Exposure–Response Relationships for Toceranib in Dogs with Solid Tumors: A Pilot Study


Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Assessment of Clinical Outcomes and AEs
2.3. Blood Sampling
2.4. Measurement of Plasma Toceranib Concentration
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
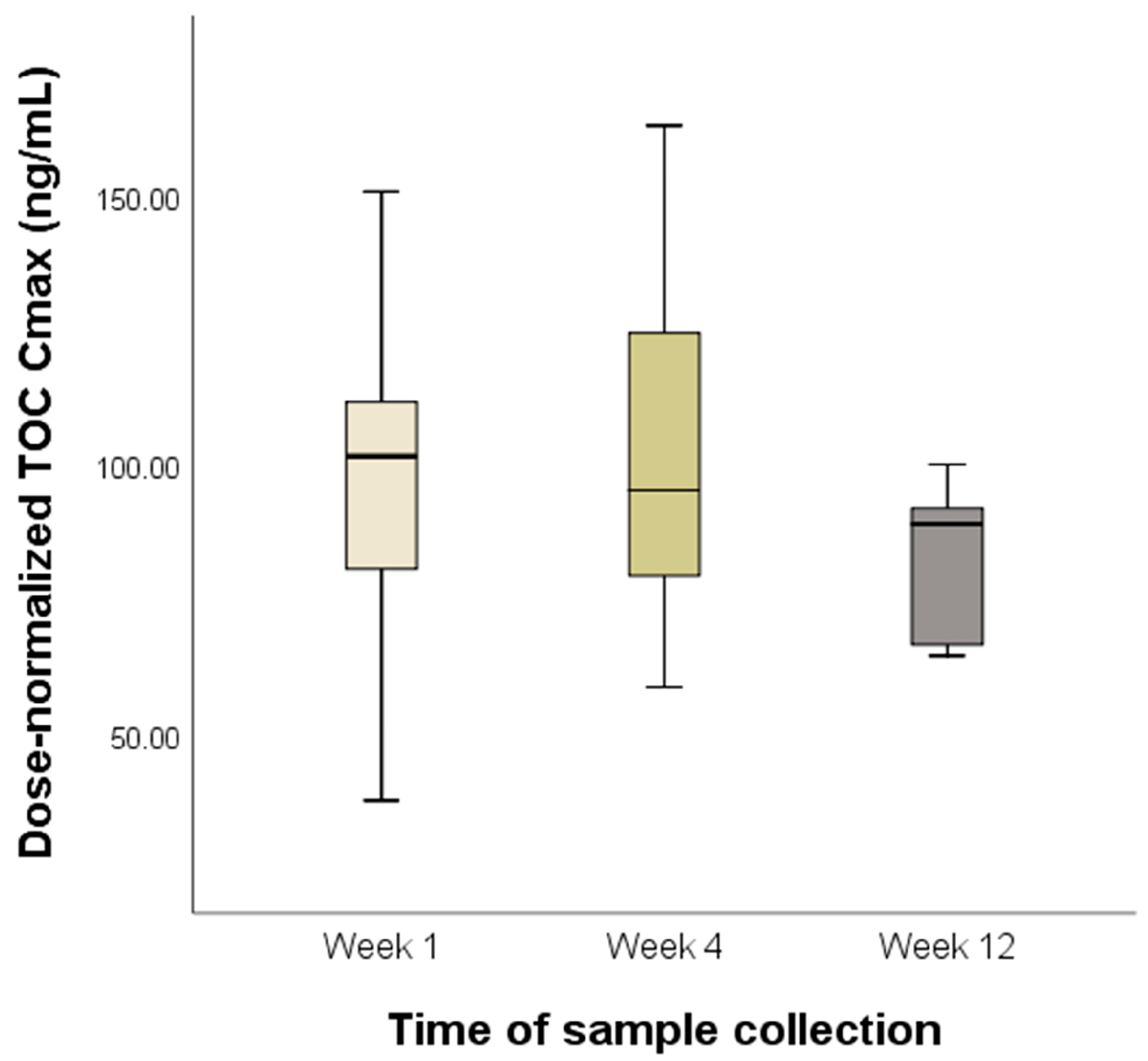
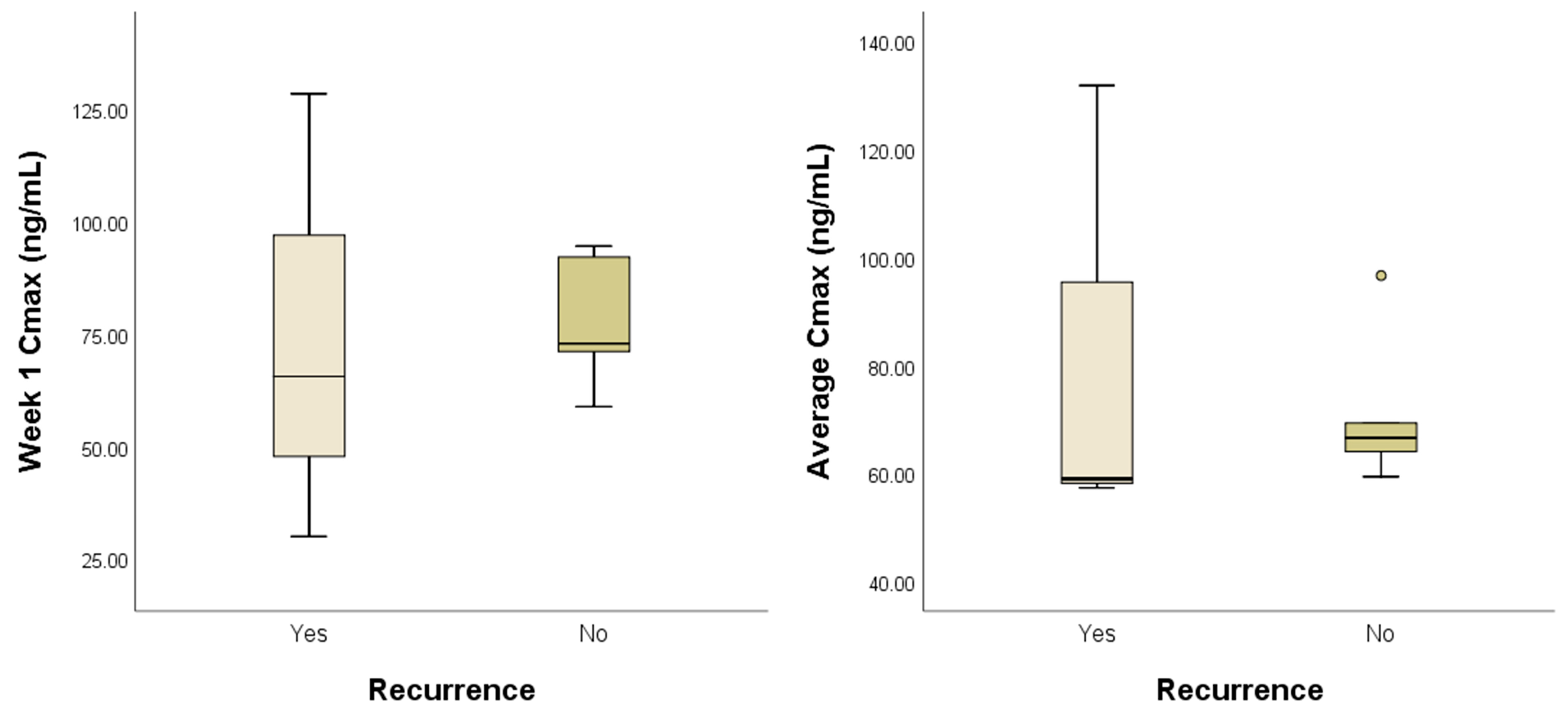
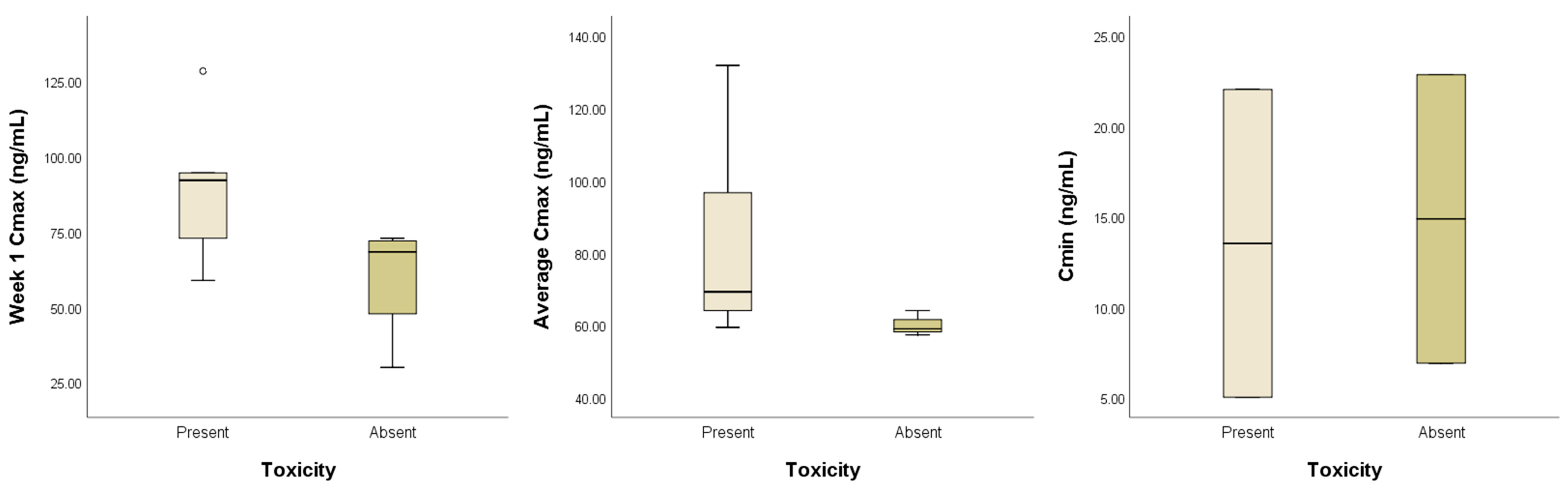
3.2. Analysis of Plasma Toceranib Concentration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AE | Adverse event |
| CM | Castrated male |
| DPOG | Dutch Pharmacology and Oncology Group |
| EP | Entrance potential |
| HCC | Hepatocellular carcinoma |
| HS | Histiocytic sarcoma |
| IS | Internal standard |
| MC | Mammary carcinoma |
| MTD | Maximum tolerated dose |
| OMM | Oral malignant melanoma |
| PC | Pulmonary carcinoma |
| PK | Pharmacokinetics |
| RTK | Receptor tyrosine kinases |
| SCC | Squamous cell carcinoma |
| SF | Spayed female |
| STS | Soft tissue sarcoma |
| TDM | Therapeutic drug monitoring |
| TOC | Toceranib phosphate |
| TKI | Tyrosine kinase inhibitor |
| WHO | World Health Organization |
References
- London, C.A.; Hannah, A.L.; Zadovoskaya, R.; Chien, M.B.; Kollias-Baker, C.; Rosenberg, M.; Downing, S.; Post, G.; Boucher, J.; Shenoy, N.; et al. Phase I dose-escalating study of SU11654, a small molecule receptor tyrosine kinase inhibitor, in dogs with spontaneous malignancies. Clin. Cancer Res. 2003, 9, 2755–2768. [Google Scholar] [PubMed]
- Bavcar, S.; Argyle, D.J. Receptor tyrosine kinase inhibitors: Molecularly targeted drugs for veterinary cancer therapy. Vet. Comp. Oncol. 2012, 10, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Mendel, D.B.; Laird, A.D.; Xin, X.; Louie, S.G.; Christensen, J.G.; Li, G.; Schreck, R.E.; Abrams, T.J.; Ngai, T.J.; Lee, L.B.; et al. In vivo antitumor activity of SU11248, a novel tyrosine kinase inhibitor targeting vascular endothelial growth factor and platelet-derived growth factor receptors: Determination of a pharmacokinetic/pharmacodynamic relationship. Clin. Cancer Res. 2003, 9, 327–337. [Google Scholar] [PubMed]
- Pryer, N.K.; Lee, L.B.; Zadovaskaya, R.; Yu, X.; Sukbuntherng, J.; Cherrington, J.M.; London, C.A. Proof of target for SU11654: Inhibition of KIT phosphorylation in canine mast cell tumors. Clin. Cancer Res. 2003, 9, 5729–5734. [Google Scholar]
- London, C.A.; Malpas, P.B.; Wood-Follis, S.L.; Boucher, J.F.; Rusk, A.W.; Rosenberg, M.P.; Henry, C.J.; Mitchener, K.L.; Klein, M.K.; Hintermeister, J.G.; et al. Multi-center, placebo-controlled, double-blind, randomized study of oral toceranib phosphate (SU11654), a receptor tyrosine kinase inhibitor, for the treatment of dogs with recurrent (either local or distant) mast cell tumor following surgical excision. Clin. Cancer Res. 2009, 15, 3856–3865. [Google Scholar] [CrossRef]
- London, C.; Mathie, T.; Stingle, N.; Clifford, C.; Haney, S.; Klein, M.K.; Beaver, L.; Vickery, K.; Vail, D.M.; Hershey, B.; et al. Preliminary evidence for biologic activity of toceranib phosphate (Palladia(®)) in solid tumours. Vet. Comp. Oncol. 2012, 10, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Frezoulis, P.; Harper, A. The role of toceranib phosphate in dogs with non-mast cell neoplasia: A systematic review. Vet. Comp. Oncol. 2022, 20, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, L.; Thamm, D.H.; Biller, B.J. Clinical and immunomodulatory effects of toceranib combined with low-dose cyclophosphamide in dogs with cancer. J. Vet. Intern. Med. 2012, 26, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, H.; Tanaka, T.; Mie, K.; Nishida, H.; Miura, N.; Akiyoshi, H. Assessment of postoperative adjuvant treatment using toceranib phosphate against adenocarcinoma in dogs. J. Vet. Intern. Med. 2020, 34, 1272–1281. [Google Scholar] [CrossRef] [PubMed]
- Bernabe, L.F.; Portela, R.; Nguyen, S.; Kisseberth, W.C.; Pennell, M.; Yancey, M.F.; London, C.A. Evaluation of the adverse event profile and pharmacodynamics of toceranib phosphate administered to dogs with solid tumors at doses below the maximum tolerated dose. BMC Vet. Res. 2013, 9, 190. [Google Scholar] [CrossRef]
- Gao, B.; Yeap, S.; Clements, A.; Balakrishnar, B.; Wong, M.; Gurney, H. Evidence for therapeutic drug monitoring of targeted anticancer therapies. J. Clin. Oncol. 2012, 30, 4017–4025. [Google Scholar] [CrossRef] [PubMed]
- Verheijen, R.B.; Yu, H.; Schellens, J.H.M.; Beijnen, J.H.; Steeghs, N.; Huitema, A.D.R. Practical Recommendations for Therapeutic Drug Monitoring of Kinase Inhibitors in Oncology. Clin. Pharmacol. Ther. 2017, 102, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Zhang, X.; Sun, G.; Liu, Z.; Zhang, H.; Yang, Y.; Ni, Y.; Dai, J.; Zhu, S.; Chen, J.; et al. Efficacy and Safety of Individualized Schedule of Sunitinib by Drug Monitoring in Patients with Metastatic Renal Cell Carcinoma. Cancer Manag. Res. 2021, 31, 6833–6845. [Google Scholar] [CrossRef]
- Westerdijk, K.; Desar, I.M.E.; Steeghs, N.; van der Graaf, W.T.A.; van Erp, N.P. Dutch Pharmacology and Oncology Group (DPOG). Imatinib, sunitinib and pazopanib: From flat-fixed dosing towards a pharmacokinetically guided personalized dose. Br. J. Clin. Pharmacol. 2020, 86, 258–273. [Google Scholar] [CrossRef] [PubMed]
- Yancey, M.F.; Merritt, D.A.; Lesman, S.P.; Boucher, J.F.; Michels, G.M. Pharmacokinetic properties of toceranib phosphate (Palladia, SU11654), a novel tyrosine kinase inhibitor, in laboratory dogs and dogs with mast cell tumors. J. Vet. Pharmacol. Ther. 2010, 33, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Laver, T.; London, C.A.; Vail, D.M.; Biller, B.J.; Coy, J.; Thamm, D.H. Prospective evaluation of toceranib phosphate in metastatic canine osteosarcoma. Vet. Comp. Oncol. 2018, 16, E23–E29. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, A.K.; Atherton, M.; Bentley, R.T.; Boudreau, C.E.; Burton, J.H.; Curran, K.M.; Dow, S.; Giuffrida, M.A.; Kellihan, H.B.; Mason, N.J.; et al. Veterinary Cooperative Oncology Group-Common Terminology Criteria for Adverse Events (VCOG-CTCAE v2) following investigational therapy in dogs and cats. Vet. Comp. Oncol. 2021, 19, 311–352. [Google Scholar] [CrossRef] [PubMed]
- van der Kleij, M.B.A.; Guchelaar, N.A.D.; Mathijssen, R.H.J.; Versluis, J.; Huitema, A.D.R.; Koolen, S.L.W.; Steeghs, N. Therapeutic Drug Monitoring of Kinase Inhibitors in Oncology. Clin. Pharmacokinet. 2023, 62, 1333–1364. [Google Scholar] [CrossRef] [PubMed]
- Groenland, S.L.; Mathijssen, R.H.J.; Beijnen, J.H.; Huitema, A.D.R.; Steeghs, N. Individualized dosing of oral targeted therapies in oncology is crucial in the era of precision medicine. Eur. J. Clin. Pharmacol. 2019, 75, 1309–1318. [Google Scholar] [CrossRef] [PubMed]
- Cawley, J.R.; Stewart, S.D.; Mochel, J.P.; Veluvolu, S.; Khanna, C.; Fenger, J.M. Pharmacokinetic Exposures Associated With Oral Administration of Sorafenib in Dogs With Spontaneous Tumors. Front. Vet. Sci. 2022, 9, 888483. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Case No. | Breed | Age (Years) | Sex | Tumor Location | Diagnosis | TNM |
|---|---|---|---|---|---|---|
| 1 | Mixed | 9 | CM | Liver | HCC | T1NXM0 |
| 2 | Scottish terrier | 8 | CM | Liver | HCC | T1N0M0 |
| 3 | Bichon Frisé | 10 | SF | Liver | HCC | T1N0M0 |
| 4 | Pomeranian | 5 | SF | Oral cavity | SCC | T1N1M0 |
| 5 | Chihuahua | 12 | SF | Mammary gland | MC | T2N0M0 |
| 6 | Boston terrier | 11 | CM | Joint | STS | T2NXM0 |
| 7 | Coton de Tulear | 7 | CM | Lung | HS | T1N0M0 |
| 8 | Japanese spitz | 9 | CM | Lung | PC | T1N1M0 |
| 9 | Poodle | 11 | CM | Liver | HCC | T1N0M0 |
| 10 | Yorkshire terrier | 12 | SF | Oral cavity | OMM | T2N1M0 |
| Case No. | Dose (mg/kg) | TOC Duration (d) | Cmax (ng/mL) | Cmin (ng/mL) | Recurrence | Toxicity | ||
|---|---|---|---|---|---|---|---|---|
| Week 1 | Week 4 | Week 12 | ||||||
| 1 | 2.78 | 172 | 72.84 | 60.1 | 75.26 | - | N | Y |
| 2 | 2.56 | 323 | 72.85 | - | 79.70 | - | N | N |
| 3 | 2.42 | 374 | 58.83 | 67.59 | 65.57 | <5 | N | Y |
| 4 | 2.77 | 143 | 128.38 | 135.35 | - | - | Y | Y |
| 5 | 2.07 | 31 | 71.07 | 56.96 | - | 6.89 | N | N |
| 6 | 2.57 | 36 | - | - | - | 22.86 | N | N |
| 7 | 2.65 | 196 | 92.06 | 67.74 | 47.44 | 22.04 | N | Y |
| 8 | 2.59 | 130 | 29.94 | 87.99 | - | - | Y | N |
| 9 | 2.78 | 227 | 94.51 | 134.61 | 60.78 | - | N | Y |
| 10 | 2.45 | 185 | 65.53 | 49.07 | - | - | Y | N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-R.; Park, J.-H.; Bae, K.; Yoon, K.-A.; Kim, J.-H. Exposure–Response Relationships for Toceranib in Dogs with Solid Tumors: A Pilot Study. Animals 2025, 15, 1025. https://doi.org/10.3390/ani15071025
Kim Y-R, Park J-H, Bae K, Yoon K-A, Kim J-H. Exposure–Response Relationships for Toceranib in Dogs with Solid Tumors: A Pilot Study. Animals. 2025; 15(7):1025. https://doi.org/10.3390/ani15071025
Chicago/Turabian StyleKim, Young-Rok, Ji-Hwan Park, Kieun Bae, Kyong-Ah Yoon, and Jung-Hyun Kim. 2025. "Exposure–Response Relationships for Toceranib in Dogs with Solid Tumors: A Pilot Study" Animals 15, no. 7: 1025. https://doi.org/10.3390/ani15071025
APA StyleKim, Y.-R., Park, J.-H., Bae, K., Yoon, K.-A., & Kim, J.-H. (2025). Exposure–Response Relationships for Toceranib in Dogs with Solid Tumors: A Pilot Study. Animals, 15(7), 1025. https://doi.org/10.3390/ani15071025