Effects of a Mindfulness and Acceptance-Based Program on Intimate Relationships in a Youth Sample: A Randomized Controlled Trial

 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Study Design
2.3. Interventions
2.4. Measures
2.5. Data Analysis
3. Results
3.1. Descriptive Parameters
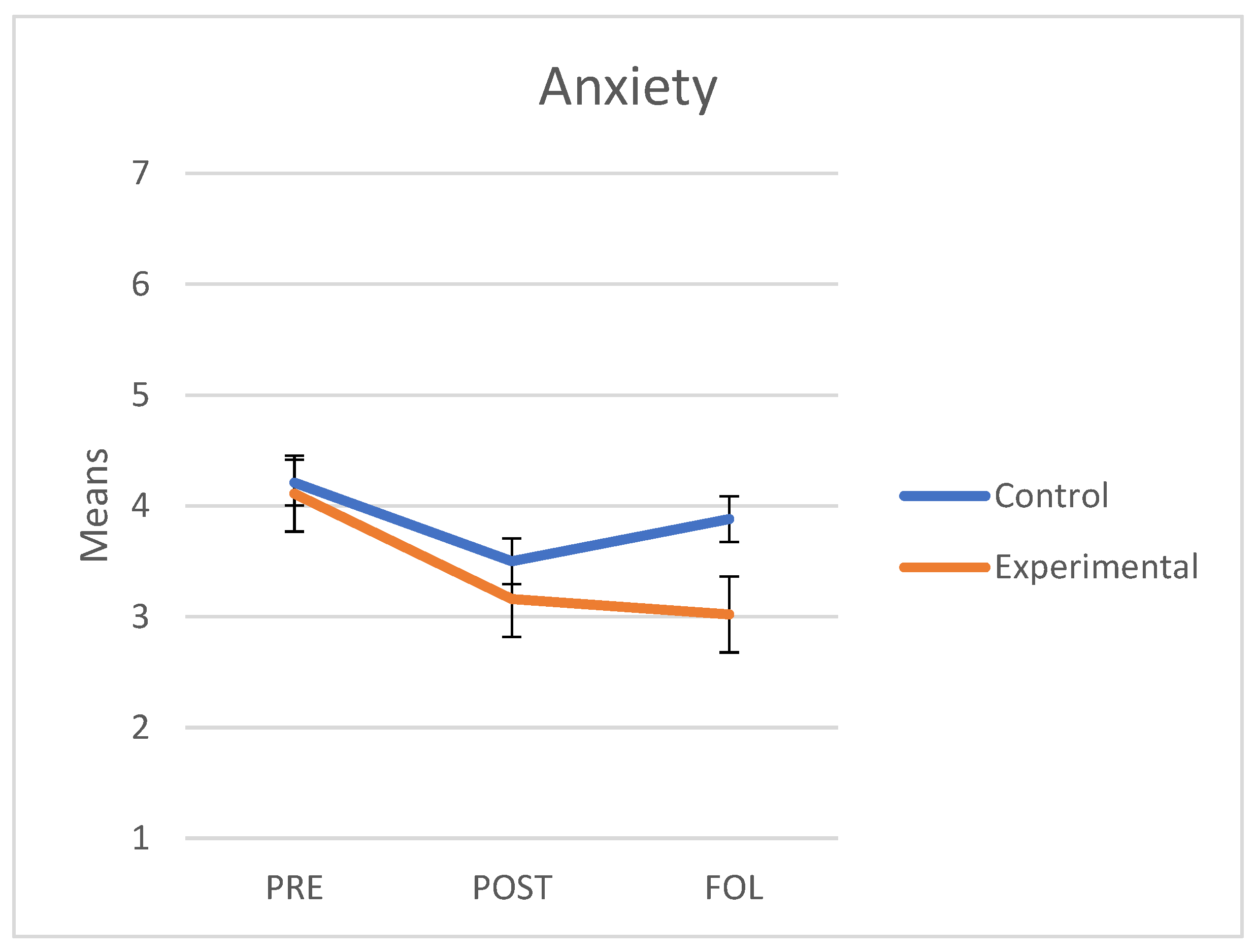
3.2. Anxiety
3.3. Avoidance
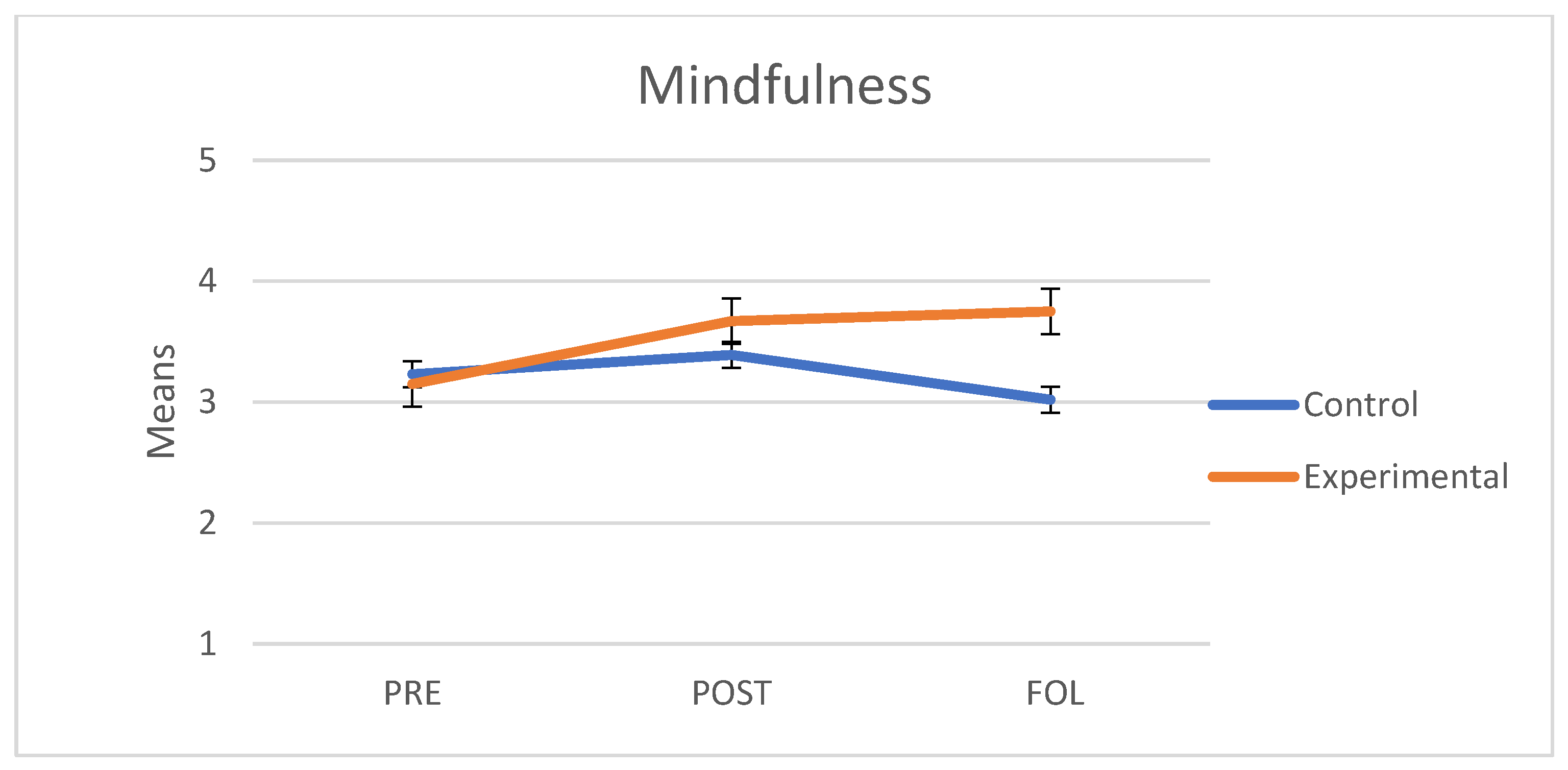
3.4. Mindfulness
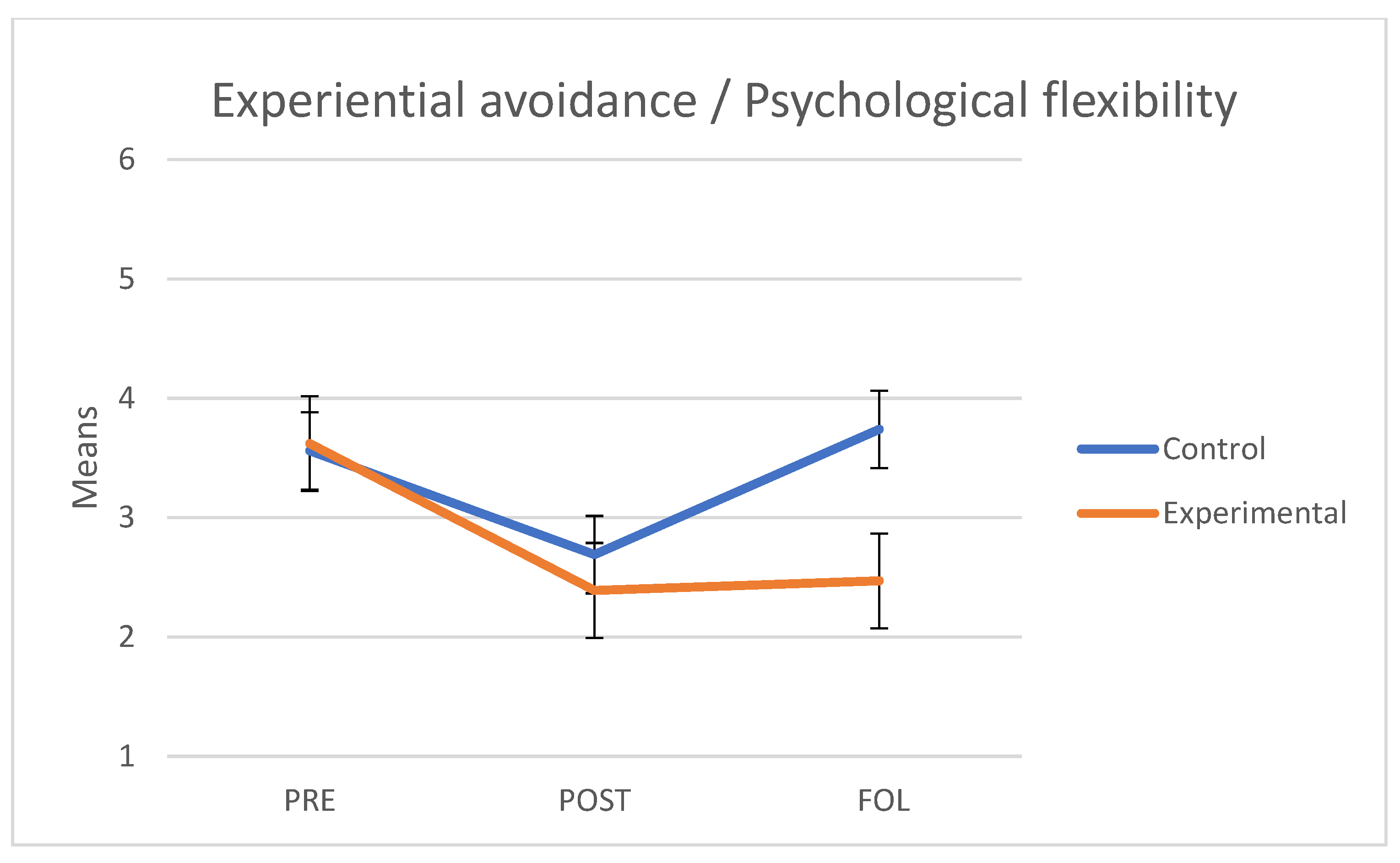
3.5. Experiential Avoidance/Psychological Flexibility
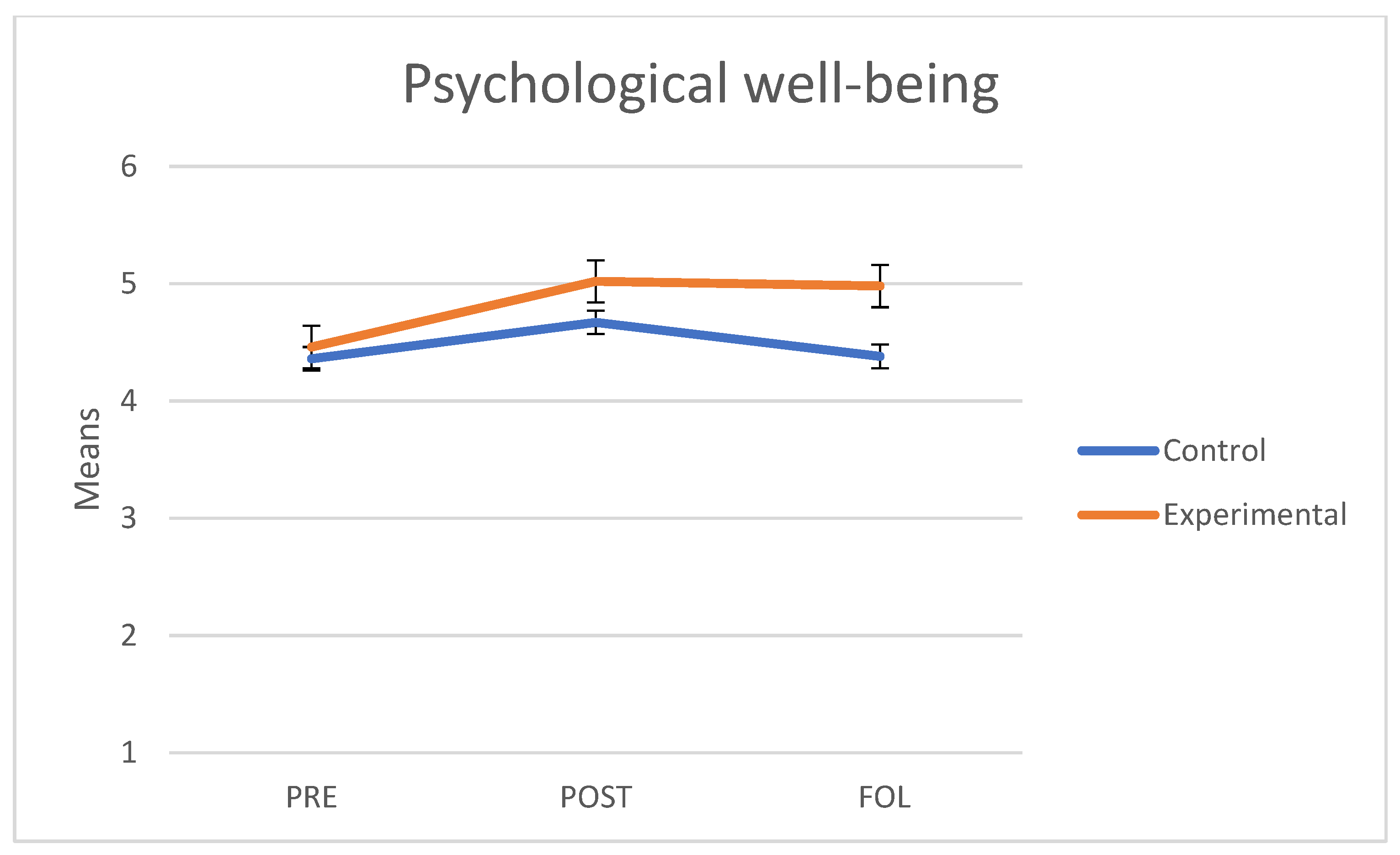
3.6. Psychological Well-Being
4. Discussion
5. Limitations
6. Future Lines of Research
7. Conclusions
8. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comparison between Program Contents | ||||
|---|---|---|---|---|
| Experimental Group | Active Control Group | |||
| Session No. | Title | Objective | Topics | |
| 1 | Well-being and mindful intimate relationships | Identify the gap that exists between idealization and the everyday reality of intimate relationships. Understand basic concepts about mindfulness, its effects and its practice. Pre-treatment assessment. | Face-to-face session 1 | Pre-treatment assessment and explanation of the procedure to follow. |
| 2 | Myths about love | Identify the myths that exist about intimate relationships. | Online psychoeducation, reflection and feedback | Text 1 for reading and reflection: Why is your brain always looking for trouble? |
| 3 | Disconnection in intimate relationships | Understand how disconnection occurs in intimate relationships. | Text 2 for reading and reflection: Empathy: how it can change your life. | |
| 4 | Managing psychological distress in intimate relationships | Acquire tools to manage psychological distress. | Text 3 for reading and reflection: Assertiveness: extending self-esteem to social relationships. A distinction is made between assertive, passive and aggressive individuals. | |
| 5 | Healing past and/or significant relationships | Identify, accept and heal the wounds from past and/or significant relationships through compassion and self-compassion. | Text 4 for reading and reflection: Anger, sadness and pain: what is going on with today’s music? | |
| 6 | Acceptance: one day of silence | Consolidate the practice of mindfulness to develop acceptance and psychological well-being through group sessions. | Text 5 for reading and reflection: Me! Me! Me! The Age of Digital Narcissism. | |
| 7 | Value-guided action | Recognize the importance of values as a guide to action in life and intimate relationships. | Text 6 for reading and reflection: Loneliness is not being alone, but being empty, according to Seneca. | |
| 8 | Full life and mindful intimate relationships | Design a plan to continue developing mindfulness, generate personal well-being and cultivate intimate relationships. Post-treatment assessment. | Face-to-face session 2 | Post-treatment assessment. |
| Reminder of the follow-up assessment (experimental group) | Sending of reading materials. | Reminder of the follow-up assessment (active control group) | Sending of animated short films on relationships: This is the Plan The Spider and The Butterfly | |
Appendix B
| Title: | Well-Being and Mindful Intimate Relationships | ||
|---|---|---|---|
| Objectives: |
| ||
| Activities | Process | Resources | Time |
| Establishing a framework for the session. | Greetings and welcome. Record of attendance, email address and telephone number. Hand over the printed material and a folder. Set group rules. Individual presentation and expectations of participants. Explanation of how the sessions are conducted. | Presentation of the work space. Rules. Attendance record. Folders and printed sheets. | 20′ |
| Defining a baseline. | Application of tests or instruments, first measurement. | Record of sociodemographic data. Informed consent to participate in the program. Printed sheets with the instruments. | 30′ |
| Psychoeducation: Complexity in intimate relationships. | Build a group space. Create three groups. Distribute the puzzles. Instructions: “Put the puzzle together” After finishing the assignment, reflect upon the activity and its similarity with intimate relationships. | Puzzle Slate Markers | 30′ |
| Introduction to the program. | Think about the Fly meditation video. Presentation of basic concepts about mindfulness and its effects. Stages of stress: stimulus, resistance, exhaustion, wear in the intimate relationship. Build a space of freedom of choice instead of reaction: the triangle of attention and the basics of practice. | The Fly meditation video. https://www.youtube.com/watch?v=t7xqGvtHxew (accessed on 16 September 2019) Power point presentation. | 20′ |
| Breath-focused meditation. | Mindfulness exercise: feeling and breathing. | Audio recording, script, instructions for practice. | 15′ |
| Explanation of the exercises for the week. | Formal practice: Breath-focused meditation (audio recording) for 15 min. Informal practice: Place 5 color tags in five places you often visit in your everyday life, stop and take 3 mindful breaths feeling how your stomach expands and contracts. Mindfulness: Moments of waiting: observing thoughts, emotions and feelings. | Sheet. Audio recording for breathing. Color tags. | 5′ |
| Closure: | In few words: What am I taking home from this workshop? Assessment of well-being from 1 to 10. Create WhatsApp group for notifications and follow-up of practice. Materials for next session: Bring an extra pair socks. | Briefcase. | 10′ |
References
- World Health Organization; Pan American Health Organization. Understanding and Addressing Violence against Women: Intimate Partner Violence; World Health Organization: Geneva, Switzerland, 2012; pp. 491–498. Available online: http://apps.who.int/iris/bitstream/10665/77434/1/WHO_RHR_12.37_eng.pdf (accessed on 15 March 2021).
- Di Napoli, I.; Procentese, F.; Carnevale, S.C.; Esposito, C.; Arcidiacono, C. Ending intimate partner violence (Ipv) and locating men at stake: An ecological approach. Int. J. Environ. Res. Public Health 2019, 16, 1652. [Google Scholar] [CrossRef]
- Shulman, S.; Connolly, J. The Challenge of Romantic Relationships in Emerging Adulthood: Reconceptualization of the Field. Emerg. Adulthood 2013, 1, 27–39. [Google Scholar] [CrossRef]
- Gómez-López, M.; Viejo, C.; Ortega-Ruiz, R. Well-being and romantic relationships: A systematic review in adolescence and emerging adulthood. Int. J. Environ. Res. Public Health 2019, 16, 2415. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, V.; Ortega-Rivera, J.; Ortega-Ruiz, R.; Viejo, C. Las relaciones sentimentales en la adolescencia: Satisfacción, conflictos y violencia [Romantic relationships in adolescence: Satisfaction, conflicts and dating violence]. Escri. Psicol. 2008, 2, 97–109. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=2878095&info=resumen&idioma=SPA (accessed on 15 March 2021).
- Arnett, J.; Žukauskiene, R.; Sugimura, K. The new life stage of emerging adulthood at ages 18-29 years: Implications for mental health. Lancet Psychiatry 2014, 1, 569–576. [Google Scholar] [CrossRef]
- Rojas-Solís, J.; Flores-Elvira, A. El Noviazgo y otros Vínculos Afectivos de la Juventud Mexicana en una Sociedad con Características Postmodernas [Courtship and other affective bonds of Mexican youth in a society with post-modern traits]. Uaricha Rev. Psicol. 2013, 10, 120–139. Available online: https://www.aacademica.org/dr.jose.luis.rojas.solis/13 (accessed on 15 March 2021).
- Rivera, D.; Cruz, C.; Muñoz, C. Satisfacción en las relaciones de pareja en la adultez emergente: El rol del apego, la intimidad y la depresión [Satisfaction in intimate relationships during emerging adulthood: The role of attachment, intimacy and depression]. Ter. Psicol. 2011, 29, 77–83. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Fermani, A.; Bongelli, R.; Carrieri, A.; Del Moral Arroyo, G.; Muzi, M.; Portelli, C. What is more important than love? Parental attachment and romantic relationship in Italian emerging adulthood. Cogent Psychol. 2019, 6, 1–20. [Google Scholar] [CrossRef]
- Fermani, A.; Bongelli, R.; Canestrari, C.; Muzi, M.; Riccioni, I.; Burro, R. Old Wine in a New Bottle. Depression and Romantic Relationships in Italian Emerging Adulthood: The Moderating Effect of Gender. Int. J. Environ. Res. Public Health 2020, 17, 4121. [Google Scholar] [CrossRef] [PubMed]
- Fumero, A.; Peñate, W.; Oyanadel, C.; Porter, B. The Effectiveness of Mindfulness-Based Interventions on Anxiety Disorders. A Systematic Meta-Review. Investig. Health Psychol. Educ. 2020, 10, 704–719. [Google Scholar] [CrossRef]
- González-García, M.; González, J. Bases neurofisiológicas de mindfulness y compasión: Una propuesta desde la teoría polivagal. Mindfulness Compassion 2017, 2, 101–111. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Dell Publishing: New York, NY, USA, 1990. [Google Scholar]
- Segal, Z.; Williams, J.M.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; The Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Gilbert, P.; Procter, S. Compassionate Mind Training for People with High Shame and Self-Criticism: Overview and Pilot Study of a Group Therapy Approach. Clin. Psychol. Psychother. 2006, 13, 353–379. [Google Scholar] [CrossRef]
- Neff, K.D.; Germer, C.K. A Pilot Study and Randomized Controlled Trial of the Mindful Self-Compassion Program. J. Clin. Psychol. 2013, 69, 28–44. [Google Scholar] [CrossRef] [PubMed]
- Claxton, S.E.; Van Dulmen, M.H.M. Casual Sexual Relationships and Experiences in Emerging Adulthood. Emerg. Adulthood 2013, 1, 138–150. [Google Scholar] [CrossRef]
- Quinn-Nilas, C. Self-Reported Trait Mindfulness and Couples’ Relationship Satisfaction: A Meta-Analysis. Mindfulness 2020, 11, 835–848. [Google Scholar] [CrossRef]
- Karremans, J.C.; Schellekens, M.P.J.; Kappen, G. Bridging the Sciences of Mindfulness and Romantic Relationships: A Theoretical Model and Research Agenda. Pers. Soc. Psychol. Rev. 2017, 21, 29–49. [Google Scholar] [CrossRef]
- Simón, V. El Reencuentro Científico con la Compasión. Mindfulness y Ciencia [The Scientific Re-encounter with Compassion. Mindfulness and Science]; Alianza Editorial: Madrid, Spain, 2014. [Google Scholar]
- Carson, J.; Carson, K.; Gil, K.; Baucom, D. Mindfulness-based relationship enhancement. Behav. Ther. 2004, 35, 471–494. [Google Scholar] [CrossRef]
- Kramer, G.; Meleo-Meyer, F.; Turner, M. Cultivating Mindfulness in Relationship. Insight Dialogue and the Interpersonal Mindfulness Program. In Mindfulness and the Therapeutic Relationship; Hick, S.F., Bien, T., Eds.; Guilford Press: New York, NY, USA, 2012; pp. 195–214. [Google Scholar]
- Karremans, J.C.; Kappen, G.; Schellekens, M.; Schoebi, D. Comparing the effects of a mindfulness versus relaxation intervention on romantic relationship wellbeing. Sci. Rep. 2020, 10, 21696. [Google Scholar] [CrossRef]
- Gehart, D.R. Mindfulness and Acceptance in Couple and Family Therapy; Guilford: New York, NY, USA, 2012; p. 247. [Google Scholar]
- Crane, R.S.; Brewer, J.; Feldman, C.; Kabat-Zinn, J.; Santorelli, S.; Williams, J.M.G.; Kuyken, W. What defines mindfulness-based programs? the warp and the weft. Psychol. Med. 2017, 47, 990–999. [Google Scholar] [CrossRef]
- Nekic, M.; Mamic, S. Intolerance of Uncertainty and Mindfulness as Determinants of Anxiety and Depression in Female Students. Behav. Sci. 2019, 9, 135. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pr. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Nanda, J. Mindful relationships. Sex. Relatsh. Ther. 2013, 28, 120–131. [Google Scholar] [CrossRef]
- Kappen, G.; Karremans, J.C.; Burk, W.J.; Buyukcan-Tetik, A. On the Association Between Mindfulness and Romantic Relationship Satisfaction: The Role of Partner Acceptance. Mindfulness 2018, 9, 1543–1556. [Google Scholar] [CrossRef] [PubMed]
- Centeno, R.; Fernandez, K. Effect of Mindfulness on Empathy and Self-Compassion: An Adapted MBCT Program on Filipino College Students. Behav. Sci. 2020, 10, 61. [Google Scholar] [CrossRef]
- Stahl, B.; Goldstein, E. Mindfulness Para Reducir el Estrés. Una guía práctica [Mindfulness to Reduce Stress. A Practical Guide]; Editorial Kairós: Barcelona, Spain, 2010. [Google Scholar]
- Neff, K.D. The development and validation of a scale to measure self-compassion. Self Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]
- Martínez, E.; Pacheco, M. El incremento de mindfulness con el ejercicio de la psicoterapia [The increase of mindfulness with the practice of psychotherapy]. Acción Psicol. 2012, 9, 6. [Google Scholar] [CrossRef]
- Hayes, S.C.; Pistorello, J.; Levin, M.E. Acceptance and Commitment Therapy as a Unified Model of Behavior Change. Couns. Psychol. 2012, 40, 976–1002. [Google Scholar] [CrossRef]
- Hayes, S.C. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav. Ther. 2004, 35, 639–665. [Google Scholar] [CrossRef]
- Stabbe, O.K.; Rolffs, J.L.; Rogge, R.D. Flexibly and/or inflexibly embracing life: Identifying fundamental approaches to life with latent profile analyses on the dimensions of the Hexaflex model. J. Context. Behav. Sci. 2019, 12, 106–118. [Google Scholar] [CrossRef]
- Daks, J.S.; Rogge, R.D. Examining the correlates of psychological flexibility in romantic relationship and family dynamics: A meta-analysis. J. Contextual Behav. Sci. 2020, 18, 214–238. [Google Scholar] [CrossRef]
- Gaspar, R.M. Terapia de aceptación y compromiso aplicada a los problemas de pareja [Acceptance and Commitment Therapy applied to intimate relationship problems]. In Múltiples aplicaciones de la Terapia de Aceptación y Compromiso (ACT); Pirámide: Madrid, Spain, 2012; pp. 203–217. [Google Scholar]
- Hayes, S.; Strosahl, K.; Wilson, K. Terapia de Aceptación y Compromiso. Proceso y práctica del Cambio Consciente (Mindfulness) [Acceptance and Commitment Therapy. The Process and Practice of Conscious Change (Mindfulness)]; Editorial Desclée De Brouwer: Bilbao, Spain, 2014. [Google Scholar]
- Moradzadeh, F.; Pirkhaefi, A. The Effectiveness of Acceptance and Commitment Therapy on Marital Satisfaction and Cognitive Flexibility among Married Employees of the Welfare Office. Iran. J. Psychiatr. Nurs. 2018, 5, 1–7. [Google Scholar] [CrossRef][Green Version]
- Patrón-Espinosa, F. La evitación experiencial como dimensión funcional de los trastornos de depresión, ansiedad y psicóticos [Experiential avoidance as a functional dimension of depression, anxiety and psychotic disorders]. J. Health Soc. Behav. 2013, 5, 85–95. [Google Scholar] [CrossRef]
- Araya-Véliz, C.; Porter, B. Habilidades del terapeuta y mindfulness [Therapeutic Skills and Mindfulness]. Rev. Argent. Clin. Psicol. 2017, 26, 232–240. [Google Scholar] [CrossRef][Green Version]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.; Vinet, E.V. Atención Plena: Validación del Five Facet Mindfulness Questionnaire (FFMQ) en estudiantes Universitarios Chilenos [Validation of the Five Facet Mindfulness Questionnaire (FFMQ) in Chilean college students]. Ter. Psicol. 2015, 33, 93–102. [Google Scholar] [CrossRef]
- Brennan, K.; Clark, C.; Shaver, P. Self-report measurement of adult attachment: An integrative overview. In Attachment Theory and Close Relationships; Simpson, J.A., Rholes, W.S., Eds.; Guilford Press: New York, NY, USA, 1998; pp. 46–76. [Google Scholar]
- Ryff, C.D. Happiness Is Everything, or Is It? Explorations on the Meaning of Psychological Well-Being. J. Pers. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Van Dierendonck, D. The construct validity of Ryff’s Scales of Psychological Well-being and its extension with spiritual well-being. Pers. Individ. Differ. 2005, 36, 629–643. [Google Scholar] [CrossRef]
- Díaz, D.; Rodríguez-Carvajal, R.; Blanco, A.; Moreno-Jiménez, B.; Gallardo, I.; Valle, C.; Van Dierendonck, D. Adaptación española de las escalas de bienestar psicológico de Ryff [Spanish adaptation of the Psychological Weil-Being Scales (PWBS)]. Psicothema 2006, 18, 572–577. Available online: https://reunido.uniovi.es/index.php/PST/article/view/8474 (accessed on 15 March 2021).
- Hayes, S.C.; Strosahl, K.; Wilson, K.G.; Bissett, R.T.; Pistorello, J.; Toarmino, D.; Polusny, M.A.; Dykstra, T.A.; Batten, S.V.; Bergan, J.; et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol. Rec. 2004, 54, 553–578. [Google Scholar] [CrossRef]
- Arias, P.; Barraca, J.; García, F. Evitación Experiencial: Adaptación del Cuestionario de Aceptación y Acción-II en Población Ecuatoriana [Adaptation of the Acceptance and Action Questionnaire-II to the Ecuadorian population]. Psicol. Conduct. under review.
- Kappen, G.; Karremans, J.C.; Burk, W.J. Effects of a Short Online Mindfulness Intervention on Relationship Satisfaction and Partner Acceptance: The Moderating Role of Trait Mindfulness. Mindfulness 2019, 10, 2186–2199. [Google Scholar] [CrossRef]
- Tan, L.B.G.; Martin, G. Mind full or mindful: A report on mindfulness and psychological health in healthy adolescents. J. Youth Adolesc. 2016, 21, 64–74. [Google Scholar] [CrossRef]
- Prozzillo, P.; Olivera, M. Flexibilidad psicológica y bienestar subjetivo en el marco de los cinco factores de la personalidad y la espiritualidad: Una relación por definir [Psychological flexibility and subjective well-being in the framework of the five factors of personality and spirituality: A relationship not yet defined]. Psocial 2019, 5, 17–25. [Google Scholar]
- Galán, A. La teoría del apego: Confusiones, delimitaciones conceptuales y desafío [Attachment theory: Confusions, conceptual delimitations and challenges]. Rev. Asoc. Esp. Neuropsiq. 2016, 36, 45–61. [Google Scholar]
- Medvedev, O.N.; Pratscher, S.D.; Bettencourt, A. Psychometric Evaluation of the Interpersonal Mindfulness Scale Using Rasch Analysis. Mindfulness 2020, 11, 2007–2015. [Google Scholar] [CrossRef]
- Romero, R.; Penas, R.; García-Conde, A.; Llombart, P.; Pérez, S.; Marco, J.H. Mindfulness-Based Cognitive Therapy for Spanish Oncology Patients: The Bartley Protocol. Psicothema 2020, 32, 508–515. [Google Scholar] [PubMed]





| PRE | POST | Follow-Up | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Groups | EG | CG | EG | CG | EG | CG | ||||||
| Variables | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD |
| Well-being | 4.46 | 0.64 | 4.36 | 0.65 | 5.02 | 0.7 | 4.67 | 0.67 | 4.98 | 0.65 | 4.38 | 0.77 |
| Psychological flexibility | 3.62 | 1.16 | 3.56 | 1.28 | 2.39 | 0.96 | 2.69 | 1.01 | 2.47 | 0.9 | 3.74 | 1.24 |
| Mindfulness | 3.15 | 0.33 | 3.23 | 0.4 | 3.67 | 0.53 | 3.39 | 0.55 | 3.75 | 0.55 | 3.02 | 0.64 |
| Anxiety | 4.11 | 1.29 | 4.21 | 0.99 | 3.16 | 1.25 | 3.5 | 1.2 | 3.02 | 1.16 | 3.88 | 1.04 |
| Avoidance | 2.68 | 1.04 | 3.41 | 0.84 | 2.23 | 0.85 | 2.94 | 0.71 | 2.08 | 0.71 | 2.97 | 0.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosales-Villacrés, M.d.L.; Oyanadel, C.; Changotasig-Loja, D.; Peñate-Castro, W. Effects of a Mindfulness and Acceptance-Based Program on Intimate Relationships in a Youth Sample: A Randomized Controlled Trial. Behav. Sci. 2021, 11, 84. https://doi.org/10.3390/bs11060084
Rosales-Villacrés MdL, Oyanadel C, Changotasig-Loja D, Peñate-Castro W. Effects of a Mindfulness and Acceptance-Based Program on Intimate Relationships in a Youth Sample: A Randomized Controlled Trial. Behavioral Sciences. 2021; 11(6):84. https://doi.org/10.3390/bs11060084
Chicago/Turabian StyleRosales-Villacrés, María de Lourdes, Cristián Oyanadel, Diana Changotasig-Loja, and Wenceslao Peñate-Castro. 2021. "Effects of a Mindfulness and Acceptance-Based Program on Intimate Relationships in a Youth Sample: A Randomized Controlled Trial" Behavioral Sciences 11, no. 6: 84. https://doi.org/10.3390/bs11060084
APA StyleRosales-Villacrés, M. d. L., Oyanadel, C., Changotasig-Loja, D., & Peñate-Castro, W. (2021). Effects of a Mindfulness and Acceptance-Based Program on Intimate Relationships in a Youth Sample: A Randomized Controlled Trial. Behavioral Sciences, 11(6), 84. https://doi.org/10.3390/bs11060084