CrossRef]
- Karssemeijer, E.G.A.; De Klijn, F.H.; Bossers, W.J.R.; Olde Rikkert, M.G.M.; Van Heuvelen, M.J.G. Ranking Barriers, Motivators, and Facilitators to Promote Physical Activity Participation of Persons with Dementia: An Explorative Study. J. Geriatr. Phys. Ther. 2020, 43, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Tierney, L.; Beattie, E. Enjoyable, engaging and individualised: A concept analysis of meaningful activity for older adults with dementia. Int. J. Older People Nurs. 2020, 15, e12306. [Google Scholar] [CrossRef] [PubMed]
- Long, A.; Di Lorito, C.; Logan, P.; Booth, V.; Howe, L.; Hood-Moore, V.; Van Der Wardt, V. The Impact of a Dementia-Friendly Exercise Class on People Living with Dementia: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2020, 17, 4562. [Google Scholar] [CrossRef]
- Portegijs, S.; Van Beek, A.P.A.; Van Tuyl, L.H.D.; Wagner, C. “We usually choose safety over freedom”: Results from focus groups with professional caregivers in long-term dementia care. BMC Health Serv. Res. 2022, 22, 677. [Google Scholar] [CrossRef]
- Brett, L.; Traynor, V.; Stapley, P.; Meedya, S. Exercise and Dementia in Nursing Homes: Views of Staff and Family Carers. J. Aging Phys. Act. 2018, 26, 89–96. [Google Scholar] [CrossRef]
- Karuncharernpanit, S.; Hendricks, J.; Toye, C. Perceptions of exercise for older people living with dementia in Bangkok, Thailand: An exploratory qualitative study. Int. J. Older People Nurs. 2016, 11, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Casas-Herrero, Á.; Sáez De Asteasu, M.L.; Antón-Rodrigo, I.; Sánchez-Sánchez, J.L.; Montero-Odasso, M.; Marín-Epelde, I.; Ramón-Espinoza, F.; Zambom-Ferraresi, F.; Petidier-Torregrosa, R.; Elexpuru-Estomba, J.; et al. Effects of Vivifrail multicomponent intervention on functional capacity: A multicentre, randomized controlled trial. J. Cachexia Sarcopenia Muscle 2022, 13, 884–893. [Google Scholar] [CrossRef]
- Bossers, W.J.R.; Scherder, E.J.A.; Boersma, F.; Hortobágyi, T.; Van Der Woude, L.H.V.; Van Heuvelen, M.J.G. Feasibility of a Combined Aerobic and Strength Training Program and Its Effects on Cognitive and Physical Function in Institutionalized Dementia Patients. A Pilot Study. PLoS ONE 2014, 9, e97577. [Google Scholar] [CrossRef]
- Di Lorito, C.; Bosco, A.; Booth, V.; Goldberg, S.; Harwood, R.H.; Van Der Wardt, V. Adherence to exercise interventions in older people with mild cognitive impairment and dementia: A systematic review and meta-analysis. Prev. Med. Rep. 2020, 19, 101139. [Google Scholar] [CrossRef]
- Di Lorito, C.; Pollock, K.; Harwood, R.; Das Nair, R.; Logan, P.; Goldberg, S.; Booth, V.; Vedhara, K.; Van Der Wardt, V. A scoping review of behaviour change theories in adults without dementia to adapt and develop the ‘PHYT in dementia’, a model promoting physical activity in people with dementia. Maturitas 2019, 121, 101–113. [Google Scholar] [CrossRef]
- Müllers, P.; Taubert, M.; Müller, N.G. Physical Exercise as Personalized Medicine for Dementia Prevention? Front. Physiol. 2019, 10, 672. [Google Scholar] [CrossRef] [PubMed]

| Reference | Study Design | Participants | Diagnosis of PwD | Age (Mean ± SD) of PwD | % Walking Aid | % Male PwD | Living Situation | Focus on | Type of PA | Duration of PA Intervention (Weeks) | Country |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Barrado-Martín, Heward, Polman and Nyman [54] | Qualitative semi-structured interviews; thematic approach | 22 PwD 24 caregivers | 15 AD 6 mixed 1 Frontal | 79.0 ± 6.5 | 27% WA | 55 | Community dwelling | Adherence | Tai Chi | 20 | UK |
| Barrado-Martín, Heward, Polman and Nyman [55] | Qualitative observations; thematic analyses | 10 PwD 10 caregivers | 9 AD 1 mixed | 78.2 ± 5.4 | 0% WA | 50 | Community dwelling | Acceptability | Tai Chi | 3–4 | UK |
| Dawson, Judge and Gerhart [53] | Randomized controlled intervention trial | 23 PwD | NA MMSE 20.8 ± 5.0 | 73.9 ± 9.1 | NA | 43.5 | Community dwelling | Facilitation | Functional exercise program (strength and balance) | 12 | USA |
| Donkers, van der Veen, Vernooij-Dassen, Nijhuis-van der Sanden and Graff [50] | Qualitative design; thematic analysis | 14 PwD 14 caregivers | 4 Memory problems 1 MCI 6 AD 3 VaD MMSE 10–24 | 80.0 ± 9.1 | 79% WA | 42.9 | Community dwelling | Delivery | Social Fitness Programme | 12 | The Netherlands |
| Hancox, Van Der Wardt, Pollock, Booth, Vedhara and Harwood [56] | Qualitative semi-structured interviews; thematic analysis | 20 PwD 19 caregivers | 1 MCI 9 AD 4 VaD 4 mixed 2 unknown MMSE 25.1 ± 3.0 | 76.6 ± 6.6 | NA | 80 | Community dwelling | Adherence | Strength and balance exercises | 12–16 | UK |
| Henskens, Nauta, Scherder, Oosterveld and Vrijkotte [58] | Quantitative NCT and qualitative process evaluation | 61 PwD | 34 AD 7 VaD 6 mixed 14 unknownMMSE 9.8 ± 5.1 (int) and 6.5 ± 5.2 (contr.) | 86.5 ± 7.1 84.2 ± 4.7 | NA | 18.9 29.9 | Nursing home | Delivery | Movement-oriented restorative care | 52 | The Netherlands |
| Henwood, Neville, Baguley and Beattie [59] | Quantitative NCT | 46 PwD | NA | 82.4 ± 6.6 | NA | 40 | Nursing home | Delivery | Aquatic exercise program | 12 | Australia |
| Kruse, Cordes, Schulz and Wollesen [60] | Quantitative uncontrolled study and qualitative interviews | 15 PwD | NA | 82 (range 75–90) | NA | 36 | Nursing home | Feasibility | Multicomponent intervention | 16 | Germany |
| MacAndrew, Kolanowski, Fielding, Kerr, McMaster, Wyles and Beattie [57] | Qualitative interviews; thematic analysis | 7 PwD | NA | 77.0 ± 10.2 | NA | 43 | Nursing home | Feasibility | Walking programme | 3 | Australia |
| Sondell, Rosendahl, Gustafson, Lindelöf and Littbrand [51] | Randomized controlled trial | 93 PwD | 34 AD 36 Vascular 8 Mixed 15 other MMSE 15.4 ± 3.4 | 84.4 ± 6.2 | 81% WA | 24.7 | Nursing home | Applicability | High-intensity functional exercise program | 16 | Sweden |
| Tak, van Uffelen, Paw, van Mechelen and Hopman-Rock [52] | Randomized controlled trial and qualitative interviews | 134 PwD | 134 MCI MMSE 28.4 ± 1.4 | 74.8 ± 2.9 | NA | 59 | Community dwelling | Adherence | Aerobic exercises | 52 | The Netherlands |
| Teri, Logsdon, McCurry, Pike and McGough [61] | Quantitative design and qualitative interviews | 255 PwD 20 case manager 10 AAAs | 255 AD MMSE 15.6 ± 7.1 | 81.3 ± 7.7 | NA | 51 | Community residing | Delivery | Multicomponent intervention | 6 | USA |
| Yu and Kolanowski [62] | Quantitative uncontrolled trial | 2 PwD | 2 AD MMSE 17 and 25 | 75 86 | NA | 50 | Community dwelling | Feasibility | Aerobic exercises | 8 | USA |
| Barriers | Motivators | Facilitators |
|---|---|---|
| Intrapersonal level | ||
| Physical or Mental Health | ||
| Physical health: |
| Physical health:
|
| Individual preferences | ||
| ||
| Interpersonal level | ||
| General support from informal caregiver, family or health professional | ||
| Support from staff in nursing homes | ||
| Social identification | ||
|
| |
| Community level | ||
| Structural and organizational factors | ||
| ||
| Physical environment | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feenstra, R.W.; de Bruin, L.J.E.; van Heuvelen, M.J.G. Factors Affecting Physical Activity in People with Dementia: A Systematic Review and Narrative Synthesis. Behav. Sci. 2023, 13, 913. https://doi.org/10.3390/bs13110913
Feenstra RW, de Bruin LJE, van Heuvelen MJG. Factors Affecting Physical Activity in People with Dementia: A Systematic Review and Narrative Synthesis. Behavioral Sciences. 2023; 13(11):913. https://doi.org/10.3390/bs13110913
Chicago/Turabian StyleFeenstra, Ruth W., Liese J. E. de Bruin, and Marieke J. G. van Heuvelen. 2023. "Factors Affecting Physical Activity in People with Dementia: A Systematic Review and Narrative Synthesis" Behavioral Sciences 13, no. 11: 913. https://doi.org/10.3390/bs13110913
APA StyleFeenstra, R. W., de Bruin, L. J. E., & van Heuvelen, M. J. G. (2023). Factors Affecting Physical Activity in People with Dementia: A Systematic Review and Narrative Synthesis. Behavioral Sciences, 13(11), 913. https://doi.org/10.3390/bs13110913