
Prognostic Nutritional Index Could Serve as a Reliable Prognostic Marker in Intensive Care Population



Abstract
1. Introduction
2. Materials and Methods
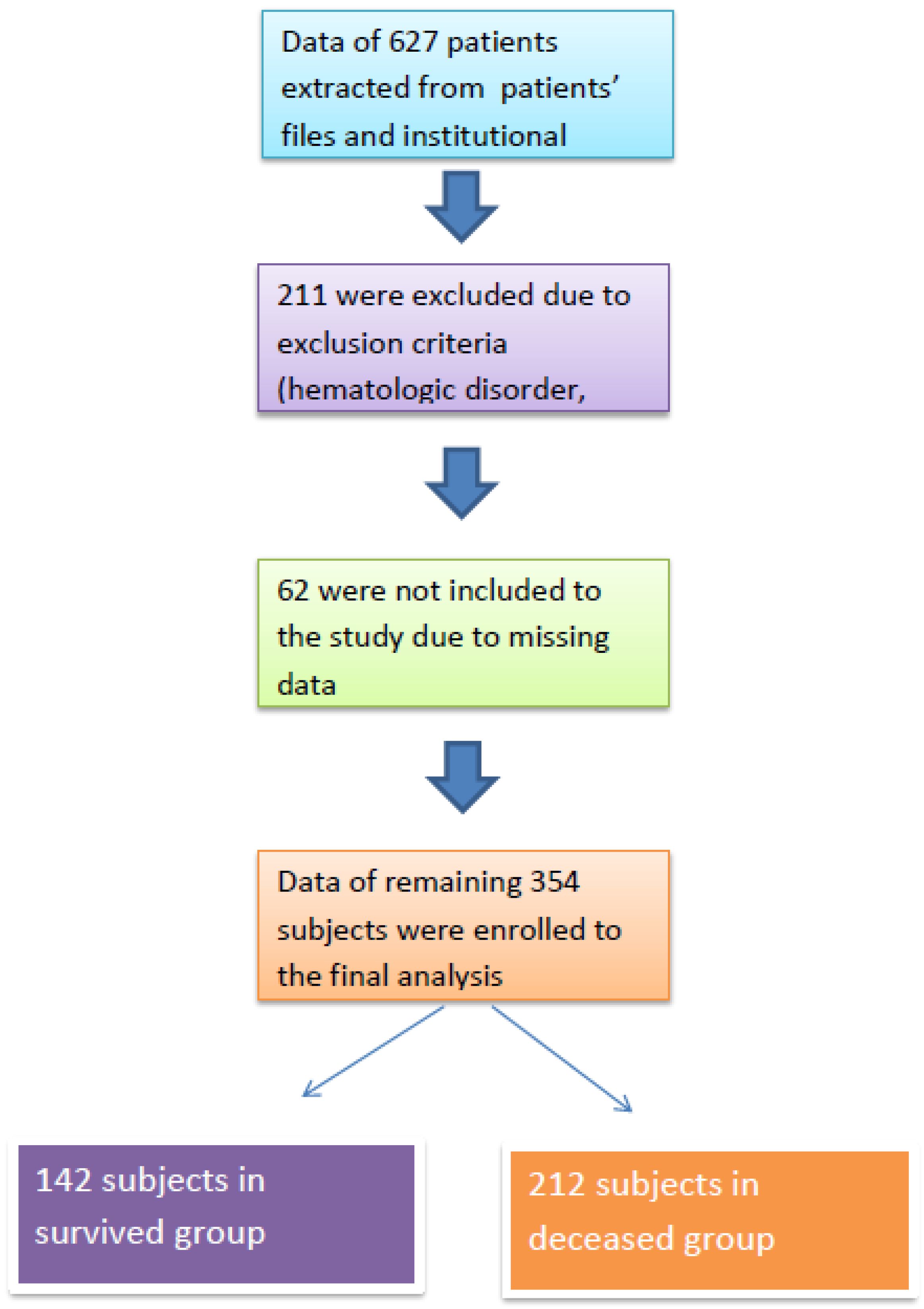
2.1. Study Population
2.2. Statistical Analyses
3. Results
4. Discussion
- (a)
- The prognostic nutritional index was significantly lower in deceased patients compared to survivors in the intensive care unit;
- (b)
- Prognostic nutritional index was significantly correlated with serum creatinine, CRP, PLT, MPV, and age in ICU patients;
- (c)
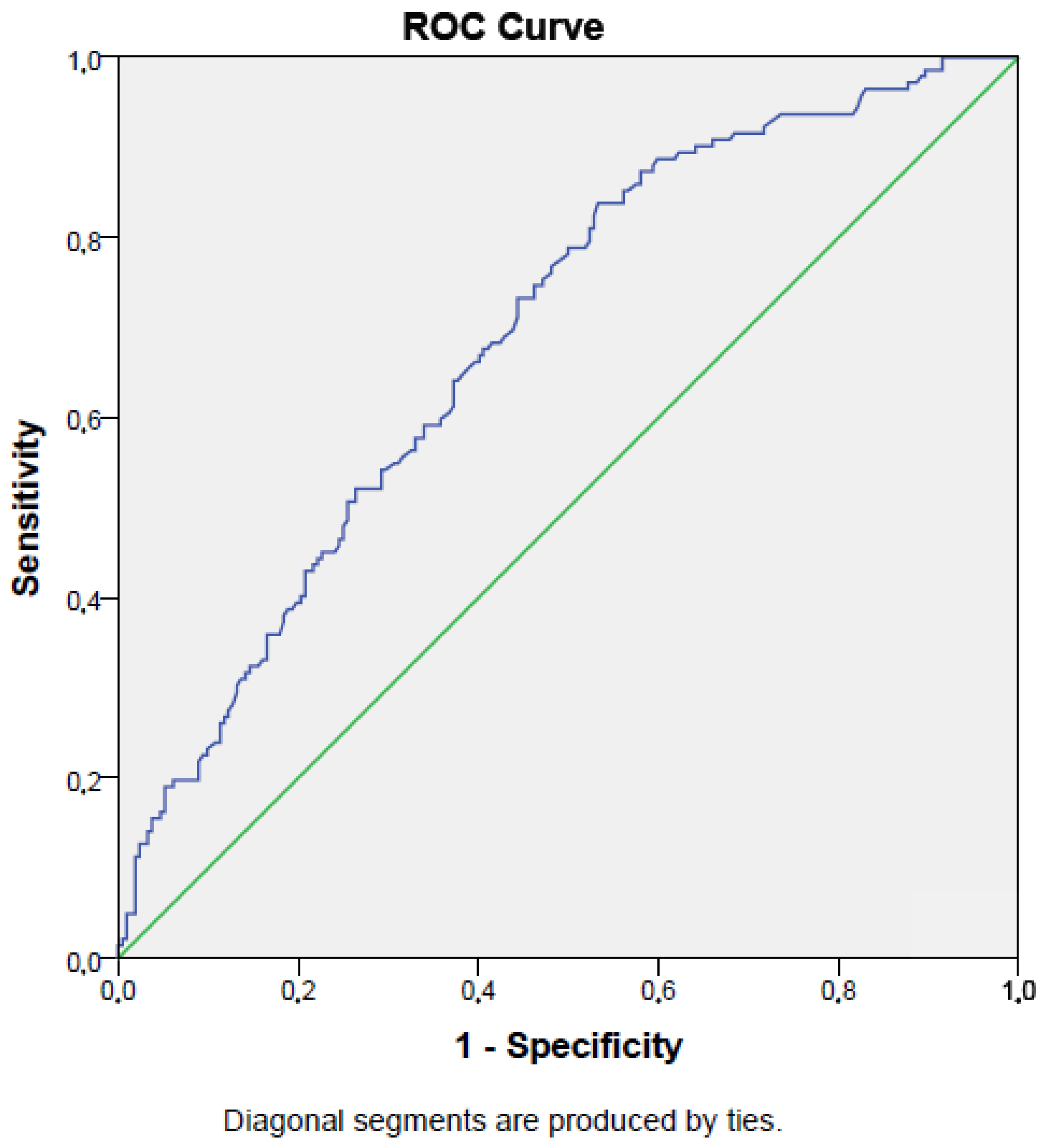
- Prognostic nutritional index demonstrated moderate sensitivity and fair specificity in predicting mortality among ICU patients;
- (d)
- Prognostic nutritional index was an independent risk factor for mortality in patients treated in the ICU.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| WBC | White blood cell count |
| neu | Neutrophil count |
| lym | Lymphocyte count |
| mono | Monocyte count |
| RDW | Red cell distribution width |
| PLT | Platelet count |
| Hb | Hemoglobin |
| Htc | Hematocrit |
| PDW | Platelet distribution width |
| MPV | Mean platelet volume |
| PG | Plasma glucose |
| CRP | c-reactive protein |
| PNI | Prognostic nutritional index |
References
- Pellathy, T.P.; Pinsky, M.R.; Hravnak, M. Intensive Care Unit Scoring Systems. Crit. Care Nurse 2021, 41, 54–64. [Google Scholar] [CrossRef]
- Karagoz, I.; Aktas, G.; Yoldas, H.; Yildiz, I.; Ogun, M.N.; Bilgi, M.; Demirhan, A. Association Between Hemogram Parameters and Survival of Critically Ill Patients. J. Intensive Care Med. 2019, 34, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Aktas, G. Association between the Prognostic Nutritional Index and Chronic Microvascular Complications in Patients with Type 2 Diabetes Mellitus. J. Clin. Med. 2023, 12, 5952. [Google Scholar] [CrossRef]
- Wullur, Y.; Taslim, N.A. Neutrophil-Lymphocyte Ratio, prognostic nutritional index and CRP-Albumin Ratio significantly predict mortality in ICU patients with low nutrition risk. Nutr. Clínica Y Dietética Hosp. 2024, 44, 253–260. [Google Scholar] [CrossRef]
- Sun, K.; Chen, S.; Xu, J.; Li, G.; He, Y. The prognostic significance of the prognostic nutritional index in cancer: A systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 2014, 140, 1537–1549. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Nakamura, T.; Casadei-Gardini, A.; Bruixola, G.; Huang, Y.L.; Hu, Z.D. Long-term and short-term prognostic value of the prognostic nutritional index in cancer: A narrative review. Ann. Transl. Med. 2021, 9, 1630. [Google Scholar] [CrossRef]
- Cheng, Y.L.; Sung, S.H.; Cheng, H.M.; Hsu, P.F.; Guo, C.Y.; Yu, W.C.; Chen, C.H. Prognostic Nutritional Index and the Risk of Mortality in Patients With Acute Heart Failure. J. Am. Heart Assoc. 2017, 6, e004876. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xiao, X.; Wu, Y.; Yang, J.; Zou, Y.; Zhao, Y.; Yang, Q.; Liu, F. Prognostic Nutritional Index as a Predictor of Diabetic Nephropathy Progression. Nutrients 2022, 14, 3634. [Google Scholar] [CrossRef]
- He, M.; Fan, Q.; Zhu, Y.; Liu, D.; Liu, X.; Xu, S.; Peng, J.; Zhu, Z. The need for nutritional assessment and interventions based on the prognostic nutritional index for patients with femoral fractures: A retrospective study. Perioper. Med. 2021, 10, 61. [Google Scholar] [CrossRef]
- Shao, Y.; Lai, Q.C.; Duan, Q.; Ge, P.; Ye, L. Nutritional indices at admission are associated with mortality rates of patients in the intensive care unit. Eur. J. Clin. Nutr. 2022, 76, 557–563. [Google Scholar] [CrossRef]
- Miano, N.; Todaro, G.; Di Marco, M.; Scilletta, S.; Bosco, G.; Di Giacomo Barbagallo, F.; Scicali, R.; Piro, S.; Purrello, F.; Di Pino, A. Malnutrition-Related Liver Steatosis, CONUT Score and Poor Clinical Outcomes in an Internal Medicine Department. Nutrients 2024, 16, 1925. [Google Scholar] [CrossRef] [PubMed]
- Shirakabe, A.; Hata, N.; Kobayashi, N.; Okazaki, H.; Matsushita, M.; Shibata, Y.; Nishigoori, S.; Uchiyama, S.; Asai, K.; Shimizu, W. The prognostic impact of malnutrition in patients with severely decompensated acute heart failure, as assessed using the Prognostic Nutritional Index (PNI) and Controlling Nutritional Status (CONUT) score. Heart Vessel. 2018, 33, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Faix, J.D. Biomarkers of sepsis. Crit. Rev. Clin. Lab. Sci. 2013, 50, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Al-Shami, I.; Hourani, H.M.A.; Alkhatib, B. The use of prognostic nutritional index (PNI) and selected inflammatory indicators for predicting malnutrition in COVID-19 patients: A retrospective study. J. Infect. Public Health 2023, 16, 280–285. [Google Scholar] [CrossRef]
- Nomellini, V.; Kaplan, L.J.; Sims, C.A.; Caldwell, C.C. Chronic Critical Illness and Persistent Inflammation: What can we Learn from the Elderly, Injured, Septic, and Malnourished? Shock 2018, 49, 4–14. [Google Scholar] [CrossRef]
- Ni, L.; Huang, J.; Ding, J.; Kou, J.; Shao, T.; Li, J.; Gao, L.; Zheng, W.; Wu, Z. Prognostic Nutritional Index Predicts Response and Prognosis in Cancer Patients Treated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 823087. [Google Scholar] [CrossRef]
- Peng, J.C.; Nie, F.; Li, Y.J.; Xu, Q.Y.; Xing, S.P.; Gao, Y. Prognostic Nutritional Index as a Predictor of 30-Day Mortality Among Patients Admitted to Intensive Care Unit with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Single-Center Retrospective Cohort Study. Med. Sci. Monit. 2022, 28, e934687-1–e934687-8. [Google Scholar] [CrossRef]
- Shimoyama, Y.; Umegaki, O.; Kadono, N.; Minami, T. Presepsin values and prognostic nutritional index predict mortality in intensive care unit patients with sepsis: A pilot study. BMC Res. Notes 2021, 14, 245. [Google Scholar] [CrossRef]
- Strauss, R.; Wehler, M.; Mehler, K.; Kreutzer, D.; Koebnick, C.; Hahn, E.G. Thrombocytopenia in patients in the medical intensive care unit: Bleeding prevalence, transfusion requirements, and outcome. Crit. Care Med. 2002, 30, 1765–1771. [Google Scholar] [CrossRef]
- Wu, X.; Li, Y.; Yang, X. Platelet phagocytosis by leukocytes in a patient with cerebral hemorrhage and thrombocytopenia caused by gram-negative bacterial infection. J. Int. Med. Res. 2022, 50, 3000605221079102. [Google Scholar] [CrossRef]
- Mitchell, O.; Feldman, D.M.; Diakow, M.; Sigal, S.H. The pathophysiology of thrombocytopenia in chronic liver disease. Hepatic Med. Evid. Res. 2016, 8, 39–50. [Google Scholar] [CrossRef]
- Moreau, D.; Timsit, J.F.; Vesin, A.; Garrouste-Orgeas, M.; de Lassence, A.; Zahar, J.R.; Adrie, C.; Vincent, F.; Cohen, Y.; Schlemmer, B.; et al. Platelet count decline: An early prognostic marker in critically ill patients with prolonged ICU stays. Chest 2007, 131, 1735–1741. [Google Scholar] [CrossRef] [PubMed]
- Puertas, M.; Zayas-Castro, J.L.; Fabri, P.J. Statistical and prognostic analysis of dynamic changes of platelet count in ICU patients. Physiol. Meas. 2015, 36, 939–953. [Google Scholar] [CrossRef]
- Korniluk, A.; Koper-Lenkiewicz, O.M.; Kamińska, J.; Kemona, H.; Dymicka-Piekarska, V. Mean Platelet Volume (MPV): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions. Mediat. Inflamm. 2019, 2019, 9213074. [Google Scholar] [CrossRef] [PubMed]
- Aktas, G.; Cakiroglu, B.; Sit, M.; Uyeturk, U.; Alçelik, A.; Savli, H.; Kemahli, E. Mean platelet volume: A simple indicator of chronic prostatitis. Acta Medica Mediterr. 2013, 29, 551–554. [Google Scholar]
- Dagistan, Y.; Dagistan, E.; Gezici, A.R.; Halicioglu, S.; Akar, S.; Özkan, N.; Gulali, A. Could red cell distribution width and mean platelet volume be a predictor for lumbar disc hernias? Ideggyogy. Szle. 2016, 69, 411–414. [Google Scholar] [CrossRef]
- Aktas, G.; Sit, M.; Tekce, H.; Alcelik, A.; Savli, H.; Simsek, T.; Ozmen, E.; Isci, A.Z.; Apuhan, T. Mean platelet volume in nasal polyps. West Indian Med. J. 2013, 62, 515–518. [Google Scholar] [CrossRef]
- Mandel, J.; Casari, M.; Stepanyan, M.; Martyanov, A.; Deppermann, C. Beyond Hemostasis: Platelet Innate Immune Interactions and Thromboinflammation. Int. J. Mol. Sci. 2022, 23, 3868. [Google Scholar] [CrossRef]
- Akan, S.; Aktas, G. Relationship between frailty, according to three frail scores, and clinical and laboratory parameters of the geriatric patients with type 2 Diabetes Mellitus. Rev. Assoc. Med. Bras. 2022, 68, 1073–1077. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, L.; Yang, X.; Wan, W.; Liu, Y.; Zhang, X. Correlation between malnutrition and mortality in older patients aged ≥90 years with multimorbidity. Geriatr. Nurs. 2024, 59, 321–329. [Google Scholar] [CrossRef]
- Suzuki, E.; Kawata, N.; Shimada, A.; Sato, H.; Anazawa, R.; Suzuki, M.; Shiko, Y.; Yamamoto, M.; Ikari, J.; Tatsumi, K.; et al. Prognostic Nutritional Index (PNI) as a Potential Prognostic Tool for Exacerbation of COPD in Elderly Patients. Int. J. Chronic Obstr. Pulm. Dis. 2023, 18, 1077–1090. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, M.D.; Bala, T.; Wang, Z.; Loftus, T.; Moore, F. Chronic Critical Illness Patients Fail to Respond to Current Evidence-Based Intensive Care Nutrition Secondarily to Persistent Inflammation, Immunosuppression, and Catabolic Syndrome. JPEN J. Parenter. Enter. Nutr. 2020, 44, 1237–1249. [Google Scholar] [CrossRef]
- Molina, P.; Vizcaíno, B.; Huarte, E.; Pallardó, L.M.; Carrero, J.J. Pathophysiology, Detection, and Treatment. In Nutritional Disorders in Chronic Kidney Disease; Craig, J., Molony, D., Strippoli, G., Eds.; Wiley: Hoboken, NJ, USA, 2022; Volume 1, pp. 617–657. [Google Scholar]
- Khor, B.H.; Tiong, H.C.; Tan, S.C.; Abdul Rahman, R.; Abdul Gafor, A.H. Protein-Energy Wasting Assessment and Clinical Outcomes in Patients with Acute Kidney Injury: A Systematic Review with Meta-Analysis. Nutrients 2020, 12, 2809. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, X.; Xiao, L.; Long, G.; Yao, L.; Wang, Z.; Zhou, L. Prognostic Nutritional Index and Systemic Immune-Inflammation Index Predict the Prognosis of Patients with HCC. J. Gastrointest. Surg. 2021, 25, 421–427. [Google Scholar] [CrossRef]
- Xia, L.J.; Li, W.; Zhai, J.C.; Yan, C.W.; Chen, J.B.; Yang, H. Significance of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and prognostic nutritional index for predicting clinical outcomes in T1-2 rectal cancer. BMC Cancer 2020, 20, 208. [Google Scholar] [CrossRef]
- Jiang, Y.; Xu, D.; Song, H.; Qiu, B.; Tian, D.; Li, Z.; Ji, Y.; Wang, J. Inflammation and nutrition-based biomarkers in the prognosis of oesophageal cancer: A systematic review and meta-analysis. BMJ Open 2021, 11, e048324. [Google Scholar] [CrossRef]
- Xie, H.; Wei, L.; Yuan, G.; Liu, M.; Tang, S.; Gan, J. Prognostic Value of Prognostic Nutritional Index in Patients With Colorectal Cancer Undergoing Surgical Treatment. Front. Nutr. 2022, 9, 794489. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jiang, Y.; Luo, Y.; Lin, X.; Song, M.; Li, J.; Zhao, J.; Li, M.; Jiang, Y.; Yin, P.; et al. Prognostic nutritional index with postoperative complications and 2-year mortality in hip fracture patients: An observational cohort study. Int. J. Surg. 2023, 109, 3395–3406. [Google Scholar] [CrossRef]
- Regolo, M.; Vaccaro, M.; Sorce, A.; Stancanelli, B.; Colaci, M.; Natoli, G.; Russo, M.; Alessandria, I.; Motta, M.; Santangelo, N.; et al. Neutrophil-to-Lymphocyte Ratio (NLR) Is a Promising Predictor of Mortality and Admission to Intensive Care Unit of COVID-19 Patients. J. Clin. Med. 2022, 11, 2235. [Google Scholar] [CrossRef]
- Ng, W.W.; Lam, S.M.; Yan, W.W.; Shum, H.P. NLR, MLR, PLR and RDW to predict outcome and differentiate between viral and bacterial pneumonia in the intensive care unit. Sci. Rep. 2022, 12, 15974. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Survived Group (n = 142) | Deceased Group (n = 212) | p | ||
|---|---|---|---|---|
| Gender | Men (n, (%)) | 82 (58) | 130 (61) | 0.50 |
| Women (n, (%)) | 60 (42) | 82 (39) | ||
| Median (IQR) | ||||
| Age (years) | 68 (27) | 73 (22) | <0.001 | |
| Serum albumin (g/dL) | 3.2 (0.8) | 2.8 (0.7) | <0.001 | |
| WBC (×103/mm3) | 11.5 (8.8) | 12.6 (10) | 0.46 | |
| neu (×103/mm3) | 9.5 (8.2) | 10.5 (9) | 0.19 | |
| lym (×103/mm3) | 1.12 (0.8) | 1(0.9) | 0.02 | |
| mono (×103/mm3) | 0.6 (0.4) | 0.6 (0.5) | 0.30 | |
| RDW (%) | 17 (4) | 16 (4) | 0.40 | |
| PLT (×103/mm3) | 217 (115) | 199 (157) | 0.002 | |
| PDW (%) | 17 (4) | 17 (6) | 0.09 | |
| MPV (fL) | 9 (3) | 8 (2.9) | <0.001 | |
| PG (mg/dL) | 133 (75) | 143 (85) | 0.06 | |
| CRP (mg/L) | 49 (82) | 112 (102) | <0.001 | |
| Serum creatinine (mg/dL) | 0.9 (0.7) | 1.3 (1.2) | <0.001 | |
| Length of ICU stay (days) | 3 (0–118) | 5 (0–97) | 0.004 | |
| NLR (%) | 8.4 (1.9–15.7) | 10.4 (4–32) | 0.01 | |
| Mean ± SD | ||||
| Hb (g/dL) | 12 ± 2.5 | 13 ± 2.4 | 0.48 | |
| Htc (%) | 36 ± 8 | 39 ± 7 | 0.56 | |
| PNI (%) | 39 ± 7.5 | 34 ± 7.3 | <0.001 | |
| p | OR | 95% CI | ||
|---|---|---|---|---|
| prognostic nutritional index | <0.001 | 0.94 | 0.90–0.97 | |
| age | 0.001 | 1.03 | 1.01–1.04 | |
| mean platelet volume | <0.001 | 1.31 | 1.16–1.48 | |
| Platelet count | 0.93 | 1 | 1–1.002 | |
| C-reactive protein | 0.001 | 1.01 | 1.002–1.09 | |
| Serum creatinine | 0.36 | 1.1 | 1.02–1.33 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karagoz, I.; Peltek Ozer, S.; Ozer, B.; Aktas, G. Prognostic Nutritional Index Could Serve as a Reliable Prognostic Marker in Intensive Care Population. Med. Sci. 2025, 13, 59. https://doi.org/10.3390/medsci13020059
Karagoz I, Peltek Ozer S, Ozer B, Aktas G. Prognostic Nutritional Index Could Serve as a Reliable Prognostic Marker in Intensive Care Population. Medical Sciences. 2025; 13(2):59. https://doi.org/10.3390/medsci13020059
Chicago/Turabian StyleKaragoz, Ibrahim, Songul Peltek Ozer, Bahri Ozer, and Gulali Aktas. 2025. "Prognostic Nutritional Index Could Serve as a Reliable Prognostic Marker in Intensive Care Population" Medical Sciences 13, no. 2: 59. https://doi.org/10.3390/medsci13020059
APA StyleKaragoz, I., Peltek Ozer, S., Ozer, B., & Aktas, G. (2025). Prognostic Nutritional Index Could Serve as a Reliable Prognostic Marker in Intensive Care Population. Medical Sciences, 13(2), 59. https://doi.org/10.3390/medsci13020059