
Relationships among Early Adversity, Positive Human and Animal Interactions, and Mental Health in Young Adults



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.3. Statistical Analyses
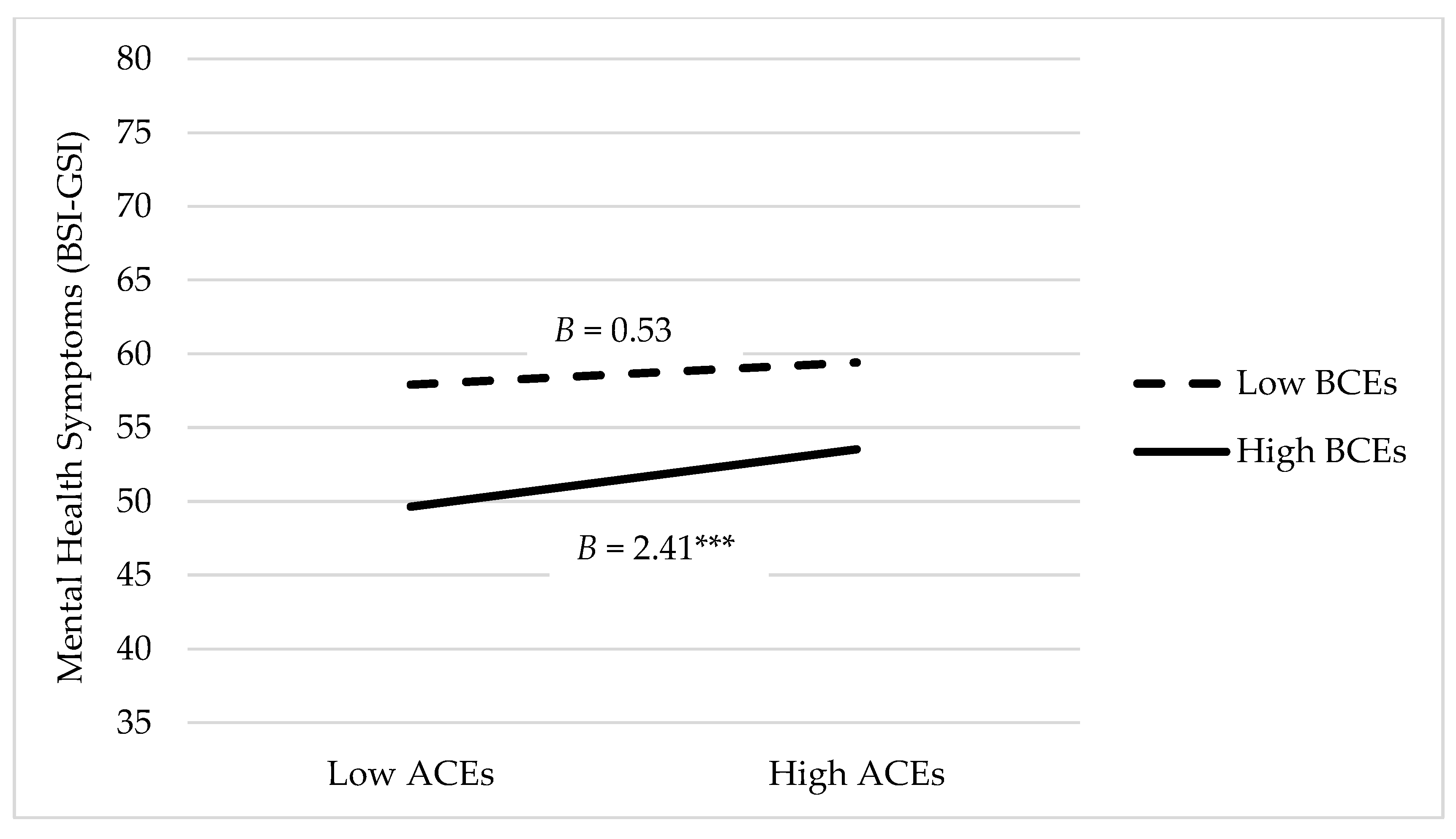
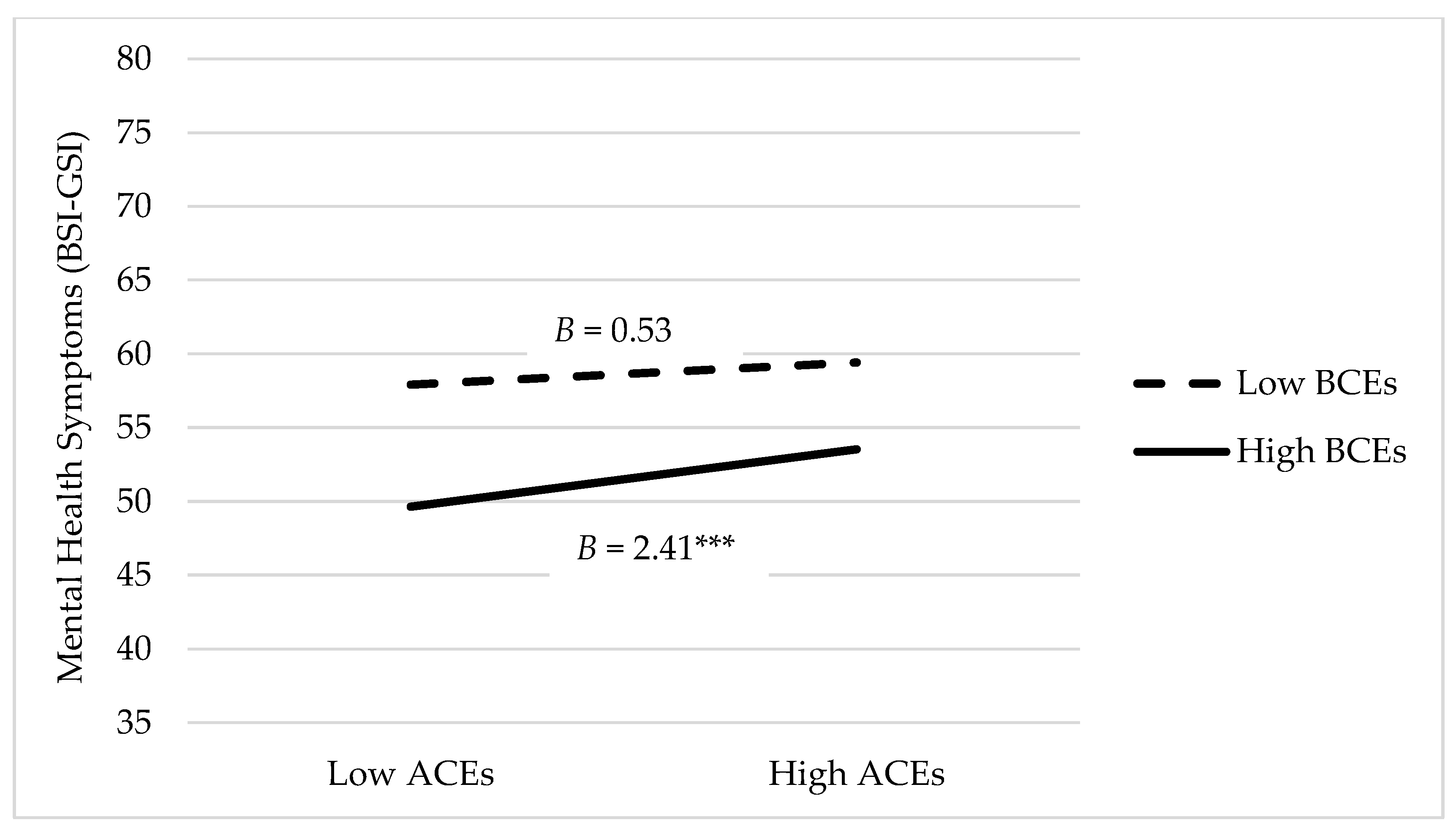
3. Results
4. Discussion
Limitations
5. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Merrick, M.T.; Ford, D.C.; Ports, K.A.; Guinn, A.S. Prevalence of adverse childhood experiences from the 2011–2014 behavioral risk factor surveillance system in 23 states. JAMA Pediatrics 2018, 172, 1038–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anda, R.F.; Felitti, V.J.; Bremner, J.D.; Walker, J.D.; Whitfield, C.; Perry, B.D.; Dube, S.R.; Giles, W.H. The enduring effects of abuse and related adverse experiences in childhood. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef]
- Brown, S.M.; Rienks, S.; McCrae, J.S.; Watamura, S.E. The co-occurrence of adverse childhood experiences among children investigated for child maltreatment: A latent class analysis. Child Abus. Negl. 2019, 87, 18–27. [Google Scholar] [CrossRef]
- Cronholm, P.F.; Forke, C.M.; Wade, R.; Bair-Merritt, M.H.; Davis, M.; Harkins-Schwarz, M.; Pachter, L.M.; Fein, J.A. Adverse childhood experiences: Expanding the concept of adversity. Am. J. Prev. Med. 2015, 49, 354–361. [Google Scholar] [CrossRef]
- Petruccelli, K.; Davis, J.; Berman, T. Adverse childhood experiences and associated health outcomes: A systematic review and meta-analysis. Child Abus. Negl. 2019, 97, 104127. [Google Scholar] [CrossRef]
- Moore, K.A.; Ramirez, A.N. Adverse childhood experience and adolescent well-being: Do protective factors matter? Child Indic. Res. 2016, 9, 299–316. [Google Scholar] [CrossRef]
- McLaughlin, K.A. Future directions in childhood adversity and youth psychopathology. J. Clin. Child Adolesc. Psychol. 2016, 45, 361–382. [Google Scholar] [CrossRef] [PubMed]
- Narayan, A.J.; Rivera, L.M.; Bernstein, R.E.; Harris, W.W.; Lieberman, A.F. Positive childhood experiences predict less psychopathology and stress in pregnant women with childhood adversity: A pilot study of the benevolent childhood experiences (BCEs) scale. Child Abus. Negl. 2018, 78, 19–30. [Google Scholar] [CrossRef]
- Crandall, A.; Miller, J.R.; Cheung, A.; Novilla, L.K.; Glade, R.; Novilla, M.L.B.; Magnusson, B.M.; Leavitt, B.L.; Barnes, M.D.; Hanson, C.L. ACEs and counter-ACEs: How positive and negative childhood experiences influence adult health. Child Abus. Negl. 2019, 96, 104089. [Google Scholar] [CrossRef]
- Bethell, C.; Jones, J.; Gombojav, N.; Linkenbach, J.; Sege, R. Positive childhood experiences and adult mental and relational health in a statewide sample: Associations across adverse childhood experiences levels. JAMA Pediatrics 2019, 173, e193007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crandall, A.; Broadbent, E.; Stanfill, M.; Magnusson, B.M.; Novilla, M.L.B.; Hanson, C.L.; Barnes, M.D. The influence of adverse and advantageous childhood experiences during adolescence on young adult health. Child Abus. Negl. 2020, 108, 104644. [Google Scholar] [CrossRef]
- Gartland, D.; Riggs, E.; Muyeen, S.; Giallo, R.; Afifi, T.O.; MacMillan, H.; Herrman, H.; Bulford, E.; Brown, S.J. What factors are associated with resilient outcomes in children exposed to social adversity? A systematic review. BMJ Open 2019, 9, e024870. [Google Scholar] [CrossRef] [Green Version]
- Melkman, E.P. Childhood adversity, social support networks and well-being among youth aging out of care: An exploratory study of mediation. Child Abus. Negl. 2017, 72, 85–97. [Google Scholar] [CrossRef]
- Zilcha-Mano, S.; Mikulincer, M.; Shaver, P.R. Pets as safe havens and secure bases: The moderating role of pet attachment orientations. J. Res. Personal. 2012, 46, 571–580. [Google Scholar] [CrossRef]
- Melson, G.F.; Schwarz, R.L.; Beck, A.M. Importance of companion animals in children’s lives: Implications for veterinary practice. J. Am. Vet. Med Assoc. 1997, 211, 1512–1518. [Google Scholar]
- Beetz, A.; Julius, H.; Turner, D.; Kotrschal, K. Effects of social support by a dog on stress modulation in male children with insecure attachment. Front. Psychol. 2012, 3, 352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purewal, R.; Christley, R.; Kordas, K.; Joinson, C.; Meints, K.; Gee, N.; Westgarth, C. Companion animals and child/adolescent development: A systematic review of the evidence. Int. J. Environ. Res. Public Health 2017, 14, 234. [Google Scholar] [CrossRef]
- Bodsworth, W.; Coleman, G. Child–companion animal attachment bonds in single and two-parent families. Anthrozoös 2001, 14, 216–223. [Google Scholar] [CrossRef]
- Westgarth, C.; Boddy, L.M.; Stratton, G.; German, A.J.; Gaskell, R.M.; Coyne, K.P.; Bundred, P.; McCune, S.; Dawson, S. Pet ownership, dog types and attachment to pets in 9–10 year old children in Liverpool, UK. BMC Vet. Res. 2013, 9, 102. [Google Scholar] [CrossRef] [Green Version]
- Carr, S.; Rockett, B. Fostering secure attachment: Experiences of animal companions in the foster home. Attach. Hum. Dev. 2017, 19, 259–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strand, E.B. Interparental conflict and youth maladjustment: The buffering effects of pets. Stress Trauma Crisis 2004, 7, 151–168. [Google Scholar] [CrossRef]
- Applebaum, J.W.; Zsembik, B.A. Pet Attachment in the Context of Family Conflict. Anthrozoös 2020, 33, 361–370. [Google Scholar] [CrossRef]
- Barlow, M.R.; Hutchinson, C.A.; Newton, K.; Grover, T.; Ward, L. Childhood neglect, attachment to companion animals, and stuffed animals as attachment objects in women and men. Anthrozoös 2012, 25, 111–119. [Google Scholar] [CrossRef]
- Hawkins, R.D.; McDonald, S.E.; O’Connor, K.; Matijczak, A.; Ascione, F.R.; Williams, J.H. Exposure to intimate partner violence and internalizing symptoms: The moderating effects of positive relationships with pets and animal cruelty exposure. Child Abus. Negl. 2019, 98, 104166. [Google Scholar] [CrossRef]
- McDonald, S.E.; O’Connor, K.; Matijczak, A.; Murphy, J.; Applebaum, J.W.; Tomlinson, C.A.; Wike, T.L.; Kattari, S.K. Victimization and psychological wellbeing among sexual and gender minority emerging adults: Testing the moderating role of emotional comfort from companion animals. J. Soc. Soc. Work Res. 2021. [CrossRef]
- Kerns, K.A.; Stuart-Parrigon, K.L.; Coifman, K.G.; van Dulmen, M.H.; Koehn, A. Pet Dogs: Does their presence influence preadolescents’ emotional responses to a social stressor? Soc. Dev. 2018, 27, 34–44. [Google Scholar] [CrossRef]
- Kertes, D.A.; Liu, J.; Hall, N.J.; Hadad, N.A.; Wynne, C.D.; Bhatt, S.S. Effect of pet dogs on children’s perceived stress and cortisol stress response. Soc. Dev. 2017, 26, 382–401. [Google Scholar] [CrossRef]
- Karatekin, C.; Ahluwalia, R. Effects of adverse childhood experiences, stress, and social support on the health of college students. J. Interpers. Violence 2020, 35, 150–172. [Google Scholar] [CrossRef]
- Blum, R.W.; Li, M.; Naranjo-Rivera, G. Measuring adverse child experiences among young adolescents globally: Relationships with depressive symptoms and violence perpetration. J. Adolesc. Health 2019, 65, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Kim, Y.; Terry, J. Adverse childhood experiences (ACEs) on mental disorders in young adulthood: Latent classes and community violence exposure. Prev. Med. 2020, 134, 106039. [Google Scholar] [CrossRef]
- Boulet, J.; Boss, M.W. Reliability and validity of the Brief Symptom Inventory. Psychol. Assess. J. Consult. Clin. Psychol. 1991, 3, 433. [Google Scholar] [CrossRef]
- Drobnjak, S. Brief Symptom Inventory. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 269–270. [Google Scholar]
- McDonald, S.E.; Vidacovich, C.; Ascione, F.R.; Williams, J.H.; Green, K.E. The children’s treatment of animals questionnaire: A rasch analysis. Anthrozoos 2015, 28, 131–144. [Google Scholar] [CrossRef]
- Dwyer, F.; Bennett, P.C.; Coleman, G.J. Development of the Monash dog owner relationship scale (MDORS). Anthrozoös 2006, 19, 243–256. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makriyianis, H.M.; Adams, E.A.; Lozano, L.L.; Mooney, T.A.; Morton, C.; Liss, M. Psycholoical inflexibility mediates the relationship between adverse childhood experiences and mental health outcomes. J. Contextual Behav. Sci. 2019, 14, 82–89. [Google Scholar] [CrossRef]
- Cohrdes, C.; Mauz, E. Self-Efficacy and emotional stability buffer negative effects of adverse childhood experiences on young adult health-related quality of life. J. Adolesc. Health 2020, 67, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, M.A.; McLaughlin, K.A. Dimensions of early experience and neural development: Deprivation and threat. Trends Cogn. Sci. 2014, 18, 580–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schilling, E.A.; Aseltine, R.H.; Gore, S. The impact of cumulative childhood adversity on young adult mental health: Measures, models, and interpretations. Soc. Sci. Med 2008, 66, 1140–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, K.A.; Sheridan, M.A. Beyond cumulative risk: A dimensional approach to childhood adversity. Curr. Dir Psychol. Sci. 2016, 25, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPhedran, S. Animal abuse, family violence, and child wellbeing: A review. J. Fam. Violence 2009, 24, 41–52. [Google Scholar] [CrossRef]
- Haden, S.; McDonald, S.E.; Murphy, J. Violence against family pets. In SAGE Handbook of Domestic Violence; Shackelford, T., Ed.; SAGE Publications: Los Angeles, CA, USA, 2020. [Google Scholar]
- Murphy, J.L.; Voorhees, E.V.; O’Connor, K.E.; Tomlinson, C.A.; Matijczak, A.; Applebaum, J.W.; Ascione, F.R.; Williams, J.H.; McDonald, S.E. Positive engagement with pets buffers the impact of intimate partner violence on callous-unemotional traits in children. J. Interpers. Violence 2021. [CrossRef] [PubMed]
- Pendry, P.; Vandagriff, J.L. Salivary Studies of the Social Neuroscience of Human–Animal Interaction. In Salivary Bioscience; Springer: Berlin/Heidelberg, Germany, 2020; pp. 555–581. [Google Scholar]
- McDonald, S.E.; Tomlinson, C.A.; Applebaum, J.W.; Moyer, S.W.; Brown, S.M.; Carter, S.; Kinser, P.A. Human–Animal Interaction and Perinatal Mental Health: A Narrative Review of Selected Literature and Call for Research. Int. J. Environ. Res. Public Health 2021, 18, 10114. [Google Scholar] [CrossRef]
- Carter, C.S.; Porges, S.W. Neural mechanisms underlying human-animal interaction: An evolutionary perspective. In The Social Neuroscience of Human-Animal Interaction; Freund, L.S., McCune, S., Esposito, L., Gee, N.R., McCardle, P., Eds.; American Psychological Association: Washington, DC, USA, 2016; pp. 89–105. [Google Scholar]
- Tomlinson, C.A.; Murphy, J.L.; Williams, J.M.; Hawkins, R.D.; Matijczak, A.; Applebaum, J.W.; McDonald, S.E. Testing the moderating role of victimization and microaggressions on the relationship between human-animal interaction and psychological adjustment among LGBTQ+ emerging adults. Hum.-Anim. Interact. Bull. 2021, 11, 16–39. [Google Scholar]
- Susser, E.; Widom, C.S. Still searching for lost truths about the bitter sorrows of childhood. Schizophr. Bull. 2012, 38, 672–675. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| M (SD) or N (%) | |
|---|---|
| Age (in years) | 19.88 (2.59) |
| Relationship Status | |
| Single, never married | 197 (92.06%) |
| Married or domestic partnership | 15 (7.00%) |
| Divorced | 1 (0.47%) |
| Prefer not to answer | 1 (0.47%) |
| Gender Identity | |
| Female | 170 (79.44%) |
| Male | 37 (17.29%) |
| Other or self-identified | 4 (1.87%) |
| Non-binary | 3 (1.40%) |
| Prefer not to answer | 0 (0.00%) |
| Ethnicity | |
| Not of Hispanic origin | 172 (80.37%) |
| Hispanic origin | 35 (16.36%) |
| Prefer not to answer | 7 (3.27%) |
| Race | |
| White | 171 (79.91%) |
| Multiple races | 17 (7.95%) |
| Asian | 10 (4.67%) |
| Black or African American | 6 (2.80%) |
| Native Hawaiian or Pacific Islander | 2 (0.93%) |
| American Indian or Alaska Native | 1 (0.47%) |
| Prefer not to answer | 7 (3.27%) |
| Education Status | |
| First-year student | 121 (56.54%) |
| Second-year student | 49 (22.90%) |
| Third-year student | 28 (13.08%) |
| Fourth-year student | 13 (6.08%) |
| Fifth-year or more student | 2 (0.93%) |
| Graduate student | 1 (0.47%) |
| Pet Ownership During Childhood a | |
| Yes, Dog(s) | 177 (82.71%) |
| Yes, Cat(s) | 83 (38.79%) |
| Yes, Other | 75 (35.05%) |
| No | 10 (4.67%) |
| ACEs a | |
| Mentally ill household member | 59 (27.57%) |
| Experienced bullying | 58 (27.10%) |
| Parental divorce/separation | 51 (23.83%) |
| Emotional abuse | 48 (22.43%) |
| Emotional neglect | 46 (21.50%) |
| Substance using household member | 47 (21.96%) |
| Felt discrimination | 38 (17.76%) |
| Incarcerated household member | 24 (11.21%) |
| Physical abuse | 23 (10.75%) |
| Sexual abuse | 20 (9.35%) |
| Crime neighborhood | 20 (9.35%) |
| Unsafe neighborhood | 14 (6.54%) |
| Witnessed domestic violence | 10 (4.67%) |
| Physical neglect | 10 (4.67%) |
| Lived in foster care | 2 (0.93%) |
| Variables | M (SD) | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|
| 1. Mental Health Symptoms (BSI-GSI) | 59.56 (12.92) | 1 | |||||
| 2. Anxiety Symptoms (BSI) | 55.73 (12.17) | 0.86 *** | 1 | ||||
| 3. Depression Symptoms (BSI) | 59.27 (11.01) | 0.88 *** | 0.76 *** | 1 | |||
| 4. Adverse Childhood Experiences (ACEs) | 2.20 (2.59) | 0.37 *** | 0.32 *** | 0.31 *** | 1 | ||
| 5. Child–Dog Emotional Closeness (MDORS) | 40.33 (7.59) | 0.07 | 0.13 | 0.04 | 0.14 | 1 | |
| 6. Child–Pet Positive Interactions (CTAQ) | 29.80 (4.27) | −0.03 | 0.03 | −0.04 | −0.01 | 0.60 *** | 1 |
| 7. Benevolent Childhood Experiences (BCEs) | 8.97 (1.57) | −0.38 *** | −0.30 *** | −0.30 *** | −0.62 *** | −0.06 | 0.03 |
| Model 1—Child–Dog Emotional Closeness | Model 2—Child–Pet Positive Interactions | Model 3—Benevolent Childhood Experiences | ||||
|---|---|---|---|---|---|---|
| B (SE) | CI | B (SE) | CI | B (SE) | CI | |
| Demographics | ||||||
| Constant | 49.01 (8.11) *** | 33.00–65.03 | 55.09 (7.40) *** | 40.49–69.69 | 55.13 (6.86) *** | 41.60–68.65 |
| Age | 0.43 (0.38) | −0.31–1.18 | 0.09 (0.34) | −0.58–0.76 | 0.16 (0.32) | −0.47–0.78 |
| Female/Non-binary/Other (Male) | 2.51 (2.52) | −2.47–7.49 | 3.16 (2.34) | −1.45–7.78 | 3.17 (2.12) | −1.02–7.35 |
| Hispanic/Latinx (Non-Hispanic/Latinx/Prefer not to say) | 1.24 (2.71) | −4.11–6.60 | 1.08 (2.49) | −3.84–6.00 | 1.17 (2.28) | −3.33–5.66 |
| Main Effects and Interactions—Model 1 (R2 = 0.14) | ||||||
| ACEs | 1.81 (0.42) *** | 0.99–2.64 | ||||
| Child–Dog Emotional Closeness | 0.01 (0.13) | −0.24–0.26 | ||||
| ACEs x Child–Dog Emotional Closeness | −0.05 (0.06) | −0.17–0.06 | ||||
| Main Effects and Interactions—Model 2 (R2 = 0.14) | ||||||
| ACEs | 1.75 (0.36) *** | 1.05–2.46 | ||||
| Child–Pet Positive Interactions | −0.12 (0.21) | −0.52–0.29 | ||||
| ACEs x Child–Dog Positive Interactions | 0.02 (0.08) | −0.14–0.18 | ||||
| Main Effects and Interactions—Model 3 (R2 = 0.21) | ||||||
| ACEs | 1.35 (0.43) ** | 0.50–2.20 | ||||
| BCEs | −3.54 (0.77) *** | −5.06–−2.02 | ||||
| ACEs x BCEs | 0.60 (0.17) *** | 0.26–0.93 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez, K.E.; McDonald, S.E.; Brown, S.M. Relationships among Early Adversity, Positive Human and Animal Interactions, and Mental Health in Young Adults. Behav. Sci. 2021, 11, 178. https://doi.org/10.3390/bs11120178
Rodriguez KE, McDonald SE, Brown SM. Relationships among Early Adversity, Positive Human and Animal Interactions, and Mental Health in Young Adults. Behavioral Sciences. 2021; 11(12):178. https://doi.org/10.3390/bs11120178
Chicago/Turabian StyleRodriguez, Kerri E., Shelby E. McDonald, and Samantha M. Brown. 2021. "Relationships among Early Adversity, Positive Human and Animal Interactions, and Mental Health in Young Adults" Behavioral Sciences 11, no. 12: 178. https://doi.org/10.3390/bs11120178
APA StyleRodriguez, K. E., McDonald, S. E., & Brown, S. M. (2021). Relationships among Early Adversity, Positive Human and Animal Interactions, and Mental Health in Young Adults. Behavioral Sciences, 11(12), 178. https://doi.org/10.3390/bs11120178