Beta Blockers Up-Titration in Patients with Heart Failure Reduced Ejection Fraction and Cardiac Resynchronization Therapy, a Single Center Study

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
4.1. Baseline Characteristic
4.2. HF Pharmacotherapy before and after CRT
4.3. Clinical and Echocardiographic Response to CRT
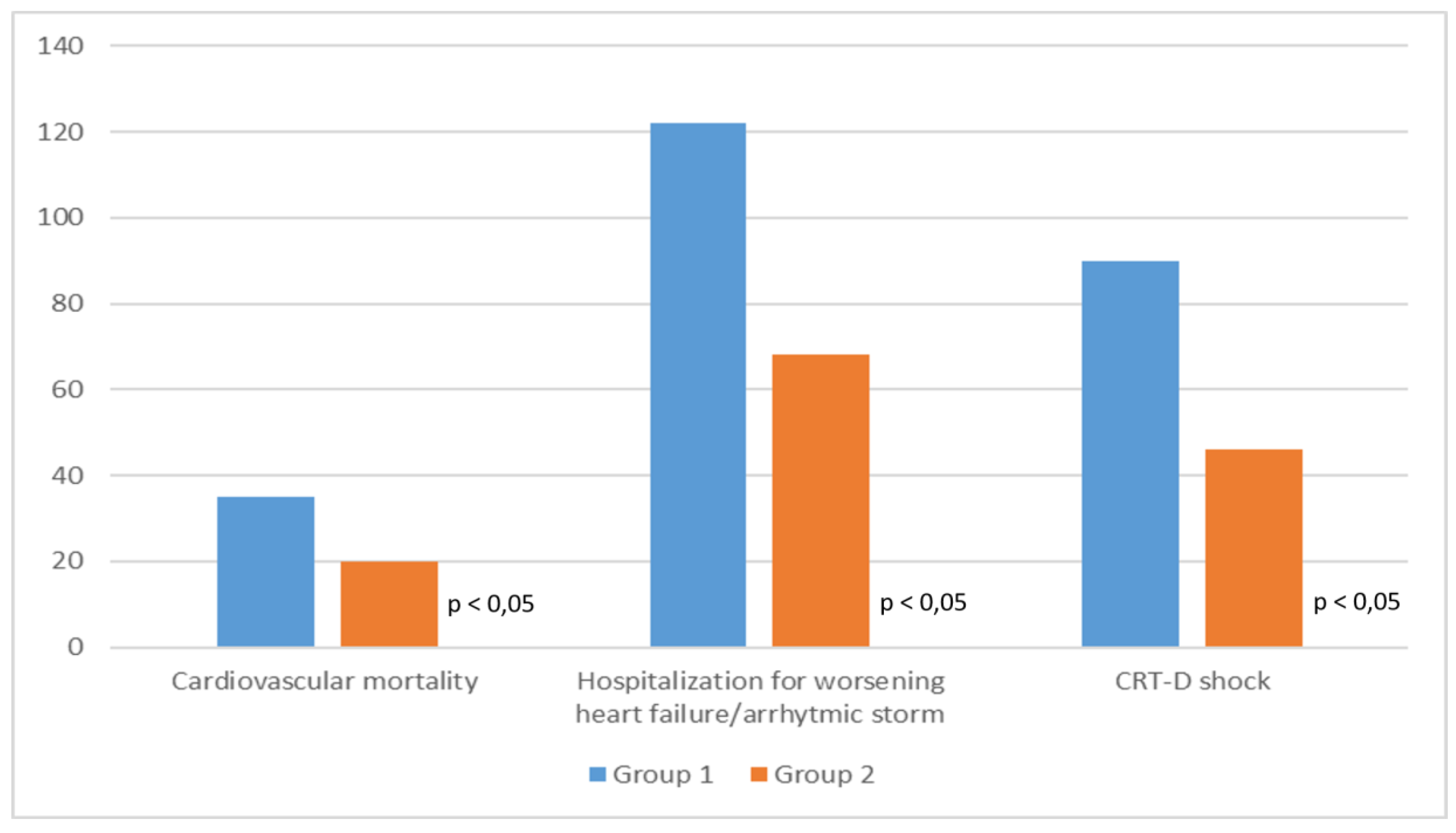
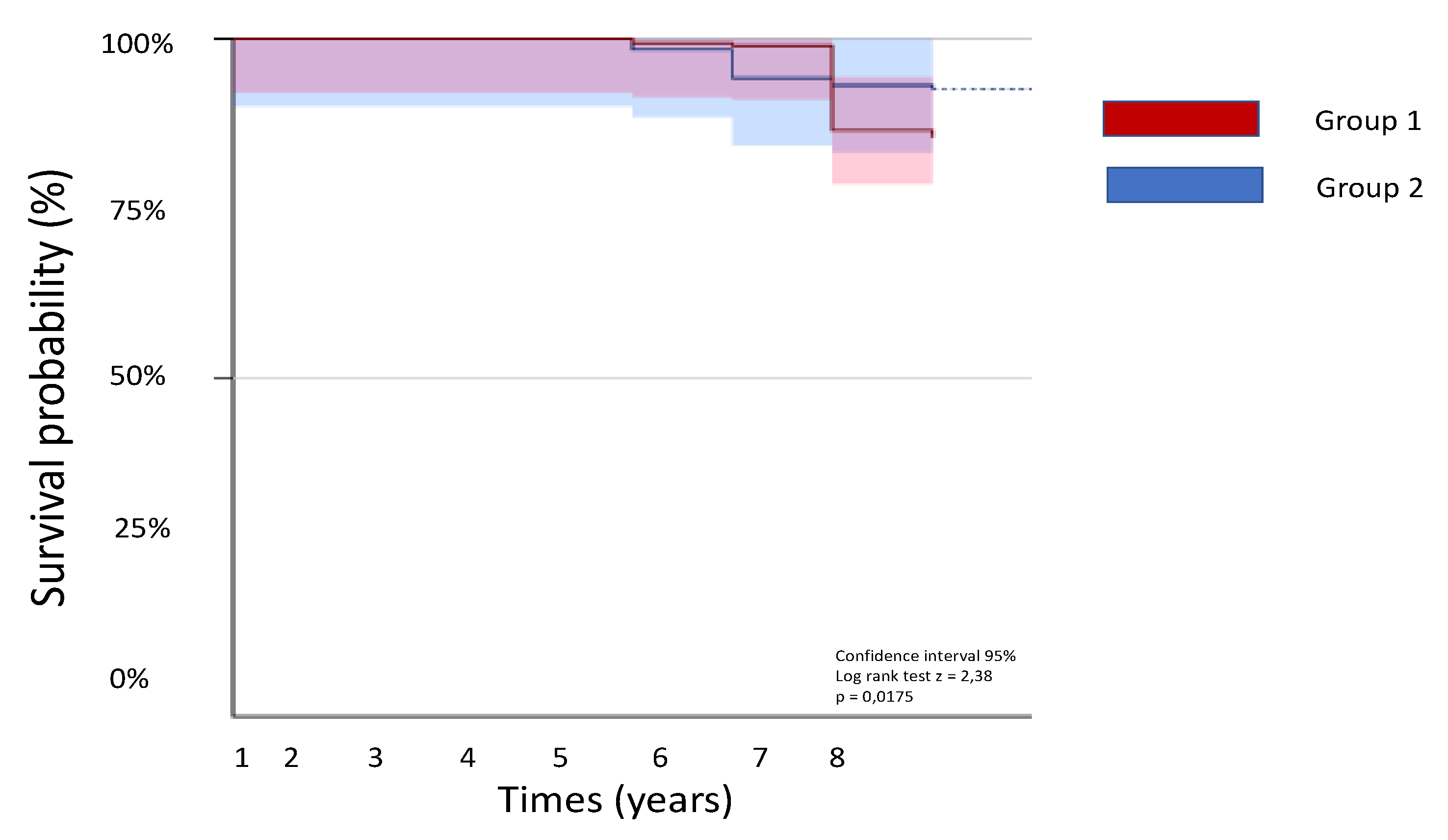
4.4. Follow-Up
5. Discussion
6. Conclusions
7. Study Limitation
Author Contributions
Funding
Conflicts of Interest
References
- Cohn, J.N. The management of chronic heart failure. N. Engl. J. Med. 1996, 335, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R. beta-adrenergic receptor blockade in chronic heart failure. Circulation 2000, 101, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. The neurohormonal hypothesis: A theory to explain the mechanism of disease progression in heart failure. J. Am. Coll. Cardiol. 1992, 20, 248–255. [Google Scholar] [CrossRef]
- Sackner-Bernstein, J.D.; Mancini, D.M. Rationale for treatment of patients with chronic heart failure with the adrenergic blockade. JAMA 1995, 274, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Bristow, M.R.; Cohn, J.N.; Colucci, W.S.; Fowler, M.B.; Gilbert, E.M.; Shusterman, N.H. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. N. Engl. J. Med. 1996, 334, 1349–1355. [Google Scholar]
- CIBIS Investigators and Committees. A randomized trial of β-blockade in heart failure: The Cardiac Insufficiency Bisoprolol Study (CIBIS). Circulation 1994, 90, 765–773. [Google Scholar]
- MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in-Congestive Heart Failure (MERIT-HF). Lancet 1999, 353, 2001–2007. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail 2016, 18, 891–975. [Google Scholar]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll Cardiol. 2017, 70, 776–803. [Google Scholar]
- Brutsaert, D.L. Nonuniformity: A physiologic modulator of contraction and relaxation of the normal heart. J. Am. Coll Cardiol. 1987, 9, 341–348. [Google Scholar] [CrossRef]
- Bleeker, G.B.; Bax, J.J.; Steendijk, P.; Schalij, M.J.; van der Wall, E.E. Left ventricular dyssynchrony in patients with heart failure: Pathophysiology, diagnosis, and treatment. Nat. Clin. Pr. Cardiovasc Med. 2006, 3, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, N.A.; Singh, J.P. Cardiac resynchronization therapy: Past, present, and future. Heart Fail. Clin. 2015, 11, 287–303. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.; Daubert, J.C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L. Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N. Engl. J. Med. 2005, 352, 1539. [Google Scholar] [CrossRef] [PubMed]
- Sundell, J.; Engblom, E.; Koistinen, J.; Ylitalo, A.; Naum, A.; Stolen, K.Q.; Kalliokoski, R.; Nekolla, S.G.; Airaksinen, K.E.; Bax, J.J. The effects of cardiac resynchronization therapy on left ventricular function, myocardial energetics, and metabolic reserve in patients with dilated cardiomyopathy and heart failure. J. Am. Coll Cardiol. 2004, 43, 1027–1033. [Google Scholar] [CrossRef] [PubMed]
- McAlister, F.A.; Ezekowitz, J.; Hooton, N.; Vandermeer, B.; Spooner, C.; Dryden, D.M.; Page, R.L.; Hlatky, M.A.; Rowe, B.H. Cardiac resynchronization therapy for patients with left ventricular systolic dysfunction: A systematic review. Jama 2007, 297, 2502–2514. [Google Scholar] [CrossRef] [PubMed]
- Nabeta, T.; Inomata, T.; Iida, Y.; Ikeda, Y.; Iwamoto-Ishida, M.; Ishii, S.; Naruke, T.; Mizutani, T.; Shinagawa, H.; Koitabashi, T.; et al. Prognostic significance of beta-blocker up-titration in conjunction with cardiac resynchronization therapy in heart failure management. Heart Vessels 2016, 31, 1109–1116. [Google Scholar] [CrossRef]
- Swedberg, K.; Hjalmarson, A.; Waagstein, F.; Wallentin, I. Prolongation of survival in congestive cardiomyopathy by the beta-receptor blockade. Lancet 1979, 301, 1374–1376. [Google Scholar] [CrossRef]
- Waagstein, F.; Bristow, M.R.; Swedberg, K.; Camerini, F.; Fowler, M.B.; Silver, M.A.; Gilbert, E.M.; Johnson, M.R.; Goss, F.G.; Hjalmarson, A. Beneficial effects of metoprolol in idiopathic dilated cardiomyopathy. Metoprolol in Dilated Cardiomyopathy (MDC) Trial Study Group. Lancet 1993, 342, 1441–1446. [Google Scholar] [CrossRef]
- Swedberg, K. History of Beta-blockers in congestive heart failure. Heart 1998, 79, 29–30. [Google Scholar] [CrossRef]
- Jafri, S.M. The effects of beta-blockers on morbidity and mortality in heart failure. Heart Fail. Rev. 2004, 9, 115–121. [Google Scholar] [CrossRef]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G. Comparison of Medical Therapy, Pacing Defibrillation in Heart Failure, Investigators. Cardiac resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N. Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.L.; Listerman, J.; Goring, J.; Giesberg, C.; Nading, M.A.; Butler, J. Beta-blocker therapy for heart failure: Should the therapeutic target be dose or heart rate reduction? Congest Heart Fail. 2006, 12, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Ezekowitz, J.A.; O’Meara, E.; McDonald, M.A.; Abrams, H.; Chan, M.; Ducharme, A.; Giannetti, N.; Grzeslo, A.; Hamilton, P.G.; Heckman, G.A.; et al. 2017 Comprehensive Update of the Canadian Cardiovascular Society Guidelines for the Management of Heart Failure. Can. J. Cardiol. 2017, 33, 1342–1433. [Google Scholar] [CrossRef] [PubMed]
- Cullington, D.; Goode, K.M.; Clark, A.L.; Cleland, J.G. Heart rate achieved or beta-blocker dose in patients with chronic heart failure: Which is the better target? Eur. J. Heart Fail. 2012, 14, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Lechat, P.; Hulot, J.S.; Escolano, S.; Mallet, A.; Leizorovicz, A.; Werhlen-Grandjean, M.; Pochmalicki, G.; Dargie, H. Heart rate and cardiac rhythm relationships with bisoprolol benefit in chronic heart failure in CIBIS II Trial. Circulation 2001, 103, 1428–1433. [Google Scholar] [CrossRef]
- Kotecha, D.; Flather, M.D.; Altman, D.G.; Holmes, J.; Rosano, G.; Wikstrand, J.; Packer, M.; Coats, A.J.S.; Manzano, L.; Böhm, M.; et al. Beta-Blockers in Heart Failure Collaborative Group. Heart Rate and Rhythm and the Benefit of Beta-Blockers in Patients with Heart Failure. J. Am. Coll Cardiol. 2017, 69, 2885–2896. [Google Scholar] [CrossRef]
- Fiuzat, M.; Wojdyla, D.; Pina, I.; Adams, K.; Whellan, D.; O’Connor, C.M. Heart Rate or Beta-Blocker Dose? Association With Outcomes in Ambulatory Heart Failure Patients With Systolic Dysfunction: Results From the HF-ACTION Trial. JACC Heart Fail. 2016, 4, 109–115. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Trial | Year | β-Blockers | n° of Patients | Effects on Mortality |
|---|---|---|---|---|
| CIBIS | 1994 | Bisoprolol | 641 | No significant difference in mortality between the two groups |
| CIBIS II | 1999 | Bisoprolol | 2647 | 34% relative risk reduction in all-cause mortality |
| BEST | 2001 | Bucindolol | 2708 | No significant difference in mortality between the two groups |
| CAPRICORN | 2001 | Carvedilol | 1959 | 23% relative risk reduction in all-cause of mortality |
| COPERNICUS | 2001 | Carvedilol | 2289 | 31% relative risk reduction in all-cause of mortality |
| COMET | 2003 | Metoprolol | 2309 | 17% relative risk reduction in all-cause of mortality |
| MERIT-HF | 1999 | Metoprolol | 3991 | 34% relative risk reduction in all-cause of mortality |
| SENIORS | 2005 | Nebivolol | 2128 | No significant difference in mortality between the two groups |
| Age (Years) | 53 + 7.1 |
| Female sex (n/%) | 162 (33.5%) |
| Ischemic cardiomyopathy (n/%) | 270 (56.25%) |
| LVEDV (ml) | 240 + 8 |
| LVEF (%) | 31 + 4 |
| Median N-terminal pro–B-type natriuretic (pg/mL) | 1720 (886–3854) |
| NYHA I/II/III/IV (n) | 3/354/115/8 |
| Hypertension (n/%) | 235 (48.9) |
| Diabetes (n/%) | 263 (54.7%) |
| Diuretics (n/%) | 310 (64.5%) |
| Digitalis (n/%) | 88 (18.3%) |
| Beta-blockers (n/%) | 480 (100%) |
| ACE-Inhibitors/Angiotensin receptor blockers (n) | 400 (83.3%) |
| Mineralocorticoid antagonist (n) | 255 (53.1%) |
| Group 1 (289 pts) | Group 2 (191 opts) | p | |
|---|---|---|---|
| Age (years) | 52.3 + 8.2 | 54 + 6.3 | 0.67 |
| Female sex (n/%) | 87 (30%) | 75 (39%) | 0.82 |
| Systolic blood pressure (mmHg) | 110 ± 12 | 115 ±10 | 0.87 |
| Heart rate (b/min) | 60 ± 5 | 58 ± 7 | 0.65 |
| Serum creatinine (mg/dl) | 1.13 + 0.8 | 1.11 + 0.6 | 0.76 |
| Ischemic cardiomyopathy (n/%) | 160 (55%) | 110 (57%) | 0.45 |
| Atrial fibrillation (n/%) | 85 (29%) | 72 (37%) | 0.81 |
| QRS duration (ms) | 148 ± 16 | 151 ± 20 | 0.46 |
| LVEDV (ml) | 250 ± 75 | 230 ± 93 | 0.61 |
| LVEF (%) | 32 ± 3 | 29 ± 5 | 0.34 |
| Complete left bundle branch block | 289 (100%) | 191 (100%) | |
| Median N-terminal pro–B-type natriuretic (pg/mL) | 1523 (886–3500) | 1758(892–3854) | 0.27 |
| NYHA I/II/III/IV (n) | 2/209/75/3 | 1/145/40/5 | 0.69 |
| Hypertension (n/%) | 130 (44%) | 105 (54%) | 0.74 |
| Diabetes (n/%) | 175 (60%) | 88 (46%) | 0.22 |
| Diuretics (n/%) | 180 (62%) | 130 (68%) | 0.46 |
| Digitalis (n/%) | 50 (17%) | 38 (19%) | 0.68 |
| Beta-blockers (n/%) | 289 (100%) | 191 (100%) | 0.47 |
| ACE-Inhibitors/Angiotensin receptor blockers (n) | 250 (86%) | 150 (78%) | 0.31 |
| Direct oral anticoagulant (n/%) | 85 (29%) | 72 (37%) | 0.81 |
| Group 1 | Beta-Blockers | Dose before CRT | Dose after CRT | p Value |
| Bisoprolol (175 pts) | 5 ± 1.25 mg | 5 ± 2.5 mg | 0.34 | |
| Carvedilol (114 pts) | 25 ± 18.75 mg | 25 ± 18.75 mg | 0.21 | |
| Group 2 | Beta-blockers | Dose before CRT | Dose after CRT | |
| Bisoprolol (110 pts) | 7.5 ± 1.25 mg | 11.25 ± 1.25 mg | 0.01 | |
| Carvedilol (81 pts) | 50 ± 12.5 mg | 75 ± 25 mg | 0.05 |
| Group 1 | Before CRT | After CRT | p Value |
| LVEDV (mL) | 250 ± 75 | 220 ± 45 | 0.25 |
| LVEF (%) | 32 ± 3 | 35 ± 3 | 0.18 |
| NYHA I/II/III/IV | 2/209/75/3 | 4/260/24/0 | 0.04 |
| Heart rate (b/min) | 60 ± 5 | 60 ± 3 | 0.55 |
| Blood pressure (mmHg) | 100 ± 8 | 104 ± 7 | 0.03 |
| Group 2 | |||
| LVEDV (mL) | 230 ± 93 | 205 ± 72 | 0.12 |
| LVEF (%) | 29±5 | 33 ± 6 | 0.09 |
| NYHA I/II/III/IV | 1/145/40/5 | 10/175/5/1 | 0.02 |
| Heart rate (b/min) | 58 ± 7 | 55 ± 5 | 0.38 |
| Blood pressure (mmHg) | 97 ± 6 | 103 ± 4 | 0.02 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masarone, D.; Verrengia, M.; Ammendola, E.; Gravino, R.; Valente, F.; Vastarella, R.; Rubino, M.; Limongelli, G.; Pacileo, G. Beta Blockers Up-Titration in Patients with Heart Failure Reduced Ejection Fraction and Cardiac Resynchronization Therapy, a Single Center Study. Med. Sci. 2019, 7, 71. https://doi.org/10.3390/medsci7060071
Masarone D, Verrengia M, Ammendola E, Gravino R, Valente F, Vastarella R, Rubino M, Limongelli G, Pacileo G. Beta Blockers Up-Titration in Patients with Heart Failure Reduced Ejection Fraction and Cardiac Resynchronization Therapy, a Single Center Study. Medical Sciences. 2019; 7(6):71. https://doi.org/10.3390/medsci7060071
Chicago/Turabian StyleMasarone, Daniele, Marina Verrengia, Ernesto Ammendola, Rita Gravino, Fabio Valente, Rossella Vastarella, Marta Rubino, Giuseppe Limongelli, and Giuseppe Pacileo. 2019. "Beta Blockers Up-Titration in Patients with Heart Failure Reduced Ejection Fraction and Cardiac Resynchronization Therapy, a Single Center Study" Medical Sciences 7, no. 6: 71. https://doi.org/10.3390/medsci7060071
APA StyleMasarone, D., Verrengia, M., Ammendola, E., Gravino, R., Valente, F., Vastarella, R., Rubino, M., Limongelli, G., & Pacileo, G. (2019). Beta Blockers Up-Titration in Patients with Heart Failure Reduced Ejection Fraction and Cardiac Resynchronization Therapy, a Single Center Study. Medical Sciences, 7(6), 71. https://doi.org/10.3390/medsci7060071