
How Successful Are Veterinary Weight Management Plans for Canine Patients Experiencing Poor Welfare Due to Being Overweight and Obese?

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
- Canine patients with either overweight or obesity listed as a concern or assessment;
- At least 12 months of age at the time of diagnosis;
- Male or female, altered or intact;
- Diagnosed in the period of 2017 to 2022;
- Medical records reporting a minimum of two weight and corresponding BCS measures.
2.2. Body Condition Scoring
2.3. Assessment of Veterinary Engagement (VE)
2.4. Prescription Diet Use
2.5. Comorbidity Assessment
2.6. Data Analysis
3. Results
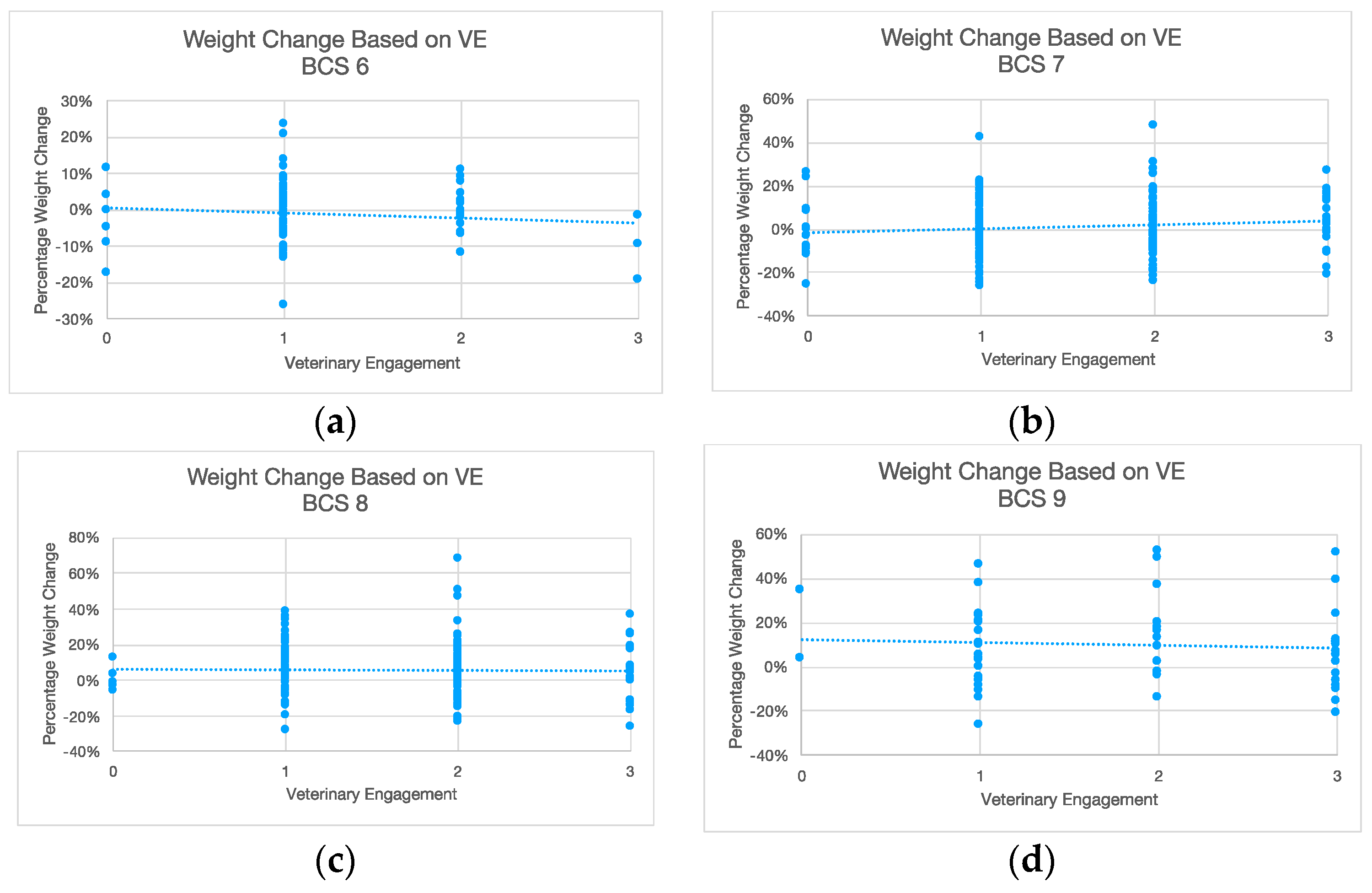
3.1. Veterinary Engagement
3.2. Prescription Weight Loss Diets
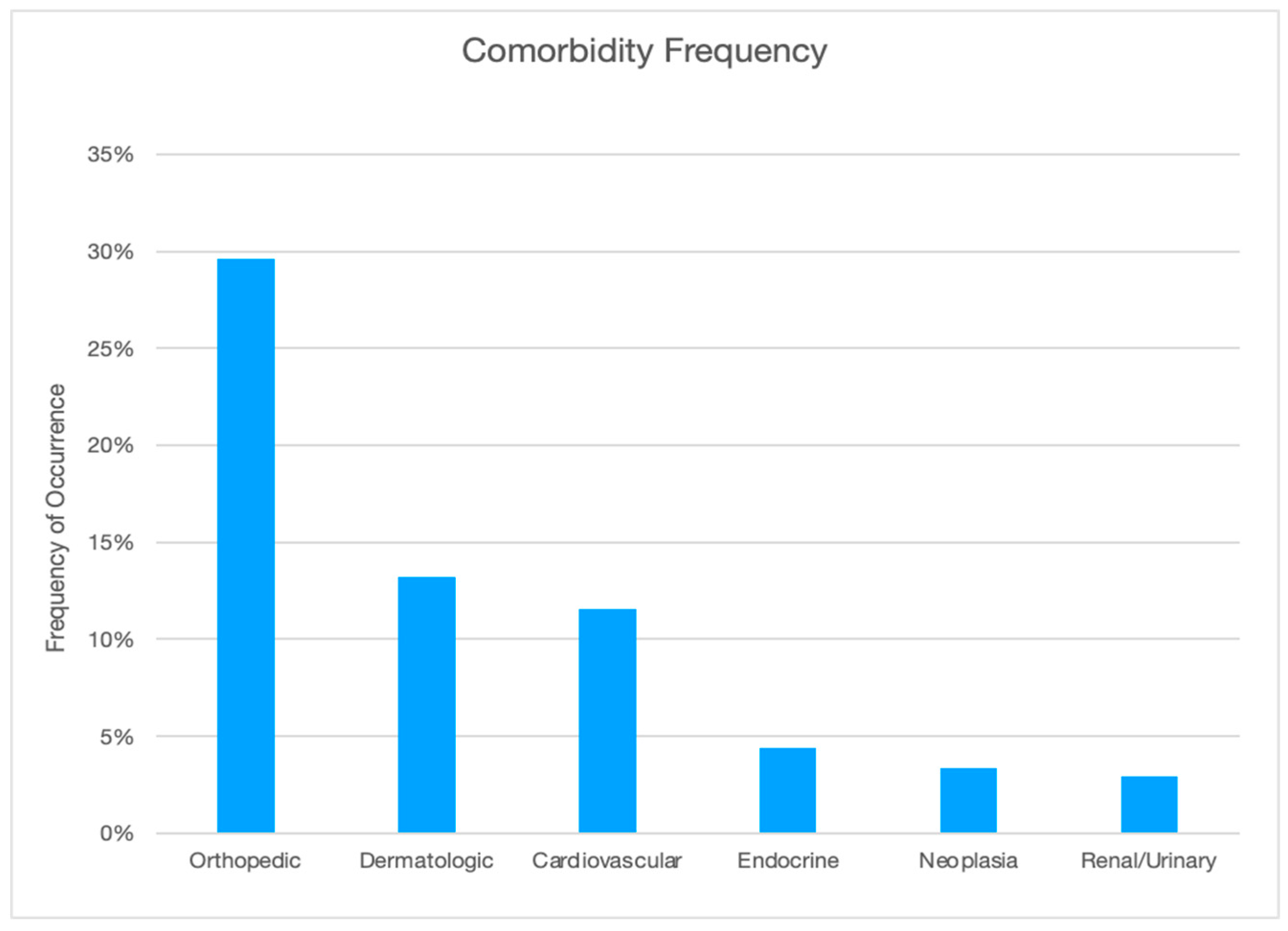
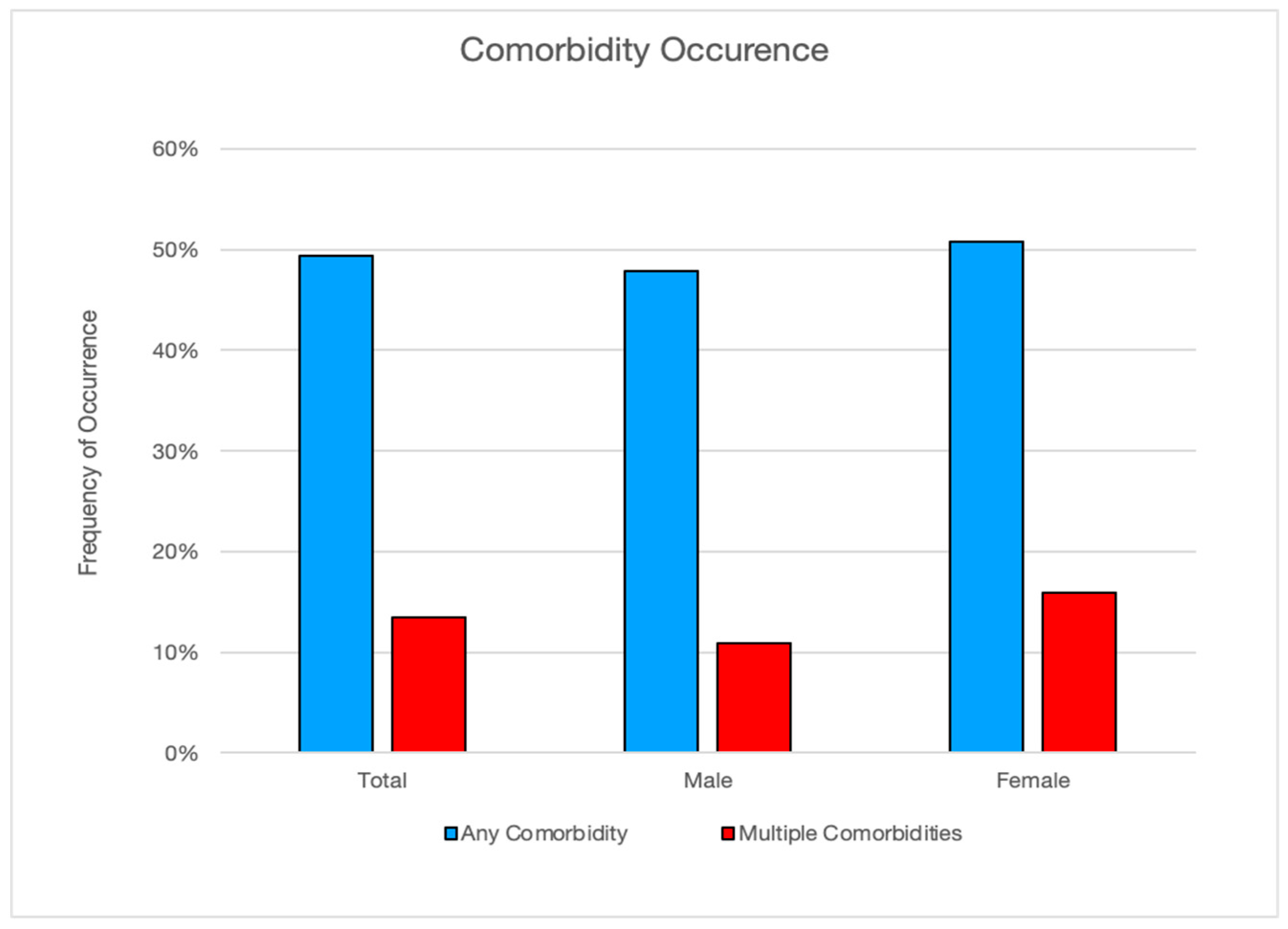
3.3. Comorbidities
4. Discussion
4.1. General Findings
4.2. Veterinary Engagement
4.3. Prescription Weight Loss Diets
4.4. Comorbidities
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Weight Management Guidelines and Resources
References
- Larsen, J.A.; Villaverde, C. Scope of the problem and perception by owners and veterinarians. In Veterinary Clinics of North America: Small Animal Practice; Farcas, A.K., Michel, K.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; Volume 46, pp. 761–772. ISBN 13:978-0-323-46270-9. [Google Scholar]
- Verbrugghe, A. Epidemiology of small animal obesity. In Obesity in the Dog and Cat, 1st ed.; Cline, M.G., Murphy, M., Eds.; CRC Press, Taylor and Francis Group: Boca Raton, FL, USA, 2019; pp. 1–15. ISBN 978-1-4987-4147-7. [Google Scholar]
- German, A.J.; Holden, S.L.; Morris, P.J.; Biourge, V. Long-term follow-up after weight management in obese dogs: The role of diet in preventing regain. Vet. J. 2011, 192, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.; German, A.J.; Churchill, J.A. Association for Pet Obesity Prevention Home Page. Available online: https://www.petobesityprevention.org/global-pet-obesity-initiative (accessed on 20 November 2022).
- British Small Animal Veterinary Association, Position Statement Page. Available online: https://www.bsava.com/position-statement/obesity/ (accessed on 7 January 2021).
- German, A.J.; Holden, S.L.; Moxham, G.L.; Holmes, K.L.; Hackett, R.M.; Rawlings, J.M. A simple reliable tool for owners to assess the body condition of their dog or cat. J. Nutr. 2006, 136, 2031s–2033s. [Google Scholar] [CrossRef]
- German, A.J. The growing problem of obesity in dogs and cats. J. Nutr. 2006, 136, 1940S–1946S. [Google Scholar] [CrossRef] [PubMed]
- Laflamme, D.P. Development and Validation of a Body Condition Score System for Dogs. Canine Pract. 1997, 22, 10–15. [Google Scholar]
- German, A.J.; Holden, S.L.; Bissot, T.; Morris, P.J.; Biourge, V. Use of starting condition score to estimate changes in body weight and composition during weight loss in obese dogs. Res. Vet. Sci. 2009, 87, 249–254. [Google Scholar] [CrossRef]
- Brooks, D.; Churchill, J.; Fein, K.; Linder, D.; Michel, K.; Tudor, K.; Ward, E.; Witzel, A. AAHA weight management guidelines for dogs and cats. JAAHA 2014, 50, 1–11. [Google Scholar]
- Association for Pet Obesity Prevention. The Global Pet Obesity Initiative Position Statement. 2019. Available online: https://static1.squarespace.com/static/6425ec5d33eaaa634113b2d4/t/653e5870610dff50a2fa1013/1698584719824/Global+pet+obesity+initiative+position+statement_2019.pdf (accessed on 12 December 2020).
- Pegram, C.; Raffan, E.; White, E.; Ashworth, A.H.; Brodbelt, D.C.; Church, D.B.; O’Neill, D.G. Frequency, breed predisposition and demographic risk factors for overweight status in dogs in the UK. J. Small Anim. Pract. 2021, 62, 521–530. [Google Scholar] [CrossRef]
- American Pet Products Association: Pet Industry Market Size, Trends & Ownership Statistics. 2021. Available online: http://www.americanpetproducts.org/press_industrytrends.asp (accessed on 22 March 2021).
- Pet Food Manufacturers Association: Pet Population Report. 2021. Available online: https://www.pfma.org.uk/pet-population-2021 (accessed on 22 August 2021).
- World Animal Foundation. Available online: https://worldanimalfoundation.org/dogs/how-many-dogs-are-in-the-world/ (accessed on 22 August 2021).
- Association for Pet Obesity Prevention. U.S. Pet Obesity Rates Plateau and Nutritional Confusion Grow. Available online: www.petobesityprevention.org/2018 (accessed on 12 August 2021).
- BANFIELD®. Pet Hospitals. Cats and Dogs Might have Gained the “Covid 15”, but New Data Reveals a Pet Obesity Epidemic Existed Long before Quarantine. Available online: https://www.banfield.com/en/about-banfield/newsroom/press-releases/2021/new-data-reveals-pet-obesity-epidemic-existed-long-before-quarantine (accessed on 30 August 2021).
- German, A.J.; Holden, S.L.; Wiseman-Orr, M.L.; Reid, J.; Nolan, A.M.; Biourge, V.; Morris, P.J.; Scott, E.M. Quality of life is reduced in obese dogs but improves after successful weight loss. Vet. J. 2012, 192, 428–434. [Google Scholar] [CrossRef]
- Yam, P.S.; Butowski, C.F.; Chitty, J.L.; Naughton, G.; Wiseman-Orr, M.L.; Parkin, T.; Reid, J. Impact of canine overweight and obesity on health-related quality of life. Prev. Vet. Med. 2016, 127, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Chandler, M.L. Impact of obesity on cardiopulmonary disease. In Veterinary Clinics of North America: Small Animal Practice; Farcas, A.K., Michel, K.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; Volume 46, pp. 817–830. ISBN 13:978-0-323-46270-9. [Google Scholar]
- Kealy, R.D.; Lawler, D.F.; Ballam, J.M.; Mantz, S.L.; Biery, D.N.; Greeley, E.H.; Lust, G.; Segre, M.; Smith, G.K.; Stowe, H.D. Effects of diet restriction on life span and age-related changes in dogs. JAVMA 2002, 220, 1315–1320. [Google Scholar] [CrossRef]
- Marshall, W.G.; Bockstahler, B.A.; Hulse, D.A.; Carmichael, S. A review of osteoarthritis and obesity: Current understanding of the relationship and benefit of obesity treatment and prevention in the dog. Vet. Comp. Orthopeadics Traumatol. 2009, 22, 371–378. [Google Scholar]
- Frye, C.W.; Shmalberg, J.W.; Wakshlag, J.J. Obesity, exercise and orthopedic disease. In Veterinary Clinics of North America: Small Animal Practice; Farcas, A.K., Michel, K.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; Volume 46, pp. 831–841. ISBN 13:978-0-323-46270-9. [Google Scholar]
- Day, M. World Small Animal Veterinary Association. Editorial: One health approach to preventing obesity in people and their pets. J. Comp. Pathol. 2017, 156, 293–295. [Google Scholar] [CrossRef]
- Clark, M.; Hoenig, M. Metabolic effects of obesity and its interaction with endocrine diseases. In Veterinary Clinics of North America: Small Animal Practice; Farcas, A.K., Michel, K.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; Volume 46, pp. 797–815. ISBN 13:978-0-323-46270-9. [Google Scholar]
- Wynn, S.G.; Witzel, A.L.; Bartges, J.W.; Moyers, T.S.; Kirk, C.A. Prevalence of asymptomatic urinary tract infections in morbidly obese dogs. PeerJ 2016, 4, e1711. [Google Scholar] [CrossRef]
- German, A.J.; Ryan, V.H.; Wood, I.S.; Trayhurn, P. Obesity, its associated disorders and the role of inflammatory adipokines in companion animals. Vet. J. 2010, 85, 4–9. [Google Scholar] [CrossRef]
- German, A.J.; Blackwell, E.; Evans, M.; Westgarth, C. Overweight dogs are more likely to display undesirable behaviours: Results of a large online survey of dog owners in the UK. J. Nutr. Sci. 2017, 6, e14. [Google Scholar] [CrossRef]
- German, A.J.; Titcomb, J.M.; Holden, S.L.; Queau, Y.; Morris, P.J.; Biourge, V. Cohort study of the success of controlled weight loss programs for obese dogs. J. Vet. Intern. Med. 2015, 29, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- German, A.J. Obesity prevention and weight maintenance after loss. In Veterinary Clinics of North America: Small Animal Practice; Farcas, A.K., Michel, K.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; Volume 46, pp. 913–929. ISBN 13:978-0-323-46270-9. [Google Scholar]
- Lawler, D.F.; Evans, R.H.; Larson, B.T.; Spitznagel, E.L.; Ellersieck, M.R.; Kealy, R.D. Influence of lifetime food restriction on causes, time, and predictors of death in dogs. JAVMA 2005, 226, 225–231. [Google Scholar] [CrossRef]
- Penell, J.C.; Morgan, D.M.; Watson, P.; Carmichael, S.; Adams, V. Body weight at 10 years of age and change in body composition between 8 and 10 years of age were related to survival in a longitudinal study of 39 Labrador retriever dogs. Acta Vet Scand. 2019, 61, 42. [Google Scholar] [CrossRef] [PubMed]
- Salt, C.; Morris, P.; Wilson, D.; Lund, E.; German, A.J. Association between lifespan and body condition in neutered client-owned dogs. J. Vet. Intern. Med. 2018, 33, 89–99. [Google Scholar] [CrossRef]
- Chiang, C.F.; Villaverde, C.; Chang, W.C.; Fascetti, A.J.; Larsen, J.A. Prevalence, Risk Factors, and Disease Associations of Overweight and Obesity in Dogs that Visited the Veterinary Medical Teaching Hospital at the University of California, Davis from January 2006 to December 2015. Top. Companion Anim. Med. 2022, 48, 100640. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, M. Canine and Feline Obesity Management. In Veterinary Clinics of North America: Small Animal Practice; Farcas, A.K., Michel, K.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; Volume 46, pp. 653–667. ISBN 13:978-0-323-46270-9. [Google Scholar]
- Bland, I.M.; Guthrie-Jones, A.; Taylor, R.D.; Hill, J. Dog obesity: Owner attitudes and behaviour. Prev. Vet. Med. 2009, 92, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Bjørnvada, C.R.; Gloor, S.; Johansena, S.S.; Sandøe, P.; Lund, T.B. Neutering increases the risk of obesity in male dogs but not in bitches—A cross-sectional study of dog- and owner-related risk factors for obesity in Danish companion dogs. Prev. Vet. Med. 2019, 170, 104730. [Google Scholar] [CrossRef]
- Raffan, E.; Dennis, R.J.; O’Donovan, C.J.; Becker, J.M.; Scott, R.A.; Smith, S.P.; Withers, D.J.; Wood, C.J.; Conci, E.; Clements, D.N.; et al. A Deletion in the Canine POMC Gene Is Associated with Weight and Appetite in Obesity-Prone Labrador Retriever Dogs. Cell Metab. 2016, 23, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Krasuska, M.; Webb, T.L. How effective are interventions designed to help owners to change their behaviour so as to manage the weight of their companion dogs? A systematic review and meta-analysis. Prev. Vet. Med. 2018, 159, 40–50. [Google Scholar] [CrossRef]
- Kienzle, E.; Bergler, R.; Mandernach, A. A comparison of the feeding behavior and the human–animal relationship in owners of normal and obese dogs. J. Nutr. 1998, 128, 2779S–2782S. [Google Scholar] [CrossRef] [PubMed]
- White, G.A.; Ward, L.; Pink, C.; Craigon, J.; Millar, K.M. “Who’s been a good dog?”—Owner perceptions and motivations for treat giving. Prev. Vet. Med. 2016, 132, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Courcier, E.A.; Thomson, R.M.; Mellor, D.J.; Yam, P.S. An epidemiological study of environmental factors associated with canine obesity. J. Small Anim. Pract. 2010, 51, 362–367. [Google Scholar] [CrossRef]
- Wainwright, J.; Millar, K.M.; White, G.A. Owners’ views of canine nutrition, weight status and wellbeing and their implications for the veterinary consultation. J. Small Anim. Pract. 2022, 63, 81–388. [Google Scholar] [CrossRef]
- Association for Pet Obesity Prevention. U.S. Pet Food, Nutrition, and Weight Management Survey Results. 2021. Available online: https://petobesityprevention.org/news/2022/8/31/1lvn0o85r9w6em21pgjchshqce57pg (accessed on 1 September 2022).
- Bartges, J.; Kushner, R.; Michel, K.; Sallisx, R.; Day, M. One health solutions to obesity in people and their pets. J. Comp. Pathol. 2017, 156, 326–333. [Google Scholar] [CrossRef]
- Suarez, L.; Bautista-Castaño, I.; Peña Romera, C.; Montoya-Alonso, J.A.; Corbera, J.A. Is Dog Owner Obesity a Risk Factor for Canine Obesity? A “One-Health” Study on Human–Animal Interaction in a Region with a High Prevalence of Obesity. Vet. Sci. 2022, 9, 243. [Google Scholar] [CrossRef]
- Kipperman, B.S.; German, A.J. The responsibility of veterinarians to address companion animal obesity. Animals 2018, 8, 143. [Google Scholar] [CrossRef]
- Vucinic, M.; Vucicevic, M.; Nenadovic, K. The COVID-19 pandemic affects owners walking with their dogs. J. Vet. Behav. 2022, 48, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Christley, R.M.; Murray, J.K.; Anderson, K.L.; Buckland, E.L.; Casey, R.A.; Harvey, N.D.; Harris, L.; Holland, K.E.; McMillan, K.M.; Mead, R.; et al. Impact of the First COVID-19 Lockdown on Management of Pet Dogs in the UK. Animals 2021, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Chan, S.C.; Ko, S.; Wang, H.H.X.; Yuan, J.; Xu, W.; Zheng, Z.; Xue, H.; Zhang, L.; Jiang, J.Y.; et al. Factors associated with weight gain during COVID-19 pandemic: A global study. PLoS ONE 2023, 18, e0284283. [Google Scholar] [CrossRef]
- DeGioia, P. Veterinarians Ponder Ideal Number of Daily Appointments. Veterinary Information Network News. 2012. Available online: https://news.vin.com/default.aspx?pid=210&catId=-1&id=5387398 (accessed on 15 February 2024).
- Cline, M.G.; Burns, K.M.; Coe, J.B.; Downing, R.; Durzi, T.; Murphy, M.; Parker, V. 2021 AAHA Nutrition and weight management guidelines for dogs and cats. JAAHA 2021, 57, 153–178. [Google Scholar] [CrossRef] [PubMed]
- Porsani, M.Y.H.; Teixeira, F.A.; Amaral, A.R.; Pedrinelli, V.; Vasques, V.; de Oliviera, A.G.; Vendramini, T.H.A.; Brunetto, M.A. Factors associated with failure of dog’s weight loss programmes. Vet. Med. Sci. 2019, 6, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Roudebush, P.; Schoenherr, W.D.; Delaney, S.J. An evidence-based review of the use of therapeutic foods, owner education, exercise, and drugs for the management of obese and overweight pets. JAVMA 2008, 233, 717–725. [Google Scholar] [CrossRef]
- Floerchinger, A.; Jackson, M.; Jewell, D.; MacLeay, J.; Paetau-Robinson, I.; Hahn, K. Effect of feeding a weight loss food beyond a caloric restriction period on body composition and resistance to weight gain in dogs. JAVMA 2015, 227, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, J.; Bissot, T.; Hours, M.; Moreno, B.; Feugier, A.; German, A.J. Success of a weight loss plan for overweight dogs: The results of an international weight loss study. PLoS ONE 2017, 12, 9. [Google Scholar] [CrossRef]
- Vitger, A.D.; Stallknecht, B.M.; Nielsen, D.H.; Bjornvad, C.R. Integration of a physical training program in a weight loss plan for overweight pet dogs. JAVMA 2016, 248, 174–182. [Google Scholar] [CrossRef]
- Murphy, M. Obesity treatment: Environment and behavior modification. In Veterinary Clinics of North America: Small Animal Practice; Farcas, A.K., Michel, K.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; Volume 46, pp. 883–898. ISBN 13:978-0-323-46270-9. [Google Scholar]
- Cottam, D.R.; Mattar, S.G.; Barinas-Mitchell, E.; Eid, G.; Kuller, L.; Kelley, D.E.; Schauer, P.R. The chronic inflammatory hypothesis for the morbidity associated with morbid obesity: Implications and effects of weight loss. Obes. Surg. 2004, 14, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Neto, G.; Brunetto, M.; Oba, P.; Champion, T.; Villaverde, C.; Vendramini, T.; Balieiro, J.; Carciofi, A.; Camacho, A. Weight loss improved arterial blood gases and respiratory parameters in obese dogs. J. Anim. Physiol. Anim. Nutr. 2018, 102, 1743–1748. [Google Scholar] [CrossRef] [PubMed]
- German, A.J.; Woods, G.R.; Holden, S.L.; Brennan, L.; Burke, C. Dangerous trends in pet obesity. Vet. Rec. 2018, 182, 25. [Google Scholar] [CrossRef] [PubMed]
- Rolph, N.C.; Noble, P.J.; German, A.J. How often do primary care veterinarians record the overweight status of dogs? J. Nutr. Sci. 2014, 3, e58. [Google Scholar] [CrossRef] [PubMed]
- German, A.J. Weight management in obese pets: The tailoring concept and how it can improve results. Acta Vet. Scand. 2015, 58, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, E.; Schultz, K.; Floerchinger, A.; Hull, J. Small animal general practitioners discuss nutrition infrequently despite assertion of indication, citing barriers. JAVMA 2022, 260, 1704–1710. [Google Scholar] [CrossRef]
- MacMartin, C.; Wheat, H.C.; Coe, J.B.; Adams, C.L. Conversation Analysis of Veterinarians’ Proposals for Long-Term Dietary Change in Companion Animal Practice in Ontario, Canada. J. Vet. Med. Educ. 2018, 45, 514–533. [Google Scholar] [CrossRef] [PubMed]
- Churchill, J.; Ward, E. Communicating with pet owners about obesity: Roles of the veterinary health care team. In Veterinary Clinics of North America: Small Animal Practice; Farcas, A.K., Michel, K.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; Volume 46, pp. 899–911. ISBN 13:978-0-323-46270-9. [Google Scholar]
- Padliya, N. Why Going beyond Body Condition Scoring Can Help Overweight Canines. Veterinary Practice News. 2022. Available online: https://www.veterinarypracticenews.com/nutrition-may-2022/?ads=disable (accessed on 15 February 2024).
- Keller, E.; Sagols, E.; Flanagan, J.; Biourge, V.; German, A.J. Use of reduced-energy content maintenance diets for modest weight reduction in overweight cats and dogs. Res. Vet. Sci. 2020, 131, 194–205. [Google Scholar] [CrossRef]
- Schake, C.; Love Does not Equal Food: The Pet Obesity Epidemic. The Good Pet Parent Blog. 2015. Available online: http://www.goodpetparent.com/2015/01/23/pet-obesity-overweight/ (accessed on 15 January 2021).
- Hours, M.A.; Sagols, E.; Junien-Castagna, A.; Feugier, A.; Moniot, D.; Daniel, I.; Biourge, V.; Samuel, S.; Queau, Y.; German, A.J. Comparison of voluntary food intake and palatability of commercial weight loss diets in healthy dogs and cats. BMC Vet. Res. 2016, 12, 274. [Google Scholar] [CrossRef]
- German, A.J.; Luxmore, J.; Holden, S.L.; Morris, P.J.; Biourge, V. Feeding obese dogs during weight loss is on average cost-neutral. J. Small Anim. Pract. 2015, 56, 366–369. [Google Scholar] [CrossRef]
- BANFIELD®. Pet Hospitals: Obesity in Dogs and Cats—State of Pet Health Report. 2017. Available online: https://www.banfieldexchange.com/VET-Report (accessed on 20 March 2021).
- Chandler, M.; Cunningham, S.; Lund, E.M.; Khanna, C.; Naramore, R.; Patel, A.; Day, M.J. Obesity and associated comorbidities in people and companion animals: A One Health Perspective. J. Comp. Pathol. 2017, 156, 296–309. [Google Scholar] [CrossRef] [PubMed]
- Lund, E.M.; Armstrong, P.J.; Kirk, C.A.; Klauser, J.S. Prevalence and risk factors for obesity in adult dogs from private US veterinary practices. Int. J. Appl. Res. Vet. Med. 2006, 4, 177–186. [Google Scholar]
- BANFIELD®. Pet Hospitals: Spotlight on Osteoarthritis—State of Pet Health Report. 2019. Available online: https://www.banfieldexchange.com/VET-Report (accessed on 20 March 2021).
- Rollins, A.W.; Shepherd, M. Pathophysiology of obesity: Metabolic effects and inflammation mediators. In Obesity in the Dog and Cat, 1st ed.; Cline, M., Murphy, M., Eds.; CRC Press, Taylor and Francis Group: Boca Raton, FL, USA, 2019; pp. 17–37. [Google Scholar]
- Laflamme, D.P. Key nutrients important in the management of canine myxomatous mitral valve disease and heart failure. JAVMA 2022, 260, S61–S70. [Google Scholar] [CrossRef] [PubMed]
- Corbee, R.J. Obesity in show dogs. J. Anim. Physiol. Anim. Nutr. 2013, 97, 904–910. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assess current weight and BCS (and ideally MCS) |
| Calculate ideal body weight |
| Obtain a detailed diet history |
| Determine current daily caloric intake |
| Calculate the daily caloric requirements for weight loss using the following formulas: |
| ○ RER in kcal/day = 70 × (ideal BW [kg])0.75 (for all dogs) |
| ○ RER in kcal/day = 30 × (ideal BW [kg]) + 70 (for dogs between 2–25 kgs) |
| Calculate the safe rate of weight loss (1–2% body weight/week) |
| Make precise diet and treat recommendations |
| Prepare detailed feeding management and exercise plans |
| Schedule follow-up appointments |
| Adjust the plan as needed |
| Create a plan for ongoing maintenance once goals are achieved |
| Level of Engagement Score | Description of Engagement |
|---|---|
| 0 | Diagnosis only. No documented discussion with client in MR. |
| 1 | Basic recommendation of “…eat less and exercise more”. |
| 2 |
|
| 3 | Recommendation of 1 and 2 above plus the following:
|
| Comorbidity Classification | Diagnoses |
|---|---|
| Orthopedic | Osteoarthritis, lameness, intervertebral disc disease, cruciate ligament tear, patella luxation, neck/back pain, dysplasia, reluctant to walk, mobility issues |
| Dermatologic | Atopy, chronic dermatitis, chronic otitis, pruritus, recessed vulva, chronic anal gland infections |
| Endocrine | Hyperadrenocorticism, hypoadrenocorticism, hypothyroidism, diabetes mellitus |
| Renal/Urinary | Recurring urinary tract infections, chronic kidney disease, proteinuria, urolithiasis, urinary incontinence |
| Cardiovascular/Respiratory | Brachycephalic obstructive airway syndrome, collapsing trachea, heart murmur, respiratory distress, chronic cough |
| Neoplastic | Lymphosarcoma, hemangiosarcoma, anal gland adenocarcinoma, carcinoma, chondrosarcoma, mammary carcinoma |
| Variable | Count | Percent |
|---|---|---|
| Number | 476 | |
| Sex | ||
| Female neutered | 236 | 49.6% |
| Female intact | 10 | 2.1% |
| Male neutered | 221 | 46.4% |
| Male intact | 9 | 1.9% |
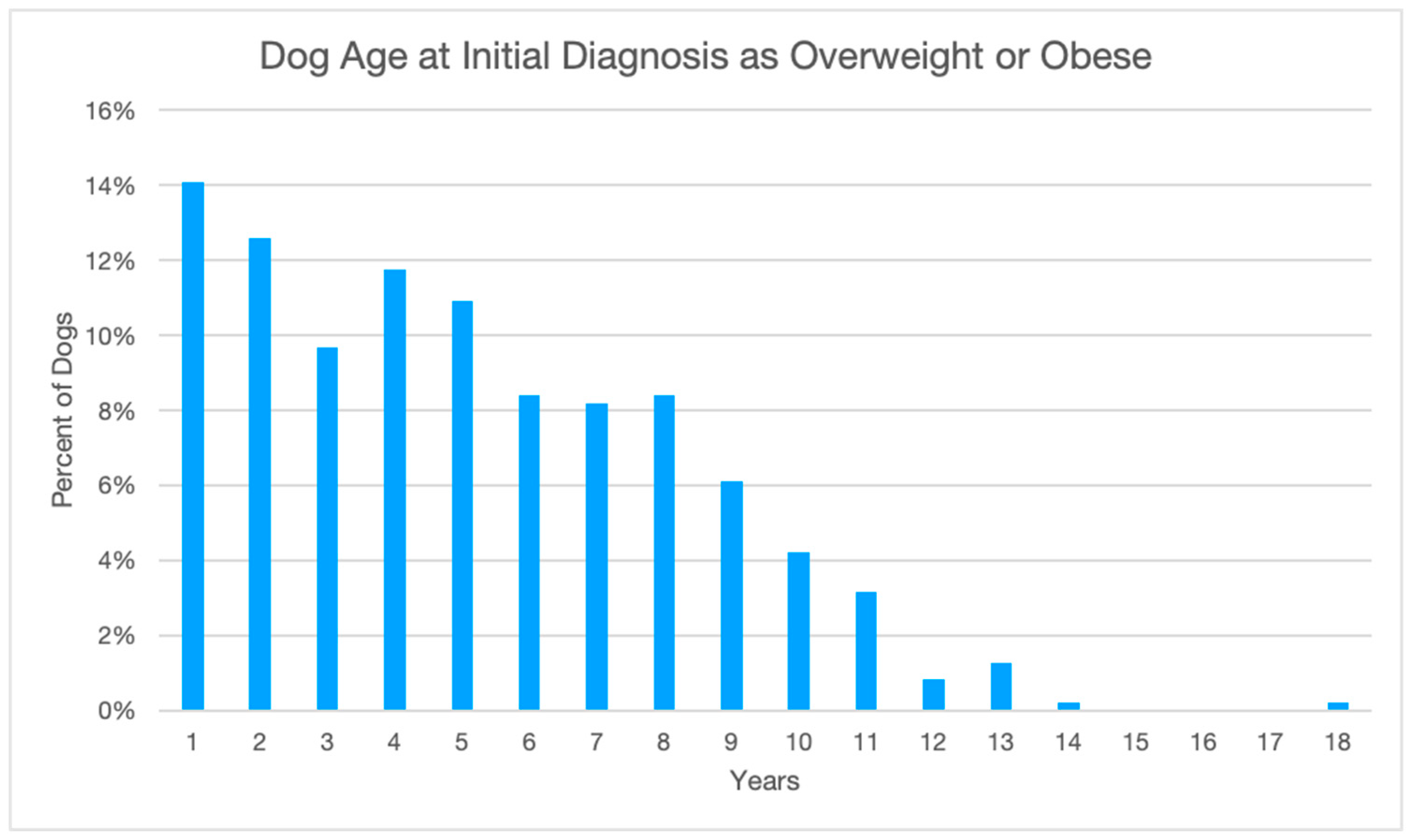
| Age (months) | ||
| Average beginning | 62 | |
| Average ending | 98 | |
| Top Breeds | ||
| Retriever, Labrador Mix | 63 | 13.2% |
| Chihuahua Mix | 48 | 10.1% |
| Shepherd Dog, German/Mix | 26 | 5.5% |
| Terrier Mix | 26 | 5.5% |
| Dachshund Mix | 19 | 4.0% |
| Retriever, Golden | 19 | 4.0% |
| Maltese Mix | 17 | 3.6% |
| Mixed Breed | 17 | 3.6% |
| Pitbull Mix | 17 | 3.6% |
| Beagle/Beagle Mix | 15 | 3.2% |
| Poodle Mix | 12 | 2.5% |
| Shih Tzu | 12 | 2.5% |
| All other | 185 | 38.9% |
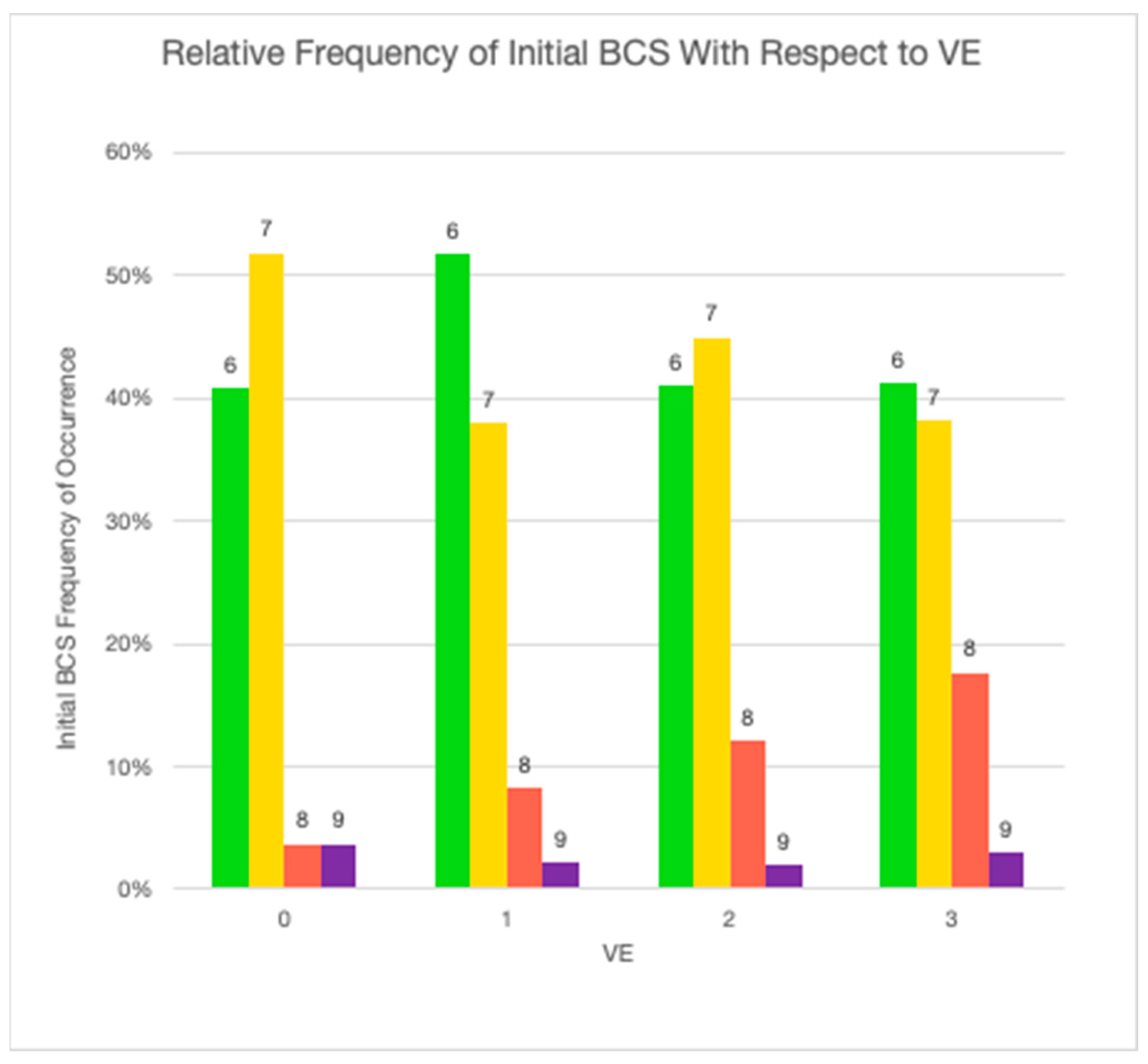
| Starting BCS | ||
| 6 | 220 | 46.2% |
| 7 | 195 | 41.0% |
| 8 | 50 | 10.5% |
| 9 | 11 | 2.3% |
| Ending BCS | ||
| 4 | 1 | 0.2% |
| 5 | 49 | 10.3% |
| 6 | 138 | 29.0% |
| 7 | 174 | 36.6% |
| 8 | 86 | 18.1% |
| 9 | 28 | 5.9% |
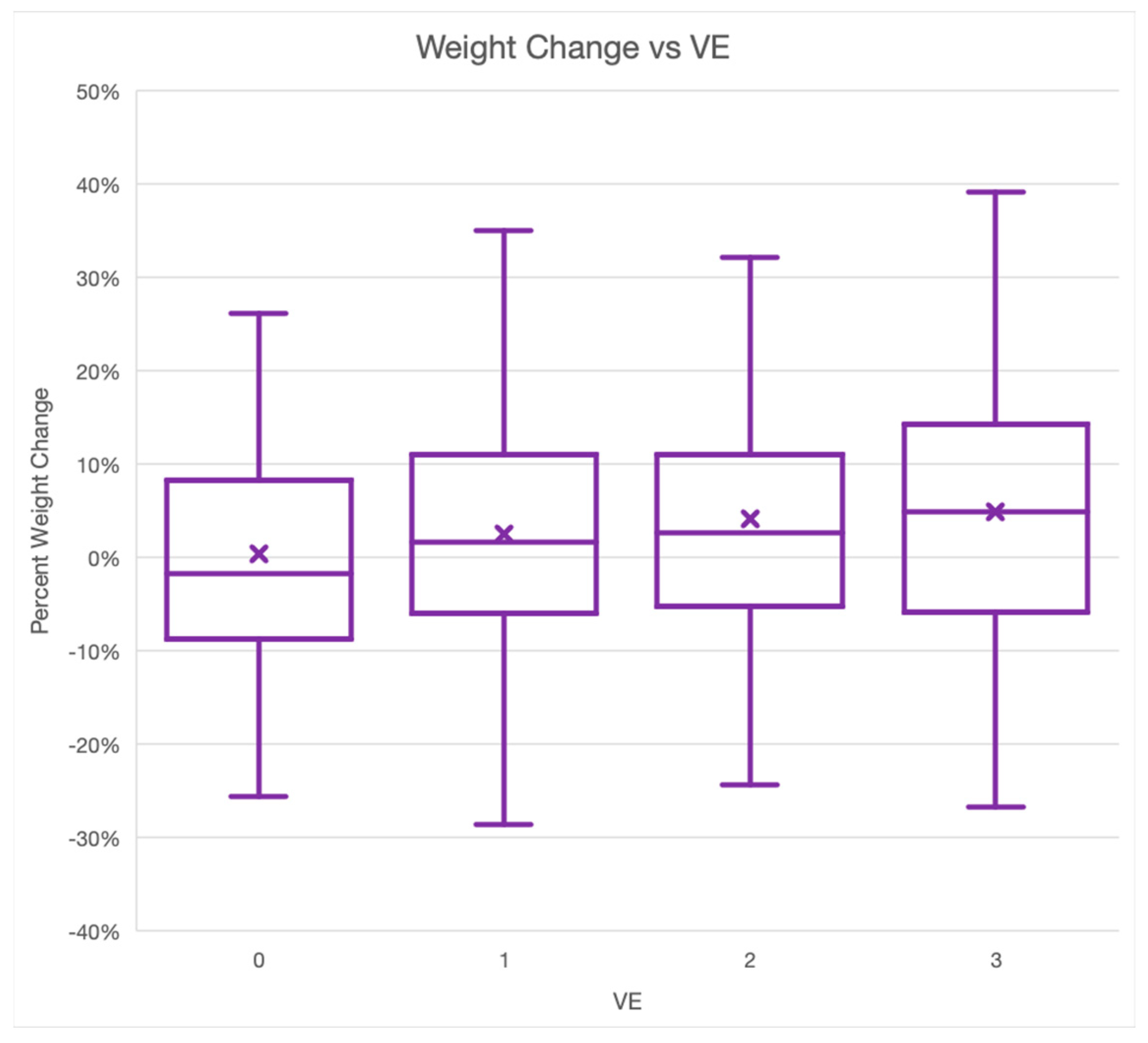
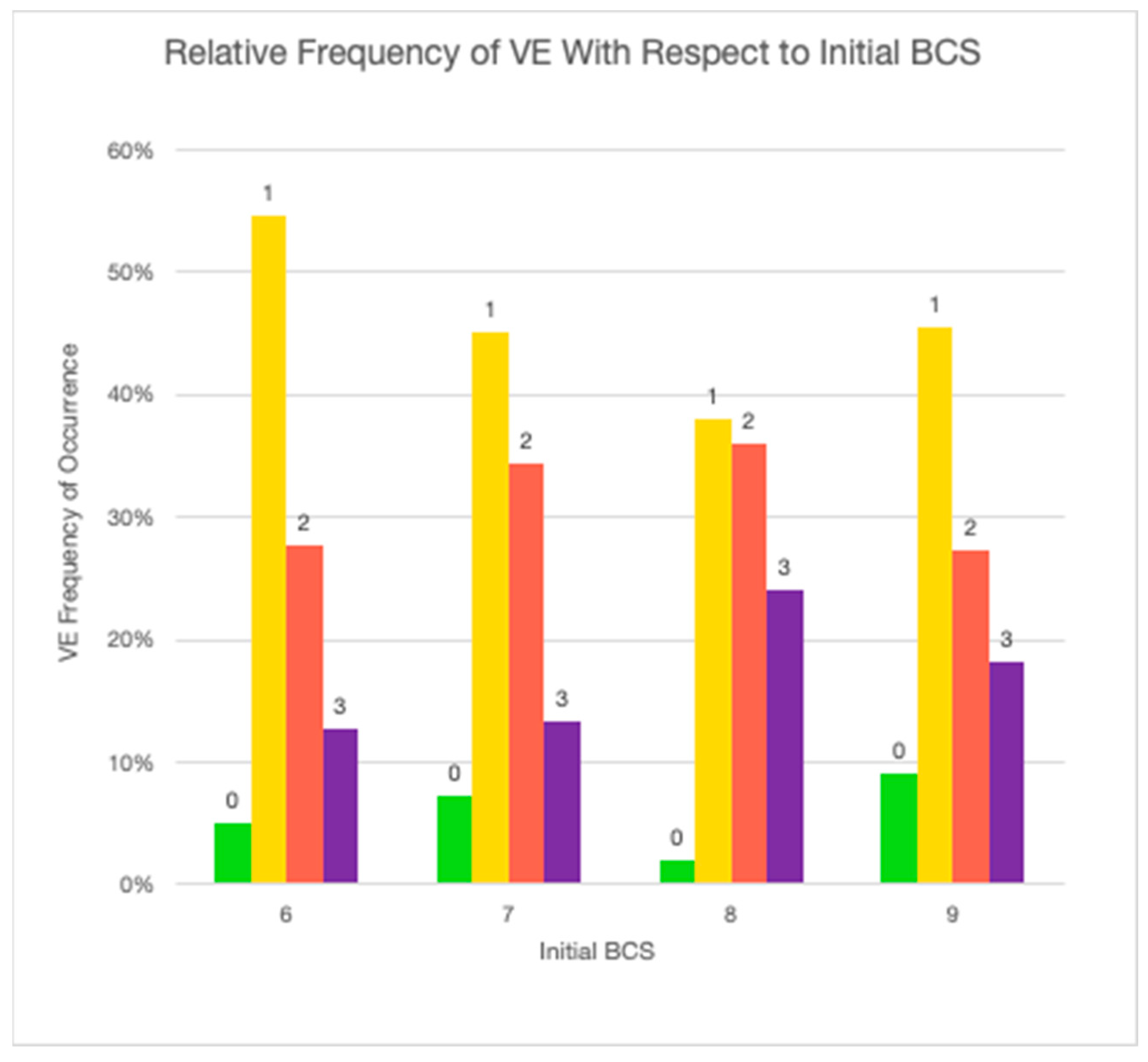
| VE Level | Overall | Lost Weight | Gained Weight | Neither | Overall Weight Change |
|---|---|---|---|---|---|
| VE 0 | 5.7% | 55.6% | 40.7% | 3.7% | 0.3% |
| Sample size | 27 | 15 | 11 | 1 | |
| % Weight change | −0.18% to −25.68% | 0.30% to 34.24% | |||
| VE 1 | 48.7% | 44.4% | 53.9% | 1.7% | 2.5% |
| Sample size | 232 | 103 | 125 | 4 | |
| % Weight change | −0.1% to −28.7% | 0.1% to 45.5% | |||
| VE 2 | 31.3% | 43.6% | 55.7% | 0.7% | 4.1% |
| Sample size | 149 | 65 | 83 | 1 | |
| % Weight change | −0.4% to −24.3% | 0.2% to 67.2% | |||
| VE 3 | 14.3% | 35.3% | 60.3% | 4.4% | 4.9% |
| Sample size | 68 | 24 | 41 | 3 | |
| % Weight change | −0.7% to −26.7% | 0.8% to 51.4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haddad, K.K. How Successful Are Veterinary Weight Management Plans for Canine Patients Experiencing Poor Welfare Due to Being Overweight and Obese? Animals 2024, 14, 740. https://doi.org/10.3390/ani14050740
Haddad KK. How Successful Are Veterinary Weight Management Plans for Canine Patients Experiencing Poor Welfare Due to Being Overweight and Obese? Animals. 2024; 14(5):740. https://doi.org/10.3390/ani14050740
Chicago/Turabian StyleHaddad, Kim K. 2024. "How Successful Are Veterinary Weight Management Plans for Canine Patients Experiencing Poor Welfare Due to Being Overweight and Obese?" Animals 14, no. 5: 740. https://doi.org/10.3390/ani14050740
APA StyleHaddad, K. K. (2024). How Successful Are Veterinary Weight Management Plans for Canine Patients Experiencing Poor Welfare Due to Being Overweight and Obese? Animals, 14(5), 740. https://doi.org/10.3390/ani14050740