
Impact of Perceived Stress and Immune Status on Decision-Making Abilities during COVID-19 Pandemic Lockdown

Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Participants
2.3. Cognitive Tasks
2.4. Questionnaires
2.5. Data Analysis
3. Results
3.1. Effects of Age and Sex on Questionnaires Scores
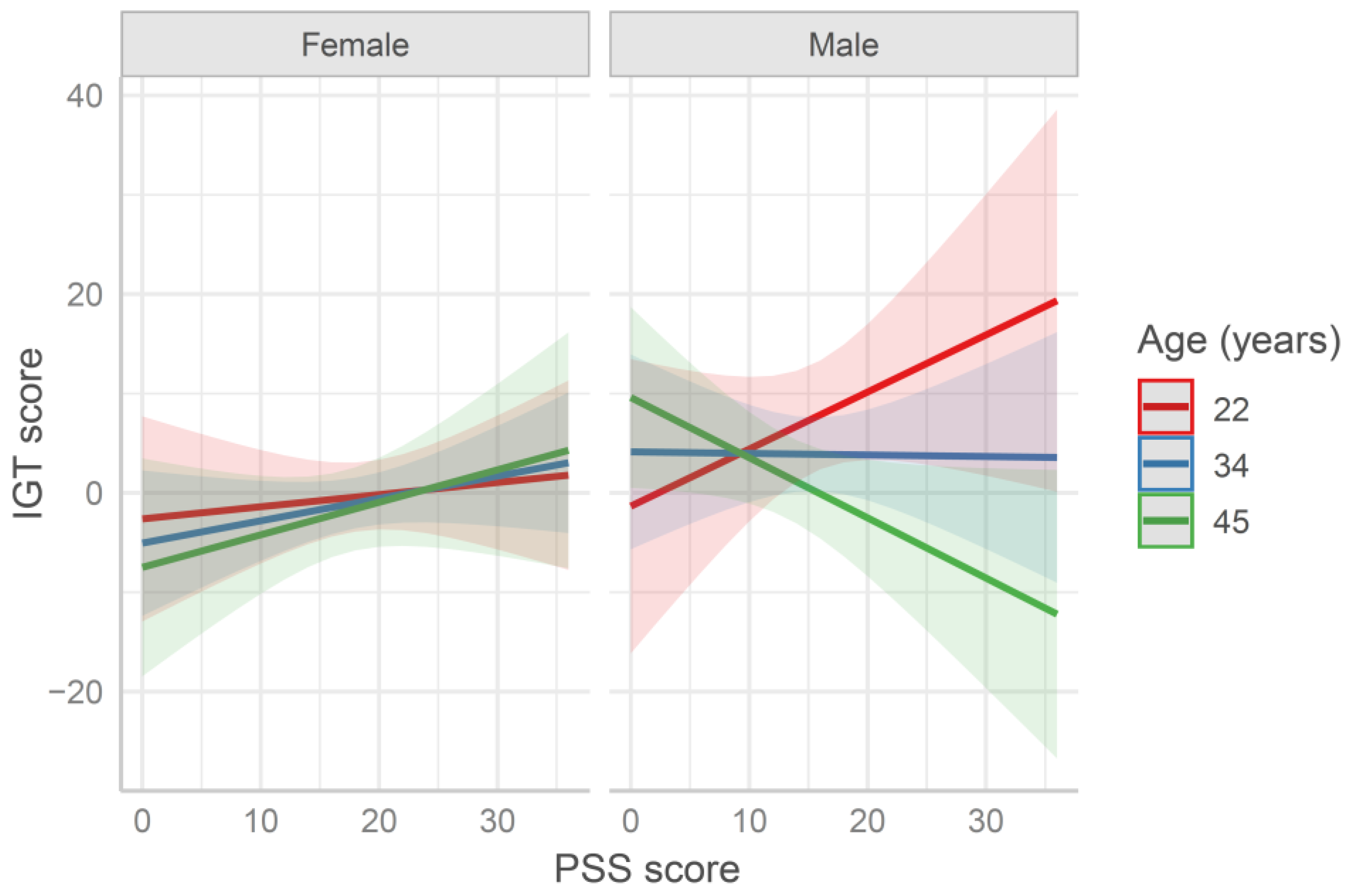
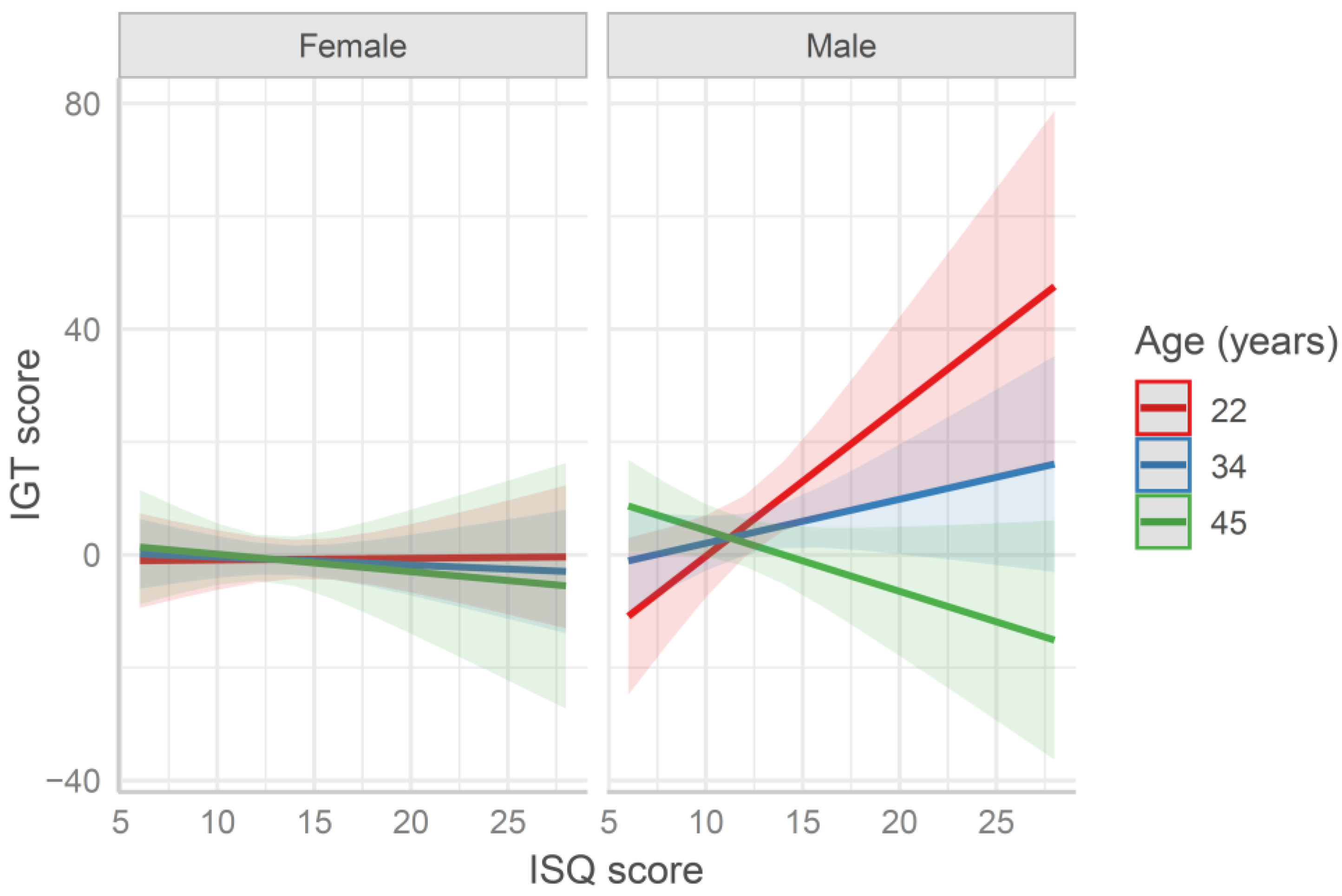
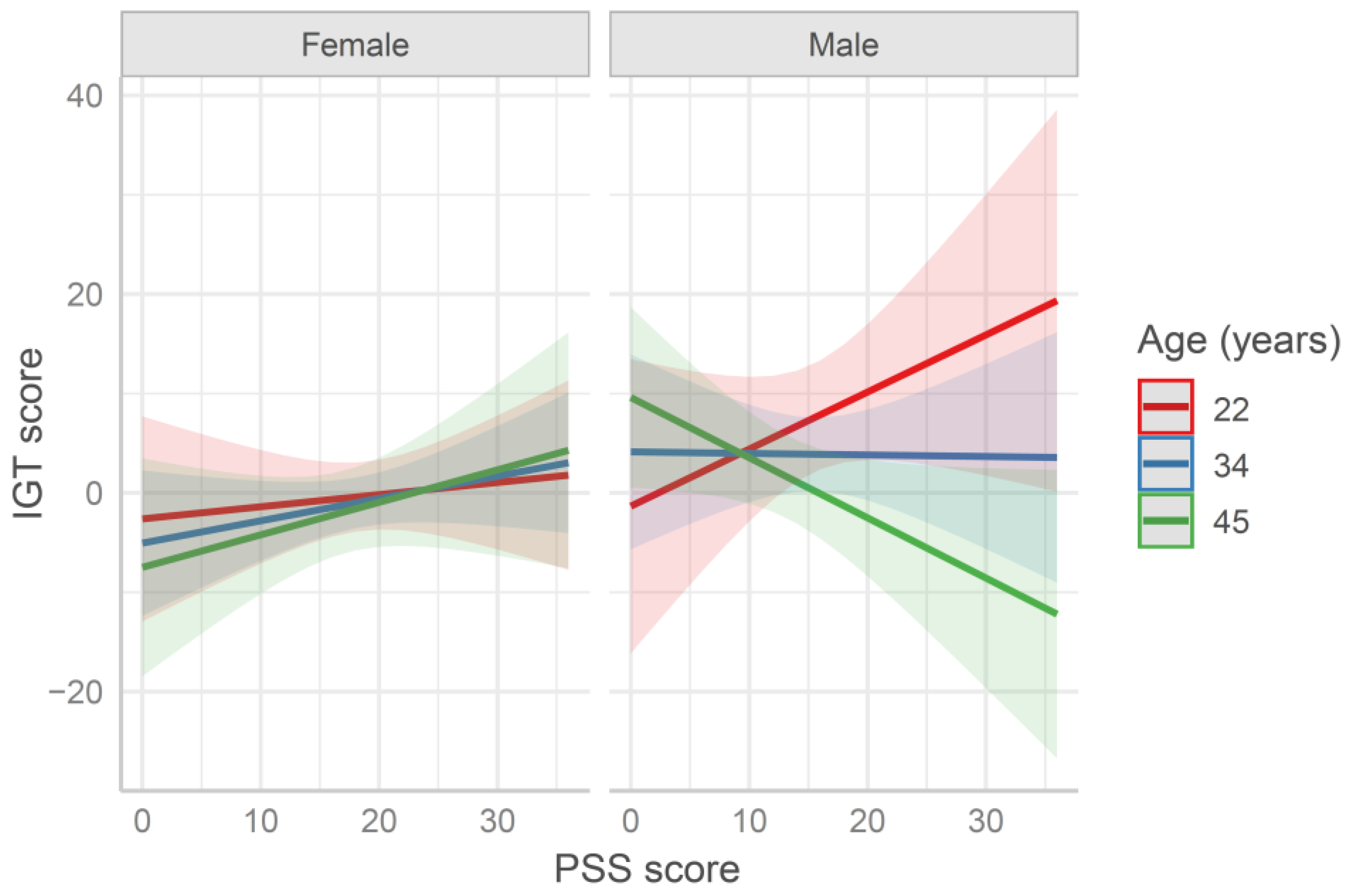
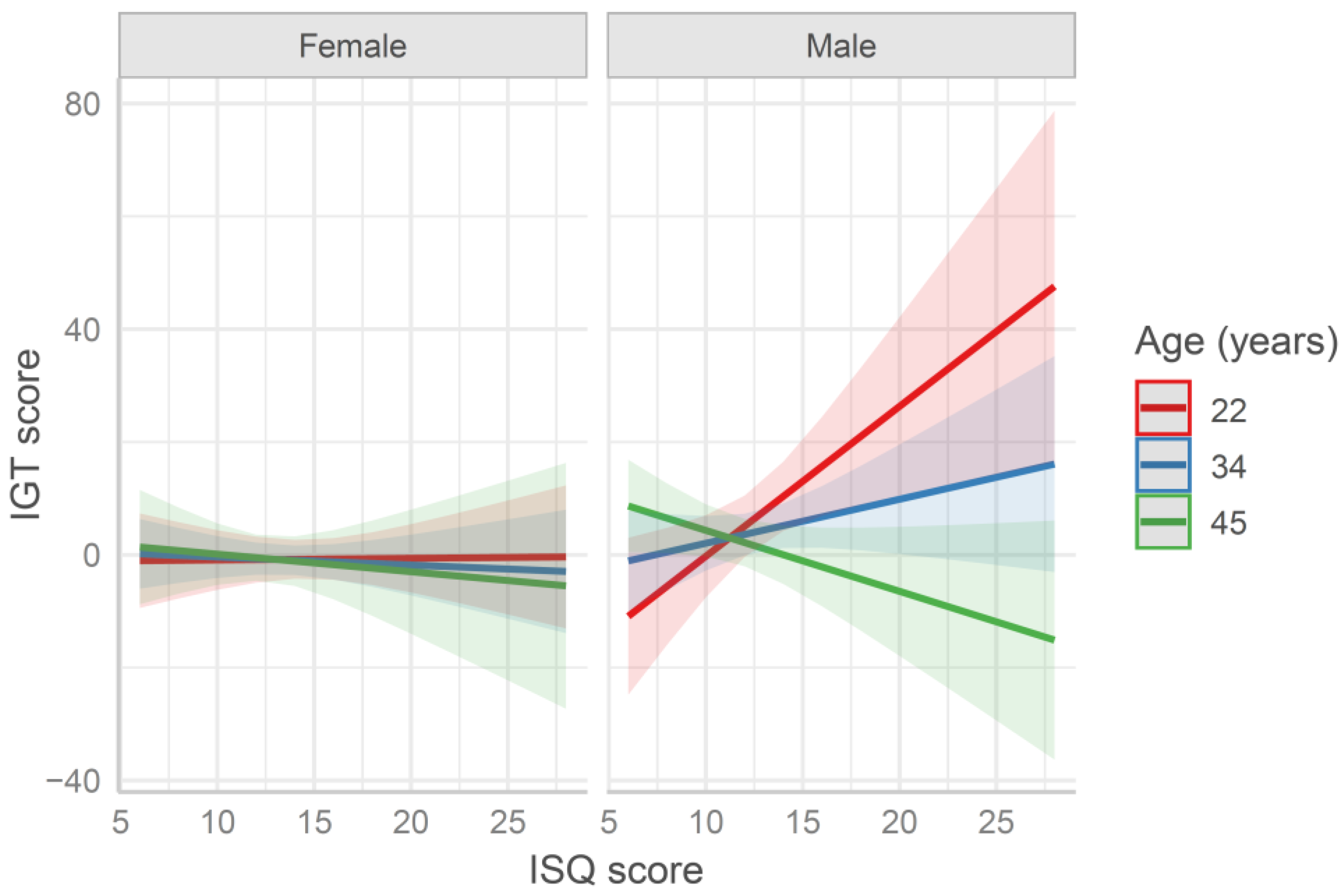
3.2. Iowa Gambling Task (IGT)
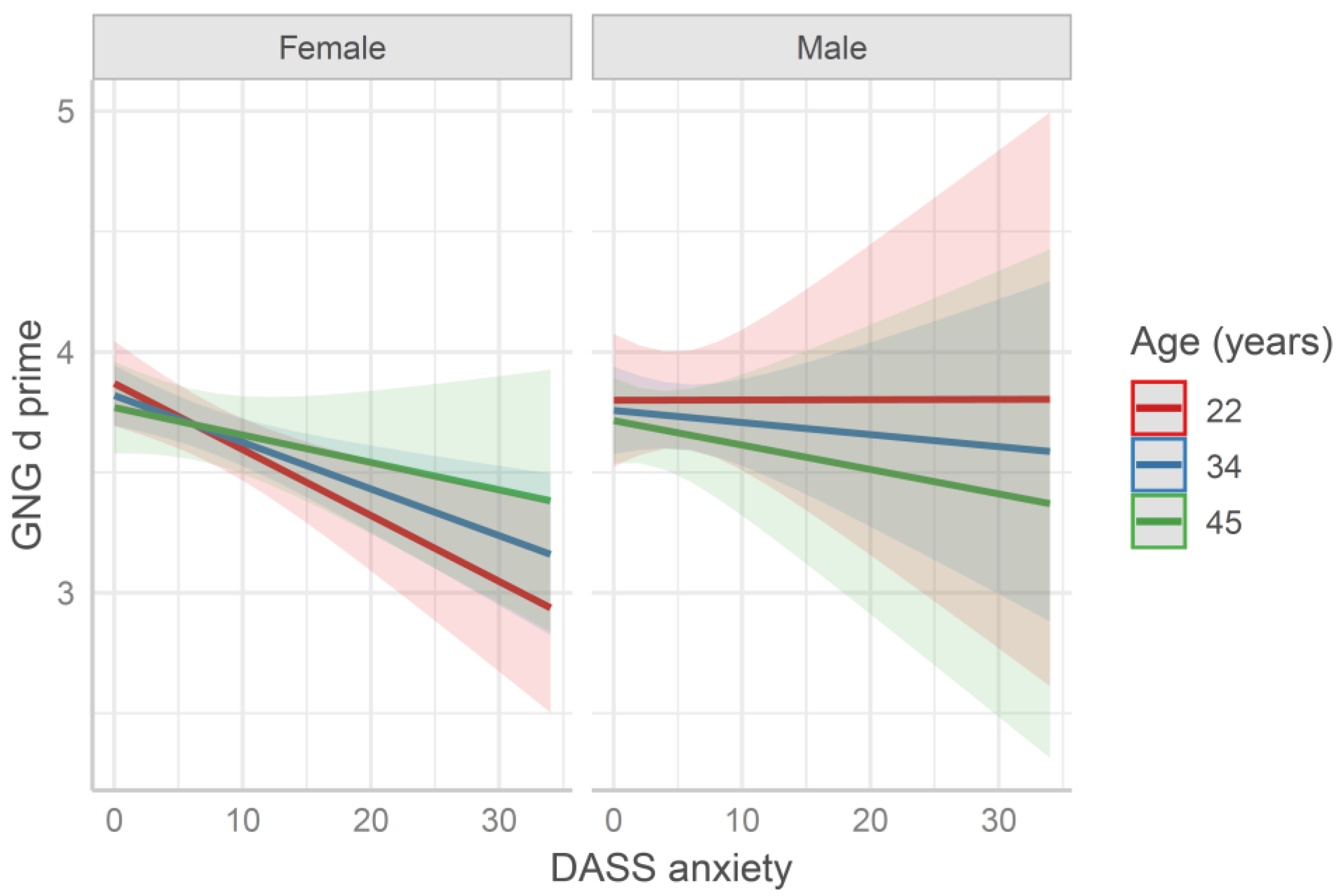
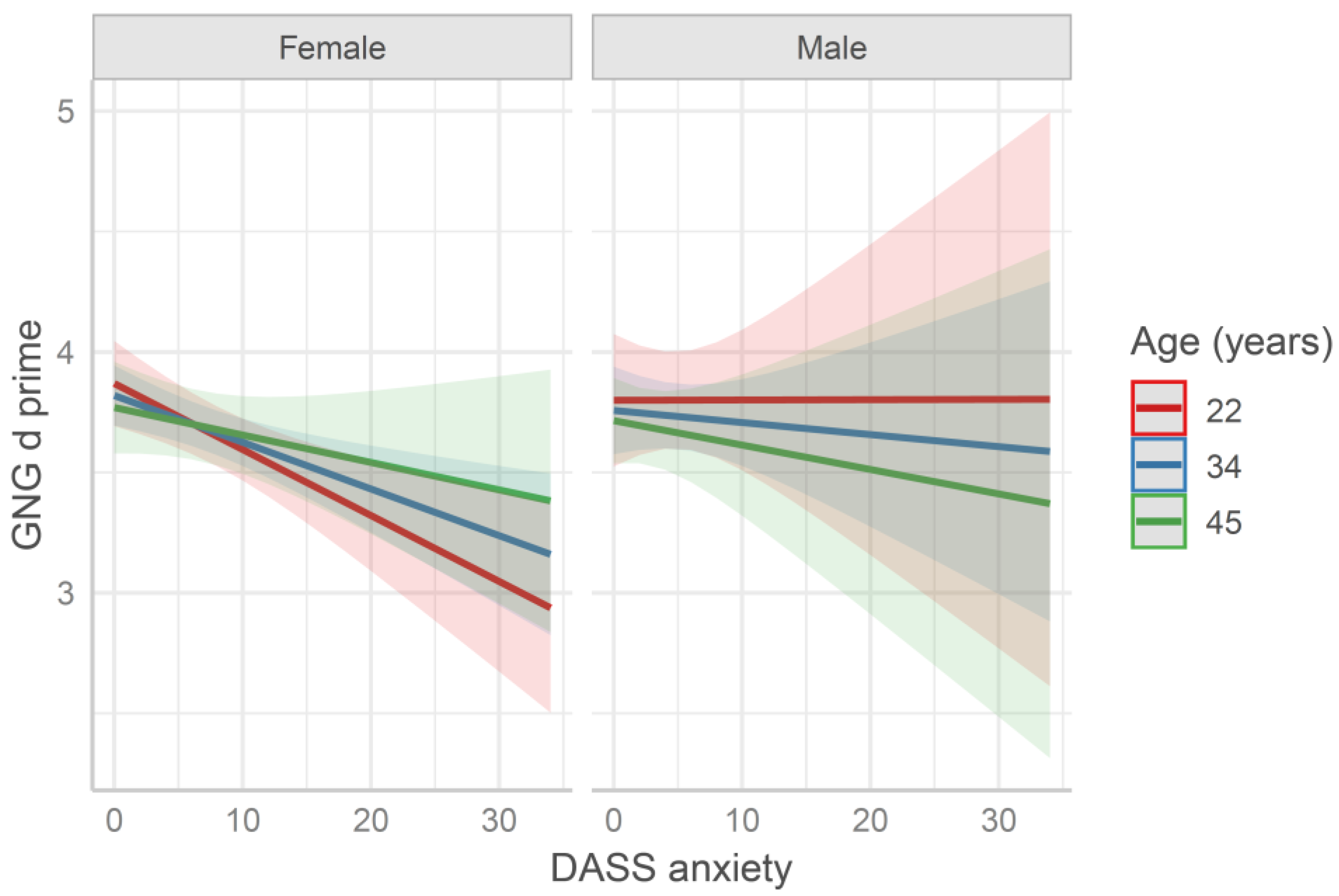
3.3. Go/No-Go Task (GNG)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bechara, A.; Damasio, A.R.; Damasio, H.; Anderson, S.W. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 1994, 50, 7–15. [Google Scholar] [CrossRef]
- Reimann, M.; Bechara, A. The somatic marker framework as a neurological theory of decision-making: Review, conceptual comparisons, and future neuroeconomics research. J. Econ. Psychol. 2010, 31, 767–776. [Google Scholar] [CrossRef]
- de Kloet, E.R.; Joëls, M.; Holsboer, F. Stress and the brain: From adaptation to disease. Nat. Rev. Neurosci. 2005, 6, 463–475. [Google Scholar] [CrossRef]
- Pappata, S.; Dehaene, S.; Poline, J.B.; Gregoire, M.C.; Jobert, A.; Delforge, J.; Frouin, V.; Bottlaender, M.; Dolle, F.; Di Giamberardino, L.; et al. In Vivo Detection of Striatal Dopamine Release during Reward: A PET Study with [11C]Raclopride and a Single Dynamic Scan Approach. Neuroimage 2002, 16, 1015–1027. [Google Scholar] [CrossRef]
- Roozendaal, B.; McReynolds, J.R.; Van der Zee, E.A.; Lee, S.; McGaugh, J.L.; McIntyre, C.K. Glucocorticoid Effects on Memory Consolidation Depend on Functional Interactions between the Medial Prefrontal Cortex and Basolateral Amygdala. J. Neurosci. 2009, 29, 14299–14308. [Google Scholar] [CrossRef] [Green Version]
- Arnsten, A.F.T. Stress signalling pathways that impair prefrontal cortex structure and function. Nat. Rev. Neurosci. 2009, 10, 410–422. [Google Scholar]
- Wang, J.; Rao, H.; Wetmore, G.S.; Furlan, P.M.; Korczykowski, M.; Dinges, D.F.; Detre, J.A. Perfusion functional MRI reveals cerebral blood flow pattern under psychological stress. Proc. Natl. Acad. Sci. USA 2005, 102, 17804–17809. [Google Scholar] [CrossRef] [Green Version]
- Porcelli, A.J.; Lewis, A.H.; Delgado, M.R. Acute Stress Influences Neural Circuits of Reward Processing. Front. Neurosci. 2012, 6, 157. [Google Scholar] [CrossRef] [Green Version]
- Porcelli, A.J.; Delgado, M.R. Acute Stress Modulates Risk Taking in Financial Decision Making. Psychol. Sci. 2009, 20, 278–283. [Google Scholar] [CrossRef] [Green Version]
- Preston, S.D.; Buchanan, T.W.; Stansfield, R.B.; Bechara, A. Effects of anticipatory stress on decision making in a gambling task. Behav. Neurosci. 2007, 121, 257–263. [Google Scholar] [CrossRef]
- Evans, J.S.B.T. In two minds: Dual-process accounts of reasoning. Trends Cogn. Sci. 2003, 7, 454–459. [Google Scholar] [CrossRef] [Green Version]
- Margittai, Z.; Nave, G.; Strombach, T.; van Wingerden, M.; Schwabe, L.; Kalenscher, T. Exogenous cortisol causes a shift from deliberative to intuitive thinking. Psychoneuroendocrinology 2016, 64, 131–135. [Google Scholar] [CrossRef]
- Porcelli, A.J.; Delgado, M.R. Stress and decision making: Effects on valuation, learning, and risk-taking. Curr. Opin. Behav. Sci. 2017, 14, 33–39. [Google Scholar]
- Yu, R. Stress potentiates decision biases: A stress induced deliberation-to-intuition (SIDI) model. Neurobiol. Stress 2016, 3, 83–95. [Google Scholar] [CrossRef] [Green Version]
- Cerqueira, J.J.; Mailliet, F.; Almeida, O.F.X.; Jay, T.M.; Sousa, N. The Prefrontal Cortex as a Key Target of the Maladaptive Response to Stress. J. Neurosci. 2007, 27, 2781–2787. [Google Scholar] [CrossRef]
- Vidal, P.M.; Pacheco, R. The cross-talk between the dopaminergic and the immune system involved in schizophrenia. Front. Pharmacol. 2020, 11, 394. [Google Scholar] [CrossRef]
- Pape, K.; Tamouza, R.; Leboyer, M.; Zipp, F. Immunoneuropsychiatry—Novel perspectives on brain disorders. Nat. Rev. Neurol. 2019, 15, 317–328. [Google Scholar] [CrossRef]
- Maydych, V. The Interplay between Stress, Inflammation, and Emotional Attention: Relevance for Depression. Front. Neurosci. 2019, 13, 384. [Google Scholar] [CrossRef]
- Huth, S.F.; Cho, S.-M.; Robba, C.; Highton, D.; Battaglini, D.; Bellapart, J.; Suen, J.Y.; Li Bassi, G.; Taccone, F.S.; Arora, R.C.; et al. Neurological Manifestations of Coronavirus Disease 2019: A Comprehensive Review and Meta-Analysis of the First 6 Months of Pandemic Reporting. Front. Neurol. 2021, 12, 664599. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar]
- Brivio, E.; Oliveri, S.; Guiddi, P.; Pravettoni, G. Incidence of PTSD and generalized anxiety symptoms during the first wave of COVID-19 outbreak: An exploratory study of a large sample of the Italian population. BMC Public Health 2021, 21, 1158. [Google Scholar] [CrossRef]
- Peters, E.M.J.; Schedlowski, M.; Watzl, C.; Gimsa, U. To stress or not to stress: Brain-behavior-immune interaction may weaken or promote the immune response to SARS-CoV-2. Neurobiol. Stress 2021, 14, 100296. [Google Scholar] [CrossRef]
- Dolsen, M.R.; Crosswell, A.D.; Prather, A.A. Links Between Stress, Sleep, and Inflammation: Are there Sex Differences? Curr. Psychiatry Rep. 2019, 21, 8. [Google Scholar] [CrossRef]
- van den Bos, R.; Harteveld, M.; Stoop, H. Stress and decision-making in humans: Performance is related to cortisol reactivity, albeit differently in men and women. Psychoneuroendocrinology 2009, 34, 1449–1458. [Google Scholar] [CrossRef]
- Kluen, L.M.; Agorastos, A.; Wiedemann, K.; Schwabe, L. Cortisol boosts risky decision-making behavior in men but not in women. Psychoneuroendocrinology 2017, 84, 181–189. [Google Scholar] [CrossRef]
- Kinner, V.L.; Wolf, O.T.; Merz, C.J. Cortisol alters reward processing in the human brain. Horm. Behav. 2016, 84, 75–83. [Google Scholar] [CrossRef]
- Lei, H.; Mochizuki, Y.; Chen, C.; Hagiwara, K.; Hirotsu, M.; Matsubara, T.; Nakagawa, S. Sex difference in the weighting of expected uncertainty under chronic stress. Sci. Rep. 2021, 11, 8700. [Google Scholar] [CrossRef]
- Kiecolt-Glaser, J.K.; Preacher, K.J.; MacCallum, R.C.; Atkinson, C.; Malarkey, W.B.; Glaser, R. Chronic stress and age-related increases in the proinflammatory cytokine IL-6. Proc. Natl. Acad. Sci. USA 2003, 100, 9090–9095. [Google Scholar] [CrossRef] [Green Version]
- Stoet, G. PsyToolkit: A software package for programming psychological experiments using Linux. Behav. Res. Methods 2010, 42, 1096–1104. [Google Scholar] [CrossRef]
- Stoet, G. PsyToolkit. Teach. Psychol. 2017, 44, 24–31. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Mondo, M.; Sechi, C.; Cabras, C. Psychometric evaluation of three versions of the Italian Perceived Stress Scale. Curr. Psychol. 2021, 40, 1884–1892. [Google Scholar] [CrossRef]
- Bottesi, G.; Ghisi, M.; Altoè, G.; Conforti, E.; Melli, G.; Sica, C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr. Psychiatry 2015, 60, 170–181. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Wilod Versprille, L.J.F.; van de Loo, A.J.A.E.; Mackus, M.; Arnoldy, L.; Sulzer, T.A.L.; Vermeulen, S.A.; Abdulahad, S.; Huls, H.; Baars, T.; Scholey, A.; et al. Development and validation of the immune status questionnaire (ISQ). Int. J. Environ. Res. Public Health 2019, 16, 4743. [Google Scholar] [CrossRef] [Green Version]
- Tarantino, V.; Vindigni, V.; Bassetto, F.; Pavan, C.; Vallesi, A. Behavioral and electrophysiological correlates of cognitive control in ex-obese adults. Biol. Psychol. 2017, 127, 198–208. [Google Scholar] [CrossRef]
- Buelow, M.T.; Barnhart, W.R. An Initial Examination of Performance on Two Versions of the Iowa Gambling Task. Arch. Clin. Neuropsychol. 2018, 33, 502–507. [Google Scholar] [CrossRef]
- Macmillan, N.A.; Creelman, C.D. Detection Theory: A User’s Guide; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2005. [Google Scholar]
- Masina, F.; Tarantino, V.; Vallesi, A.; Mapelli, D. Repetitive TMS over the left dorsolateral prefrontal cortex modulates the error positivity: An ERP study. Neuropsychologia 2019, 133, 107153. [Google Scholar] [CrossRef]
- Henningsen, A. Estimating Censored Regression Models in R using the censReg Package. R Packag. Vignettes Collect. 2010, 5, 12. [Google Scholar]
- Mangiafico, S.S. An R Companion for the Handbook of Biological Statistics; Version 1.3.2; 2015. Available online: http://rcompanion.org/rcompanion/ (accessed on 1 September 2021).
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting linear miced-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Bechara, A.; Damasio, H.; Tranel, D.; Damasio, A.R. Deciding Advantageously Before Knowing the Advantageous Strategy. Science 1997, 275, 1293–1295. [Google Scholar] [CrossRef] [Green Version]
- Reavis, R.; Overman, W.H. Adult sex differences on a decision-making task previously shown to depend on the orbital prefrontal cortex. Behav. Neurosci. 2001, 115, 196–206. [Google Scholar] [CrossRef]
- Lüdecke, D. sjPlot: Data Visualization for Statistics in Social Science; R Package Version 2.8; 2019. Available online: https://cran.microsoft.com/web/packages/sjPlot/sjPlot.pdf (accessed on 1 September 2021).
- Venables, W.N.; Ripley, B.D. Modern Applied Statistics with S. Statistics and Computing; Springer: New York, NY, USA, 2002; ISBN 978-1-4419-3008-8. [Google Scholar]
- Shieh, G. Detecting Interaction Effects in Moderated Multiple Regression With Continuous Variables Power and Sample Size Considerations. Organ. Res. Methods 2008, 12, 510–528. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A nationwide survey of psychological distress among italian people during the covid-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Mather, M.; Lighthall, N.R. Risk and Reward Are Processed Differently in Decisions Made Under Stress. Curr. Dir. Psychol. Sci. 2012, 21, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Arnsten, A.F.T. Prefrontal cortical network connections: Key site of vulnerability in stress and schizophrenia. Int. J. Dev. Neurosci. 2011, 29, 215–223. [Google Scholar] [CrossRef] [Green Version]
- McEwen, B.S.; Nasca, C.; Gray, J.D. Stress Effects on Neuronal Structure: Hippocampus, Amygdala, and Prefrontal Cortex. Neuropsychopharmacology 2016, 41, 3–23. [Google Scholar] [CrossRef] [Green Version]
- Negrón-Oyarzo, I.; Aboitiz, F.; Fuentealba, P. Impaired Functional Connectivity in the Prefrontal Cortex: A Mechanism for Chronic Stress-Induced Neuropsychiatric Disorders. Neural Plast. 2016, 7539065. [Google Scholar] [CrossRef] [Green Version]
- Shansky, R.M.; Lipps, J. Stress-induced cognitive dysfunction: Hormone-neurotransmitter interactions in the prefrontal cortex. Front. Hum. Neurosci. 2013, 7, 123. [Google Scholar] [CrossRef] [Green Version]
- Arnsten, A.F.T.; Raskind, M.A.; Taylor, F.B.; Connor, D.F. The effects of stress exposure on prefrontal cortex: Translating basic research into successful treatments for post-traumatic stress disorder. Neurobiol. Stress 2015, 1, 89–99. [Google Scholar]
- Bloomfield, M.A.; McCutcheon, R.A.; Kempton, M.; Freeman, T.P.; Howes, O. The effects of psychosocial stress on dopaminergic function and the acute stress response. eLife 2019, 8, e46797. [Google Scholar] [CrossRef]
- Doll, B.B.; Hutchison, K.E.; Frank, M.J. Dopaminergic Genes Predict Individual Differences in Susceptibility to Confirmation Bias. J. Neurosci. 2011, 31, 6188–6198. [Google Scholar] [CrossRef] [Green Version]
- Cavanagh, J.F.; Neville, D.; Cohen, M.X.; Van de Vijver, I.; Harsay, H.; Watson, P.; Buitenweg, J.I.; Ridderinkhof, K.R. Individual Differences in Risky Decision-Making Among Seniors Reflect Increased Reward Sensitivity. Front. Neurosci. 2012, 6, 111. [Google Scholar] [CrossRef] [Green Version]
- Raio, C.M.; Konova, A.B.; Otto, A.R. Trait impulsivity and acute stress interact to influence choice and decision speed during multi-stage decision-making. Sci. Rep. 2020, 10, 7754. [Google Scholar] [CrossRef]
- Frank, M.J.; Claus, E.D. Anatomy of a decision: Striato-orbitofrontal interactions in reinforcement learning, decision making, and reversal. Psychol. Rev. 2006, 113, 300–326. [Google Scholar] [CrossRef] [Green Version]
- Gassen, J.; Prokosch, M.L.; Eimerbrink, M.J.; Proffitt Leyva, R.P.; White, J.D.; Peterman, J.L.; Burgess, A.; Cheek, D.J.; Kreutzer, A.; Nicolas, S.C.; et al. Inflammation Predicts Decision-Making Characterized by Impulsivity, Present Focus, and an Inability to Delay Gratification. Sci. Rep. 2019, 9, 4928. [Google Scholar] [CrossRef]
- Lighthall, N.R.; Gorlick, M.A.; Schoeke, A.; Frank, M.J.; Mather, M. Stress modulates reinforcement learning in younger and older adults. Psychol. Aging 2013, 28, 35–46. [Google Scholar] [CrossRef] [Green Version]
- Moustafa, A.A.; Tindle, R.; Frydecka, D.; Misiak, B. Impulsivity and its relationship with anxiety, depression and stress. Compr. Psychiatry 2017, 74, 173–179. [Google Scholar] [CrossRef]
- Roxburgh, A.D.; White, D.J.; Cornwell, B.R. Anxious arousal alters prefrontal cortical control of stopping. Eur. J. Neurosci. 2020, 1–13. [Google Scholar] [CrossRef]
- Aram, S.; Levy, L.; Patel, J.B.; Anderson, A.A.; Zaragoza, R.; Dashtestani, H.; Chowdhry, F.A.; Gandjbakhche, A.; Tracy, J.K. The Iowa Gambling Task: A Review of the Historical Evolution, Scientific Basis, and Use in Functional Neuroimaging. SAGE Open 2019, 9, 215824401985691. [Google Scholar] [CrossRef]
- Krain, A.L.; Wilson, A.M.; Arbuckle, R.; Castellanos, F.X.; Milhama, M.P. Distinct neural mechanisms of risk and ambiguity: A meta-analysis of decision-making. Neuroimage 2006, 32, 477–484. [Google Scholar] [CrossRef]
- Dantzer, R.; Kelley, K.W. Twenty years of research on cytokine-induced sickness behavior. Brain. Behav. Immun. 2007, 21, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Aron, A.R.; Robbins, T.W.; Poldrack, R.A. Inhibition and the right inferior frontal cortex: One decade on. Trends Cogn. Sci. 2014, 18, 177–185. [Google Scholar] [CrossRef]
- Sumner, R.C.; Parton, A.; Nowicky, A.V.; Kishore, U.; Gidron, Y. Hemispheric lateralisation and immune function: A systematic review of human research. J. Neuroimmunol. 2011, 240–241, 1–12. [Google Scholar] [CrossRef]
- Cerqueira, J.J.; Almeida, O.F.X.; Sousa, N. The stressed prefrontal cortex. Left? Right! Brain. Behav. Immun. 2008, 22, 630–638. [Google Scholar] [CrossRef]
- Verbruggen, F.; Aron, A.R.; Band, G.P.H.; Beste, C.; Bissett, P.G.; Brockett, A.T.; Brown, J.W.; Chamberlain, S.R.; Chambers, C.D.; Colonius, H.; et al. A consensus guide to capturing the ability to inhibit actions and impulsive behaviors in the stop-signal task. eLife 2019, 8, e46323. [Google Scholar] [CrossRef]
- Rungratsameetaweemana, N.; Itthipuripat, S.; Salazar, A.; Serences, J.T. Expectations do not alter early sensory processing during perceptual decision-making. J. Neurosci. 2018, 38, 5632–5648. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Age < 34 y | Age > 34 y | |||
|---|---|---|---|---|
| F | M | F | M | |
| PSS | 18.8 (6.5) | 16.1 (6) | 18.2 (6.9) | 13.3 (7) |
| DASS Depression | 12.3 (8.8) | 11.3 (9) | 10.1 (10.5) | 7.9 (8.8) |
| DASS Anxiety | 7.7 (7.8) | 5.1 (4.7) | 6 (7.2) | 3.7 (6.5) |
| DASS Stress | 17.1 (9.6) | 12.4 (7.2) | 14.6 (8.7) | 11.3 (8.8) |
| ISQ | 14.9 (3.8) | 12.8 (2.8) | 12.6 (3) | 11.7 (3) |
| Current General Health | 7.8 (1.1) | 8 (1.2) | 7.5 (1.1) | 7.8 (1) |
| Current Immune Functioning | 7.7 (1.4) | 8.1 (1.3) | 8.1 (1.2) | 8.3 (1.2) |
| Button A or B | Button C or D | |||
|---|---|---|---|---|
| % Choice | RTs | % Choice | RTs | |
| First 50 Trials | 49.3 (17.3) | 1319 ms (581) | 50.7 (17.3) | 1225 ms (560) |
| Last 50 Trials | 43.9 (23.6) | 930 ms (487) | 56.1 (23.6) | 847 ms (439) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarantino, V.; Tasca, I.; Giannetto, N.; Mangano, G.R.; Turriziani, P.; Oliveri, M. Impact of Perceived Stress and Immune Status on Decision-Making Abilities during COVID-19 Pandemic Lockdown. Behav. Sci. 2021, 11, 167. https://doi.org/10.3390/bs11120167
Tarantino V, Tasca I, Giannetto N, Mangano GR, Turriziani P, Oliveri M. Impact of Perceived Stress and Immune Status on Decision-Making Abilities during COVID-19 Pandemic Lockdown. Behavioral Sciences. 2021; 11(12):167. https://doi.org/10.3390/bs11120167
Chicago/Turabian StyleTarantino, Vincenza, Ilaria Tasca, Nicoletta Giannetto, Giuseppa Renata Mangano, Patrizia Turriziani, and Massimiliano Oliveri. 2021. "Impact of Perceived Stress and Immune Status on Decision-Making Abilities during COVID-19 Pandemic Lockdown" Behavioral Sciences 11, no. 12: 167. https://doi.org/10.3390/bs11120167
APA StyleTarantino, V., Tasca, I., Giannetto, N., Mangano, G. R., Turriziani, P., & Oliveri, M. (2021). Impact of Perceived Stress and Immune Status on Decision-Making Abilities during COVID-19 Pandemic Lockdown. Behavioral Sciences, 11(12), 167. https://doi.org/10.3390/bs11120167