The Mediator Role of Body Image-Related Cognitive Fusion in the Relationship between Disease Severity Perception, Acceptance and Psoriasis Disability

 , , , ,
, , , ,  , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.2.1. Sociodemographic and Clinical Questionnaire
2.2.2. Psoriasis Disability Index
2.2.3. Cognitive Fusion Questionnaire—Body Image
2.2.4. Acceptance and Action Questionnaire—II
2.2.5. Self-Compassion Scale
2.3. Data Analysis
3. Results
3.1. Sample Characterization
3.2. Comparison Between Psoriasis Disability Index, Body Image-Related Cognitive Fusion, Acceptance and Action, and Self-Compassion Frequencies in this Study and in the Original Authors’ Studies
3.3. Correlations between Sociodemographic, Clinical and Psychological Variables
3.4. Hierarchical Multiple Linear Regression: Predictors of Psoriasis Disability Index (Final Model)
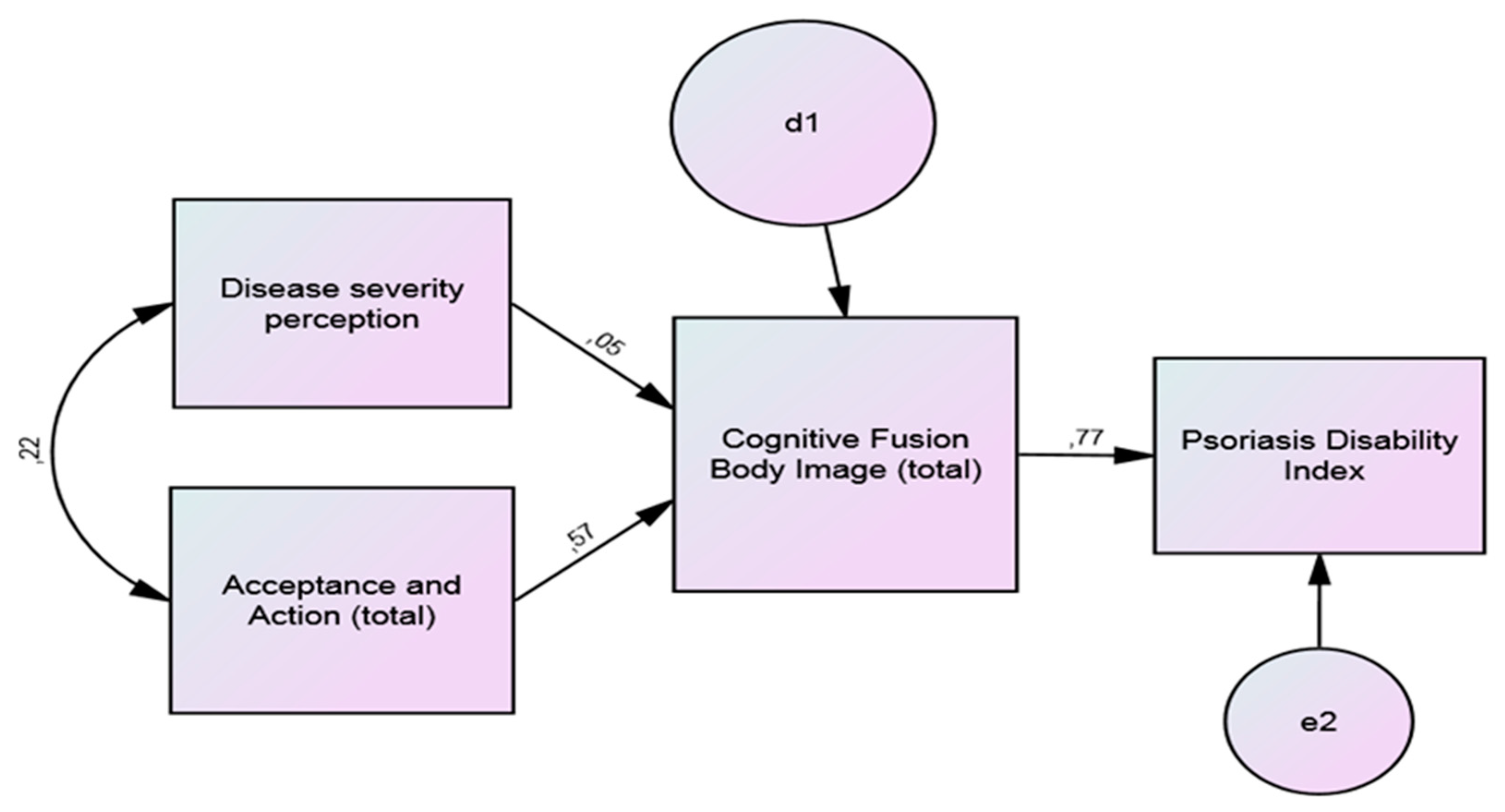
3.5. Body Image as Mediator of Acceptance and Disease Severity Perception, and PDI
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Parisi, R.; Webb, R.T.; Kleyn, C.E.; Carr, M.J.; Kapur, N.; Griffiths, C.E.M.; Ashcroft, D.M. Psychiatric morbidity and suicidal behaviour in psoriasis. Br. J. Dermatol. 2019, 180, e16. [Google Scholar] [CrossRef]
- Christophers, E.; Kerkhof, P.C.M. Severity, heterogeneity and systemic inflammation in psoriasis. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 643–647. [Google Scholar] [CrossRef]
- Founta, O.; Adamzik, K.; Tobin, A.-M.; Kirby, B.; Hevey, D. Psychological distress, alexithymia and alcohol misuse in patients with psoriasis: A cross-sectional study. J. Clin. Psychol. Med. Settings 2018, 26, 200–219. [Google Scholar] [CrossRef]
- Deveci, E.; Kocacenk, T.; Şahan, E.; Yılmaz, O.; Öztürk, A.; Kırpınar, İ. Oxidative stress and inflammatory response in patients with psoriasis; is there any relationship with psychiatric comorbidity and cognitive functions? Psychiatry Clin. Psychopharmacol. 2019, 29, 682–695. [Google Scholar] [CrossRef]
- Finlay, A.Y.; Kelly, S.E. Psoriasis—An index of disability. Clin. Exp. Dermatol. 1987, 12, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Thyssen, J.P.; Wu, J.J.; Skov, L. Psoriasis and depression. Br. J. Dermatol. 2019, 180, e12. [Google Scholar] [CrossRef][Green Version]
- Erdogan, H.; Altinoz, A.; Acer, E.; Saracoglu, Z.; Bilgin, M. Evaluation of anxiety sensitivity in patients with psoriasis. Dermatol. Sin. 2019, 37, 28. [Google Scholar] [CrossRef]
- Remröd, C.; Sjöström, K.; Svensson, Å. Pruritus in psoriasis: A study of personality traits, depression and anxiety. Acta Derm. Venereol. 2015, 95, 439–443. [Google Scholar] [CrossRef]
- Chen, A.; Beck, K.M.; Tan, E.; Koo, J. Stigmatization in Psoriasis. J. Psoriasis Psoriatic Arthritis 2018, 3, 100–106. [Google Scholar] [CrossRef]
- Ghorbanibirgani, A.; Fallahi-Khoshknab, M.; Zarea, K.; Abedi, H. The lived experience of psoriasis patients from social stigma and rejection: A qualitative study. Iran. Red Crescent Med. J. 2016, 18, e27893. [Google Scholar] [CrossRef][Green Version]
- Obradors, M.; Blanch, C.; Comellas, M.; Figueras, M.; Lizan, L. Health-related quality of life in patients with psoriasis: A systematic review of the European literature. Qual. Life Res. 2016, 25, 2739–2754. [Google Scholar] [CrossRef] [PubMed]
- Tomas-Aragones, L.; Marron, S. Body image and body dysmorphic concerns. Acta Derm. Venereol. 2014, 96, 47–50. [Google Scholar] [CrossRef]
- Rosińska, M.; Rzepa, T.; Szramka-Pawlak, B.; Żaba, R. Body Image and depressive symptoms in person suffering from psoriasis. Psychiatr. Pol. 2017, 51, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Adamska, M.; Miniszewska, J. Determinants of acceptance of an illness in the case of patients suffering from psoriasis treated in the hospital and outpatient clinic settings. Health Psychol. Rep. 2016, 4, 54–64. [Google Scholar] [CrossRef][Green Version]
- D’Alton, P.; Kinsella, L.; Walsh, O.; Sweeney, C.; Timoney, I.; Lynch, M.; O’Connor, M.; Kirby, B. Mindfulness-Based Interventions for Psoriasis: A Randomized Controlled Trial. Mindfulness 2018, 10, 288–300. [Google Scholar] [CrossRef]
- Hayes, S.C.; Wilson, K.G.; Gifford, E.V.; Follette, V.M.; Strosahl, K. Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. J. Consult. Clin. Psychol. 1996, 64, 1152–1168. [Google Scholar] [CrossRef]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary psychometric properties of the acceptance and action questionnaire–II: A revised measure of psychological inflexibility and experiential avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef]
- Neff, K.D. The self-compassion scale is a valid and theoretically coherent measure of self-compassion. Mindfulness 2015, 7, 264–274. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Eifert, G.H.; Forsyth, J.P.; Arch, J.; Espejo, E.; Keller, M.; Langer, D. Acceptance and commitment therapy for anxiety disorders: Three case studies exemplifying a unified treatment protocol. Cogn. Behav. Pract. 2009, 16, 368–385. [Google Scholar] [CrossRef]
- Nazik, H.; Nazik, S.; Gul, F. Body image, self-esteem, and quality of life in patients with psoriasis. Indian Dermatol. Online J. 2017, 8, 343. [Google Scholar] [CrossRef] [PubMed]
- Trindade, I.A.; Ferreira, C. The impact of body image-related cognitive fusion on eating psychopathology. Eat. Behav. 2014, 15, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.; Trindade, I.A.; Duarte, C.; Pinto-Gouveia, J. Getting entangled with body image: Development and validation of a new measure. Psychol. Psychother. Theory Res. Pract. 2014, 88, 304–316. [Google Scholar] [CrossRef]
- Khoury, L.R.; Danielsen, P.L.; Skiveren, J. Body image altered by psoriasis. A study based on individual interviews and a model for body image. J. Dermatolog. Treat. 2013, 25, 2–7. [Google Scholar] [CrossRef]
- Nair, S.; Riaz, O. Psoriasis and its correlation with depression and body image: Case report. Clin. Oncol. 2018, 3, 4–6. [Google Scholar]
- Łakuta, P.; Przybyła-Basista, H. Toward a better understanding of social anxiety and depression in psoriasis patients: The role of determinants, mediators, and moderators. J. Psychosom. Res. 2017, 94, 32–38. [Google Scholar] [CrossRef]
- Lawrence, J.W.; Fauerbach, J.A.; Thombs, B.D. A test of the moderating role of importance of appearance in the relationship between perceived scar severity and body-esteem among adult burn survivors. Body Image 2006, 3, 101–111. [Google Scholar] [CrossRef]
- Apifarma Dia Mundial da Psoríase [Psoriasis Global Day]. Available online: https://www.apifarma.pt/publicacoes/factsheetsAD/Documents/FichaDiamundialPsoriasefinal.pdf (accessed on 7 August 2020).
- Fernandes, B.; Ferreira, P.L.; Figueiredo, A. Quality of Life in Psoriasis Patients. Validation of the Portuguese Version of the Psoriasis Disability Index. J. Port. Soc. Dermatol. Venereol. 2012, 70, 53. [Google Scholar] [CrossRef]
- Gillanders, D.T.; Bolderston, H.; Bond, F.W.; Dempster, M.; Flaxman, P.E.; Campbell, L.; Kerr, S.; Tansey, L.; Noel, P.; Ferenbach, C.; et al. The development and initial validation of the cognitive fusion questionnaire. Behav. Ther. 2014, 45, 83–101. [Google Scholar] [CrossRef]
- Pinto-Gouveia, J.; Gregorio, S.; Dinis, A.; Xavier, A. Experiential avoidance in clinical and non-clinical samples: AAQ-II Portuguese Version. Int. J. Psychol. Psychol. Ther. 2012, 12, 139–156. [Google Scholar]
- Neff, K.D. The development and validation of a scale to measure self-compassion. Self Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]
- Castilho, P.; Pinto-Gouveia, J.; Duarte, J. Evaluating the multifactor structure of the long and short versions of the self-compassion scale in a clinical sample. J. Clin. Psychol. 2015, 71, 856–870. [Google Scholar] [CrossRef]
- Stuntzner, S. Compassion and Self-compassion: Conceptualization of and application to adjustment to disability. J. Appl. Rehabil. Couns. 2017, 48, 15–25. [Google Scholar] [CrossRef]
- Groot, J.; Nybo Andersen, A.M.; Adam, A.; Tind Nielsen, T.E.; Blegvad, C.; Skov, L. Associations between maternal socioeconomic position and psoriasis: A cohort study among the offspring of the Danish National Birth Cohort. Br. J. Dermatol. 2018, 180, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Löfvendahl, S.; Theander, E.; Svensson, Å.; Carlsson, K.S.; Englund, M.; Petersson, I.F. Validity of Diagnostic codes and prevalence of physician-diagnosed psoriasis and psoriatic arthritis in Southern Sweden—A population-based register study. PLoS ONE 2014, 9, e98024. [Google Scholar] [CrossRef]
- Kimball, A.B.; Augustin, M.; Gordon, K.B.; Krueger, G.G.; Pariser, D.; Fakharzadeh, S.; Goyal, K.; Calabro, S.; Lee, S.; Lin, R.; et al. Correlation of psoriasis activity with socioeconomic status: Cross-sectional analysis of patients enrolled in the Psoriasis Longitudinal Assessment and Registry (PSOLAR). Br. J. Dermatol. 2018, 179, 984–986. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.H.; Yao; Hong, S.; Fung; Lui, Y.; Ji; Chan, X.; Lai Wan, C. Dynamic balancing in illness coping: An interpretative phenomenological analysis on the lived experience of chinese patients with psoriasis. Health Sci. J. 2017, 11, 515. [Google Scholar] [CrossRef]
- Nguyen, C.; Beroukhim, K.; Danesh, M.; Babikian, A.; Koo, J.; Leon, A. The psychosocial impact of acne, vitiligo, and psoriasis: A review. Clin. Cosmet. Investig. Dermatol. 2016, 9, 383–392. [Google Scholar] [CrossRef]
- Augustin, M. Cumulative life course impairment: Identifying patients at risk. Dermatol. Dis. Cumul. Life Course Impair. 2013, 44, 74–81. [Google Scholar]
- Hawro, T.; Zalewska, A.; Hawro, M.; Kaszuba, A.; Królikowska, M.; Maurer, M. Impact of psoriasis severity on family income and quality of life. J. Eur. Acad. Dermatol. Venereol. 2014, 29, 438–443. [Google Scholar] [CrossRef]
- Kouris, A.; Platsidaki, E.; Kouskoukis, C.; Christodoulou, C. Psychological parameters of psoriasis. Psychiatriki 2017, 28, 54–59. [Google Scholar] [CrossRef]
- Wojtyna, E.; Łakuta, P.; Marcinkiewicz, K.; Bergler-Czop, B.; Brzezińska-Wcisło, L. Gender, Body image and social support: Biopsychosocial deter minants of depression among patients with psoriasis. Acta Derm. Venereol. 2017, 97, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Łakuta, P.; Marcinkiewicz, K.; Bergler-Czop, B.; Brzezińska-Wcisło, L. How does stigma affect people with psoriasis? Adv. Dermatol. Allergol. 2017, 1, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Nordbø, E.C.A.; Aamodt, G.; Ihlebæk, C.M. Subjective health complaints in individuals with psoriasis and psoriatic arthritis: Associations with the severity of the skin condition and illness perceptions—A cross-sectional study. Int. J. Behav. Med. 2017, 24, 438–446. [Google Scholar] [CrossRef]
- Lebwohl, M.G.; Kavanaugh, A.; Armstrong, A.W.; Van Voorhees, A.S. US Perspectives in the management of psoriasis and psoriatic arthritis: Patient and physician results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis (MAPP) survey. Am. J. Clin. Dermatol. 2015, 17, 87–97. [Google Scholar] [CrossRef]
- Flynn, M.K.; Hernandez, J.O.; Hebert, E.R.; James, K.K.; Kusick, M.K. Cognitive fusion among hispanic college students: Further validation of the cognitive fusion questionnaire. J. Context. Behav. Sci. 2018, 7, 29–34. [Google Scholar] [CrossRef]
- Sakson-Obada, O.; Pawlaczyk, M.; Gerke, K.; Adamski, Z. Acceptance of psoriasis in the context of body image, body experience, and social support. Health Psychol. Rep. 2017, 3, 251–257. [Google Scholar] [CrossRef]
- Bardeen, J.R.; Fergus, T.A. The interactive effect of cognitive fusion and experiential avoidance on anxiety, depression, stress and posttraumatic stress symptoms. J. Context. Behav. Sci. 2016, 5, 1–6. [Google Scholar] [CrossRef]
- Hapenny, J.E.; Fergus, T.A. Cognitive fusion, experiential avoidance, and their interactive effect: Examining associations with thwarted belongingness and perceived burdensomeness. J. Context. Behav. Sci. 2017, 6, 35–41. [Google Scholar] [CrossRef]


{kind=link}
| Sociodemographic Variables | % |
|---|---|
| Age (M ± SD) | 54.99 ± 13.72 |
| Gender (%) | |
| Female | 48.0 |
| Male | 52.0 |
| Marital Status (%) | |
| Not married/Committed | 24.0 |
| Married/Committed | 76.0 |
| Education (%) | |
| Non-graduate | 53.3 |
| Graduate | 46.7 |
| Occupation (%) | |
| Active | 57.3 |
| Inactive | 42.7 |
| Clinical variables | |
| Years of diagnosis (M ± SD) | 23.96 ± 15.40 |
| Family history of psoriasis (%) | |
| No | 57.3 |
| Yes | 42.7 |
| Other diseases (%) | |
| No | 56.0 |
| Yes | 44.0 |
| Satisfaction with current treatment (%) | |
| No | 30.7 |
| Yes | 69.3 |
| Disease severity perception (%) | |
| Mild | 22.7 |
| Moderate | 58.7 |
| Severe | 18.7 |
| Anxiolytics and antidepressants (%) | |
| No | 73.3 |
| Yes | 26.7 |
| Impact in social life (%) | |
| None or little | 68.0 |
| Some or a lot | 32.0 |
| Variables | This Study | Original Authors’ Instruments Studies [24,30,32,34] | Statistical Comparison | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | M | SD | α | n | M | SD | α | t | df | p | d | |
| Psoriasis Disability Index (total) | 75 | 8.44 | 7.33 | 0.82 | 171 | 2.10 | 1.60 | 0.89 | 7.414 | 77, 111 | <0.001 | 1.95 |
| Daily activities | 75 | 4.44 | 3.95 | 0.87 | 171 | 3.10 | 2.20 | 0.83 | 2.756 | 94, 743 | 0.007 | 0.42 |
| Work or school | 75 | 0.93 | 1.48 | 0.56 | 171 | 0.99 | 1.70 | 0.75 | −0.279 | 160, 962 | 0.780 | 0.04 |
| Personal relationships | 75 | 0.71 | 1.10 | 0.80 | 171 | 1.40 | 2.20 | 0.87 | −3.273 | 239, 942 | 0.001 | 0.40 |
| Leisure | 75 | 1.67 | 1.88 | 0.57 | 171 | 1.70 | 2.10 | 0.85 | −0.111 | 156, 724 | 0.912 | 0.02 |
| Treatment (1 item) | 75 | 0.69 | 0.77 | − | 171 | 2.30 | 2.90 | − | −6.738 | 216, 210 | <0.001 | 0.76 |
| Body Image Cognitive Fusion (total) | 75 | 28.15 | 13.89 | 0.98 | 31 | 51.74 | 12.12 | 0.96 | 8.725 | 63, 792 | <0.001 | 1.81 |
| Acceptance and Action (total) | 75 | 33.19 | 8.21 | 0.73 | 297 | 33.47 | 9.46 | 0.90 | 0.256 | 128, 332 | 0.799 | 0.03 |
| Self-Compassion (total) | 75 | 84.51 | 15.83 | 0.83 | 298 | 60.25 | 15.79 | 0.92 | −12.643 | 89, 803 | <0.001 | 1.53 |
| Self-Kindness | 75 | 13.77 | 4.35 | 0.83 | 298 | 10.57 | 3.87 | 0.92 | −6.234 | 83, 743 | <0.001 | 0.78 |
| Self-Judgment | 75 | 17.29 | 4.31 | 0.86 | 298 | 18.41 | 4.05 | 0.93 | 2.174 | 84, 904 | 0.032 | 0.27 |
| Common Humanity | 75 | 12.19 | 3.45 | 0.80 | 298 | 10.09 | 3.15 | 0.85 | −5.102 | 84, 277 | <0.001 | 0.64 |
| Isolation | 75 | 14.17 | 3.33 | 0.84 | 298 | 14.77 | 3.31 | 0.89 | 1.502 | 86, 246 | 0.137 | 0.18 |
| Mindfulness | 75 | 12.85 | 3.19 | 0.73 | 298 | 9.55 | 2.88 | 0.85 | −8.678 | 84, 041 | <0.001 | 1.09 |
| Over-identification | 75 | 14.23 | 3.19 | 0.79 | 298 | 14.77 | 3.24 | 0.88 | 1.408 | 86, 805 | 0.163 | 0.17 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Years of education | 1 | −0.028 | 0.053 | −0.004 | 0.070 | 0.106 | −0.031 | −0.168 | −0.187 | −0.085 | −0.044 | −0.070 | −0.236 * | −0.067 | 0.111 | −0.079 | 0.067 | −0.205 | 0.012 | −0.055 | −0.089 | −0.076 |
| 2. Other diseases | 1 | 0.159 | 0.097 | 0.182 | 0.194 | 0.098 | 0.087 | 0.120 | −0.088 | 0.066 | 0.115 | 0.004 | 0.181 | 0.260 * | −0.292 * | −0.239 * | −.230 * | −0.189 | −0.330 ** | −0.120 | −0.140 | |
| 3. Family history of psoriasis | 1 | 0.054 | 0.106 | 0.089 | −0.022 | 0.096 | 0.137 | −0.016 | −0.015 | 0.110 | −0.007 | 0.116 | 0.106 | 0.042 | 0.132 | −0.072 | 0.268 * | −0.086 | 0.083 | −0.155 | ||
| 4. Disease severity perception | 1 | 0.004 | 0.273 * | 0.460 ** | 0.247 * | 0.213 | 0.195 | 0.173 | 0.311 ** | −0.134 | 0.269 * | 0.218 | −0.215 | −0.229 * | −0.185 | −0.081 | −0.122 | −0.101 | −0.186 | |||
| 5. Satisfaction with treatment | 1 | 0.009 | −0.051 | −0.047 | −0.036 | −0.246 * | −0.020 | 0.021 | 0.187 | −0.148 | −0.031 | −0.017 | 0.085 | −0.029 | 0.045 | −0.096 | −0.040 | −0.071 | ||||
| 6. Anxiolytics/antidepressants | 1 | 0.221 | 0.200 | 0.163 | 0.048 | 0.272 * | 0.252 * | −0.034 | 0.219 | 0.252 * | −0.309 ** | −0.219 | −.330 ** | 0.002 | −.286 * | −0.210 | −0.281 * | |||||
| 7. Impact in social life | 1 | 0.687 ** | 0.671 ** | 0.462 ** | 0.494 ** | 0.564 ** | 0.114 | 0.645 ** | 0.432 ** | −0.329 ** | −0.218 | −0.432 ** | 0.026 | −0.319 ** | −0.052 | −0.394 ** | ||||||
| 8. PDI (total) | 1 | 0.938 ** | 0.656 ** | 0.677 ** | 0.822 ** | 0.455 ** | 0.764 ** | 0.521 ** | −0.491 ** | −0.353 ** | −0.504 ** | −0.058 | −0.440 ** | −0.242 * | −0.510 ** | |||||||
| 9. Daily activities | 1 | 0.492 ** | 0.537 ** | 0.655 ** | 0.475 ** | 0.756 ** | 0.481 ** | −0.447 ** | −0.343 ** | −0.437 ** | −0.065 | −0.379 ** | −0.238 * | −0.458 ** | ||||||||
| 10. Work or school | 1 | 0.344 ** | 0.495 ** | 0.088 | 0.466 ** | 0.423 ** | −0.364 ** | −0.218 | −0.370 ** | −0.042 | −0.356 ** | −0.191 | −0.403 ** | |||||||||
| 11. Personal relationships | 1 | 0.591 ** | 0.148 | 0.572 ** | 0.410 ** | −0.439 ** | −0.293 * | −0.495 ** | −0.078 | −0.373 ** | −0.217 | −0.420 ** | ||||||||||
| 12. Leisure | 1 | 0.208 | 0.644 ** | 0.408** | −0.411 ** | −0.312 ** | −0.436 ** | −0.071 | −0.354 ** | −0.175 | −0.406 ** | |||||||||||
| 13. Treatment | 1 | 0.100 | 0.088 | −0.039 | 0.003 | −0.062 | 0.144 | −0.158 | 0.025 | −0.131 | ||||||||||||
| 14. Body image (total) | 1 | 0.540 ** | −0.615 ** | −0.417 ** | −0.570 ** | −0.194 | −0.532 ** | −0.341 ** | −0.607 ** | |||||||||||||
| 15. Acceptance Action (total) | 1 | −0.590 ** | −0.264 * | −0.540 ** | −0.172 | −0.625 ** | −0.347 ** | −0.654 ** | ||||||||||||||
| 16. Self-compassion (total) | 1 | 0.758 ** | 0.732 ** | 0.570 ** | 0.770 ** | 0.752 ** | 0.771 ** | |||||||||||||||
| 17. Self-kindness | 1 | 0.292 * | 0.657 ** | 0.261 * | 0.737 ** | 0.282 * | ||||||||||||||||
| 18. Self-judgment | 1 | 0.034 | 0.773 ** | 0.214 | 0.825 ** | |||||||||||||||||
| 19. Common Humanity | 1 | 0.133 | 0.622 ** | 0.043 | ||||||||||||||||||
| 20. Isolation | 1 | 0.370 ** | 0.864 ** | |||||||||||||||||||
| 21. Mindfulness | 1 | 0.379 ** | ||||||||||||||||||||
| 22. Over-identification | 1 |
| Model | R | R2 | R2 Adjusted | Standardized Error of the Estimate | R2 Change | F Change | df1 | df2 | Significant F Change |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 0.168 | 0.028 | 0.015 | 7.270 | 0.028 | 2.116 | 1 | 73 | 0.150 |
| 2 | 0.721 | 0.520 | 0.470 | 5.332 | 0.492 | 11.454 | 6 | 67 | <0.001 |
| 3 | 0.835 | 0.698 | 0.651 | 4.328 | 0.178 | 12.558 | 3 | 64 | <0.001 |
| B | Error | β | t | p | |||||
| 1 | (Constant) | 13.012 | 3.253 | −4.001 | <0.001 | ||||
| Years of education | −0.929 | 0.639 | −0.168 | −1.455 | 0.150 | ||||
| 2 | (Constant) | −2.256 | 4.275 | −0.528 | 0.599 | ||||
| Years of education | −0.889 | 0.474 | −0.160 | −1.874 | 0.065 | ||||
| Other diseases | −0.146 | 1.303 | −0.010 | −0.112 | 0.911 | ||||
| Family history of psoriasis | 1.790 | 1.271 | 0.122 | 1.408 | 0.164 | ||||
| Disease severity perception | −1.267 | 1.104 | −0.112 | −1.148 | 0.255 | ||||
| Satisfaction with treatment | −0.175 | 1.369 | −0.011 | −0.128 | 0.899 | ||||
| Anxiolytics/antidepressants | 1.307 | 1.491 | 0.079 | 0.877 | 0.384 | ||||
| Impact in social life | 6.182 | 0.830 | 0.719 | 7.452 | <0.001 | ||||
| 3 | (Constant) | −0.613 | 7.159 | −0.086 | 0.932 | ||||
| Years of education | −0.897 | 0.393 | −0.162 | −2.282 | 0.026 | ||||
| Other diseases | −1.590 | 1.102 | −0.108 | −1.443 | 0.154 | ||||
| Family history of psoriasis | 0.958 | 1.089 | 0.065 | 0.880 | 0.382 | ||||
| Disease severity perception | −0.963 | 0.903 | −0.085 | −1.067 | 0.290 | ||||
| Satisfaction with treatment | 0.984 | 1.144 | 0.062 | 0.861 | 0.393 | ||||
| Anxiolytics/antidepressants | 0.318 | 1.240 | 0.019 | 0.257 | 0.798 | ||||
| Impact in social life | 3.160 | 0.886 | 0.367 | 3.567 | 0.001 | ||||
| Body image (total) | 0.228 | 0.062 | 0.433 | 3.694 | <0.001 | ||||
| Acceptance Action (total) | 0.119 | 0.083 | 0.134 | 1.444 | 0.153 | ||||
| Self-compassion (total) | −0.039 | 0.048 | −0.083 | −0.799 | 0.427 | ||||
| Independent Variable | Mediator Variable | Dependent Variable | B Mean Indirect Effect | SE of Mean | 95% CI Mean Indirect Effect (Lower and Upper) | p |
|---|---|---|---|---|---|---|
| Disease severity perception | Body image | Psoriasis disability index | 0.035 | 0.004 | 0.028; 0.043 | <0.001 *** |
| Acceptance and action | 0.444 | 0.041 | 0.368; 0.530 | <0.001 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, V.; Leite, Â.; Constante, D.; Correia, R.; Almeida, I.F.; Teixeira, M.; Vidal, D.G.; Sousa, H.F.P.e.; Dinis, M.A.P.; Teixeira, A. The Mediator Role of Body Image-Related Cognitive Fusion in the Relationship between Disease Severity Perception, Acceptance and Psoriasis Disability. Behav. Sci. 2020, 10, 142. https://doi.org/10.3390/bs10090142
Almeida V, Leite Â, Constante D, Correia R, Almeida IF, Teixeira M, Vidal DG, Sousa HFPe, Dinis MAP, Teixeira A. The Mediator Role of Body Image-Related Cognitive Fusion in the Relationship between Disease Severity Perception, Acceptance and Psoriasis Disability. Behavioral Sciences. 2020; 10(9):142. https://doi.org/10.3390/bs10090142
Chicago/Turabian StyleAlmeida, Vera, Ângela Leite, Diana Constante, Rita Correia, Isabel Filipa Almeida, Maribel Teixeira, Diogo Guedes Vidal, Hélder Fernando Pedrosa e Sousa, Maria Alzira Pimenta Dinis, and Ana Teixeira. 2020. "The Mediator Role of Body Image-Related Cognitive Fusion in the Relationship between Disease Severity Perception, Acceptance and Psoriasis Disability" Behavioral Sciences 10, no. 9: 142. https://doi.org/10.3390/bs10090142
APA StyleAlmeida, V., Leite, Â., Constante, D., Correia, R., Almeida, I. F., Teixeira, M., Vidal, D. G., Sousa, H. F. P. e., Dinis, M. A. P., & Teixeira, A. (2020). The Mediator Role of Body Image-Related Cognitive Fusion in the Relationship between Disease Severity Perception, Acceptance and Psoriasis Disability. Behavioral Sciences, 10(9), 142. https://doi.org/10.3390/bs10090142