
A Scoping Review of Interventions for Family Bereavement Care during the COVID-19 Pandemic

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Research Questions
- -
- What types of interventions to reduce grief and complicated grief during the COVID-19 pandemic were addressed in the existing literature?
- -
- In what settings were these interventions provided?
- -
- What were the assessment tools used to assess grief/family grief?
- -
- Were there specific components of intervention design (frequency, single or grouped interventions, individual or interdisciplinary application, dose, duration, who delivered intervention, and the application of the intervention) that subsequently influenced outcomes during bereavement?
- -
- Were these interventions effective?
2.2. Eligibility Criteria
2.3. Literature Search Strategies
2.4. Data Charting and Summarizing Data
2.5. Ethical Considerations
3. Results
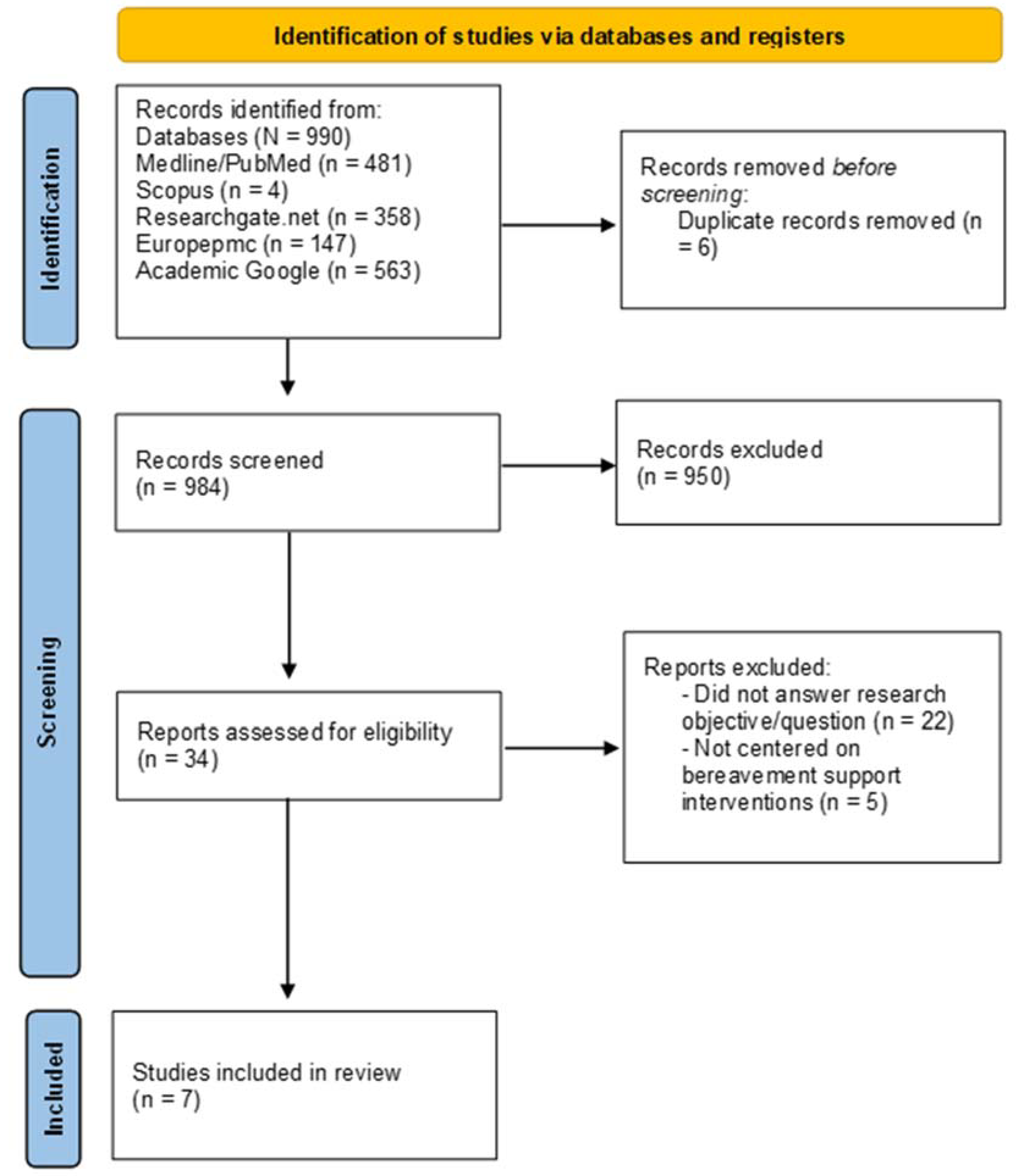
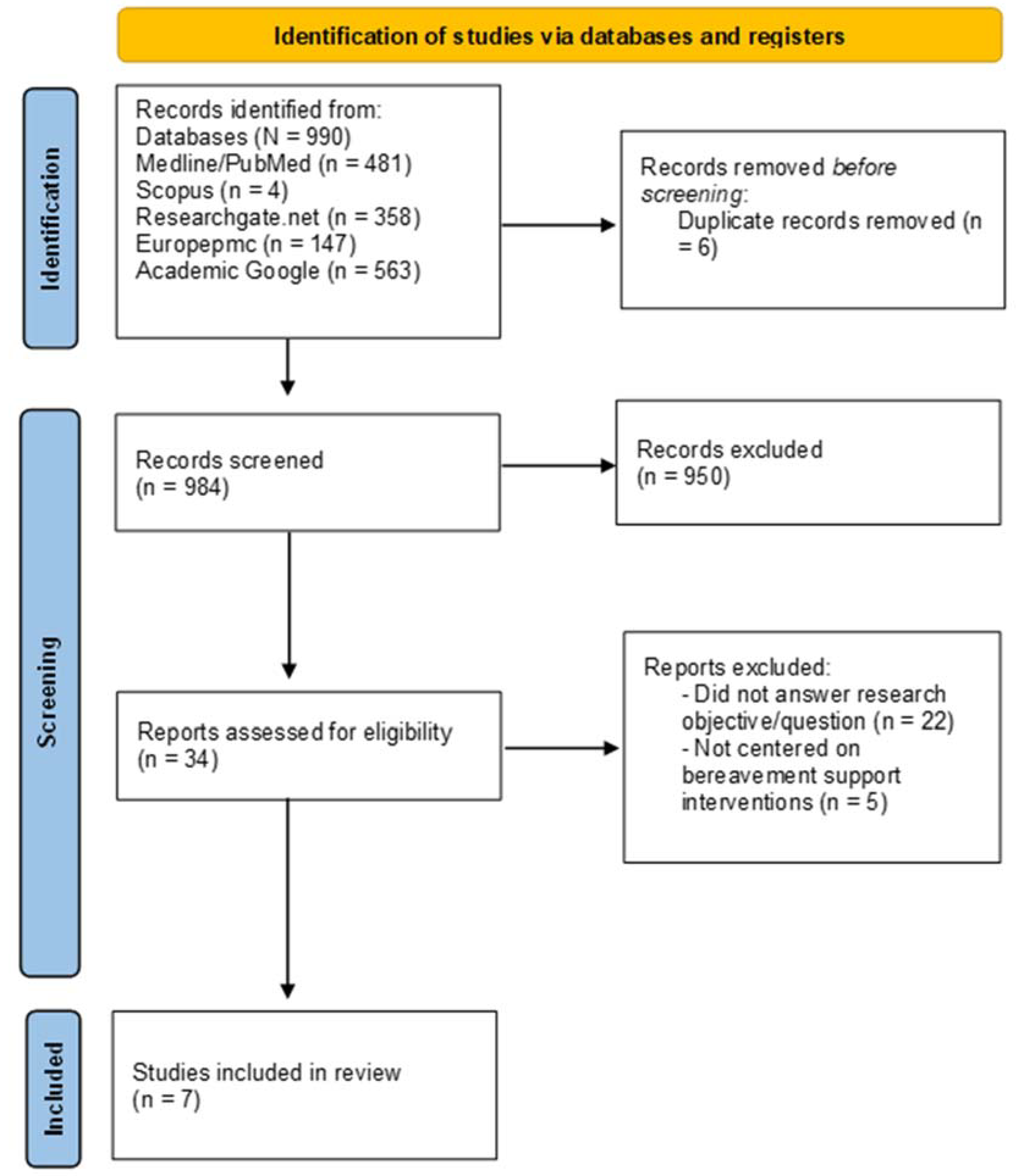
3.1. Study Selection and Characteristics
3.2. Research Key Topics
3.2.1. Types of Support Programs and Bereavement Interventions
3.2.2. Outcome Measurement Tools
- (a)
- Bereavement risk assessment following a patient’s death—Inventory of Traumatic Grief (ITG) and the Grief-related Avoidance Questionnaire (GRAQ) to evaluate grief symptoms and avoidance behaviours in the bereaved [31];
- (b)
- Complicated or prolonged bereavement assessment following a patient’s death—Prolonged Grief Questionnaire (PG-13) [31], an algorithm for diagnostic criteria for PGD; Traumatic Grief Inventory—Clinician Administered (TGI-CA) to assess Persistent Complex Bereavement Disorder (PCBD) symptoms [29,30]; PTSD Checklist for DSM-5 (PCL-5) and Post-Traumatic Stress Disorder Symptom Scale to evaluate PTSD symptoms [28,29,30,31]; and the Inventory of Complicated Grief [27] to assess indicators of pathological grief, such as anger, disbelief, and hallucinations;
- (c)
- Psychiatric symptoms assessment in bereaved families (e.g., anxiety, stress, and depression)—Patient Health Questionnaire (PHQ-9) [29]; Center for Epidemiologic Studies Depression Scale (CES-D) [28]; Depression Anxiety and Stress Scale (DASS-21) [28,31]; the Generalized Anxiety Disorder 7-Item (GAD-7) scale [28]; Typical Beliefs Questionnaire (TBQ) [31] to measure maladaptive cognitions common in the bereaved; and the Plutchik Suicide Risk Scale and the Scale for Suicidal Intention (SSI) to measure the severity of suicidal intentions [28,31].
3.2.3. Evidence on the Impacts of Interventions
4. Discussion
4.1. Implications and Suggestions for Research and Practice
- Comparing internet-based versus in-person support for the bereaved aimed at different stages of the grieving trajectory (e.g., immediate or long-term adjustment);
- Comparing interventions with high- vs. low-risk people, including the risk management process;
- Assessing the effectiveness of various psychosocial and psychotherapy interventions in reducing psychologic distress and enhancing social functioning;
- Comparing the benefits of individual vs. group support during the different stages of the grieving process;
- Establishing a link between self-reported and objectively assessed outcomes;
- Comparing the effectiveness of different types of interveners;
- Determining how information regarding bereavement processes influences professional behaviour as well as the behaviour, grieving process, and results of bereaved people.
4.2. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus (COVID-19). Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19 (accessed on 22 March 2022).
- Albuquerque, S.; Teixeira, A.M.; Rocha, J.C. COVID-19 and Disenfranchised Grief. Front. Psychiatry 2021, 12, 638874. [Google Scholar] [CrossRef]
- Laranjeira, C.; Querido, A. Changing rituals and practices surrounding COVID-19 related deaths: Implications for mental health nursing. Br. J. Ment. Health Nurs. 2021, 10, 1–5. [Google Scholar] [CrossRef]
- Mitima-Verloop, H.B.; Mooren, T.; Boelen, P.A. Facilitating grief: An exploration of the function of funerals and rituals in relation to grief reactions. Death Stud. 2021, 45, 735–745. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Fernández, C.; Meneses-Falcón, C. I can’t believe they are dead. Death and mourning in the absence of goodbyes during the COVID-19 pandemic. Health Soc. Care Community 2021. ahead of print. [Google Scholar] [CrossRef]
- Stroebe, M.; Schut, H. Bereavement in Times of COVID-19: A Review and Theoretical Framework. Omega 2021, 82, 500–522. [Google Scholar] [CrossRef]
- Wallace, C.L.; Wladkowski, S.P.; Gibson, A.; White, P. Grief During the COVID-19 Pandemic: Considerations for Palliative Care Providers. J. Pain Symptom Manag. 2020, 60, e70–e76. [Google Scholar] [CrossRef]
- Zhai, Y.; Du, X. Loss and grief amidst COVID-19: A path to adaptation and resilience. Brain Behav. Immun. 2020, 87, 80–81. [Google Scholar] [CrossRef]
- Worden, J.W. Grief Counselling and Grief Therapy: A Handbook for the Mental Health Practitioner, 5th ed.; Springer: London, UK, 2018. [Google Scholar]
- Khosravi, M. Worden’s task-based approach for supporting people bereaved by COVID-19. Curr. Psychol. 2021, 40, 5735–5736. [Google Scholar] [CrossRef]
- Wojtkowiak, J.; Lind, J.; Smid, G.E. Ritual in Therapy for Prolonged Grief: A Scoping Review of Ritual Elements in Evidence-Informed Grief Interventions. Front. Psychiatry 2021, 11, 623835. [Google Scholar] [CrossRef]
- Harrop, E.; Goss, S.; Farnell, D.; Longo, M.; Byrne, A.; Barawi, K.; Torrens-Burton, A.; Nelson, A.; Seddon, K.; Machin, L.; et al. Support needs and barriers to accessing support: Baseline results of a mixed-methods national survey of people bereaved during the COVID-19 pandemic. Palliat. Med. 2021, 35, 1985–1997. [Google Scholar] [CrossRef]
- Johannsen, M.; Damholdt, M.F.; Zachariae, R.; Lundorff, M.; Farver-Vestergaard, I.; O’Connor, M. Psychological interventions for grief in adults: A systematic review and meta-analysis of randomized controlled trials. J. Affect. Disord. 2019, 253, 69–86. [Google Scholar] [CrossRef]
- Maciejewski, P.K.; Maercker, A.; Boelen, P.A.; Prigerson, H.G. “Prolonged grief disorder” and “persistent complex bereavement disorder”, but not “complicated grief”, are one and the same diagnostic entity: An analysis of data from the Yale Bereavement Study. World Psychiatry 2016, 15, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.M. The Many Faces of Grief: A Systematic Literature Review of Grief During the COVID-19 Pandemic. Illn. Crisis Loss 2021. ahead of print. [Google Scholar] [CrossRef]
- Diolaiuti, F.; Marazziti, D.; Beatino, M.F.; Mucci, F.; Pozza, A. Impact and consequences of COVID-19 pandemic on complicated grief and persistent complex bereavement disorder. Psychiatry Res. 2021, 300, 113916. [Google Scholar] [CrossRef]
- Wagner, B.; Rosenberg, N.; Hofmann, L.; Maass, U. Web-Based Bereavement Care: A Systematic Review and Meta-Analysis. Front. Psychiatry 2020, 11, 525. [Google Scholar] [CrossRef]
- Mayland, C.R.; Harding, A.J.E.; Preston, N.; Payne, S. Supporting Adults Bereaved Through COVID-19: A Rapid Review of the Impact of Previous Pandemics on Grief and Bereavement. J. Pain Symptom Manag. 2020, 60, e33–e39. [Google Scholar] [CrossRef]
- Selman, L.E.; Chao, D.; Sowden, R.; Marshall, S.; Chamberlain, C.; Koffman, J. Bereavement Support on the Frontline of COVID-19: Recommendations for Hospital Clinicians. J. Pain Symptom Manag. 2020, 60, e81–e86. [Google Scholar] [CrossRef]
- Dias, N.; Hendricks-Ferguson, V.L.; Wei, H.; Boring, E.; Sewell, K.; Haase, J.E. A Systematic Literature Review of the Current State of Knowledge Related to Interventions for Bereaved Parents. Am. J. Hosp. Palliat. Care 2019, 36, 1124–1133. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Laranjeira, C.; Moura, D.; Marcon, S.; Jaques, A.; Salci, M.A.; Carreira, L.; Cuman, R.; Querido, A. Family bereavement care interventions during the COVID-19 pandemic: A scoping review protocol. BMJ Open 2022, 12, e057767. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 Version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: North Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Borghi, L.; Menichetti, J.; Vegni, E. Early Bereavement Psychological Intervention working group. A Phone-Based Early Psychological Intervention for Supporting Bereaved Families in the Time of COVID-19. Front. Public Health 2021, 9, 625691. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; Martínez-Luna, S.C.; Hernández Jiménez, M.J.; De La Rosa-Gómez, A.; Arenas-Landgrave, P.; Santoveña, E.E.; Arzola-Sánchez, C.; Silva, J.A.; Nicolas, A.M.; Guadián, A.M.; et al. A Self-Applied Multi-Component Psychological Online Intervention Based on UX, for the Prevention of Complicated Grief Disorder in the Mexican Population During the COVID-19 Outbreak: Protocol of a Randomized Clinical Trial. Front. Psychol. 2021, 12, 644782. [Google Scholar] [CrossRef]
- Reitsma, L.; Boelen, P.A.; de Keijser, J.; Lenferink, L.I.M. Online treatment of persistent complex bereavement disorder, posttraumatic stress disorder, and depression symptoms in people who lost loved ones during the COVID-19 pandemic: Study protocol for a randomized controlled trial and a controlled trial. Eur. J. Psychotraumatol. 2021, 12, 1987687. [Google Scholar] [CrossRef]
- Schrauwen, D. The Effectiveness of an Unguided Online Grief-Specific Cognitive Behavioral Therapy for People Who Have Lost a Loved one during the COVID-19 Pandemic. Master’s Thesis, Clinical Psychology, University Utrecht, Utrecht, The Netherlands, 2021. [Google Scholar]
- Tang, R.; Xie, T.; Jiao, K.; Xu, X.; Zou, X.; Qian, W.; Wang, J. Grief Reactions and Grief Counseling among Bereaved Chinese Individuals during COVID-19 Pandemic: Study Protocol for a Randomized Controlled Trial Combined with a Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 9061. [Google Scholar] [CrossRef]
- Menichetti Delor, J.P.; Borghi, L.; Cao di San Marco, E.; Fossati, I.; Vegni, E. Phone follow up to families of COVID-19 patients who died at the hospital: Families’ grief reactions and clinical psychologists’ roles. Int. J. Psychol. 2021, 56, 498–511. [Google Scholar] [CrossRef]
- Mallet, J.; Le Strat, Y.; Colle, M.; Cardot, H.; Dubertret, C. Sustaining the unsustainable: Rapid implementation of a Support Intervention for Bereavement during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2021, 68, 102–103. [Google Scholar] [CrossRef]
- Selman, L.; Farnell, D.; Longo, M.; Goss, S.; Seddon, K.; Torrens-Burton, A.; Mayland, C.R.; Wakefield, D.; Johnston, B.; Byrne, A.; et al. Risk factors associated with poorer experiences of end-of-life care and challenges in early bereavement: Results of a national online survey of people bereaved during the COVID-19 pandemic. Palliat. Med. 2022, 36, 717–729. [Google Scholar] [CrossRef]
- Gesi, C.; Carmassi, C.; Cerveri, G.; Carpita, B.; Cremone, I.M.; Dell’Osso, L. Complicated Grief: What to Expect After the Coronavirus Pandemic. Front. Psychiatry 2020, 11, 489. [Google Scholar] [CrossRef]
- Goveas, J.S.; Shear, M.K. Grief and the COVID-19 Pandemic in Older Adults. Focus 2021, 19, 374–378. [Google Scholar] [CrossRef]
- Boelen, P.A.; Eisma, M.C.; Smid, G.E.; de Keijser, J.; Lenferink, L.I. Remotely delivered cognitive behavior therapy for disturbed grief during the covid-19 crisis: Challenges and opportunities. J. Loss Trauma 2020, 26, 211–219. [Google Scholar] [CrossRef]
- Joaquim, R.; Pinto, A.; Guatimosim, R.; Paula, J.; Costa, D.; Diaz, A.; da Silva, A.G.; Pinheiro, M.I.; Serpa, A.L.; Miranda, D.M.; et al. Bereavement and psychological distress during COVID-19 pandemics: The impact of death experience on mental health. Curr. Opin. Behav. Sci. 2021, 2, 100019. [Google Scholar] [CrossRef]
- Eklund, R.; Eisma, M.C.; Boelen, P.A.; Arnberg, F.K.; Sveen, J. Mobile app for prolonged grief among bereaved parents: Study protocol for a randomised controlled trial. BMJ Open 2021, 11, e052763. [Google Scholar] [CrossRef]
- Mortazavi, S.S.; Shahbazi, N.; Taban, M.; Alimohammadi, A.; Shati, M. Mourning During Corona: A Phenomenological Study of Grief Experience Among Close Relatives During COVID-19 Pandemics. Omega 2021, 302228211032736, ahead of print. [Google Scholar] [CrossRef]
- Søgaard Neilsen, A.; Wilson, R.L. Combining e-mental health intervention development with human computer interaction (HCI) design to enhance technology-facilitated recovery for people with depression and/or anxiety conditions: An integrative literature review. Int. J. Ment. Health Nurs. 2019, 28, 22–39. [Google Scholar] [CrossRef] [Green Version]
- Bartone, P.T.; Bartone, J.V.; Violanti, J.M.; Gileno, Z.M. Peer Support Services for Bereaved Survivors: A Systematic Review. Omega 2019, 80, 137–166. [Google Scholar] [CrossRef]
- Carr, D.; Boerner, K.; Moorman, S. Bereavement in the Time of Coronavirus: Unprecedented Challenges Demand Novel Interventions. J. Aging Soc. Policy 2020, 32, 425–431. [Google Scholar] [CrossRef]

{kind=link}
| Key Concepts | TITLE-ABS-KEY |
|---|---|
| ((“family grief *”) OR (“caregiving grief *”) OR (“bereave *”) OR (“mourn *”) OR (“grieve”) OR (“grieving”) OR (“widow”)) | |
| AND | ((“psychosocial intervention”) OR (“psychotherapeutic intervention”) OR (psychology *) OR (“psychotherapy *”) OR (“counselling”) OR (“therapeutic alliance”) OR (“social support”) OR (“self-care”) OR (“self-management intervention”) OR (“e-health”) OR (“education *”)) |
| AND | ((“pandemic *”) OR (“epidemic *”) OR (“COVID-19”) OR (Corona *) OR (“2019-nCoV”) OR (“SARS-CoV-2”)) |
| Authors/Country | Intervention | Study Design | Study Objectives | Sample Characteristics (n) | Outcomes/Methods | Key Results |
|---|---|---|---|---|---|---|
| Borghi et al. [27]—Italy | Phone-based psychological intervention [27] | Descriptive and cross-sectional study | Describe the experience of a Clinical Psychology Unit in Milan that provided a phone-based early psychological intervention to families of hospitalized COVID-19 patients who died during the pandemic’s first wave [27]. | “284 families were called, and 246 family members received the intervention (38 family members were unreachable)” [27] (p. 3). | Phone calls acted as a psychological intervention to help all families, while also assessing psycho-emotional issues and risk factors that needed more specialized care. The “assessment of risk and protective factors” determined the presence or absence of factors affecting grief, sustaining “coping strategies and resources” from family members, and shaping “how much the complex interplay of very early risk and protective factors may have potentially affected the normal bereavement process in each family member” [27] (p. 4). | Written reports were reported after each call. “Most bereaved family members felt grateful for the call and support”. After this assessment, the family member evaluated to be at risk for grieving difficulties was offered the possibility of a referral for “further psychological support” [27] (p. 4). |
| Mallet et al. [33]—France | The Support Intervention for Bereavement (SIB) involved screening for risk factors in caregivers (CG). Family members could have a one-time intervention or long-term follow-up. The intervention was always individual (one on one). The authors created a hotline number with a dedicated phone (available every weekday, 9am–5pm, with the possibility to record a message). They also created a messaging group to facilitate communication, and produced a letter introducing the SIB, with contact information and condolence letter [33]. | Case study with action research approach | Apply a creative telehealth solution that supports families and provides bereavement care [33]. | After screening, the nurse called 15 relatives (13 bereaved; 2 relatives of patients who were not dead (but with a high mortality risk)), sometimes more than once. The mean duration of each call was thirty minutes. The SIB was also contacted for possible situations leading to death (with survival at the end). Six of the thirteen bereaved contacts were followed up at least four times, for forty-five minutes calls [33]. | First-line intervention (outcomes) —risk factors for complicated grief; —symptoms of acute grief; —adaptive strategies and resilience traits. Second-line intervention Of the 13 bereaved initial contacts, 6 were referred for psychological follow-up with SIB volunteers. This intervention was available according to the situation, discussed by the SIB. With the relative’s authorization, a referral psychologist or psychiatrist could call the bereaved and propose a short follow-up (maximum of 4 calls, mean call duration of 45 min). A cognitive behavioural therapy (CBT) model was used, as it provides a specific framework to treat complex grief reactions [33]. | In all situations, the relative requested help; 38.4% of the bereaved contacts also asked for help in the funerary rituals in the context of COVID-19; 31% also sought help with announcing the death to other family members. None of them had the opportunity to say goodbye. The complaints mainly concerned sleep disorders, anxiety about isolation linked to COVID-19, and loss of appetite. They indicated no suicide intent, but half of them reported a heightened sense of guilt. Two grieving people felt stigmatized and embarrassed to reveal the cause of death to a friend [33]. |
| Menichetti Delor et al. [32]—Italy | Phone call intervention—The main goals were: (a) to support the family by providing a safe space for them to express their loss-related emotions; (b) to verify and sustain spontaneous psycho-emotional resources; and, finally, (c) to refer for additional psychological support if the psychologist observed highly complex/at-risk situations [32]. | Qualitative approach | Evaluate the contents and functions of this early psychological phone follow-up by the clinical psychologists who participated in the calls [32]. | Over the course of three months, 246 families were contacted. Following each conversation, psychologists completed written reports. Such reports described the contents of the conversation and provided further information on the timing and position of the interlocutor within the family [32]. | The following topics were investigated: (i) family experiences and needs that surfaced during the calls; (ii) family solutions in place to cope with loss; (iii) activities taken by the psychologist during the call; and (iv) roles played by the calls according to the interviewee [32] (p. 11). | The findings revealed a convergence in initial reactions of loss and trauma, which was worsened by characteristics specific to the present “emergency scenario, such as a lack of protective factors (e.g., social support, life chances) and the presence of shared precipitating/perpetuating causes (e.g., isolation, feelings of guilt, lack of farewell rituals)” [32] (p. 10). |
| Schrauwen [30]—Netherlands | The intervention consisted of an eight-week unguided online behavioural therapy (including exposure, cognitive restructuring, and behavioural activation) [30]. | RCT | Investigate the efficacy of an online grief-specific cognitive behavioural therapy (CBT) intervention for bereaved individuals during the COVID-19 pandemic [30]. | Eligible participants were randomly attributed to either the treatment group (N = 21) or waitlist-control group (N = 32) [30]. | Persistent Complex Bereavement Disorder (PCBD), post-traumatic stress disorder (PTSD), and depression symptom severity were assessed during (1) pre-treatment/pre-waiting period and (2) post-treatment and/or post-waiting period. Assessment consisted of clinical telephone interviews [30]. | Analysis found a significant effect of the online grief-specific CBT-intervention on PCBD and PTSD symptom levels, with a stronger effect for PCBD [30]. |
| Dominguez-Rodriguez et al. [28]—México | Online multi-component psychological intervention (based on cognitive behavioural therapy (CNT), mindfulness, behavioural activation therapy (BAT), and positive psychology (PP)) [28]. | RCT—study protocol | Provide a self-administered intervention consisting of 12 sessions based on CBT, mindfulness, BAT, and PP, with the goal of lowering the risk of developing Complicated Grief Disorder (CGD), especially from the COVID-19 contingency, and improving quality of life [28]. | Eligible participants: - Adults (>18 years old) who had suffered the loss of a loved one in a period no longer than 6 months prior to the study; - Symptoms of general anxiety disorder and/or depression and/or, grief symptoms; - Access to a communication device with access to the internet [28]. | Intended outcomes: Improved life satisfaction and quality of life are expected following the conclusion of the intervention. After the intervention, anxiety and depression symptoms are expected to decrease, and sleep quality to improve. Such changes are likely to last between 3 and 6 months after the intervention procedure is completed [28]. | Not reported |
| Tang et al. [31]—China | Online grief counselling program [31] | RCT—study protocol | Investigate the mental health of bereaved people during the COVID-19 pandemic, train grief counsellors to support the bereaved people, and assess the effectiveness of grief counselling [31]. | “160 Chinese bereaved people will be recruited online. Participants in this research must be over the age of 18 and have lost first-degree relatives during COVID-19 [31] (p. 8). | Intended outcomes: “reducing prolonged grief symptoms, post-traumatic symptoms, depression levels, and suicidal intentions in bereaved individuals” [31] (p. 8). | Not reported |
| Reitsma et al. [29]—Germany | Grief-specific online CBT (based on psychoeducation; cognitive restructuring assignments; exposure; behavioural activation assignments) [29] | RCT—study protocol | Examine the effectiveness of grief-specific online CBT in lowering PCBD, PTSD, and depressive symptoms in bereaved people due to COVID-19 pandemic [29]. | Participants are people who lost a loved one at least 3 months earlier during the COVID-19 pandemic with clinically relevant levels of PCBD, PTSD, and/or depression [29]. | Intended outcomes: decreasing symptom-levels of PCBD, PTSD, and depression [29]. | Not reported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laranjeira, C.; Moura, D.; Salci, M.A.; Carreira, L.; Covre, E.; Jaques, A.; Cuman, R.N.; Marcon, S.; Querido, A. A Scoping Review of Interventions for Family Bereavement Care during the COVID-19 Pandemic. Behav. Sci. 2022, 12, 155. https://doi.org/10.3390/bs12050155
Laranjeira C, Moura D, Salci MA, Carreira L, Covre E, Jaques A, Cuman RN, Marcon S, Querido A. A Scoping Review of Interventions for Family Bereavement Care during the COVID-19 Pandemic. Behavioral Sciences. 2022; 12(5):155. https://doi.org/10.3390/bs12050155
Chicago/Turabian StyleLaranjeira, Carlos, Débora Moura, Maria Aparecida Salci, Lígia Carreira, Eduardo Covre, André Jaques, Roberto Nakamura Cuman, Sonia Marcon, and Ana Querido. 2022. "A Scoping Review of Interventions for Family Bereavement Care during the COVID-19 Pandemic" Behavioral Sciences 12, no. 5: 155. https://doi.org/10.3390/bs12050155
APA StyleLaranjeira, C., Moura, D., Salci, M. A., Carreira, L., Covre, E., Jaques, A., Cuman, R. N., Marcon, S., & Querido, A. (2022). A Scoping Review of Interventions for Family Bereavement Care during the COVID-19 Pandemic. Behavioral Sciences, 12(5), 155. https://doi.org/10.3390/bs12050155