Anxiety and Depression in Belgium during the First 15 Months of the COVID-19 Pandemic: A Longitudinal Study

 , ,
, ,
Abstract
:1. Introduction
- (1)
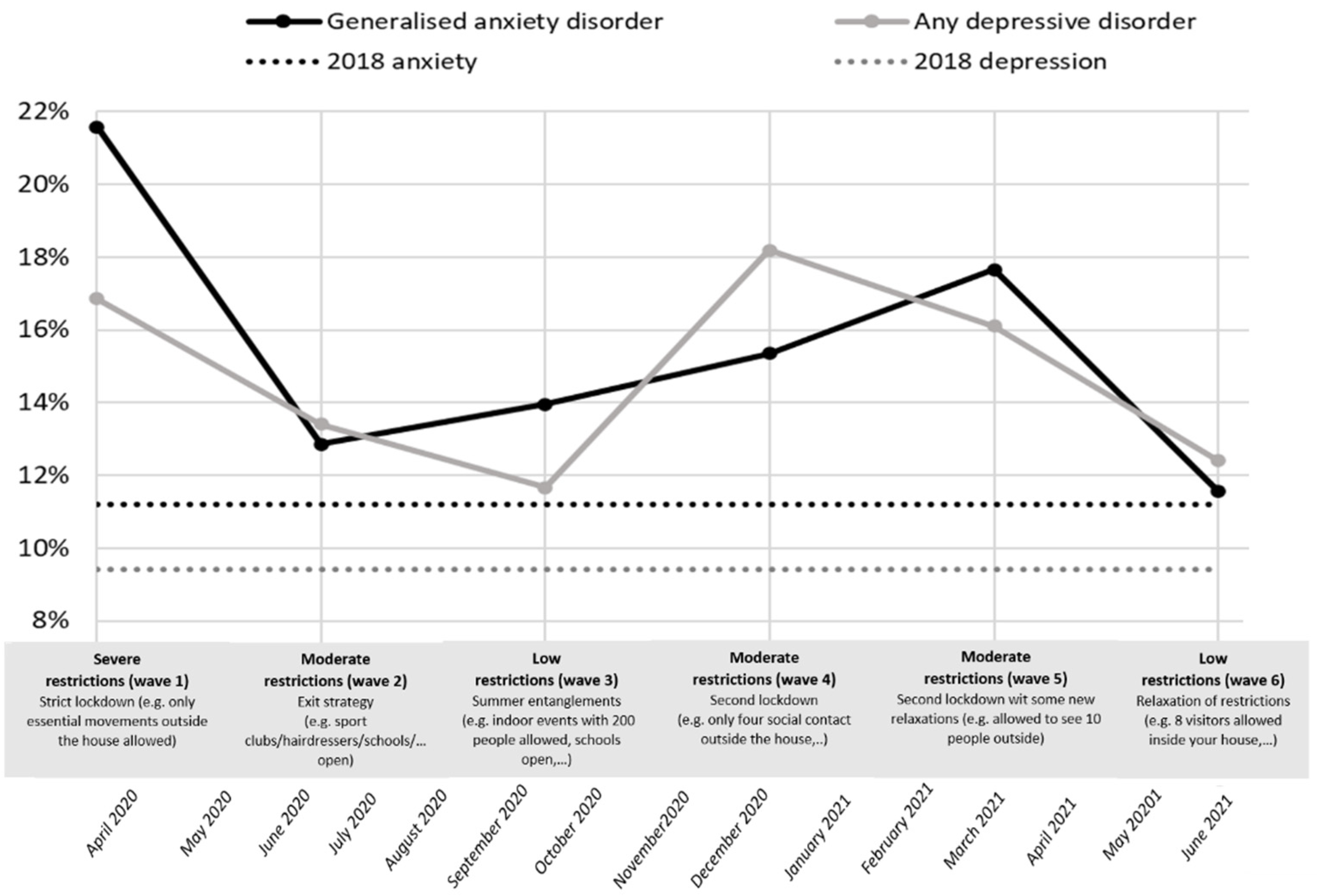
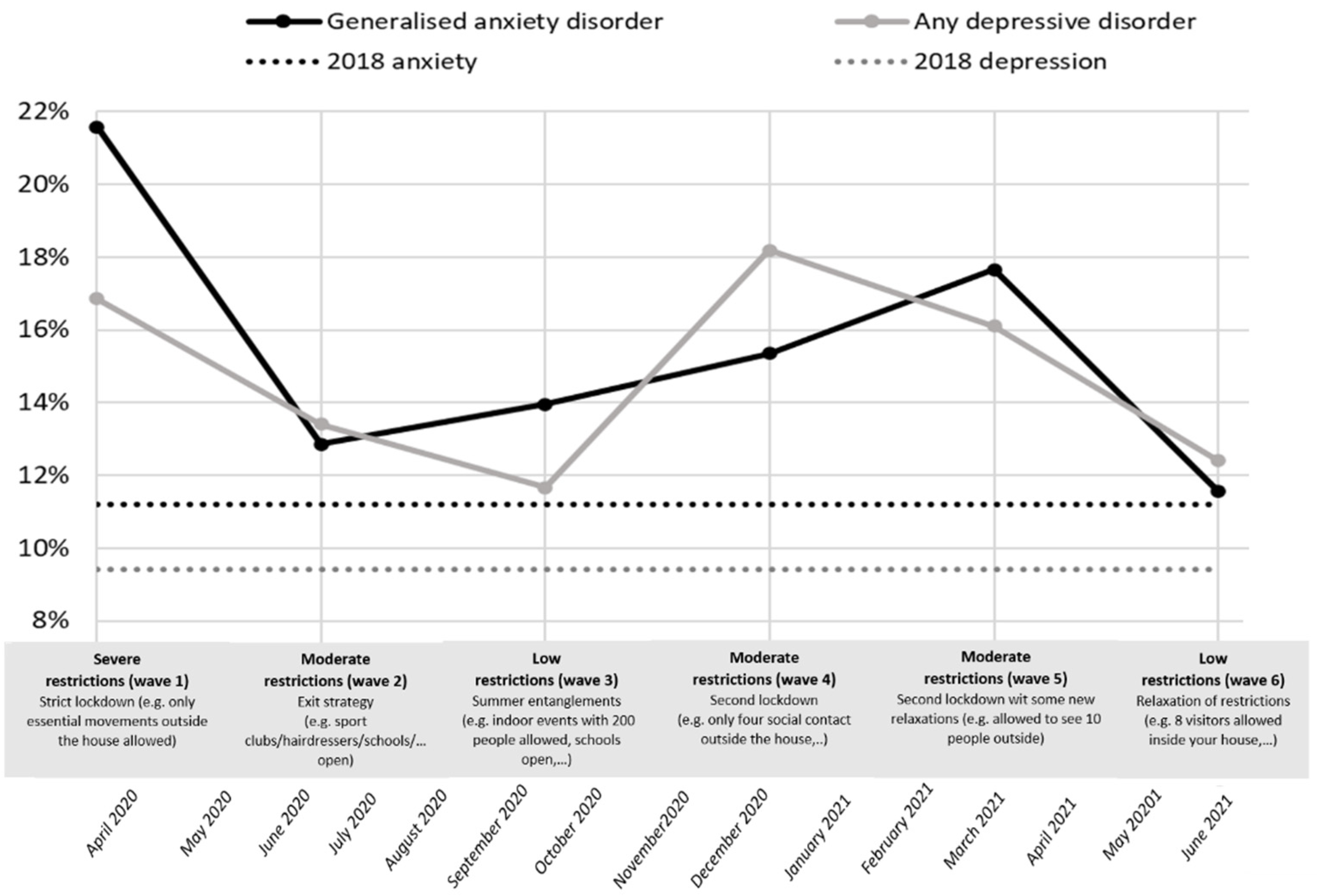
- During the first 15 months of the pandemic in Belgium, times of strict lockdown measures are associated with a higher prevalence of symptoms of anxiety and depression, compared with times of relaxation of the measures;
- (2)
- The following risk factors are associated with anxiety and depression during the COVID-19 pandemic in Belgium: female gender, young age, single parent, extravert personality, exposure to COVID-19, lower level of education, and having a pre-existing mental health problem;
- (3)
- Time periods with stricter policy measures have greater impacts on mental distress among the high-risk groups mentioned above.
2. Materials and Methods
2.1. Setting
2.2. Dataset
2.3. Measures
2.3.1. Mental Distress
2.3.2. Predictor Variables
2.3.3. Statistical Analysis
2.3.4. Model Building
3. Results
3.1. Descriptive Statistics
3.2. Predictors of Mental Distress
3.2.1. Anxiety
3.2.2. Depression
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- −
- Feeling nervous or anxious;
- −
- Not being able to stop worrying or not being able to control your worries;
- −
- Worrying too much about different things;
- −
- Having difficulty relaxing;
- −
- Being so restless that it’s difficult for you to keep still;
- −
- Being easily upset or irritable and feeling scared.
- −
- Having little interest or pleasure in activities;
- −
- Feeling down, depressed, or hopeless;
- −
- Trouble falling or staying asleep, or sleeping too much;
- −
- Feeling tired or having little energy;
- −
- Poor appetite or overeating;
- −
- Feeling bad about yourself—or that you are a failure or have let yourself or your family down;
- −
- Trouble concentrating on things, such as reading the newspaper or watching television;
- −
- Thoughts that you would be better off if you were no longer alive;
- −
- Feeling lonely.
Appendix B
References
- Daly, M.; Sutin, A.R.; Robinson, E. Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Acaps. COVID-19 Government Measures Dataset. 2021. Available online: https://www.acaps.org/covid-19-government-measures-dataset (accessed on 10 April 2022).
- WHO. Coronavirus Disease (COVID-19) Situation Reports. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 20 March 2022).
- Chaturvedi, K.; Vishwakarma, D.K.; Singh, N. COVID-19 and its impact on education, social life and mental health of students: A survey. Child. Youth Serv. Rev. 2020, 121, 105866. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D. The COVID-19 outbreak: Crucial role the psychiatrists can play. Asian J. Psychiatry 2020, 50, 102014. [Google Scholar] [CrossRef] [PubMed]
- Lorant, V.; Smith, P.; Broeck, K.V.D.; Nicaise, P. Psychological distress associated with the COVID-19 pandemic and suppression measures during the first wave in Belgium. BMC Psychiatry 2021, 21, 112. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain. Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Green, P. Risks to children and young people during COVID-19 pandemic. BMJ 2020, 369, m1669. [Google Scholar] [CrossRef]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child. Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Li, L.Z.; Wang, S. Prevalence and predictors of general psychiatric disorders and loneliness during COVID-19 in the United Kingdom. Psychiatry Res. 2020, 291, 113267. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Shi, L.; Lu, Z.-A.; Que, J.-Y.; Huang, X.-L.; Liu, L.; Ran, M.-S.; Gong, Y.-M.; Yuan, K.; Yan, W.; Sun, Y.-K.; et al. Prevalence of and Risk Factors Associated With Mental Health Symptoms Among the General Population in China During the Coronavirus Disease 2019 Pandemic. JAMA Netw. Open 2020, 3, e2014053. [Google Scholar] [CrossRef]
- Holingue, C.; Badillo-Goicoechea, E.; Riehm, K.E.; Veldhuis, C.B.; Thrul, J.; Johnson, R.M.; Fallin, M.D.; Kreuter, F.; Stuart, E.A.; Kalb, L.G. Mental distress during the COVID-19 pandemic among US adults without a pre-existing mental health condition: Findings from American trend panel survey. Prev. Med. 2020, 139, 106231. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain. Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Smillie, L.D.; Kern, M.L.; Uljarevic, M. Extraversion: Description, development, and mechanisms. In Handbook of Personality Development; Guilford Publications: New York, NY, USA, 2018; pp. 118–136. [Google Scholar]
- Zelenski, J.M.; Sobocko, K.; Whelan, A.D.C. Introversion, Solitude, and Subjective Well-Being. In The Handbook of Solitude: Psychological Perspectives on Social Isolation, Social Withdrawal, and Being Alone, 1st ed.; Coplan, R.J., Bowker, J.C., Eds.; Wiley: Hoboken, NJ, USA, 2013; pp. 184–201. [Google Scholar] [CrossRef]
- Harris, K.; English, T.; Harms, P.D.; Gross, J.J.; Jackson, J.J. Why Are Extraverts More Satisfied? Personality, Social Experiences, and Subjective Well–Being in College. Eur. J. Personal. 2017, 31, 170–186. [Google Scholar] [CrossRef]
- Lucas, R.E.; Le, K.; Dyrenforth, P.S. Explaining the Extraversion/Positive Affect Relation: Sociability Cannot Account for Extraverts’ Greater Happiness. J. Pers. 2008, 76, 385–414. [Google Scholar] [CrossRef]
- Srivastava, S.; Angelo, K.M.; Vallereux, S.R. Extraversion and positive affect: A day reconstruction study of person–environment transactions. J. Res. Personal. 2008, 42, 1613–1618. [Google Scholar] [CrossRef]
- Drieskens, S.; Berger, N.; Vandevijvere, S.; Gisle, L.; Braekman, E.; Charafeddine, R.; De Ridder, K.; Demarest, S. Short-term impact of the COVID-19 confinement measures on health behaviours and weight gain among adults in Belgium. Arch. Public Health 2021, 79, 1. [Google Scholar] [CrossRef]
- Gisle, L.; Drieskens, S.; Demarest, S.; Van der Heyden, J. Enquête de Santé 2018: Santé Mentale. Sciensano.be. 2018. Available online: https://www.sciensano.be/fr/biblio/enquete-de-sante-2018-sante-mentale (accessed on 20 March 2022).
- Demarest, S.; Berete, F.; Charafeddine, R.; van der Heyden, J. Méthodologie, Enquête de Santé 2018. Sciensano. 2018. Available online: https://www.sciensano.be/sites/default/files/method_fr_2018.pdf (accessed on 10 April 2022).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2010, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Kocalevent, R.-D.; Berg, L.; Beutel, M.E.; Hinz, A.; Zenger, M.; Härter, M.; Nater, U.; Brähler, E. Social support in the general population: Standardization of the Oslo social support scale (OSSS-3). BMC Psychol. 2018, 6, 31. [Google Scholar] [CrossRef] [PubMed]
- Soto, C.; John, O.P. Short and extra-short forms of the Big Five Inventory–2: The BFI-2-S and BFI-2-XS. J. Res. Personal. 2017, 68, 69–81. [Google Scholar] [CrossRef]
- Deutskens, E.; De Ruyter, J.; Wetzels, M.; Oosterveld, P. Response Rate and Response Quality of Internet-Based Surveys: An Experimental Study. Mark. Lett. 2004, 15, 21–36. [Google Scholar] [CrossRef] [Green Version]
- John, O.; Soto, C. The importance of being valid: Reliability and the process of construct validation. In Handbook of Research Methods in Personality Psychology; The Guilford Press: New York, NY, USA, 2007; pp. 461–494. [Google Scholar]
- Altman, D.G.; Royston, P. The cost of dichotomising continuous variables. BMJ 2006, 332, 1080. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, A.A.; McCoach, D.B. Multilevel Modeling of Educational Data; IAP: Charlotte, NC, USA, 2008. [Google Scholar]
- Little, R.J.A. A Test of Missing Completely at Random for Multivariate Data with Missing Values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Berglund, P.A. Using SAS for Multiple Imputation and Analysis of Longitudinal Data. In Proceedings of the SAS® Global Forum 2018 Conference, Denver, CO, USA, 8–11 April 2018; Available online: https://www.sas.com/content/dam/SAS/support/en/sas-global-forum-proceedings/2018/1738-2018.pdf (accessed on 10 April 2022).
- Beutels, P.; Pepermans, K. Mentaal Welzijn in Tijden van COVID-19: Ups en Downs van een Bevolking Onder Druk. 2020. Available online: https://blog.uantwerpen.be/corona/mentaal-welzijn/ (accessed on 1 December 2020).
- Lorant, V.; van den Broeck, K. Evaluation de l’état de Santé Mentale et Santé Sociale de la Population Belge Pendant la Période du Confinement: Résultats de la Vague 1 et 2.’ UCLouvain, Universiteit Antwerpen. 2019. Available online: https://cdn.uclouvain.be/groups/cms-editors-irss/irss-sophie/rapport_covidetmoi_vague1et2.pdf (accessed on 20 May 2020).
- Généreux, M.; Schluter, P.J.; Hung, K.K.; Wong, C.S.; Mok, C.P.Y.; O’Sullivan, T.; David, M.D.; Carignan, M.-E.; Blouin-Genest, G.; Champagne-Poirier, O.; et al. One Virus, Four Continents, Eight Countries: An Interdisciplinary and International Study on the Psychosocial Impacts of the COVID-19 Pandemic among Adults. Int. J. Environ. Res. Public Health 2020, 17, 8390. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 10227. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- McLean, C.P.; Anderson, E.R. Brave men and timid women? A review of the gender differences in fear and anxiety. Clin. Psychol. Rev. 2009, 29, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Bekker, M.H.; van Mens-Verhulst, J. Anxiety Disorders: Sex Differences in Prevalence, Degree, and Background, But Gender-Neutral Treatment. Gend. Med. 2007, 4, S178–S193. [Google Scholar] [CrossRef]
- Carter, R.; Silverman, W.K.; Jaccard, J. Sex Variations in Youth Anxiety Symptoms: Effects of Pubertal Development and Gender Role Orientation. J. Clin. Child. Adolesc. Psychol. 2011, 40, 730–741. [Google Scholar] [CrossRef] [PubMed]
- Lengua, L.J.; Stormshak, E.A. Gender, gender roles, and personality: Gender differences in the prediction of coping and psychological symptoms. Sex Roles 2000, 43, 787–820. [Google Scholar] [CrossRef]
- Andrew, A.; Cattan, S.; Dias, M.C.; Farquharson, C.; Kraftman, L.; Krutikova, S.; Phimister, A.; Sevilla, A. Inequalities in Children’s Experiences of Home Learning during the COVID-19 Lockdown in England. Fisc. Stud. 2020, 41, 653–683. [Google Scholar] [CrossRef]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Yao, L.; Bai, H.; Cai, Z.; Yang, B.X.; et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain. Behav. Immun. 2020, 87, 11–17. [Google Scholar] [CrossRef]
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, H.; Zeng, H.; Zhang, S.; Du, Q.; Jiang, T.; Du, B. The differential psychological distress of populations affected by the COVID-19 pandemic. Brain. Behav. Immun. 2020, 87, 49–50. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef] [PubMed]
- Orben, A.; Tomova, L.; Blakemore, S.-J. The effects of social deprivation on adolescent development and mental health. Lancet Child. Adolesc. Health 2020, 4, 634–640. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Havenaar, J.M.; Cwikel, J.; Bromet, E.J. Toxic Turmoil: Psychological and Societal Consequences of Ecological Disasters; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2002. [Google Scholar]
- Altemus, M.; Sarvaiya, N.; Epperson, C.N. Sex differences in anxiety and depression clinical perspectives. Front. Neuroendocrinol. 2014, 35, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Every-Palmer, S.; Jenkins, M.; Gendall, P.; Hoek, J.; Beaglehole, B.; Bell, C.; Williman, J.; Rapsey, C.; Stanley, J. Psychological distress, anxiety, family violence, suicidality, and wellbeing in New Zealand during the COVID-19 lockdown: A cross-sectional study. PLoS ONE 2020, 15, e0241658. [Google Scholar] [CrossRef] [PubMed]
- Van Droogenbroeck, F.; Spruyt, B.; Keppens, G. Gender differences in mental health problems among adolescents and the role of social support: Results from the Belgian health interview surveys 2008 and 2013. BMC Psychiatry 2018, 18, 6. [Google Scholar] [CrossRef] [Green Version]
- Layard, R.; Clark, A.; Senik, C. The causes of happiness and misery. In World Happiness Report; United Nations: New York, NY, USA, 2012; pp. 58–89. [Google Scholar]
- Mahamid, F.A.; Veronese, G.; Bdier, D. Fear of coronavirus (COVID-19) and mental health outcomes in Palestine: The mediating role of social support. Curr. Psychol. 2021, 1–10. [Google Scholar] [CrossRef]
- Wiederhold, B.K. Social Media Use During Social Distancing. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 275–276. [Google Scholar] [CrossRef] [Green Version]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative synthesis of psychological and coping responses towards emerging infectious disease outbreaks in the general population: Practical considerations for the COVID-19 pandemic. Singap. Med. J. 2020, 61, 350–356. [Google Scholar] [CrossRef]
- Besser, A.; Priel, B. Attachment, depression, and fear of death in older adults: The roles of neediness and perceived availability of social support. Personal. Individ. Differ. 2008, 44, 1711–1725. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Paulino, M.; Dumas-Diniz, R.; Brissos, S.; Brites, R.; Alho, L.; Simões, M.R.; Silva, C.F. COVID-19 in Portugal: Exploring the immediate psychological impact on the general population. Psychol. Health Med. 2020, 26, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.-Y.; Kok, A.A.L.; Eikelenboom, M.; Horsfall, M.; Jörg, F.; Luteijn, R.A.; Rhebergen, D.; van Oppen, P.; Giltay, E.J.; Penninx, B.W.J.H. The mental health impact of the COVID-19 pandemic on people with and without depressive, anxiety, or obsessive-compulsive disorders: A longitudinal study of three Dutch case-control cohorts. Lancet Psychiatry 2021, 8, 121–129. [Google Scholar] [CrossRef]
- Anglim, J.; Horwood, S.; Smillie, L.D.; Marrero, R.J.; Wood, J.K. Predicting psychological and subjective well-being from personality: A. meta-analysis. Psychol. Bull. 2020, 146, 279–323. [Google Scholar] [CrossRef] [Green Version]
- Steel, P.; Schmidt, J.; Shultz, J. Refining the relationship between personality and subjective well-being. Psychol. Bull. 2008, 134, 138–161. [Google Scholar] [CrossRef]
- Folk, D.; Okabe-Miyamoto, K.; Dunn, E.; Lyubomirsky, S. Did Social Connection Decline During the First Wave of COVID-19?: The Role of Extraversion. Collabra Psychol. 2020, 6, 1. [Google Scholar] [CrossRef]
- Wijngaards, I.; De Zilwa, S.C.M.S.; Burger, M.J. Extraversion Moderates the Relationship Between the Stringency of COVID-19 Protective Measures and Depressive Symptoms. Front. Psychol. 2020, 11, 568907. [Google Scholar] [CrossRef]
- Braekman, E.; Drieskens, S.; Charafeddine, R.; Demarest, S.; Berete, F.; Gisle, L.; Tafforeau, J.; Van Der Heyden, J.; Van Hal, G. Mixing mixed-mode designs in a national health interview survey: A pilot study to assess the impact on the self-administered questionnaire non-response. BMC Med. Res. Methodol. 2019, 19, 212. [Google Scholar] [CrossRef] [Green Version]
- Braekman, E.; Charafeddine, R.; Demarest, S.; Drieskens, S.; Berete, F.; Gisle, L.; Van der Heyden, J.; Van Hal, G. Comparing web-based versus face-to-face and paper-and-pencil questionnaire data collected through two Belgian health surveys. Int. J. Public Health 2020, 65, 5–16. [Google Scholar] [CrossRef]
- Evans, J.R.; Mathur, A. The value of online surveys. Internet Res. 2005, 15, 195–219. [Google Scholar] [CrossRef]
- Spiritus-Beerden, E.; Verelst, A.; Devlieger, I.; Langer Primdahl, N.; Botelho Guedes, F.; Chiarenza, A.; De Maesschalck, S.; Durbeej, N.; Garrido, R.; Gaspar de Matos, M.; et al. Mental Health of Refugees and Migrants during the COVID-19 Pandemic: The Role of Experienced Discrimination and Daily Stressors. Int. J. Environ. Res. Public. Health 2021, 18, 6354. [Google Scholar] [CrossRef] [PubMed]
- Braekman, E.; Demarest, S.; Charafeddine, R.; Drieskens, S.; Berete, F.; Gisle, L.; Van der Heyden, J.; Van Hal, G. Unit Response and Costs in Web Versus Face-To-Face Data Collection: Comparison of Two Cross-sectional Health Surveys. J. Med. Internet Res. 2022, 24, e26299. [Google Scholar] [CrossRef] [PubMed]
- Infurna, F.J.; Luthar, S.S. Re-evaluating the notion that resilience is commonplace: A review and distillation of directions for future research, practice, and policy. Clin. Psychol. Rev. 2018, 65, 43–56. [Google Scholar] [CrossRef]
- Kissler, S.M.; Tedijanto, C.; Goldstein, E.; Grad, Y.H.; Lipsitch, M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science 2020, 368, 860–868. [Google Scholar] [CrossRef]
- Trautmann, S.; Rehm, J.; Wittchen, H.-U. The economic costs of mental disorders: Do our societies react appropriately to the burden of mental disorders? EMBO Rep. 2016, 17, 1245–1249. [Google Scholar] [CrossRef]

{kind=link}
| T1 | 2–9 April 2020 | N = 49,335 | Severe restrictions | Strict lockdown (e.g., only essential movements outside the house allowed) |
| T2 | 28 May–5 June 2020 | N = 33,913 | Moderate restrictions | Exit strategy (e.g., sports clubs/hairdressers/schools/etc. open) |
| T3 | 24 September–2 October 2020 | N = 30,845 | Low restrictions | Summer entanglements (e.g., indoor events with 200 people allowed, etc.) |
| T4 | 3–11 December 2020 | N = 29,855 | Moderate restrictions | Second lockdown (e.g., only four social contacts outside the house allowed, etc.) |
| T5 | 18–25 March 2021 | N = 20,410 | Moderate restrictions | Second lockdown with some relaxations (e.g., allowed to see 10 people outside, etc.) |
| T6 | 10–20 June 2021 | N = 17,774 | Low restrictions | Relaxation of restrictions (e.g., 8 visitors inside your house allowed, etc.) |
| T1 | T2 | T3 | T4 | T5 | T6 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | N | % | ||
| Gender | Men | 675 | 36.7 | 672 | 36.5 | 675 | 36.7 | 671 | 36.6 | 672 | 36.6 | 671 | 36.5 |
| Women | 1162 | 63.2 | 1165 | 63.4 | 1160 | 63.2 | 1164 | 63.4 | 1164 | 63.3 | 1165 | 63.4 | |
| Other | 1 | 0.1 | 1 | 0.1 | 1 | 0.1 | 1 | 0.1 | 2 | 0.1 | 2 | 0.1 | |
| Region | Flanders | 1182 | 64.3 | 1181 | 64.3 | 1176 | 64.1 | 1178 | 64.2 | 1180 | 64.2 | 1178 | 64.2 |
| Brussels | 199 | 10.8 | 201 | 10.9 | 203 | 11.1 | 203 | 11.1 | 202 | 11.0 | 204 | 11.0 | |
| Walloon | 457 | 24.9 | 456 | 24.8 | 455 | 24.8 | 455 | 24.8 | 456 | 24.8 | 456 | 24.8 | |
| Age | 18–29 | 94 | 5.1 | 91 | 5.2 | 96 | 5.2 | 94 | 5.1 | 66 | 3.6 | 68 | 3.6 |
| 30–49 | 591 | 32.2 | 591 | 32.1 | 588 | 32.2 | 592 | 32.2 | 584 | 31.8 | 585 | 31.8 | |
| 50–64 | 682 | 37.1 | 682 | 37.1 | 682 | 37.1 | 680 | 37.0 | 659 | 35.9 | 657 | 35.8 | |
| 65+ | 471 | 25.6 | 470 | 25.6 | 469 | 25.6 | 470 | 25.6 | 529 | 28.8 | 528 | 28.8 | |
| Average age ± standard deviation | 45.8 ± 14.2 | 49.9 ± 14.4 | 50.8 ± 14 | 51.4 ± 14.2 | 53.2 ± 14.1 | 52.7 ± 14.7 | |||||||
| Household composition | Living alone, without children | 389 | 21.2 | 399 | 21.7 | 404 | 22.0 | 411 | 22.4 | 414 | 22.5 | 417 | 22.7 |
| Couple, without child(ren) | 748 | 40.7 | 746 | 40.6 | 738 | 40.2 | 749 | 40.8 | 746 | 40.6 | 753 | 41.0 | |
| Couple, with child(ren) | 497 | 27.0 | 499 | 27.2 | 512 | 27.8 | 495 | 27.0 | 499 | 27.1 | 485 | 26.4 | |
| Living alone, with children | 93 | 5.1 | 92 | 5.0 | 89 | 4.9 | 92 | 5.0 | 91 | 5.0 | 92 | 5.0 | |
| Together with parent(s), family, friends or acquaintances | 82 | 4.5 | 84 | 4.6 | 76 | 4.1 | 75 | 4.1 | 72 | 3.9 | 74 | 4.0 | |
| Other | 29 | 1.6 | 18 | 1.0 | 17 | 0.9 | 14 | 0.8 | 16 | 0.9 | 17 | 0.9 | |
| Work status | Paid job | 1128 | 61.4 | 1125 | 61.2 | 1099 | 59.8 | 1097 | 59.7 | 1091 | 59.4 | 1089 | 59.4 |
| Unemployed (not temporarily interrupted)) | 43 | 2.3 | 43 | 2.3 | 40 | 2.2 | 35 | 1.9 | 40 | 2.2 | 40 | 2.1 | |
| Invalidity | 47 | 2.6 | 47 | 2.6 | 45 | 2.5 | 44 | 2.4 | 46 | 2.5 | 46 | 2.5 | |
| Studies | 16 | 0.9 | 17 | 0.9 | 16 | 0.9 | 15 | 0.8 | 14 | 0.8 | 14 | 0.7 | |
| Retirement | 534 | 29.0 | 549 | 29.9 | 570 | 31.1 | 577 | 31.4 | 590 | 32.1 | 595 | 32.4 | |
| Household work | 43 | 2.3 | 43 | 2.3 | 45 | 2.4 | 43 | 2.3 | 40 | 2.2 | 40 | 2.1 | |
| Other | 27 | 1.5 | 14 | 0.8 | 20 | 1.1 | 25 | 1.4 | 16 | 0.9 | 13 | 0.7 | |
| Education | Secondary degree (or lower) | 477 | 25.9 | 476 | 25.8 | 481 | 26.2 | 474 | 25.8 | 475 | 25.8 | 479 | 26 |
| Higher education | 1361 | 74.1 | 1362 | 74.2 | 1355 | 73.8 | 1362 | 74.2 | 1363 | 74.2 | 1359 | 74 | |
| Infected/Exposed to COVID-19 | Yes | 1364 | 74.2 | 1362 | 74.2 | 1363 | 74.2 | 1362 | 74.2 | 1364 | 74.2 | 1362 | 74.2 |
| No | 474 | 25.8 | 473 | 25.8 | 474 | 25.8 | 474 | 25.8 | 474 | 25.8 | 475 | 25.8 | |
| Social Support | |||||||||||||
| Poor | 479 | 26 | 486 | 26.4 | 425 | 23.1 | 628 | 34.2 | 548 | 29.8 | 399 | 21.7 | |
| Moderate | 940 | 51.2 | 875 | 47.7 | 920 | 50.2 | 853 | 46.4 | 904 | 49.2 | 855 | 46.6 | |
| Strong | 419 | 22.8 | 476 | 25.9 | 490 | 26.7 | 354 | 19.3 | 386 | 21.0 | 584 | 31.8 | |
| Personality traits | Introversion | 239 | 13.0 | 239 | 13.0 | 238 | 13.0 | 239 | 13.0 | 239 | 13.0 | 240 | 13.0 |
| Middle | 1288 | 70.1 | 1288 | 70.1 | 1288 | 70.1 | 1286 | 70.1 | 1288 | 70.1 | 1286 | 70.1 | |
| Extraversion | 311 | 16.9 | 311 | 16.9 | 310 | 16.9 | 311 | 16.9 | 311 | 16.9 | 312 | 16.9 | |
| Pre-existing mental health problem | Yes | 189 | 10.3 | 189 | 10.3 | 189 | 10.2 | 189 | 10.3 | 189 | 10.3 | 191 | 10.3 |
| No | 1648 | 89.7 | 1649 | 89.7 | 1647 | 89.8 | 1647 | 89.7 | 1648 | 89.7 | 1647 | 89.7 | |
| Model 1 (Intercept Only) | Model 2 (Time) | Model 3 (Time + Background Variables) | Model 4 (Other Explanatory Variables) | Model 5 (Time * Gender) | ||
|---|---|---|---|---|---|---|
| Estimate (SE) | Estimate (SE) | Estimate (SE) | Estimate (SE) | Estimate (SE) | ||
| Fixed effects | ||||||
| Intercept | 4.16 *** (1.00) | 3.89 *** (0.11) | 2.37 *** (0.28) | 0.77 *** (0.37) | 0.83 * (0.37) | |
| Time | 1 | 1.17 *** (0.09) | 1.16 *** (0.09) | 1.12 *** (0.09) | 0.75 *** (0.15) | |
| 2 | −0.16 (0.09) | −0.17 (0.09) | −0.20 * (0.09) | −0.08 (0.15) | ||
| 3 (ref.) | ||||||
| 4 | 0.55 *** (0.09) | 0.56 *** (0.09) | 0.43 *** (0.09) | 0.35 * (0.15) | ||
| 5 | 0.36 *** (0.09) | 0.40 *** (0.09) | 0.31 *** (0.09) | 0.33 * (0.15) | ||
| 6 | −0.26 ** (0.09) | −0.21 * (0.09) | −0.18 * (0.09) | −0.23 (0.15) | ||
| Gender | Man (ref.) | |||||
| Woman | 0.84 *** (0.18) | 0.79 *** (0.17) | 0.69 *** (0.21) | |||
| Region | Flanders (ref.) | |||||
| Brussels | 0.92 ** (0.29) | 0.77 * (0.27) | 0.77 ** (0.27) | |||
| Walloon | 0.95 *** (0.21) | 0.90 *** (0.20) | 0.90 *** (0.20) | |||
| Age | 18–29 (ref.) | 1.50 *** (0.40) | 1.31 ** (0.39) | 1.32 ** (0.39) | ||
| 30–49 | 1.38 *** (0.26) | 1.07 *** (0.26) | 1.08 *** (0.26) | |||
| 50–64 | 0.48 * (0.21) | 0.29 (0.21) | 0.30 (0.21) | |||
| 65+ | - | - | - | |||
| Household type | Living alone, without children | −0.06 (0.20) | −0.28 (0.19) | −0.28 (0.19) | ||
| Couple, without child(ren) (ref.) | - | - | - | |||
| Couple, with child(ren) | 0.05(0.18) | 0.04(0.18) | 0.03(0.17) | |||
| Living alone, with children | −0.06 (0.32) | −0.32 (0.31) | −0.33 (0.31) | |||
| Together with parent(s), family, friends, or acquaintances | −0.22 (0.34) | −0.28 (0.33) | −0.31 (0.33) | |||
| Other | −0.59 (0.40) | −0.71 (0.39) | −0.70 (0.39) | |||
| Work status | Paid job (ref.) | - | - | - | ||
| Unemployed (not temporarily interrupted)) | 0.82 * (0.32) | 0.70 * (0.32) | 0.70 * (0.32) | |||
| Invalidity | 0.85 * (0.39) | 0.39 (0.38) | 0.40 (0.38) | |||
| Studies | −0.12 (0.60) | 0.00 (0.59) | −0.01 (0.59) | |||
| Retirement | −0.70 *** (0.20) | −0.68 *** (0.20) | −0.68 *** (0.20) | |||
| Household work | 0.31 (0.41) | 0.39 (0.41) | 0.40 (0.41) | |||
| Other | 0.17 (0.38) | 0.17 (0.37) | 0.16 (0.37) | |||
| Education | Secondary degree (or lower) | 0.51 ** (0.17) | 0.45 ** (0.17) | 0.44 ** (0.17) | ||
| Higher degree (ref.) | ||||||
| Infected/exposed to COVID−19 | Yes | 0.47 ** (0.19) | 0.47 ** (0.19) | |||
| No (ref.) | ||||||
| Social support | Poor | 1.32 *** (0.12) | 1.32 *** (0.12) | |||
| Moderate | 0.44 *** (0.09) | 0.45 *** (0.09) | ||||
| Strong (ref.) | ||||||
| Personality traits | Introvert (ref.) | - | ||||
| Middle | 0.64 * (0.25) | 0.64 * (0.25) | ||||
| Extravert | 1.98 *** (0.31) | 1.98 *** (0.32) | ||||
| Pre-existing mental health problem | Yes | 2.61 *** (0.29) | 2.60 *** (0.29) | |||
| No (ref.) | ||||||
| Time*Gender | 1-Women | 0.57 ** (0.19) | ||||
| 1-Men (ref.) | ||||||
| 2-Women | −0.19 (0.19) | |||||
| 2-Men (ref.) | ||||||
| 4-Women | 0.12 (0.19) | |||||
| 4-Men (ref.) | ||||||
| 5-Women | −0.03 (0.19) | |||||
| 5-Men (ref.) | ||||||
| 6-Women | 0.08 (0.19) | |||||
| 6-Men (ref.) | ||||||
| 3-Women | ||||||
| 3-Men (ref.) | ||||||
| Error variance | ||||||
| Level-2 | 7.70 *** (0.11) | 7.41 *** (0.11) | 7.41 *** (0.11) | 7.38 *** (0.11) | 7.37 *** (0.11) | |
| Level-1 intercept | 14.71 *** (0.53) | 14.76 *** (0.53) | 13.18 *** (0.47) | 11.30 *** (0.42) | 11.30 *** (0.42) | |
| Model Fit | ||||||
| AIC | 58,344 | 58,004 | 57,849 | 57,565 | 57,556 | |
| BIC | 58,360 | 58,048 | 57,993 | 57,741 | 57,760 |
| Model 1 (Intercept Only) | Model 2 (Time) | Model 3 (Time + Background Variables) | Model 4 (Other Explanatory Variables) | ||
|---|---|---|---|---|---|
| Fixed effects | |||||
| Intercept | 4.18 *** (0.10) | 3.84 *** (0.11) | 2.15 *** (0.28) | 0.31 (0.38) | |
| Time | 1 | 0.44 *** (0.09) | 0.43 *** (0.09) | 0.38 *** (0.09) | |
| 2 | 0.10 (0.09) | 0.09 (0.09) | 0.06 (0.09) | ||
| 3 (ref.) | |||||
| 4 | 0.77 *** (0.09) | 0.77 *** (0.09) | 0.62 *** (0.09) | ||
| 5 | 0.73 *** (0.09) | 0.78 *** (0.09) | 0.68 *** (0.09) | ||
| 6 | 0.05 (0.09) | 0.11 (0.09) | 0.14 (0.09) | ||
| Gender | Man (ref.) | ||||
| Woman | 0.57 ** (0.19) | 0.49 ** (0.18) | |||
| Region | Flanders (ref.) | ||||
| Brussels | 1.18 *** (0.30) | 1.05 *** (0.28) | |||
| Walloon | 1.09 *** (0.22) | 1.06 *** (0.21) | |||
| Age | 18–29 | 1.80 ***(0.40) | 1.61 *** (0.38) | ||
| 30–49 | 1.43 *** (0.27) | 1.11 *** (0.26) | |||
| 50–64 | 0.71 *** (0.21) | 0.51 * (0.21) | |||
| 65+ (ref.) | - | - | |||
| Household type | Living alone, without children | 0.56 *** (0.21) | 0.34 (0.20) | ||
| Couple, without child(ren) (ref.) | - | - | |||
| Couple, with child(ren) | 0.00 (0.18) | −0.05 (0.18) | |||
| Living alone, with children | 0.11 (0.32) | −0.13 (0.31) | |||
| Together with parent(s), family, friends or acquaintances | 0.52 (0.34) | 0.41 (0.33) | |||
| Other | −0.39 (0.39) | −0.53 (0.38) | |||
| Work status | Paid job (ref.) | ||||
| Unemployed (not temporarily interrupted)) | 0.81 ** (0.31) | 0.72 * (0.31) | |||
| Invalidity | 1.35 *** (0.39) | 0.93 * (0.38) | |||
| Studies | −0.39 (0.58) | −0.22 (0.57) | |||
| Retirement | −0.67 *** (0.20) | −0.64 ** (0.19) | |||
| Household work | 0.68 (0.42) | 0.72 (0.40) | |||
| Other | 0.38 (0.36) | 0.40 (0.35) | |||
| Education | Secondary degree (or lower) | 0.38 * (0.18) | 0.31 (0.17) | ||
| Higher degree (ref.) | - | - | |||
| Infected/exposed to COVID-19 | Yes | 0.43 * (0.21) | |||
| No (ref.) | - | ||||
| Social support | Poor | 1.49 *** (0.11) | |||
| Moderate | 0.50 *** (0.09) | ||||
| Strong (ref.) | |||||
| Personality trait | Introvert (ref.) | - | |||
| Middle | 0.75 ** (0.27) | ||||
| Extravert | 2.71 *** (0.33) | ||||
| Pre-existing mental health problem | Yes | 2.95 *** (0.30) | |||
| No (ref.) | - | ||||
| Error variance | |||||
| Level-2 | 6.76 *** (0.10) | 6.64 *** (0.10) | 6.64 *** (0.10) | 6.59 *** (0.10) | |
| Level-1 intercept | 17.34 *** (0.61) | 17.35 *** (0.61) | 15.46 *** (0.55) | 12.79 *** (0.47) | |
| Model Fit | |||||
| AIC | 57,415 | 57,261 | 57,102 | 56,710 | |
| BIC | 57,431 | 57,306 | 57,245 | 56,886 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bruggeman, H.; Smith, P.; Berete, F.; Demarest, S.; Hermans, L.; Braekman, E.; Charafeddine, R.; Drieskens, S.; De Ridder, K.; Gisle, L. Anxiety and Depression in Belgium during the First 15 Months of the COVID-19 Pandemic: A Longitudinal Study. Behav. Sci. 2022, 12, 141. https://doi.org/10.3390/bs12050141
Bruggeman H, Smith P, Berete F, Demarest S, Hermans L, Braekman E, Charafeddine R, Drieskens S, De Ridder K, Gisle L. Anxiety and Depression in Belgium during the First 15 Months of the COVID-19 Pandemic: A Longitudinal Study. Behavioral Sciences. 2022; 12(5):141. https://doi.org/10.3390/bs12050141
Chicago/Turabian StyleBruggeman, Helena, Pierre Smith, Finaba Berete, Stefaan Demarest, Lize Hermans, Elise Braekman, Rana Charafeddine, Sabine Drieskens, Karin De Ridder, and Lydia Gisle. 2022. "Anxiety and Depression in Belgium during the First 15 Months of the COVID-19 Pandemic: A Longitudinal Study" Behavioral Sciences 12, no. 5: 141. https://doi.org/10.3390/bs12050141
APA StyleBruggeman, H., Smith, P., Berete, F., Demarest, S., Hermans, L., Braekman, E., Charafeddine, R., Drieskens, S., De Ridder, K., & Gisle, L. (2022). Anxiety and Depression in Belgium during the First 15 Months of the COVID-19 Pandemic: A Longitudinal Study. Behavioral Sciences, 12(5), 141. https://doi.org/10.3390/bs12050141