LDLR Gene Polymorphisms (rs5925 and rs1529729) Are Associated with Susceptibility to Coronary Artery Disease in a South Indian Population


Abstract
1. Introduction
2. Subjects and Methods
2.1. Collection of Blood Samples and Clinical History
2.2. Extraction of DNA
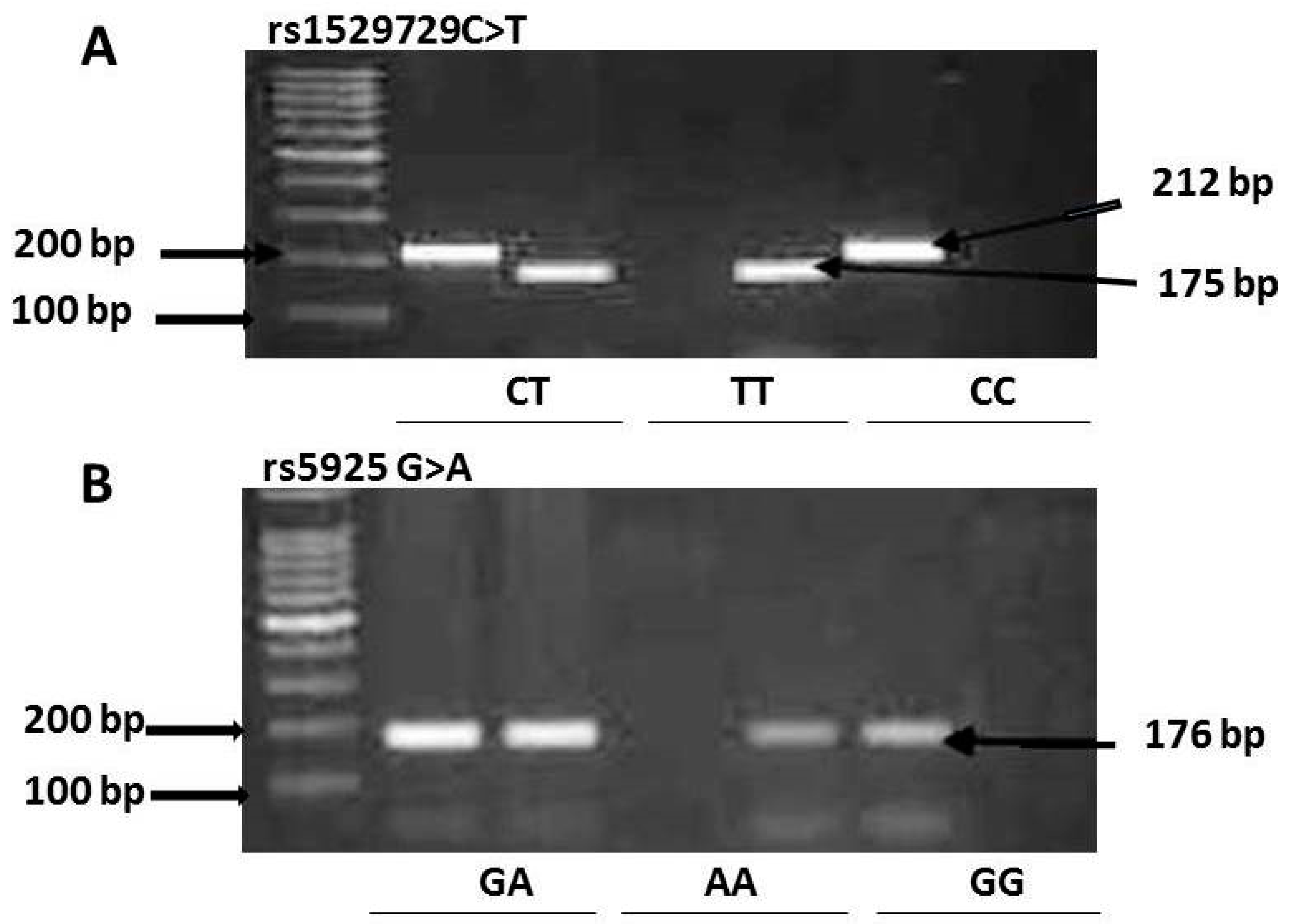
2.3. Genotyping of the LDLR Polymorphisms (rs5925 and rs1529729)
2.4. Statistical Analysis
3. Results
3.1. The Genotype Frequency of the LDLR Polymorphisms rs1529729 and rs5925
3.2. rs1529729 C > T and rs5925 G > A Polymorphisms Were Associated with CAD
4. Discussion
4.1. Association of rs1529729 C > T and rs5925 G > A Genotypes with CAD
4.2. The Frequency of the rs5925 and rs1529729 Polymorphisms in Different Populations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De Rosa, S.; Arcidiacono, B.; Chiefari, E.; Brunetti, A.; Indolfi, C.; Foti, D.P. Type 2 Diabetes Mellitus and Cardiovascular Disease: Genetic and Epigenetic Links. Front. Endocrinol. (Lausanne) 2018, 9, 2. [Google Scholar] [CrossRef] [PubMed]
- Fioranelli, M.; Bottaccioli, A.G.; Bottaccioli, F.; Bianchi, M.; Rovesti, M.; Roccia, M.G. Stress and Inflammation in Coronary Artery Disease: A Review Psychoneuroendocrineimmunology-Based. Front. Immunol. 2018, 9, 2031. [Google Scholar] [CrossRef] [PubMed]
- Lusis, A.J. Genetics of atherosclerosis. Trends Genet. 2012, 28, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Manduteanu, I.; Simionescu, M. Inflammation in atherosclerosis: A cause or a result of vascular disorders? J. Cell. Mol. Med. 2012, 16, 1978–1990. [Google Scholar] [CrossRef] [PubMed]
- Tousoulis, D.; Oikonomou, E.; Economou, E.K.; Crea, F.; Kaski, J.C. Inflammatory cytokines in atherosclerosis: Current therapeutic approaches. Eur. Heart J. 2016, 37, 1723–1732. [Google Scholar] [CrossRef] [PubMed]
- Van De Sluis, B.; Wijers, M.; Herz, J. News on the molecular regulation and function of hepatic low-density lipoprotein receptor and LDLR-related protein 1. Curr. Opin. Lipidol. 2017, 28, 241–247. [Google Scholar] [CrossRef]
- Abisambra, J.F.; Fiorelli, T.; Padmanabhan, J.; Neame, P.; Wefes, I.; Potter, H. LDLR expression and localization are altered in mouse and human cell culture models of Alzheimer’s disease. PLoS ONE 2010, 5, e8556. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, K.L.; Ruan, X.Z.; Liu, B.C. Dysregulation of the Low-Density Lipoprotein Receptor Pathway Is Involved in Lipid Disorder-Mediated Organ Injury. Int. J. Biol. Sci. 2016, 12, 569–579. [Google Scholar] [CrossRef]
- Nikolic, J.; Belot, L.; Raux, H.; Legrand, P.; Gaudin, Y.; Albertini, A.A. Structural basis for the recognition of LDL-receptor family members by VSV glycoprotein. Nat. Commun. 2018, 9, 1029. [Google Scholar] [CrossRef]
- Litvinov, D.Y.; Savushkin, E.V.; Dergunov, A.D. Intracellular and Plasma Membrane Events in Cholesterol Transport and Homeostasis. J. Lipids 2018, 2018, 22. [Google Scholar] [CrossRef]
- Elfaki, I.; Almutairi, F.M.; Mir, R.; Khan, R.; Abu-Duhier, F. Cytochrome P450 CYP1B1*2 gene and its Association with T2D in Tabuk Population, Northwestern Region of Saudi Arabia. Asian J. Pharm. Clin. Res. 2018, 11, 55–59. [Google Scholar] [CrossRef]
- Dadaev, T.; Saunders, E.J.; Newcombe, P.J.; Anokian, E.; Leongamornlert, D.A.; Brook, M.N.; Cieza-Borrella, C.; Mijuskovic, M.; Wakerell, S.; Al Olama, A.A.; et al. Fine-mapping of prostate cancer susceptibility loci in a large meta-analysis identifies candidate causal variants. Nat. Commun. 2018, 9, 2256. [Google Scholar] [CrossRef]
- Almutairi, F.M.; Mir, R.; Abu-Duhier, F.; Khan, R.; Harby, K.; Elfaki, I. SLC2A2 Gene (Glucose Transporter 2) Variation is Associated with an Increased Risk of Developing T2d in an Ethnic Population of Saudi Arabia. Indian J. Public Health Res. Dev. 2019, 10, 600–605. [Google Scholar] [CrossRef]
- Van der Harst, P.; Verweij, N. Identification of 64 Novel Genetic Loci Provides an Expanded View on the Genetic Architecture of Coronary Artery Disease. Circ. Res. 2018, 122, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Mir, R.; Jha, C.K.; Elfaki, I.; Rehman, S.; Javid, J.; Khullar, N.; Banu, S.; Chahal, S.M.S. MicroRNA-224 (rs188519172 A>G) gene variability is associated with a decreased susceptibility to Coronary Artery Disease: A Case-Control Study. Microrna 2018, 8, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Jha, C.K.; Mir, R.; Elfaki, I.; Khullar, N.; Rehman, S.; Javid, J.; Banu, S.; Chahal, S.M.S. Potential impact of microRNA-423 gene variability in coronary artery disease. Endocr. Metab. Immune Disord. Drug Targets 2018, 19, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Mir, R.; Jha, C.K.; Elfaki, I.; Javid, J.; Rehman, S.; Khullar, N.; Banu, S.; Chahal, S.M.S. Incidence of MicroR-4513C/T Gene Variability in Coronary Artery Disease- A case-Control Study. Endocr. Metab. Immune Disord. Drug Targets 2019. [Google Scholar] [CrossRef] [PubMed]
- Jha, C.K.; Mir, R.; Khullar, N.; Banu, S.; Chahal, S.M.S. LDLR rs688 TT Genotype and T Allele Are Associated with Increased Susceptibility to Coronary Artery Disease-A Case-Control Study. J. Cardiovasc. Dev. Dis. 2018, 5, 31. [Google Scholar] [CrossRef]
- Jha, C.K.; Mir, R.; Elfaki, I.; Javid, J.; Babakr, A.T.; Banu, S.; Chahal, S.M.S. Evaluation of the Association of Omentin 1 rs2274907 A>T and rs2274908 G<A Gene Polymorphisms with Coronary Artery Disease in Indian Population: A Case Control Study. J. Pers. Med. 2019, 9, 30. [Google Scholar]
- Strisciuglio, T.; Franco, D.; Di Gioia, G.; De Biase, C.; Morisco, C.; Trimarco, B.; Barbato, E. Impact of genetic polymorphisms on platelet function and response to anti platelet drugs. Cardiovasc. Diagn. Ther. 2018, 8, 610–620. [Google Scholar] [CrossRef]
- Elfaki, I.; Mir, R.; Almutairi, F.M.; Duhier, F.M.A. Cytochrome P450: Polymorphisms and Roles in Cancer, Diabetes and Atherosclerosis. Asian Pac. J. Cancer Prev. 2018, 19, 2057–2070. [Google Scholar] [PubMed]
- Galasso, G.; Santulli, G.; Piscione, F.; De Rosa, R.; Trimarco, V.; Piccolo, R.; Cassese, S.; Iaccarino, G.; Trimarco, B.; Chiariello, M. The GPIIIA PlA2 polymorphism is associated with an increased risk of cardiovascular adverse events. BMC Cardiovasc. Disord. 2010, 10, 41. [Google Scholar] [CrossRef] [PubMed]
- Strom, T.B.; Tveten, K.; Laerdahl, J.K.; Leren, T.P. Mutation G805R in the transmembrane domain of the LDL receptor gene causes familial hypercholesterolemia by inducing ectodomain cleavage of the LDL receptor in the endoplasmic reticulum. FEBS Open Biol. 2014, 4, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Jha, C.K.; Chahal, S.M.S.; Khullar, N.; Banu, S.; Mir, R. High-Quality Genomic DNA Extraction From Long Term Stored (LTS) Whole Blood Samples Using Glass Bead Method. Int. J. Health Sci. Res. 2016, 6, 288–292. [Google Scholar]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef] [PubMed]
- Prabhakaran, D.; Jeemon, P.; Roy, A. Cardiovascular Diseases in India: Current Epidemiology and Future Directions. Circulation 2016, 133, 1605–1620. [Google Scholar] [CrossRef] [PubMed]
- Wong, B.; Kruse, G.; Kutikova, L.; Ray, K.K.; Mata, P.; Bruckert, E. Cardiovascular Disease Risk Associated With Familial Hypercholesterolemia: A Systematic Review of the Literature. Clin. Ther. 2016, 38, 1696–1709. [Google Scholar] [CrossRef] [PubMed]
- Kathiresan, S.; Melander, O.; Anevski, D.; Guiducci, C.; Burtt, N.P.; Roos, C.; Hirschhorn, J.N.; Berglund, G.; Hedblad, B.; Groop, L.; et al. Polymorphisms associated with cholesterol and risk of cardiovascular events. N. Engl. J. Med. 2008, 358, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.D.; Hsiao, K.M.; Wang, T.C.; Lee, T.H.; Kuo, Y.W.; Huang, Y.C.; Hsu, H.L.; Lin, Y.H.; Wu, C.Y.; Huang, Y.C.; et al. Mutual effect of rs688 and rs5925 in regulating low-density lipoprotein receptor splicing. DNA Cell Biol. 2014, 33, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Nikolajević-Starčević, J.; Popović, D.; Letonja, M.Š.; Makuc, J.; Šeruga, M.; Vujkovac, A.C.; Pražnikar, Z.J.; Stare, J.; Petrovič, D. Polymorphism AvaII of the LDL receptor (rs5925) is associated with carotid-intima media thickness in patients with diabetes mellitus type 2. Slov. Med. J. 2014, 83, 5–12. [Google Scholar]
- Al-Khateeb, A.; Zahri, M.K.; Mohamed, M.S.; Sasongko, T.H.; Ibrahim, S.; Yusof, Z.; Zilfalil, B.A. Analysis of sequence variations in low-density lipoprotein receptor gene among Malaysian patients with familial hypercholesterolemia. BMC Med. Genet. 2011, 12, 40. [Google Scholar] [CrossRef] [PubMed]
- Rios-Gonzalez, B.E.; Ibarra-Cortes, B.; Ramirez-Lopez, G.; Sanchez-Corona, J.; Magana-Torres, M.T. Association of polymorphisms of genes involved in lipid metabolism with blood pressure and lipid values in mexican hypertensive individuals. Dis. Markers 2014, 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.D.; Lee, T.H.; Kuo, Y.W.; Huang, Y.C.; Hsu, H.L.; Lin, Y.H.; Wu, C.Y.; Huang, Y.C.; Lee, M.; Hsiao, K.M. Polymorphisms at the LDLR locus may be associated with ischemic cerebrovascular disease independent of lipid profile. Curr. Neurovasc. Res. 2012, 9, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Lagos, J.; Zambrano, T.; Rosales, A.; Salazar, L.A. APOE polymorphisms contribute to reduced atorvastatin response in Chilean Amerindian subjects. Int. J. Mol. Sci. 2015, 16, 7890–7899. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.X.; Aung, L.H.; Long, X.J.; Yan, T.T.; Cao, X.L.; Huang, F.; Wu, J.Z.; Yang, D.Z.; Lin, W.X.; Pan, S.L. Interactions of several genetic polymorphisms and alcohol consumption on blood pressure levels. Biofactors 2015, 41, 339–351. [Google Scholar] [CrossRef]
- Jamaldini, S.H.; Babanejad, M.; Mozaffari, R.; Nikzat, N.; Jalalvand, K.; Badiei, A.; Sanati, H.; Shakerian, F.; Afshari, M.; Kahrizi, K.; et al. Association of polymorphisms at LDLR locus with coronary artery disease independently from lipid profile. Acta. Med. Iran. 2014, 52, 352–359. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| SNP | Primer Sequence | Product Size | Ta | |
|---|---|---|---|---|
| rs1529729 | F1 Forward primer (C allele) | 5-GTGGTGCCATGTATAACACCC-3 | 175 bp | 61 °C |
| R1 Reverse primer | 5-CAAGAACCCAAGTTTGGAAAC-3 | |||
| F2 Forward primer (T allele) | 5-GTGGTGCCATGTATAACACCT-3 | 212 bp | ||
| R2 Reverse primer | 5-CTATATCTGGAGGCAAGAACCTGA-3 | |||
| rs5925 | Reverse primer (G allele) | 5′-GGGTGAGGTTGTGGAAGACG-3′ | 176 bp | 57 °C |
| Reverse primer (A allele) | 5′-GGGTGAGGTTGTGGAAGACA-3′ | 176 bp | ||
| Common Forward primer | 5′-CAGTGTTTAACGGGATTTGT-3′ |
| Variables | No. of CAD Cases (n = 200 (100%) | No. of Healthy Controls (n = 200 (100%) |
|---|---|---|
| No. of cases and controls | 200 (100%) | 200 (100%) |
| Gender difference | ||
| Males | 180 (90%) | 176 (88%) |
| Females | 20 (10%) | 24 (12%) |
| Age difference | ||
| Age ≤50 | 90 (45%) | 88 (44%) |
| Age >50 | 110 (55%) | 112 (56%) |
| Variables | CAD Cases (n = 200) | (%) |
|---|---|---|
| Random blood sugar (RBS) | ||
| ≤140 mg | 129 | (64.5%) |
| >140 mg | 71 | (35.5%) |
| Cholesterol | ||
| ≤200 mg | 176 | (88%) |
| >200 mg | 24 | (12%) |
| High-density lipoprotein cholesterol (HDL-C) | ||
| ≤40 mg | 166 | (83%) |
| >40 mg | 34 | (17%) |
| Low-density lipoprotein cholesterol (LDL-C) | ||
| ≤100 mg | 150 | (75%) |
| >100 mg | 50 | (25%) |
| Triglycerides (TGL) | ||
| ≤150 mg | 105 | (52.5%) |
| >150 mg | 95 | (47.5%) |
| Coronary heart disease (CHD) in family | ||
| Yes | 15 | (7.5%) |
| No | 185 | (92.5%) |
| Hypertension | ||
| Yes | 29 | (14.5%) |
| No | 171 | (85.5%) |
| Type 2 diabetes | ||
| Yes | 39 | (19.5%) |
| No | 161 | (80.5%) |
| Smoking | ||
| Yes | 121 | (60.5%) |
| No | 79 | (39.5%) |
| Alcohol | ||
| Yes | 71 | (35.5%) |
| No | 129 | (64.5%) |
| Pan masala | ||
| Yes | 4 | (2%) |
| No | 196 | (98%) |
| SNP | Genotype | C/C | C/T | T/T | Chi-Square | Df | P-Value |
|---|---|---|---|---|---|---|---|
| rs1529729 | CAD patients n = 200 (%) | 18 (9%) | 154 (77%) | 28 (14%) | 23.85 | 2 | 0.0001 |
| Controls n = 200 (%) | 42 (21%) | 152 (76%) | 06 (3%) | ||||
| rs5925 | Genotype | G/G | G/A | A/A | Chi-square | Df | P-value |
| CAD patients n = 200 (%) | 54 (27%) | 124 (62%) | 22 (11%) | 10.1 | 2 | 0.006 | |
| Controls n = 200 (%) | 30 (15%) | 152 (76%) | 18 (9%) |
| SNP | Genotypes | Healthy Controls | CAD Cases | Odds Ratio (OR) (95% CI) | Risk Ratio (RR) | P-Value |
|---|---|---|---|---|---|---|
| rs1529729 | (n = 200) | (n = 200) | ||||
| Codominant | ||||||
| LDLR-CC | 42 | 18 | 1 (ref.) | 1 (ref.) | ||
| LDLR-CT | 152 | 154 | 0.42 (0.23–0.77) | 0.59 (0.39–0.89) | 0.0047 | |
| LDLR-TT | 06 | 28 | 0.09 (0.03–0.26) | 0.36 (0.24–0.55) | 0.0001 | |
| Dominant | ||||||
| LDLR-CC | 42 | 18 | 1 (ref.) | 1 (ref.) | ||
| LDLR-(CT + TT) | 158 | 182 | 0.37 (0.21–0.67) | 0.56 (0.38–0.84) | 0.001 | |
| Recessive | ||||||
| LDLR-(CC + CT) | 194 | 172 | 1 (ref.) | 1 (ref.) | ||
| LDLR-TT | 06 | 28 | 0.19 (0.076–0.47) | 0.57 (0.47–0.69) | 0.0003 | |
| Allele | ||||||
| LDLR-C | 236 | 190 | 1 (ref.) | 1 (ref.) | ||
| LDLR-T | 164 | 210 | 0.63 (0.47–0.83) | 0.79 (0.69–0.91) | 0.0011 | |
| rs5925 | Codominant | |||||
| LDLR-GG | 30 | 54 | 1 (ref.) | 1 (ref.) | ||
| LDLR-GA | 152 | 124 | 0.45 (0.27–0.75) | 0.65 (0.47–0.88) | 0.002 | |
| LDLR-AA | 18 | 22 | 0.67 (0.32–1.46) | 0.79 (0.50–1.24) | 0.322 | |
| Dominant | ||||||
| LDLR-GG | 30 | 54 | 1 (ref.) | 1 (ref.) | ||
| LDLR-(GA+AA) | 170 | 146 | 0.477 (0.28–0.78) | 0.66 (0.48–0.9) | 0.003 | |
| Recessive | ||||||
| LDLR-(GG+GA) | 182 | 178 | 1 (ref.) | 1 (ref.) | ||
| LDLR-AA | 18 | 22 | 1.24 (0.64–2.4) | 1.12 (0.78–1.6) | 0.5 | |
| Allele | ||||||
| LDLR-G | 212 | 232 | 1 (ref.) | 1 (ref.) | ||
| LDLR-A | 188 | 168 | 0.8 (0.61–1.07) | 0.9 (0.78–1.03) | 0.107 |
| rs1529729 | rs5925 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subjects | n = 200 | C/C | C/T | T/T | X2 | DF | P value | G/G | G/A | A/A | X2 | DF | P-value |
| Correlation with gender | |||||||||||||
| Males | 180 | 15 | 138 | 27 | 2.2 | 2 | 0.33 | 48 | 111 | 21 | 0.83 | 2 | 0.66 |
| Females | 20 | 03 | 16 | 01 | 06 | 13 | 01 | ||||||
| Correlation with age | |||||||||||||
| Age ≤ 50 | 90 | 07 | 73 | 10 | 1.61 | 2 | 0.447 | 23 | 58 | 09 | 0.43 | 2 | 0.806 |
| Age > 50 | 110 | 11 | 81 | 18 | 31 | 66 | 13 | ||||||
| Correlation with RBS | |||||||||||||
| RBS ≤ 140 mg | 129 | 13 | 98 | 18 | 0.52 | 2 | 0.77 | 33 | 83 | 13 | 0.87 | 2 | 0.647 |
| RBS > 140 mg | 71 | 05 | 56 | 10 | 21 | 41 | 09 | ||||||
| Correlation with cholesterol | |||||||||||||
| Cholesterol ≤ 200 mg | 176 | 14 | 137 | 25 | 1.96 | 2 | 0.375 | 45 | 114 | 17 | 5.33 | 2 | 0.069 |
| Cholesterol > 200 mg | 24 | 04 | 17 | 03 | 09 | 10 | 05 | ||||||
| Correlation with HDL | |||||||||||||
| HDL ≤ 40 mg | 166 | 14 | 128 | 24 | 0.5 | 2 | 0.778 | 44 | 104 | 18 | 0.18 | 2 | 0.913 |
| HDL > 40 mg | 34 | 04 | 26 | 04 | 10 | 20 | 04 | ||||||
| Correlation with LDL | |||||||||||||
| LDL ≤ 100 mg | 150 | 15 | 113 | 22 | 1.07 | 2 | 0.5857 | 44 | 92 | 14 | 2.77 | 2 | 0.25 |
| LDL > 100 mg | 50 | 03 | 41 | 06 | 10 | 32 | 08 | ||||||
| Correlation with TGL | |||||||||||||
| TGL ≤ 150 mg | 105 | 10 | 79 | 16 | 0.4 | 2 | 0.8187 | 25 | 66 | 14 | 1.95 | 2 | 0.377 |
| TGL > 150 mg | 95 | 08 | 75 | 12 | 29 | 58 | 08 | ||||||
| Correlation with hypertension | |||||||||||||
| Hypertension | 29 | 03 | 22 | 04 | 0.07 | 2 | 0.9656 | 04 | 22 | 03 | 3.26 | 2 | 0.195 |
| No hypertension | 171 | 15 | 132 | 24 | 50 | 102 | 19 | ||||||
| Correlation with diabetes | |||||||||||||
| Diabetes | 39 | 04 | 30 | 05 | 0.13 | 2 | 0.9371 | 07 | 28 | 04 | 2.24 | 2 | 0.326 |
| No diabetes | 161 | 14 | 124 | 23 | 47 | 96 | 18 | ||||||
| Correlation with CHD | |||||||||||||
| CHD | 15 | 02 | 11 | 02 | 0.37 | 2 | 0.8311 | 01 | 12 | 02 | 3.41 | 2 | 0.181 |
| No CHD | 185 | 16 | 143 | 26 | 53 | 112 | 20 | ||||||
| Correlation with smoking | |||||||||||||
| Smoking | 121 | 13 | 93 | 15 | 1.6 | 2 | 0.4493 | 26 | 45 | 08 | 2.32 | 2 | 0.313 |
| No smoking | 79 | 05 | 61 | 13 | 28 | 79 | 14 | ||||||
| Correlation with alcohol | |||||||||||||
| Alcohol | 71 | 8 | 52 | 11 | 1.01 | 2 | 0.6035 | 18 | 47 | 06 | 1.07 | 2 | 0.585 |
| No alcohol | 129 | 10 | 102 | 17 | 36 | 77 | 16 | ||||||
| Correlation with pan masala | |||||||||||||
| Pan masala | 04 | 00 | 04 | 00 | 1.22 | 2 | 0.5434 | 00 | 03 | 01 | 1.94 | 2 | 0.379 |
| No pan masala | 196 | 18 | 150 | 28 | 54 | 121 | 21 | ||||||
| rs5925 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Country | Disease | n | Homozygous Wild Type | % | Heterozygous | % | Homozygous Mutant | % | Reference |
| Mexico | Hypertension | 160 | 36 | 22.5 | 73 | 45.63 | 51 | 31.87 | [32] |
| Controls | 160 | 34 | 21.25 | 82 | 51.25 | 44 | 27.5 | ||
| Slovenia | Type 2 diabetes | 399 | 67 | 16.8 | 189 | 47.4 | 143 | 35.8 | [30] |
| Controls | 196 | 26 | 13.3 | 91 | 46.4 | 79 | 40.3 | ||
| Taiwan | Ischemic stroke | 815 | 52 | 6.4 | 262 | 32.1 | 501 | 61.5 | [33] |
| Controls | 430 | 17 | 4 | 146 | 34 | 267 | 62 | ||
| Chile | Hypercholesterolemia | 116 | 25 | 21.6 | 78 | 67.2 | 13 | 11.2 | [34] |
| Controls | NA | NA | NA | NA | |||||
| China | Blood pressure | 608 | 297 | 48.8 | 237 | 39 | 74 | 12.2 | [35] |
| Controls | 616 | 348 | 56.5 | 216 | 35.1 | 52 | 8.4 | ||
| Present study | CAD | 200 | 54 | 27 | 124 | 62 | 22 | 11 | |
| Controls | 200 | 30 | 15 | 152 | 76 | 18 | 9 | ||
| Country | Disease | n | Homozygous Wild Type | % | Heterozygous | % | Homozygous Mutant | % | Reference |
| rs1529729 | |||||||||
| Iran | CAD | 170 | 43 | 25.44 | 103 | 60.36 | 24 | 14.2 | [36] |
| Controls | 104 | 29 | 28.43 | 44 | 42.16 | 31 | 29.41 | ||
| Sweden | Cardiovascular | 5084 | 1610 | 31.7 | 2481 | 48.8 | 993 | 19.5 | [28] |
| Controls | NA | NA | NA | NA | |||||
| Present | CAD cases | 200 | 18 | 9 | 154 | 77 | 28 | 14 | |
| study | Controls | 200 | 42 | 21 | 152 | 76 | 6 | 3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
K. Jha, C.; Mir, R.; Elfaki, I.; Banu, S.; Chahal, S.M.S. LDLR Gene Polymorphisms (rs5925 and rs1529729) Are Associated with Susceptibility to Coronary Artery Disease in a South Indian Population. Med. Sci. 2019, 7, 80. https://doi.org/10.3390/medsci7070080
K. Jha C, Mir R, Elfaki I, Banu S, Chahal SMS. LDLR Gene Polymorphisms (rs5925 and rs1529729) Are Associated with Susceptibility to Coronary Artery Disease in a South Indian Population. Medical Sciences. 2019; 7(7):80. https://doi.org/10.3390/medsci7070080
Chicago/Turabian StyleK. Jha, Chandan, Rashid Mir, Imadeldin Elfaki, Shaheena Banu, and S. M. S. Chahal. 2019. "LDLR Gene Polymorphisms (rs5925 and rs1529729) Are Associated with Susceptibility to Coronary Artery Disease in a South Indian Population" Medical Sciences 7, no. 7: 80. https://doi.org/10.3390/medsci7070080
APA StyleK. Jha, C., Mir, R., Elfaki, I., Banu, S., & Chahal, S. M. S. (2019). LDLR Gene Polymorphisms (rs5925 and rs1529729) Are Associated with Susceptibility to Coronary Artery Disease in a South Indian Population. Medical Sciences, 7(7), 80. https://doi.org/10.3390/medsci7070080