The Role of Family Relationships in Eating Disorders in Adolescents: A Narrative Review




Abstract
1. Introduction: Eating Disorders in Adolescence
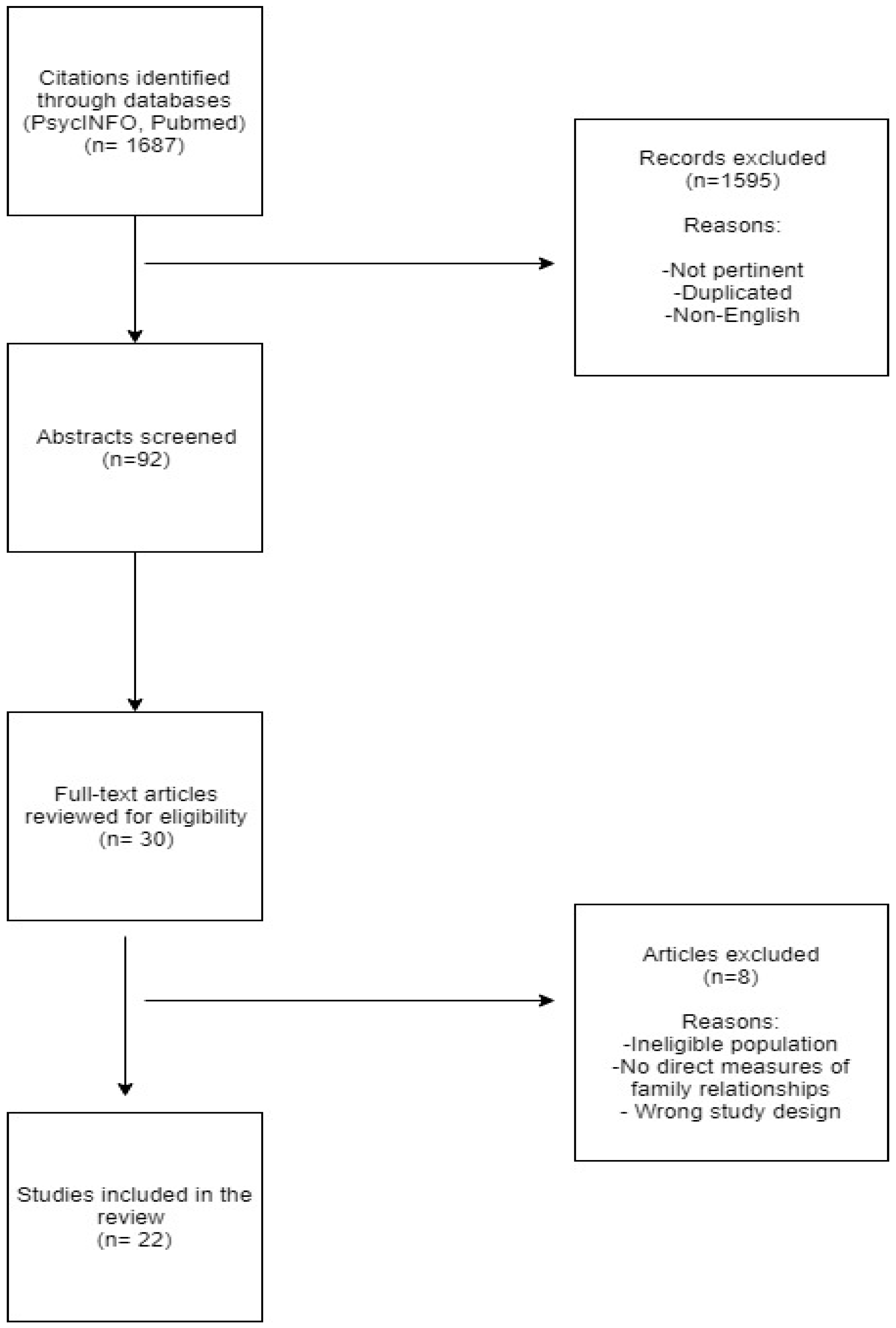
2. Methods
3. Theoretical Frameworks on Eating Disorders in Adolescence: A Reflection on Relational Aspects
3.1. First Theoretical and Clinical Contributions
3.1.1. The Theory of Family Systems: The Possible Influence of Family Environment on Offspring
3.1.2. The Relational-Systemic Paradigm: Family Relationships in Eating Disorders
4. Empirical Evidence of the Family Relationship in Eating Disorders: Synthesizing the Contributions
4.1. Results
4.1.1. Contemporary Approaches
4.1.2. An Empirical Relational-Systemic Perspective of Family Functioning
4.1.3. A Possible Integrate Perspective for Understanding Eating Disorders: Developmental Psychopathology and Relational Systemic Approach
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lask, B.; Bryant-Waugh, R. Eating Disorders in Childhood and Adolescence; Routledge: Abingdon, UK, 2013. [Google Scholar]
- Dalle Grave, R. Eating disorders: Progress and challenges. Eur. J. Intern. Med. 2011, 22, 153–160. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Harrison, P.J. Eating disorders. Lancet 2003, 361, 407–416. [Google Scholar] [CrossRef]
- Sigel, E. Eating Disorders. Adolesc. Med. State Art Rev. 2008, 19, 547–572. [Google Scholar]
- Treasure, J.; Schmidt, U.; Van Furth, E. Handbook of Eating Disorders; John Wiley & Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing, Inc.: Arlington County, VA, USA, 2013. [Google Scholar]
- Gowers, S.G.; North, C. Difficulties in family functioning and adolescent anorexia nervosa. Br. J. Psychiatry 1999, 174, 63–66. [Google Scholar] [CrossRef]
- Smink, F.R.; van Hoeken, D.; Hoek, H.W. Epidemiology, course, and outcome of eating disorders. Curr. Opin. Psychiatry 2013, 26, 543–548. [Google Scholar] [CrossRef]
- Smink, F.R.; van Hoeken, D.; Oldehinkel, A.J.; Hoek, H.W. Prevalence and severity of DSM-5 eating disorders in a community cohort of adolescents. Int. J. Eat. Disord. 2014, 47, 610–619. [Google Scholar] [CrossRef]
- Treasure, J.; Duarte, T.A.; Schmidt, U. Eating disorders. Lancet 2020. [Google Scholar] [CrossRef]
- Crone, E.A.; Dahl, R.E. Understanding adolescence as a period of social–affective engagement and goal flexibility. Nat. Rev. Neurosci. 2012, 13, 636–650. [Google Scholar] [CrossRef]
- Mitchison, D.; Mond, J.; Bussey, K.; Griffiths, S.; Trompeter, N.; Lonergan, A.; Pike, K.M.; Murray, S.B.; Hay, P. DSM-5 full syndrome, other specified, and unspecified eating disorders in Australian adolescents: prevalence and clinical significance. Psychol. Med. 2019, 1–10. [Google Scholar] [CrossRef]
- Pearson, C.M.; Zapolski, T.C.B.; Smith, G.T.A. Longitudinal test of impulsivity and depression pathways to early binge eating onset. Int. J. Eat. Disord. 2015, 48, 230–237. [Google Scholar] [CrossRef]
- Ammaniti, M.; Sergi, G. Clinical dynamics during adolescence: Psychoanalytic and attachment perspectives. Psychoanal. Inq. 2003, 23, 54–80. [Google Scholar] [CrossRef]
- Ammaniti, M.; Speranza, A.M.; Tambelli, R.; Muscetta, S.; Lucarelli, L.; Vismara, L.; Odorisio, F.; Cimino, S. A prevention and promotion intervention program in the field of mother–infant relationship. Child Adolesc. Soc. Work J. 2006, 27, 70–90. [Google Scholar] [CrossRef]
- Sameroff, A.J.; McDonough, S.C.; Rosenblum, K. Treating Parent—Infant Relationship Problems: Strategies for Intervention; Guilford Press: New York, NY, USA, 2004. [Google Scholar]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behav. Res. Ther. 2003, 41, 509–528. [Google Scholar] [CrossRef]
- Kaye, W.H.; Wagner, A.; Fudge, J.L.; Paulus, M. Neurocircuity of Eating Disorders. In Behavioral Neurobiology of Eating Disorders; Springer: Berlin/Heidelberg, Germany, 2010; pp. 37–57. [Google Scholar]
- Walsh, B.T.; Devlin, M.J. Eating disorders: Progress and problems. Science 1998, 280, 1387–1390. [Google Scholar] [CrossRef]
- Levine, M.; Smolak, L. Toward a Model of the Developmental Psychopathology of Eating Disorders: The Example of Early Adolescence. In The Etiology of Bulimia Nervosa: The Individual and Familial Context; Taylor & Francis: Abingdon, UK, 2013; pp. 59–80. [Google Scholar]
- Amianto, F.; Abbate-Daga, G.; Morando, S.; Sobrero, C.; Fassino, S. Personality development characteristics of women with anorexia nervosa, their healthy siblings and healthy controls: What prevents and what relates to psychopathology? Psychiatry Res. 2011, 187, 401–408. [Google Scholar] [CrossRef]
- Berge, J.M.; Wall, M.; Larson, N.; Eisenberg, M.E.; Loth, K.A.; Neumark-Sztainer, D. The unique and additive associations of family functioning and parenting practices with disordered eating behaviors in diverse adolescents. J. Behav. Med. 2014, 37, 205–217. [Google Scholar] [CrossRef]
- Berge, J.M.; Wall, M.; Loth, K.; Neumark-Sztainer, D. Parenting style as a predictor of adolescent weight and weight-related behaviors. J. Adolesc. Health 2010, 46, 331–338. [Google Scholar] [CrossRef]
- Holtom-Viesel, A.; Allan, S. A systematic review of the literature on family functioning across all eating disorder diagnoses in comparison to control families. Clin. Psychol. Rev. 2014, 34, 29–43. [Google Scholar] [CrossRef]
- Langdon-Daly, J.; Serpell, L. Protective factors against disordered eating in family systems: A systematic review of research. J. Eat. Disord. 2017, 5, 12. [Google Scholar] [CrossRef]
- Tambelli, R.; Cimino, S.; Cerniglia, L.; Ballarotto, G. Early maternal relational traumatic experiences and psychopathological symptoms: A longitudinal study on mother-infant and father-infant interactions. Sci. Rep. 2015, 5, 13984. [Google Scholar] [CrossRef]
- Bateson, G. Steps to An Ecology of Mind: Collected Essays in Anthropology, Psychiatry, Evolution, and Epistemology; University of Chicago Press: Chicago, IL, USA, 2000. [Google Scholar]
- Bowen, M. Toward the Differentiation of Self in One’s Family of Origin, Family Therapy in Clinical Practice; Jason Aronson: New York, NY, USA, 1974. [Google Scholar]
- Hoffman, L. Beyond power and control: Toward a ‘second order’ family systems therapy. Fam. Syst. Med. 1985, 4, 381–396. [Google Scholar] [CrossRef]
- Ackerman, N.W. The growing edge of family therapy. Fam. Process 1971, 10, 143–156. [Google Scholar] [CrossRef]
- Haley, J. Family therapy. Int. J. Psychiatry 1970, 9, 233–242. [Google Scholar] [PubMed]
- Minuchin, S.; Rosman, B.; Baker, L. Psychosomatic Families: Anorexia Nervosa in Context; Harvard University Press: Cambridge, MA, USA, 1978. [Google Scholar]
- Selvini Palazzoli, M.; Viaro, M. The anorectic process in the family: A six-stage model as a guide for individual therapy. Fam. Process 1988, 27, 129–148. [Google Scholar] [CrossRef] [PubMed]
- Selvini, M.P. Towards a general model of psychotic family games. J. Marital Fam. 1986, 12, 339–349. [Google Scholar] [CrossRef]
- Von Bertalanffy, L. An outline of general system theory. Br. J. Philos. Sci. 1950, 1, 134–165. [Google Scholar] [CrossRef]
- Aragona, M.; Catapano, R.; Loriedo, C.; Alliani, D. The psychosomatic family system: Are families with Eating Disorders more enmeshed and rigid than normal controls? Dialogues Philos. Ment. Neuro Sci. 2011, 4, 10–15. [Google Scholar]
- Grasso, M.; Nazzaro, F.; Vona, L.; Capacchione, G.; Loriedo, C. Maturity fears and weight phobia in eating disorders: Research of a relationship. Rivista di Psichiatria 2012, 47, 319–326. [Google Scholar]
- Cerniglia, L.; Cimino, S.; Ballarotto, G. Mother and father-child interaction with their 24-month-old children during feeding, considerino paternal involvement and the child’s temperament in a community sample. Infant Men. Health J. 2014, 35, 473–481. [Google Scholar] [CrossRef]
- Le Grange, D.; Lock, J.; Loeb, K.; Nicholls, D. Academy for eating disorders position paper: The role of the family in eating disorders. Int. J. Eat. Disord. 2010, 43, 1–5. [Google Scholar] [CrossRef]
- Minuchin, S. Families and Family Therapy; Harvard University Press: Cambridge, MA, USA, 1974. [Google Scholar]
- Andolfi, M. Engaging fathers in family therapy with violent adolescents. Aust. N. Z. J. Fam. Ther. 2013, 34, 172–185. [Google Scholar] [CrossRef]
- Leung, J.T.; Shek, D.T. Parent–adolescent discrepancies in perceived parenting characteristics and adolescent developmental outcomes in poor Chinese families. J. Child Fam. Stud. 2014, 23, 200–213. [Google Scholar] [CrossRef] [PubMed]
- Boscolo, L.; Cecchin, G. Training in Systemic Therapy at the Milan Centre. In Family Therapy Supervision: Recent Developments in Practice; Psychological Corp: New York, NY, USA, 1982; pp. 153–165. [Google Scholar]
- Selvini Palazzoli, M. Anorexia nervosa: A syndrome of the affluent society. J. Strateg. Syst. Ther. 1985, 4, 12–16. [Google Scholar]
- Selvini, M.P.; Boscolo, L.; Cecchin, G.; Prata, G. Hypothesizing-circularity-neutrality: Three guidelines for the conductor of the session. Fam. Process 1980, 19, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Stierlin, H.; Weber, G. Unlocking the Family Door: A Systemic Approach to the Understanding and Treatment of Anorexia Nervosa; Brunner/Mazel Publishers, Inc.: New York, NY, USA, 1989. [Google Scholar]
- Gómez-López, M.; Viejo, C.; Ortega-Ruiz, R. Well-Being and Romantic Relationships: A Systematic Review in Adolescence and Emerging Adulthood. Int. J. Environ. Res. Public Health 2019, 16, 2415. [Google Scholar] [CrossRef] [PubMed]
- Herpertz-Dahlmann, B.; Seitz, J.; Konrad, K. Aetiology of anorexia nervosa: From a “psychosomatic family model” to a neuropsychiatric disorder? Eur. Arch. Psychiatry Clin. Neurosci. 2011, 261, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Watzlawick, P.; Bavelas, J.B.; Jackson, D.D. Pragmatics of Human Communication: A Study of Interactional Patterns, Pathologies and Paradoxes; WW Norton & Company: New York, NY, USA, 2011. [Google Scholar]
- Gillett, K.S.; Harper, J.M.; Larson, J.H.; Berrett, M.E.; Hardman, R.K. Implicit Family Process Rules in Eating-Disordered and Non-Eating-Disordered Families. J. Marital Fam. Ther. 2009, 35, 159–174. [Google Scholar] [CrossRef]
- Sim, L.A.; Homme, J.H.; Lteif, A.N.; VandeVoort, J.L.; Schak, K.M.; Ellingson, J. Family functioning and maternal distress in adolescent girls with anorexia nervosa. Int. J. Eat. Disord. 2009, 42, 531–539. [Google Scholar] [CrossRef]
- Hayaki, J. Negative reinforcement eating expectancies, emotion dysregulation, and symptoms of bulimia nervosa. Int. J. Eat. Disord. 2009, 42, 552–556. [Google Scholar] [CrossRef]
- Haines, J.; Rifas-Shiman, S.L.; Horton, N.J.; Kleinman, K.; Bauer, K.W.; Davison, K.K.; Walton, K.; Austin, S.B.; Field, A.E.; Gillman, M.W. Family functioning and quality of parent-adolescent relationship: cross-sectional associations with adolescent weight-related behaviors and weight status. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 68. [Google Scholar] [CrossRef]
- Tafà, M.; Marzilli, E.; Cimino, S.; Cerniglia, L.; Bracaglia, F. Anorexic families and bulimic families: Psychopathological risk and family functioning. Rassegna di Psicologia 2017, 34, 5–23. [Google Scholar]
- Visani, E.; Orrù, C.; Zullo, D.; Loriedo, C. Stili di Funzionamento Delle Famiglie con una Persona con Disturbi del Comportamento Alimentare. In Faces IV. Il Modello Circonflesso di Olson Nella Clinica e Nella Ricerca; Visani, E., di Nuovo, S., Loriedo, C., Eds.; Franco Angeli: Milano, Italy, 2014; pp. 101–113. [Google Scholar]
- Lyke, J.; Matsen, J. Family functioning and risk factors for disordered eating. Eat. Behav. 2013, 14, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Goossens, L.; Braet, C.; Van Durme, K.; Decaluwé, V.; Bosmans, G. The parent–child relationship as predictor of eating pathology and weight gain in preadolescents. J. Clin. Child Adolesc. Psychol. 2012, 41, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Laghi, F.; Pallini, S.; D’Alessio, M.; Baiocco, R. Development and validation of the Efficacious Self-Presentation Scale. J. Genet. Psychol. 2011, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hasenboehler, K.; Munsch, S.; Meyer, A.H.; Kappler, C.; Vögele, C. Family structure, body mass index, and eating behavior. Int. J. Eat. Disord. 2009, 42, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Story, M.; Sherwood, N.E. Five-year longitudinal predictive factors for disordered eating in a population-based sample of overweight adolescents: Implications for prevention and treatment. Int. J. Eat. Disord. 2009, 42, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Laghi, F.; McPhie, M.L.; Baumgartner, E.; Rawana, J.S.; Pompili, S.; Baiocco, R. Family functioning and dysfunctional eating among Italian adolescents: The moderating role of gender. Child Psychiatry Hum. Dev. 2016, 47, 43–52. [Google Scholar] [CrossRef]
- Fisher, M.; Bushlow, M. Perceptions of family styles by adolescents with eating disorders and their parents. Int. J. Addol. Med. 2015, 27, 443–449. [Google Scholar] [CrossRef]
- Haycraft, E.; Goodwin, H.; Meyer, C. Adolescents’ level of eating psychopathology is related to perceptions of their parents’ current feeding practices. J. Adolesc. Health 2014, 54, 204–208. [Google Scholar] [CrossRef]
- Micali, N.; Ploubidis, G.; De Stavola, B.; Simonoff, E.; Treasure, J. Frequency and patterns of eating disorder symptoms in early adolescence. J. Adolesc. Health 2014, 54, 574–581. [Google Scholar] [CrossRef]
- Horesh, N.; Sommerfeld, E.; Wolf, M.; Zubery, E.; Zalsman, G. Father–daughter relationship and the severity of eating disorders. Eur. Psychiatry 2015, 30, 114–120. [Google Scholar] [CrossRef]
- Pilecki, M.W.; Józefik, B. Perception of transgenerational family relationships: Comparison of eating-disordered patients and their parents. Med. Sci. Monit. 2013, 19, 1114–1124. [Google Scholar] [CrossRef] [PubMed]
- Ciao, A.C.; Accurso, E.C.; Fitzsimmons-Craft, E.E.; Le Grange, D. Predictors and moderators of psychological changes during the treatment of adolescent bulimia nervosa. Behav. Res. 2015, 69, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Dare, C.; Le Grange, D.; Eisler, I.; Rutherford, J. Redefining the psychosomatic family: Family process of 26 eating disorder families. Int. J. Eat. Disord. 1994, 16, 211–226. [Google Scholar] [CrossRef]
- Casper, R.C.; Troiani, M. Family functioning in anorexia nervosa differs by subtype. Int. J. Eat. Disord. 2001, 30, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Emanuelli, F.; Ostuzzi, R.; Cuzzolaro, M.; Baggio, F.; Lask, B.; Waller, G. Family functioning in adolescent anorexia nervosa: A comparison of family members’ perceptions. Eat. Weight Disord. 2004, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mcdermott, B.M.; Batik, M.; Roberts, L.; Gibbon, P. Parent and child report of family functioning in a clinical child and adolescent eating disorders sample. Aust. N. Z. J. Psychiatry 2002, 36, 509–514. [Google Scholar] [CrossRef]
- Shisslak, C.M.; McKeon, R.T.; Crago, M. Family dysfunction in normal weight bulimic and bulimic anorexic families. J. Clin. Psychol. 1990, 46, 185–189. [Google Scholar] [CrossRef]
- Kog, E.; Vandereycken, W. Family interaction in eating disorder patients and normal controls. Int. J. Eat. Disord. 1989, 8, 11–23. [Google Scholar] [CrossRef]
- Szabo, C.P.; Goldin, J.; Le Grange, D. Application of the family relations scale to a sample of anorexics, bulimics and non-psychiatric controls: A preliminary study. Eur. Eat. Disord. Rev. 1999, 7, 37–46. [Google Scholar] [CrossRef]
- Wooldridge, T.; Lytle, P.P. An overview of anorexia nervosa in males. Eat. Disord. 2012, 20, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Zucker, N.; Moskovich, A.; Vinson, M.; Watson, K. Emotions and Empathic Understanding: Capitalizing on Relationships in Those with Eating Disorders. In A Collaborative Approach to Eating Disorders; Alexander, J., Treasure, J., Eds.; Routledge: New York, NY, USA, 2013; pp. 52–61. [Google Scholar]
- Paciello, M.; Fida, R.; Tramontano, C.; Cole, E.; Cerniglia, L. Moral dilemma in adolescence: The role of values, prosocial moral reasoning and moral disengagement in helping decision making. Eur. J. Dev. Psychol. 2013, 10, 190–205. [Google Scholar] [CrossRef]
- Schmidt, U.; Treasure, J. Anorexia nervosa: Valued and visible. A cognitive-interpersonal maintenance model and its implications for research and practice. Br. J. Clin. Psychol. 2006, 45, 343–366. [Google Scholar] [CrossRef] [PubMed]
- Sroufe, L.A.; Rutter, M. The domain of developmental psychopathology. Child Dev. 1984, 55, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, P.E.; Garner, D.M. Anorexia Nervosa: A Multidimensional Approach; Brunner/Mazel: New York, NY, USA, 1982. [Google Scholar]
- Lau, W.C.; Rafii, M.Y.; Ismail, M.R.; Puteh, A.; Latif, M.A.; Ramli, A. Review of functional markers for improving cooking, eating, and the nutritional qualities of rice. Front. Plant Sci. 2015, 6, 832. [Google Scholar] [CrossRef]
- Henry, C.S.; Robinson, L.C.; Neal, R.A.; Huey, E.L. Adolescent perceptions of overall family system functioning and parental behaviors. J. Child Fam. Stud. 2006, 15, 308–318. [Google Scholar] [CrossRef]
- Olson, D.H.; Sprenkle, D.H.; Russell, C.S. Circumplex model of marital and family systems: I. Cohesion and adaptability dimensions, family types, and clinical applications. Fam. Process 1979, 18, 3–28. [Google Scholar] [CrossRef]
- Olson, D.H. Circumplex Model of family systems: VIII. Family assessment and intervention. J. Fam. Psychother. 1988, 4, 7–49. [Google Scholar]
- Olson, D.H. Circumplex model of marital and family sytems. J. Fam. Psychother. 2000, 22, 144–167. [Google Scholar]
- Olson, D. FACES IV and the circumplex model: Validation study. J. Marital Fam. 2011, 37, 64–80. [Google Scholar] [CrossRef]
- Olson, D.H.; Gorall, D.M. Faces IV and the Circumplex Model; Life Innovations: Minneapolis, MN, USA, 2006. [Google Scholar]
- Kluck, A.S. Family factors in the development of disordered eating: Integrating dynamic and behavioral explanations. Eat. Behav. 2008, 9, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Vidović, V.; Jures, V.; Begovac, I.; Mahnik, M.; Tocilj, G. Perceived family cohesion, adaptability and communication in eating disorders. Eur. Eat. Disord. Rev. 2005, 3, 19–28. [Google Scholar] [CrossRef]
- Hoste, R.R.; Hewell, K.; Le Grange, D. Family interaction among white and ethnic minority adolescents with bulimia nervosa and their parents. Eur. Eat. Disord. Rev. 2007, 15, 152–158. [Google Scholar] [CrossRef]
- Steinhausen, H.C.; Gavez, S.; Winkler Metzke, C. Psychosocial correlates, outcome, and stability of abnormal adolescent eating behavior in community samples of young people. Int. J. Eat. Disord. 2005, 37, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Schuetzmann, M.; Richter-Appelt, H.; Schulte-Markwort, M.; Schimmelmann, B.G. Associations among the perceived parent–child relationship, eating behavior, and body weight in preadolescents: Results from a community-based sample. J. Pediatr. Psychol. 2008, 33, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Laghi, F.; Baiocco, R.; Ghezzi, E.; Cacioppo, M. Family functioning and eating disorders in adolescence. Counselling 2012, 5, 55–69. [Google Scholar]
- Croll, J.; Neumark-Sztainer, D.; Story, M.; Ireland, M. Prevalence and risk and protective factors related to disordered eating behaviors among adolescents: Relationship to gender and ethnicity. J. Adolesc. Health 2002, 31, 166–175. [Google Scholar] [CrossRef]
- Wisotsky, W.; Dancyger, I.; Fornari, V.; Katz, J.; Wisotsky, W.L.; Swencionis, C. The relationship between eating pathology and perceived family functioning in eating disorder patients in a day treatment program. Eat. Disord. 2003, 11, 89–99. [Google Scholar] [CrossRef]
- Pauls, B.S.; Daniels, T. Relationship among Family, Peer Networks and Bulimic Symptomatology in College Women. Can. J. Couns. 2000, 34, 260–272. [Google Scholar]
- Stice, E.; Agras, W.S. Predicting onset and cessation of bulimic behaviors during adolescence: A longitudinal grouping analysis. Behav. Ther. 1998, 29, 257–276. [Google Scholar] [CrossRef]
- Van den Berg, P.; Thompson, J.K.; Obremski-Brandon, K.; Coovert, M. The tripartite influence model of body image and eating disturbance: A covariance structure modeling investigation testing the mediational role of appearance comparison. J. Psychosom. Res. 2002, 53, 1007–1020. [Google Scholar] [CrossRef]
- Laghi, F.; Pompili, S.; Zanna, V.; Castiglioni, M.C.; Criscuolo, M.; Chianello, I.; Mazzoni, S.; Baiocco, R. How adolescents with anorexia nervosa and their parents perceive family functioning? J. Health Psychol. 2016, 22, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Baiocco, R.; Cacioppo, M.; Laghi, F.; Tafà, M. Factorial and construct validity of FACES IV among Italian adolescents. J. Child. Fam. Stud. 2013, 22, 962–970. [Google Scholar] [CrossRef]
- Laliberté, M.; Boland, F.J.; Leichner, P. Family climates: Family factors specific to disturbed eating and bulimia nervosa. J. Clin. Psychol. 1999, 55, 1021–1040. [Google Scholar] [CrossRef]
- Dancyger, I.; Fornari, V.; Scionti, L.; Wisotsky, W.; Sunday, S. Do daughters with eating disorders agree with their parents’ perception of family functioning? Compr. Psychiatry 2005, 46, 135–139. [Google Scholar] [CrossRef]
- Cicchetti, D. The emergence of developmental psychopathology. Child Dev. 1984, 55, 1–7. [Google Scholar] [CrossRef]
- Cummings, E.M.; Davies, P.T.; Campbell, S.B. New directions in the study of parenting and child development. Dev. Psychopathol. Fam. Process 2000, 71, 205–211. [Google Scholar]
- Mikulincer, M.; Shaver, P.R.; Pereg, D. Attachment theory and affect regulation: The dynamics, development, and cognitive consequences of attachment-related strategies. Motiv. Emot. 2003, 27, 77–102. [Google Scholar] [CrossRef]
- Cook-Darzens, S.; Doyen, C.; Falissard, B.; Mouren, M.C. Self-perceived family functioning in 40 French families of anorexic adolescents: Implications for therapy. Eur. Eat. Disord. Rev. 2005, 13, 223–236. [Google Scholar] [CrossRef]
- Bearman, S.K.; Presnell, K.; Martinez, E.; Stice, E. The skinny on body dissatisfaction: A longitudinal study of adolescent girls and boys. J. Youth Adolesc. 2006, 35, 217–229. [Google Scholar] [CrossRef]
- Blodgett Salafia, E.H.; Gondoli, D.M.; Corning, A.F.; McEnery, A.M.; Grundy, A.M. Psychological distress as a mediator of the relation between perceived maternal parenting and normative maladaptive eating among adolescent girls. J. Couns. Psychol. 2007, 54, 434. [Google Scholar] [CrossRef]
- Creswell, C.; Cooper, P.J.; Murray, L. Parents with Anxiety Disorders. In Parental Psychiatric Disorder: Distressed Parents and Their Families; Cambridge University Press: Cambridge, UK, 2015; pp. 127–137. [Google Scholar]
- Madigan, S.; Moran, G.; Schuengel, C.; Pederson, D.R.; Otten, R. Unresolved maternal attachment representations, disrupted maternal behavior and disorganized attachment in infancy: Links to toddler behavior problems. J. Child Psychol. Psychiatry 2007, 48, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Verkuijl, N.E.; Richter, L.; Norris, S.A.; Stein, A.; Avan, B.; Ramchandani, P.G. Postnatal depressive symptoms and child psychological development at 10 years: A prospective study of longitudinal data from the South African Birth to Twenty cohort. Lancet Psychiatry 2014, 1, 454–460. [Google Scholar] [CrossRef]
- Crandall, A.; Deater-Deckard, K.; Riley, A.W. Maternal emotion and cognitive control capacities and parenting: A conceptual framework. Dev. Rev. 2015, 36, 105–126. [Google Scholar] [CrossRef]
- Engen, H.G.; Singer, T. Compassion-based emotion regulation up-regulates experienced positive affect and associated neural networks. Soc. Cogn. Affect. Neur. 2015, 10, 1291–1301. [Google Scholar] [CrossRef]
- Cimino, S.; Cerniglia, L.; Paciello, M. Mothers with depression, anxiety or eating disorders: Outcomes on their children and the role of paternal psychological profiles. Child Psychiatry Hum. Dev. 2015, 46, 228–236. [Google Scholar] [CrossRef]
- Cooper, P.J.; Murray, L.; Halligan, S.L. Treatment of Postpartum Depression. In Encyclopedia on Early Childhood Development; Tremblay, R., Barr, R., Peters, R., Boivin, M., Eds.; Centre of Excellence for Early Childhood Development: Montreal, QC, Canada, 2010; Available online: http://centaur.reading.ac.uk/17495 (accessed on 21 January 2020).
- Cimino, S.; Cerniglia, L.; Paciello, M.; Sinesi, S. A six-year prospective study on children of mothers with eating disorders: The role of paternal psychological profiles. Eur. Eat. Disord. Rev. 2013, 21, 238–246. [Google Scholar] [CrossRef]
- Erol, A.; Yazici, F.; Toprak, G. Family functioning of patients with an eating disorder compared with that of patients with obsessive compulsive disorder. Compr. Psychiatry 2007, 48, 47–50. [Google Scholar] [CrossRef]
- Woodside, D.B.; Swinson, R.P.; Kuch, K.; Heinmaa, M. Family functioning in anxiety and eating disorders—A comparative study. Compr. Psychiatry 1996, 37, 139–143. [Google Scholar] [CrossRef]
- Academy for Eating Disorders. Worldwide Charter for Action on Eating Disorders. Rights and Expectations for People with Eating Disorders and Their Families. 2008. Available online: http://www.aedweb.org/documents/WWCharter3.pdf (accessed on 21 January 2020).


{kind=link}
| Study | Year | Design | Country | Sample Size | Type of Sample | Age Range (Years) | Investigated Family Issues | Main Results |
|---|---|---|---|---|---|---|---|---|
| Berge et al. [22] | 2014 | C | USA | N = 2793 | R | 11–19 | Family functioning and parenting practices | Parental psychological control moderated the protective relationship between family functioning and disordered eating behaviors in adolescent girls |
| Berge et al. [23] | 2010 | C | USA | N = 2516 | R | 13–18 | Family relationships and parental style | Authoritative parenting style may play a protective role related to adolescent overweight |
| Aragona et al. [36] | 2011 | C | Italy | N = 60 | CL | 13–18 | Family functioning (adaptability and cohesion) and psychopathological symptoms | High levels of cohesion were found in families with adolescents with eating disorders (hyper-involvement of family members) |
| Leung and Shek [42] | 2014 | C | China | N = 275 | HR | 11–16 | Family relationships (parent–adolescent; parental responsiveness and control) | Adolescents generally perceived lower levels of parenting behaviors than did their parents |
| Gillett et al. [50] | 2009 | C | USA | N = 102 | CL | 14–20 | Family process rules (kindness; expressiveness and connection; constraining thoughts, feelings, and self; inappropriate caretaking; and monitoring | Eating-disordered youth reported a lower proportion of facilitative family rules and a higher proportion of constraining family rules than did parents and siblings |
| Sim et al. [51] | 2009 | C | USA | N = 55 | CL | 14–18 | Family functioning and psychological symptoms | Families of girls with AN experienced greater family conflict, reduced parental alliance, and increased feelings of depression |
| Hayaki [52] | 2009 | C | USA | N = 115 | HR | 16–20 | Family situation and emotion dysregulation (alexithymia and experiential avoidance) | Individuals who expect eating to provide emotional relief may be especially susceptible to disordered eating (bulimia nervosa) |
| Haines et al. [53] | 2016 | C | Canada | N = 3768 | R | 14–24 | Family functioning and quality of mother- and father-adolescent relationship | High family functioning was associated with lower odds of disordered eating |
| Tafà et al. [54] | 2017 | C | Italy | N = 90 | CL | 13–15 | Family functioning (adaptability and cohesion) and psychopathological symptoms | Anorexic families show a maladaptive functioning and anorexic adolescents present intense psychopathological disturbances |
| Visani et al. [55] | 2014 | C | Italy | N = 35 | CL | 14–17 | Family functioning (adaptability and cohesion) and psychopathological symptoms | Families with female adolescents with eating disorders report a problematic family functioning, with anorexic daughters showing severe psychopathological symptoms |
| Lyke and Matsen [56] | 2013 | C | USA | N = 91 | R | 14–18 | Family functioning (problem-solving, communication, roles, affective involvement, or behavior control) | Unhealthy general functioning predicted adolescent problems |
| Goossens et al. [57] | 2012 | L | Belgium | N = 601 | R | 10–12 | Parent-child relationship (parental style and attachment) | Longitudinal association between parent-child relationships and eating pathology and weight gain in preadolescents. |
| Laghi et al. [58] | 2012 | P | Italy | N = 438 | R | 14–18 | Family functioning (adaptability and cohesion) and psychopathological symptoms | Family functioning predicts risk factors of eating disorders (binge eating disorder) |
| Hasenboehler et al. [59] | 2009 | C | Switzerland | N = 57 | R | 10–12 | Family structures (hierarchy, conflict, restrained eating) | Family structure is associated with overweight and with eating behavior |
| Neumark-Sztainer et al. [60] | 2009 | L | USA | N = 412 | HR | 14–18 | Family structures (family connectedness, body satisfaction, regular meals) | Family connectedness represents a protective factor for disordered eating among overweight adolescents |
| Laghi et al. [61] | 2017 | C | Italy | N = 72 | CL | Mean age 14.86 years | Family functioning (adaptability and cohesion) | Girls with anorexia nervosa poor satisfaction about family environment and rated their families as less communicative, flexible, cohesive, and more disengaged |
| Fisher and Bushlow [62] | 2015 | C | USA | N = 44 | CL | 14–18 | Family functioning (adaptability and cohesion) | A great majority of patients and parents reported their families as being connected/very connected |
| Haycraft et al. [63] | 2014 | C | UK | N = 528 | R | 13–15 | Family situation (perceptions of parental feeding practices) | An intense perceived pressure from parents to eat food and lower perceived parental responsibility for food are related to more unhealthy eating-related attitudes in female adolescents |
| Micali et al. [64] | 2014 | L | UK | N = 7082 | R | 13–15 | Family burden and psychological symptoms | An extreme level of fear of weight gain, avoidance of fattening foods, and distress about weight and shape were common among girls |
| Horesh et al. [65] | 2015 | C | Israel | N = 86 | R | 13–16 | Parent-child relationship (father-daughter relationship; parental style: bonds and protection) | A negative perception of the father’s parenting style is associated with eating disorders and depressive symptoms |
| Pilecki and Józefik [66] | 2013 | C | Poland | N = 112 | CL | 13–20 | Intergenerational family relationship (autonomy, intimacy) | A relevant association between daughters’ and fathers’ perceptions of autonomy in their families of origin was found (transgenerational transmission of autonomy and intimacy in eating disorders) |
| Ciao et al. [67] | 2015 | P | USA | N = 80 | CL | 15–18 | Family-based treatment and supportive psychotherapy | Treatments were found to be efficacious with respect to bulimic symptoms |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erriu, M.; Cimino, S.; Cerniglia, L. The Role of Family Relationships in Eating Disorders in Adolescents: A Narrative Review. Behav. Sci. 2020, 10, 71. https://doi.org/10.3390/bs10040071
Erriu M, Cimino S, Cerniglia L. The Role of Family Relationships in Eating Disorders in Adolescents: A Narrative Review. Behavioral Sciences. 2020; 10(4):71. https://doi.org/10.3390/bs10040071
Chicago/Turabian StyleErriu, Michela, Silvia Cimino, and Luca Cerniglia. 2020. "The Role of Family Relationships in Eating Disorders in Adolescents: A Narrative Review" Behavioral Sciences 10, no. 4: 71. https://doi.org/10.3390/bs10040071
APA StyleErriu, M., Cimino, S., & Cerniglia, L. (2020). The Role of Family Relationships in Eating Disorders in Adolescents: A Narrative Review. Behavioral Sciences, 10(4), 71. https://doi.org/10.3390/bs10040071