
Clinical Phenotypes and Mortality Biomarkers: A Study Focused on COVID-19 Patients with Neurological Diseases in Intensive Care Units


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Statistical Analysis
2.1.1. k-Means Algorithm
- Determining the number of clusters k;
- Setting centroids by first shuffling the dataset, and then randomly selecting data points to replace the centroids;
- Calculating the distance between data points and all centroids;
- Allocating each data point to the closest cluster (centroid);
- Updating the position of the centroid according to the assigned data;
- Retaining iteration until there is no change to the centroids.
2.1.2. Stable Sparse Biomarkers Detection: The Procedure to Select a Stable and Sparse Classifier
3. Results
3.1. Characteristics of k-Means Algorithm-Defined Phenotypes for COVID-19 Patients in ICUs Considering Fifteen Symptoms, Fourteen Comorbidities and Age
- ✓ Phenotype class 1: mean age 72.3 years—hypertension, coronary artery disease, cough and fever; n = 222 (17.74% of the sample);
- ✓ Phenotype class 2: mean age 63 years—asthma, cough and fever; n = 67 (5.3% of the sample);
- ✓ Phenotype class 3: mean age 74.5 years—hypertension, diabetes and cough; n = 255 (20.3% of the sample);
- ✓ Phenotype class 4: mean age 67.8 years—hypertension and no symptoms; n = 394 (31.4% of the sample);
- ✓ Phenotype class 5: mean age 53 years—cough and no comorbidities; n = 123 (9.8% of the sample);
- ✓ Phenotype class 6: mean age 60 years—without symptoms and comorbidities; n = 191 (15.2% of the sample);
3.2. Defined Phenotypes for COVID-19 Patients with Pre-Existing Neurological Diseases in ICUs
3.3. Defined Phenotypes and Mortality Rate in COVID-19 Patients with and without Neurological Diseases in ICUs
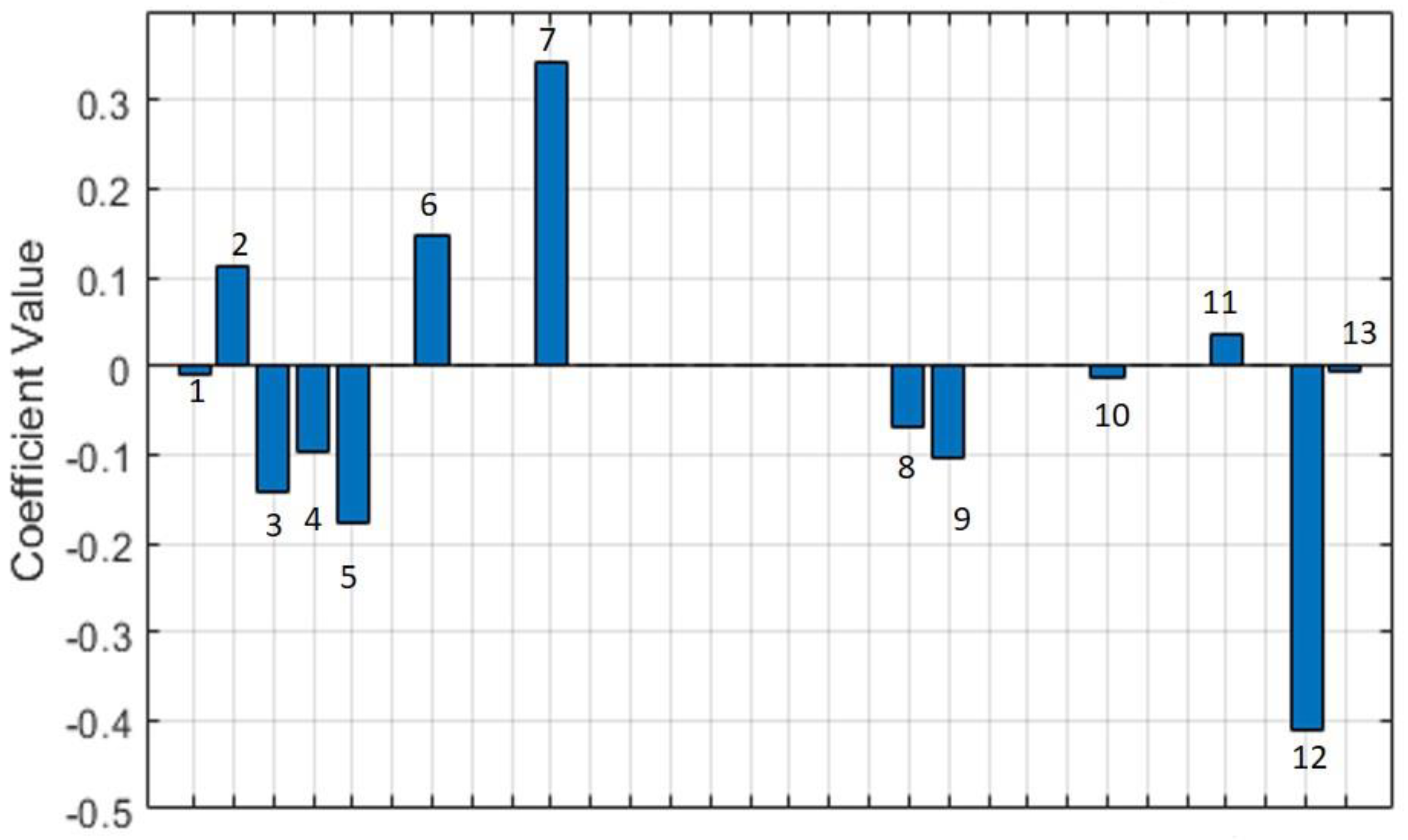
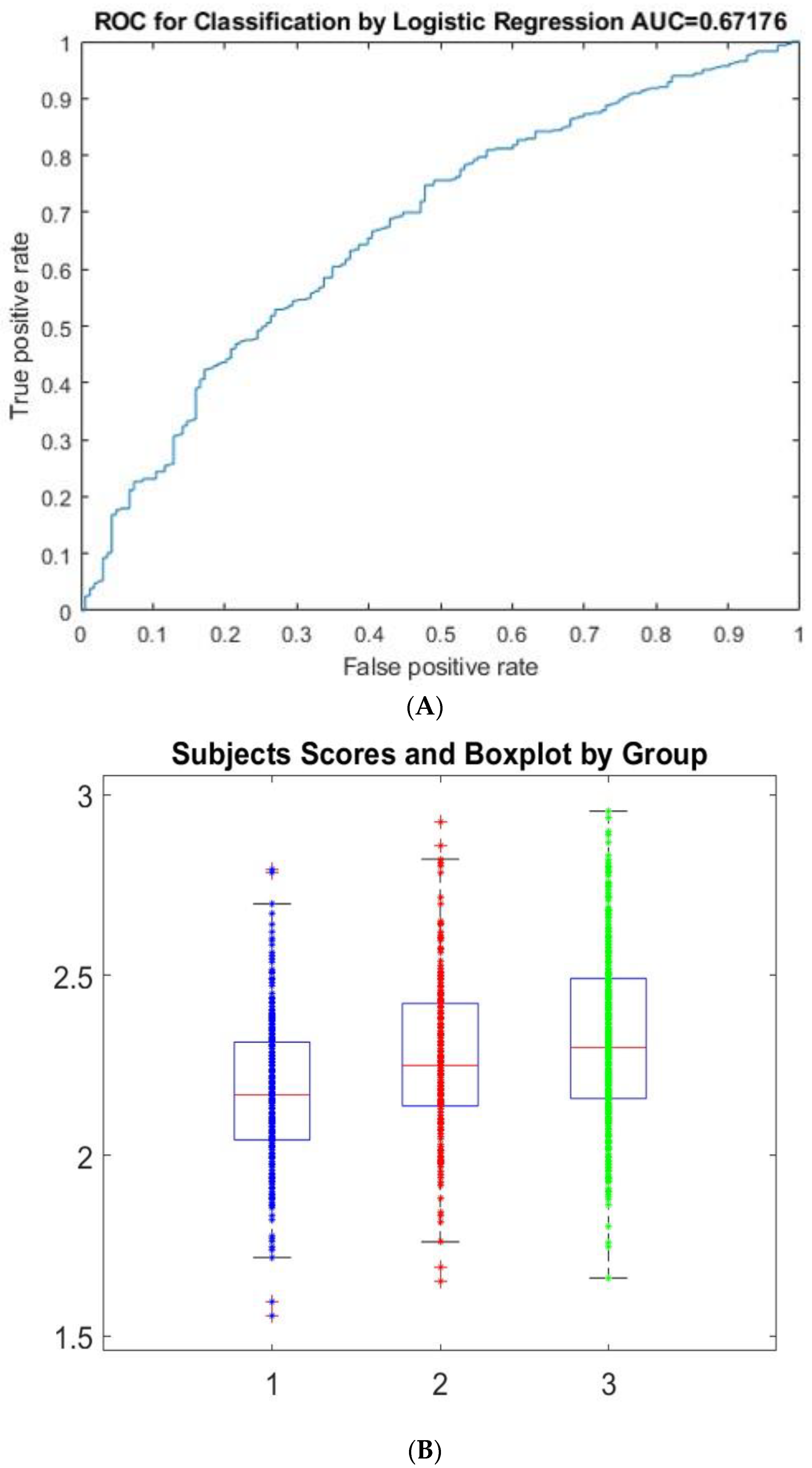
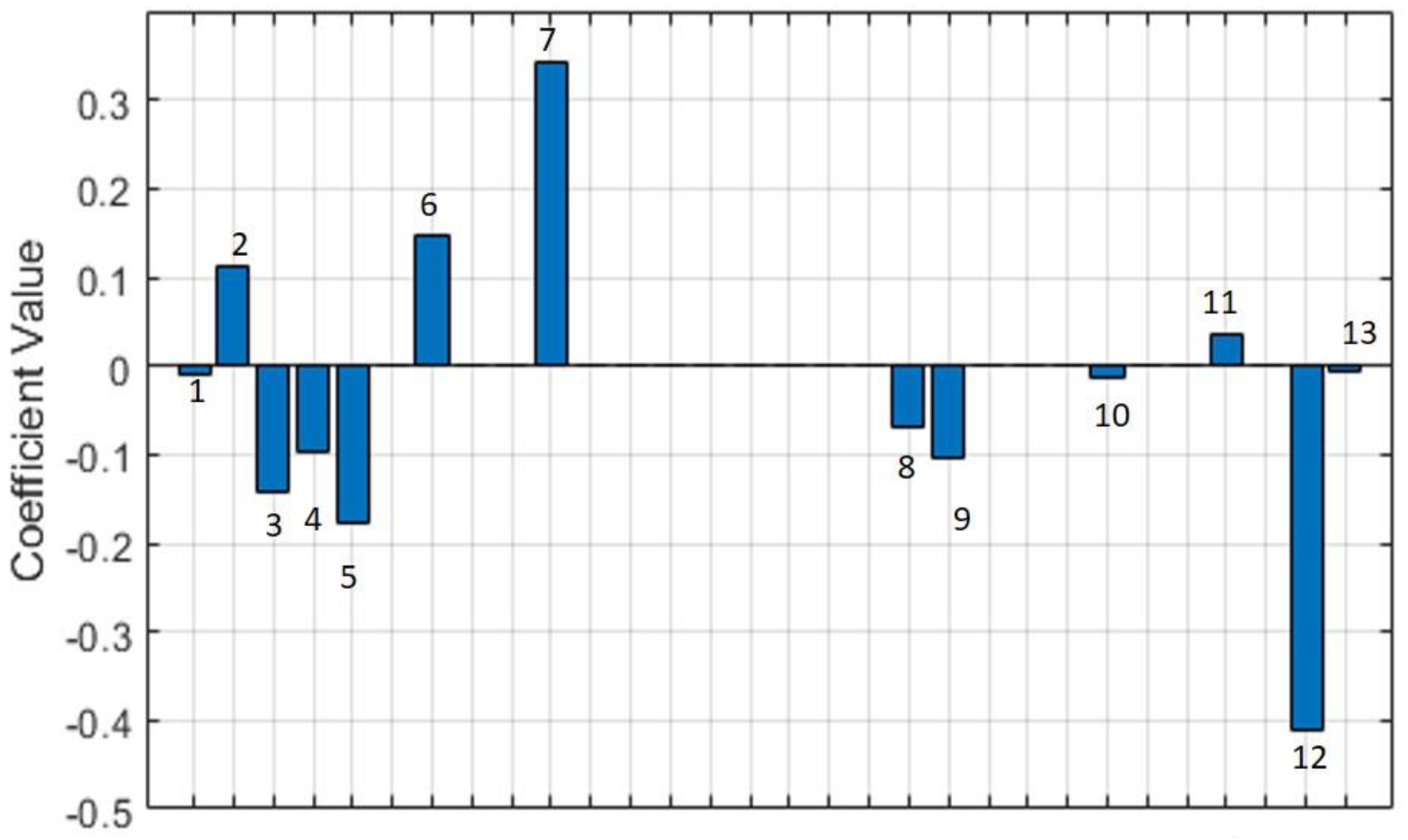
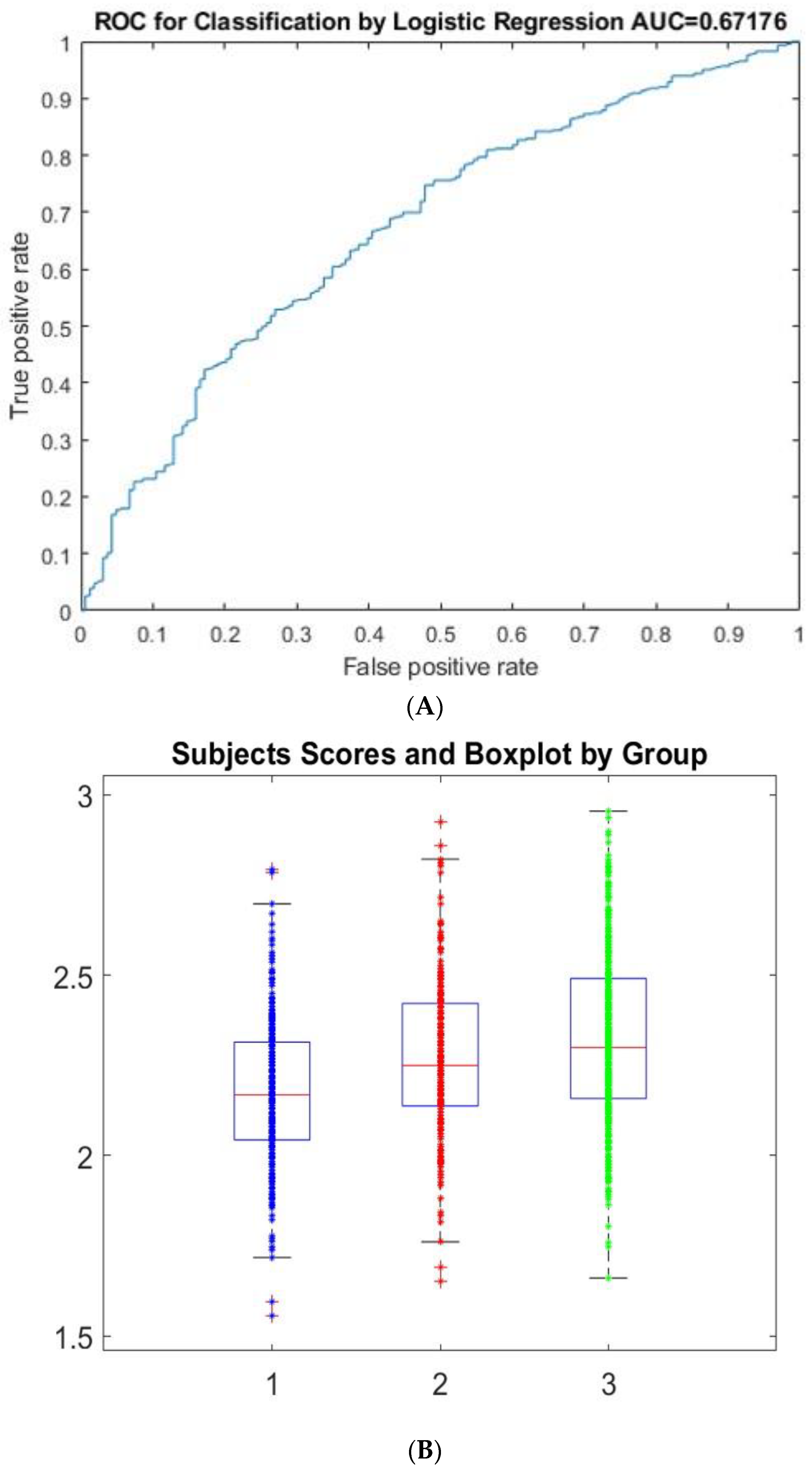
3.4. Stable Sparse Classifiers Procedure (SSC) Based on Mortality Prediction in COVID-19 Patients in ICUs
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, D.; Sharma, R.; Patwardhan, B.; Mathur, R.D. Clinical Spectrum of COVID-19 Cases and their Correlation with S.LDH Levels- An Observational Study from Southeast Rajasthan. J. Assoc. Physicians India 2021, 69, 11–12. [Google Scholar] [PubMed]
- Wu, X.; Liu, L.; Jiao, J.; Yang, L.; Zhu, B.; Li, X. Characterisation of clinical, laboratory and imaging factors related to mild vs. severe COVID-19 infection: A systematic review and meta-analysis. Ann. Med. 2020, 52, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Wang, Z.; Liao, H.; Marley, G.; Wu, D.; Tang, W. Epidemiologic, clinical, and laboratory findings of the COVID-19 in the current pandemic: Systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 640. [Google Scholar] [CrossRef]
- Armstrong, R.A.; Kane, A.D.; Cook, T.M. Decreasing mortality rates in ICU during the COVID-19 pandemic. Anaesthesia 2021, 76 (Suppl. 3). [Google Scholar] [CrossRef]
- Alban, A.; Chick, S.E.; Dongelmans, D.A.; Vlaar, A.P.J.; Sent, D. ICU capacity management during the COVID-19 pandemic using a process simulation. Intensive Care Med. 2020, 46, 1624–1626. [Google Scholar] [CrossRef]
- Armstrong, R.A.; Kane, A.D.; Cook, T.M. Outcomes from intensive care in patients with COVID-19: A systematic review and meta-analysis of observational studies. Anaesthesia 2020, 75, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Aboueshia, M.; Hussein, M.H.; Attia, A.S.; Swinford, A.; Miller, P.; Omar, M.; Toraih, E.A.; Saba, N.; Safah, H.; Duchesne, J.; et al. Cancer and COVID-19: Analysis of patient outcomes. Future Oncol. 2021, 17, 3499–3510. [Google Scholar] [CrossRef]
- Drake, T.M.; Riad, A.M.; Fairfield, C.J.; Egan, C.; Knight, S.R.; Pius, R.; Hardwick, H.E.; Norman, L.; Shaw, C.A.; McLean, K.A.; et al. COVID19-related and all-cause mortality risk among middle-aged and older adults across the first epidemic wave of SARS-CoV-2 infection: A population-based cohort stuJune 2020.dy in Southern Catalonia, Spain, March. Lancet 2021, 398, 223–237. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Imam, Z.; Odish, F.; Gill, I.; O’Connor, D.; Armstrong, J.; Vanood, A.; Ibironke, O.; Hanna, A.; Ranski, A.; Halalau, A. Older age and comorbidity are independent mortality predictors in a large cohort of 1305 COVID-19 patients in Michigan, United States. J. Intern. Med. 2020, 288, 469–476. [Google Scholar] [CrossRef]
- Baig, A.M.; Sanders, E.C. Potential neuroinvasive pathways of SARS-CoV-2: Deciphering the spectrum of neurological deficit seen in coronavirus disease-2019 (COVID-19). J. Med. Virol. 2020, 92, 1845–1857. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.; Ghosh, R.; Dubey, S.; Dubey, M.J.; Benito-León, J.; Kanti Ray, B. Neurological and Neuropsychiatric Impacts of COVID-19 Pandemic. Can. J. Neurol. Sci. 2021, 48, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Depner, M.; Fuchs, O.; Genuneit, J.; Karvonen, A.M.; Hyvärinen, A.; Kaulek, V.; Roduit, C.; Weber, J.; Schaub, B.; Lauener, R.; et al. Clinical and epidemiologic phenotypes of childhood asthma. Am. J. Respir. Crit. Care Med. 2014, 189, 129–138. [Google Scholar] [CrossRef]
- Reddy, K.; Sinha, P.; O’Kane, C.M.; Gordon, A.C.; Calfee, C.S.; McAuley, D.F. Subphenotypes in critical care: Translation into clinical practice. Lancet Respir. Med. 2020, 8, 631–643. [Google Scholar] [CrossRef]
- Sinha, P.; Calfee, C.S. Phenotypes in acute respiratory distress syndrome: Moving towards precision medicine. Curr. Opin. Crit. Care 2019, 25, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Bosch-Bayard, J.; Galán-García, L.; Fernandez, T.; Lirio, R.B.; Bringas-Vega, M.L.; Roca-Stappung, M.; Ricardo-Garcell, J.; Harmony, T.; Valdes-Sosa, P.A. Stable Sparse Classifiers Identify qEEG Signatures that Predict Learning Disabilities (NOS) Severity. Front. Neurosci. 2017, 11, 749. [Google Scholar] [CrossRef] [PubMed]
- DLaDC, W. Clustering Academic Press Library in Signal Processing. Signal. Processing Theory Mach. Learn. 2004, 1, 1115–1149. [Google Scholar]
- Wang, X.; Jehi, L.; Ji, X.; Mazzone, P.J. Phenotypes and Subphenotypes of Patients With COVID-19: A Latent Class Modeling Analysis. Chest 2021, 159, 2191–2204. [Google Scholar] [CrossRef]
- Rubio-Rivas, M.; Corbella, X.; Mora-Luján, J.M.; Loureiro-Amigo, J.; López Sampalo, A.; Yera Bergua, C.; Esteve Atiénzar, P.J.; Díez García, L.F.; Gonzalez Ferrer, R.; Plaza Canteli, S.; et al. Predicting Clinical Outcome with Phenotypic Clusters in COVID-19 Pneumonia: An Analysis of 12, 066 Hospitalized Patients from the Spanish Registry SEMI-COVID-19. J. Clin. Med. 2020, 9, 3488. [Google Scholar] [CrossRef]
- Ryan, C.; Minc, A.; Caceres, J.; Balsalobre, A.; Dixit, A.; Ng, B.K.; Schmitzberger, F.; Syed-Abdul, S.; Fung, C. Predicting severe outcomes in COVID-19 related illness using only patient demographics, comorbidities and symptoms. Am. J. Emerg. Med. 2021, 45, 378–384. [Google Scholar] [CrossRef]
- Jakhmola, S.; Indari, O.; Baral, B.; Kashyap, D.; Varshney, N.; Das, A.; Chatterjee, S.; Jha, H.C. Comorbidity Assessment Is Essential During COVID-19 Treatment. Front. Physiol. 2020, 11, 984. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhang, J.; Zhou, J.; Yi, H.; Lin, Z.; Liu, Y.; Zhu, M.; Wang, H.; Zhang, W.; Xu, H.; et al. Clinical characteristics of re-positive COVID-19 patients in Huangshi, China: A retrospective cohort study. PLoS ONE 2020, 15, e0241896. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Wang, Q.; Zhao, J.; Yang, P.; McGoogan, J.M.; Feng, Z.; Huang, C. Time Course of a Second Outbreak of COVID-19 in Beijing, China, June–July 2020. JAMA 2020, 324, 1458–1459. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Guan, Q.; Liu, M.; Zhuang, Y.J.; Yuan, Y.; Wang, S.S.; Li, J.; Chen, Z.; Yang, X.L.; Tang, Z.R.; Jia, H.J.; et al. Epidemiological investigation of a family clustering of COVID-19. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 629–633. [Google Scholar] [CrossRef]
- Chen, G.; Wu, M.Z.; Qin, C.J.; Wu, B.B.; Luo, W.R.; Liu, L.; Liu, J.Y. Epidemiological analysis of 18 patients with COVID-19. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 12522–12526. [Google Scholar]
- Jakhmola, S.; Baral, B.; Muduli, K.; Suar, M.; Das, P.; Patnaik, P.K.; Mohakud, N.K.; Jha, H.C. The interrelation of COVID-19 and neurological modalities. Neurol. Sci. 2021, 42, 2157–2160. [Google Scholar] [CrossRef]
- Sardu, C.; Maggi, P.; Messina, V.; Iuliano, P.; Sardu, A.; Iovinella, V.; Paolisso, G.; Marfella, R. Could Anti-Hypertensive Drug Therapy Affect the Clinical Prognosis of Hypertensive Patients With COVID-19 Infection? Data from Centers of Southern Italy. J. Am. Heart Assoc. 2020, 9, e016948. [Google Scholar] [CrossRef]
- Mizumoto, K.; Kagaya, K.; Chowell, G. Early epidemiological assessment of the transmission potential and virulence of coronavirus disease 2019 (COVID-19) in Wuhan City, China, January–February, 2020. BMC Med. 2020, 18, 217. [Google Scholar] [CrossRef]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [Green Version]
- Cillóniz, C.; Rodríguez-Hurtado, D.; Torres, A. Characteristics and Management of Community-Acquired Pneumonia in the Era of Global Aging. Med. Sci. 2018, 6, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.; Zeng, N.; Chen, Q.; Wu, Y.; Cai, S.; Li, G.; Li, F.; Kong, J. Clinical prognostic significance of serum high mobility group box-1 protein in patients with community-acquired pneumonia. J. Int. Med. Res. 2019, 47, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Mas Bermejo, P.; Sánchez Valdés, L.; Somarriba López, L.; Valdivia Onega, N.C.; Vidal Ledo, M.J.; Alfonso Sánchez, I.; Seuc Jo, A.; Almeida Cruz, Y.; Morales Ojeda, R. Equity and the Cuban National Health System’s response to COVID-19. Rev. Panam. Salud Publica 2021, 45, e80. [Google Scholar] [CrossRef] [PubMed]
- García-Azorín, D.; Abildúa, M.J.A.; Aguirre, M.E.E.; Fernández, S.F.; Moncó, J.C.G.; Guijarro-Castro, C.; Platas, M.G.; Delgado, F.R.; Andrés, J.M.L.; Ezpeleta, D. Neurological presentations of COVID-19: Findings from the Spanish Society of Neurology neuroCOVID-19 registry. J. Neurol. Sci. 2021, 423, 117283. [Google Scholar] [CrossRef]
- Cagnazzo, F.; Arquizan, C.; Derraz, I.; Dargazanli, C.; Lefevre, P.H.; Riquelme, C.; Gaillard, N.; Mourand, I.; Gascou, G.; Bonafe, A.; et al. Neurological manifestations of patients infected with the SARS-CoV-2: A systematic review of the literature. J. Neurol. 2021, 268, 2656–2665. [Google Scholar] [CrossRef]
- Romagnolo, A.; Balestrino, R.; Imbalzano, G.; Ciccone, G.; Riccardini, F.; Artusi, C.A.; Bozzali, M.; Ferrero, B.; Montalenti, E.; Montanaro, E.; et al. Neurological comorbidity and severity of COVID-19. J. Neurol. 2021, 268, 762–769. [Google Scholar] [CrossRef]
- Baig, A.M. Updates on What ACS Reported: Emerging Evidences of COVID-19 with Nervous System Involvement. ACS Chem. Neurosci. 2020, 11, 1204–1205. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Dahly, D.L.; Damen, J.A.A.; Debray, T.P.A.; et al. Prediction models for diagnosis and prognosis of COVID-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [Green Version]
- Aghagoli, G.; Gallo Marin, B.; Soliman, L.B.; Sellke, F.W. Cardiac involvement in COVID-19 patients: Risk factors, predictors, and complications: A review. J. Card. Surg. 2020, 35, 1302–1305. [Google Scholar] [CrossRef]
- Du, R.H.; Liang, L.R.; Yang, C.Q.; Wang, W.; Cao, T.Z.; Li, M.; Guo, G.Y.; Du, J.; Zheng, C.L.; Zhu, Q.; et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: A prospective cohort study. Eur. Respir. J. 2020, 55, 2000524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Hwang, H.; Hong, H.; Yim, J.J.; Lee, J. A systematic review and meta-analysis of regional risk factors for critical outcomes of COVID-19 during early phase of the pandemic. Sci. Rep. 2021, 11, 9784. [Google Scholar] [CrossRef] [PubMed]
- Baradaran, A.; Ebrahimzadeh, M.H.; Baradaran, A.; Kachooei, A.R. Prevalence of Comorbidities in COVID-19 Patients: A Systematic Review and Meta-Analysis. Otolaryngol. Head Neck Surg. 2021, 164, 244–254. [Google Scholar] [CrossRef]
- Guo, T.; Shen, Q.; Ouyang, X.; Guo, W.; Li, J.; He, W.; Yu, B.; Wu, C.; Zhou, Z.; Luo, H.; et al. Clinical Findings in Diabetes Mellitus Patients with COVID-19. J. Diabetes Res. 2021, 2021, 7830136. [Google Scholar] [CrossRef]
- Hussain, A.; Bhowmik, B.; do Vale Moreira, N.C. COVID-19 and diabetes: Knowledge in progress. Diabetes Res. Clin. Pract. 2020, 162, 108142. [Google Scholar] [CrossRef]
- Singhania, N.; Bansal, S.; Nimmatoori, D.P.; Ejaz, A.A.; McCullough, P.A.; Singhania, G. Current Overview on Hypercoagulability in COVID-19. Am. J. Cardiovasc. Drugs 2020, 20, 393–403. [Google Scholar] [CrossRef]
- Taylor, E.H.; Marson, E.J.; Elhadi, M.; Macleod, K.D.M.; Yu, Y.C.; Davids, R.; Boden, R.; Overmeyer, R.C.; Ramakrishnan, R.; Thomson, D.A.; et al. Factors associated with mortality in patients with COVID-19 admitted to intensive care: A systematic review and meta-analysis. Anaesthesia 2021, 76, 1224–1232. [Google Scholar] [CrossRef]
- García-Azorín, D.; Martínez-Pías, E.; Trigo, J.; Hernández-Pérez, I.; Valle-Peñacoba, G.; Talavera, B.; Simón-Campo, P.; de Lera, M.; Chavarría-Miranda, A.; López-Sanz, C.; et al. Neurological Comorbidity Is a Predictor of Death in COVID-19 Disease: A Cohort Study on 576 Patients. Front. Neurol. 2020, 11, 781. [Google Scholar] [CrossRef]
- Elrashdy, F.; Redwan, E.M.; Uversky, V.N. Why COVID-19 Transmission Is More Efficient and Aggressive Than Viral Transmission in Previous Coronavirus Epidemics? Biomolecules 2020, 10, 1312. [Google Scholar] [CrossRef]
- Sahai, A.; Bhandari, R.; Koupenova, M.; Freedman, J.; Godwin, M.; McIntyre, T.; Chung, M.; Iskandar, J.P.; Kamran, H.; Aggarwal, A.; et al. SARS-CoV-2 Receptors are Expressed on Human Platelets and the Effect of Aspirin on Clinical Outcomes in COVID-19 Patients. Res. Sq. 2020, 1. [Google Scholar] [CrossRef]
- Messina, F.; Giombini, E.; Agrati, C.; Vairo, F.; Ascoli Bartoli, T.; Al Moghazi, S.; Piacentini, M.; Locatelli, F.; Kobinger, G.; Maeurer, M.; et al. COVID-19: Viral-host interactome analyzed by network based-approach model to study pathogenesis of SARS-CoV-2 infection. J. Transl. Med. 2020, 18, 233. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Tang, X.; Fan, H.; Luo, Y.; Song, Y.; Xu, Y.; Chen, Y. Potential mechanisms of hemorrhagic stroke in elderly COVID-19 patients. Aging 2020, 12, 10022–10034. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, G.; Lippi, G.; Michael Henry, B. Cerebrovascular disease is associated with an increased disease severity in patients with Coronavirus Disease 2019 (COVID-19): A pooled analysis of published literature. Int. J. Stroke 2020, 15, 385–389. [Google Scholar] [CrossRef]
- Romagnolo, A.; Imbalzano, G.; Artusi, C.A.; Balestrino, R.; Ledda, C.; De Rosa, F.G.; Riccardini, F.; Montanaro, E.; Bozzali, M.; Rizzone, M.G.; et al. Neurological comorbidities and COVID-19-related case fatality: A cohort study. J. Neurol. Sci. 2021, 428, 117610. [Google Scholar] [CrossRef]
- Liu, N.; Sun, J.; Wang, X.; Zhao, M.; Huang, Q.; Li, H. The Impact of Dementia on the Clinical Outcome of COVID-19: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2020, 78, 1775–1782. [Google Scholar] [CrossRef]
- July, J.; Pranata, R. Prevalence of dementia and its impact on mortality in patients with coronavirus disease 2019: A systematic review and meta-analysis. Geriatr. Gerontol. Int. 2021, 21, 172–177. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Nemati, H.; Shahisavandi, M.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; et al. Nervous system diseases are associated with the severity and mortality of patients with COVID-19: A systematic review and meta-analysis. World J. Pediatr. 2021, 17, 495–499. [Google Scholar] [CrossRef]
- El-Qushayri, A.E.; Ghozy, S.; Reda, A.; Kamel, A.M.A.; Abbas, A.S.; Dmytriw, A.A. The impact of Parkinson’s disease on manifestations and outcomes of COVID-19 patients: A systematic review and meta-analysis. Rev. Med. Virol. 2021, 14, e2278. [Google Scholar] [CrossRef]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef]
- Núñez, I.; Priego-Ranero, A.; García-González, H.B.; Jiménez-Franco, B.; Bonilla-Hernández, R.; Domínguez-Cherit, G.; Merayo-Chalico, J.; Crispín, J.C.; Barrera-Vargas, A.; Valdés-Ferrer, S.I. Common hematological values predict unfavorable outcomes in hospitalized COVID-19 patients. Clin. Immunol. 2021, 225, 108682. [Google Scholar] [CrossRef] [PubMed]
- Hanff, T.C.; Harhay, M.O.; Brown, T.S.; Cohen, J.; Mohareb, A.M. Is there an association between COVID-19 mortality and the renin–angiotensin system—a call for epidemiologic investigations. Clin. Infect. Dis. 2020, 71, 870–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yang, Y.; Zhang, C.; Huang, F.; Wang, F.; Yuan, J.; Liu, L.; Jiang, C.; Zhou, C.; Xu, J.; et al. Clinical and biochemical indexes from 2019-nCoV infected patients linked to viral loads and lung injury. Sci. China Life Sci. 2020, 63, 364–374. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.H.; Minn, D.; Kim, Y.K. Autoantibodies in moderate and critical cases of COVID-19. Clin. Transl. Sci, 2021; published online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Pascolini, S.; Vannini, A.; Deleonardi, G.; Ciordinik, M.; Sensoli, A.; Carletti, I.; Muratori, P.; Lenzi, M.; Muratori, L.; Giostra, F.; et al. COVID-19 and immunological dysregulation: Can autoantibodies be useful? Clin. Transl. Sci. 2021, 14, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.-W.; Zhang, H.-Z.; Liu, C.; Dong, K.E. Autoantibodiesin COVID-19: Frequency and function. Autoimmun. Rev. 2021, 20, 102754. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales Chacón, L.M.; Galán García, L.; Cruz Hernández, T.M.; Pavón Fuentes, N.; Maragoto Rizo, C.; Morales Suarez, I.; Morales Chacón, O.; Abad Molina, E.; Rocha Arrieta, L. Clinical Phenotypes and Mortality Biomarkers: A Study Focused on COVID-19 Patients with Neurological Diseases in Intensive Care Units. Behav. Sci. 2022, 12, 234. https://doi.org/10.3390/bs12070234
Morales Chacón LM, Galán García L, Cruz Hernández TM, Pavón Fuentes N, Maragoto Rizo C, Morales Suarez I, Morales Chacón O, Abad Molina E, Rocha Arrieta L. Clinical Phenotypes and Mortality Biomarkers: A Study Focused on COVID-19 Patients with Neurological Diseases in Intensive Care Units. Behavioral Sciences. 2022; 12(7):234. https://doi.org/10.3390/bs12070234
Chicago/Turabian StyleMorales Chacón, Lilia María, Lídice Galán García, Tania Margarita Cruz Hernández, Nancy Pavón Fuentes, Carlos Maragoto Rizo, Ileana Morales Suarez, Odalys Morales Chacón, Elianne Abad Molina, and Luisa Rocha Arrieta. 2022. "Clinical Phenotypes and Mortality Biomarkers: A Study Focused on COVID-19 Patients with Neurological Diseases in Intensive Care Units" Behavioral Sciences 12, no. 7: 234. https://doi.org/10.3390/bs12070234
APA StyleMorales Chacón, L. M., Galán García, L., Cruz Hernández, T. M., Pavón Fuentes, N., Maragoto Rizo, C., Morales Suarez, I., Morales Chacón, O., Abad Molina, E., & Rocha Arrieta, L. (2022). Clinical Phenotypes and Mortality Biomarkers: A Study Focused on COVID-19 Patients with Neurological Diseases in Intensive Care Units. Behavioral Sciences, 12(7), 234. https://doi.org/10.3390/bs12070234