
Agreement of Doppler Ultrasound and Visual Sphygmomanometer Needle Oscillation with Invasive Blood Pressure in Anaesthetised Dogs

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Instrumentation
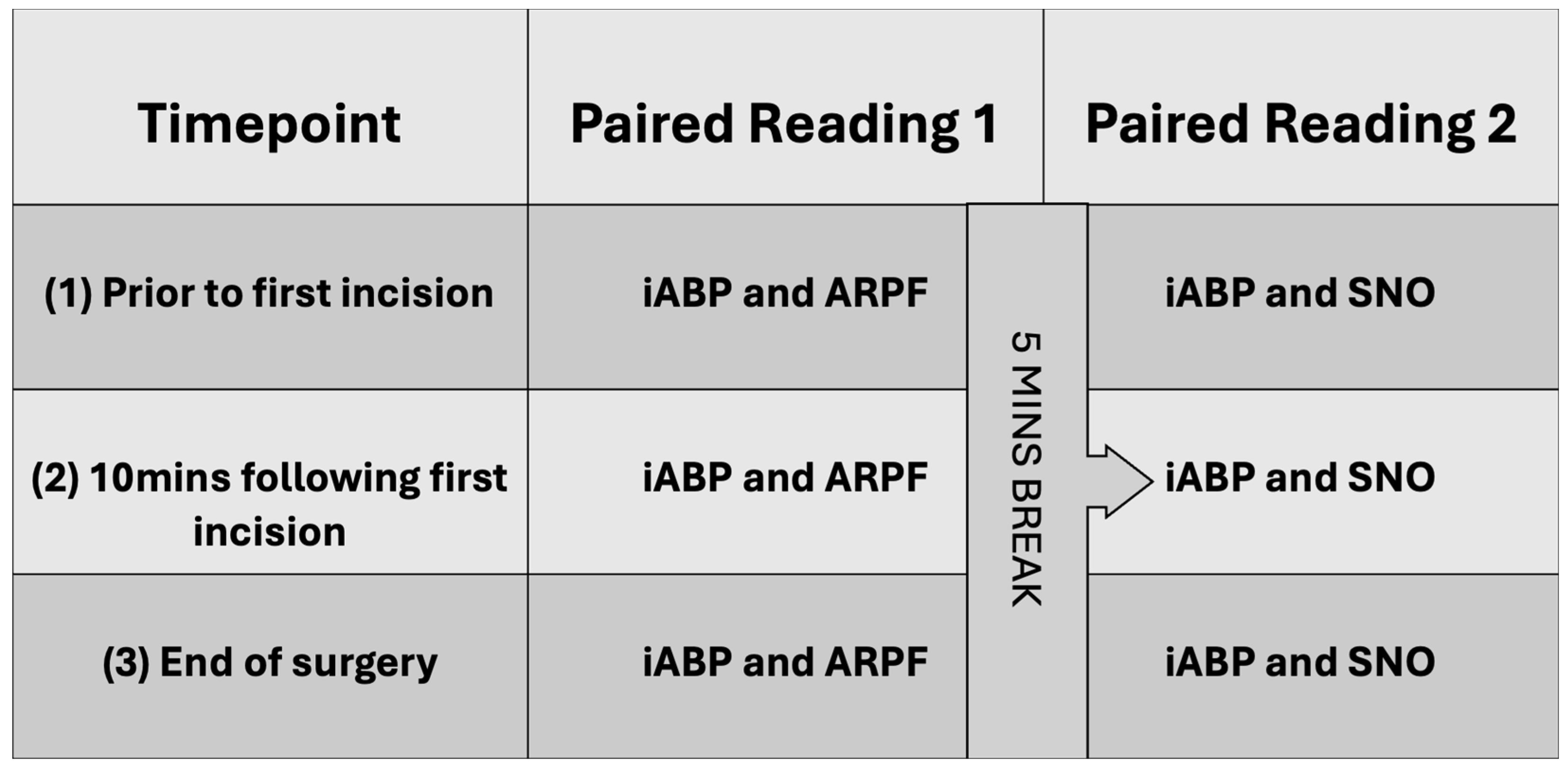
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Population
3.2. Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kittleson, M.D.; Olivier, N.B. Measurement of systemic arterial blood pressure. Vet. Clin. N. Am. Small Anim. Pract. 1983, 13, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.; Atkins, C.; Bagley, R.; Carr, A.; Cowgill, L.; Davidson, M.; Egner, B.; Elliott, J.; Henik, R.; Labato, M.; et al. Guidelines for the Identification, Evaluation, and Management of Systemic Hypertension in Dogs and Cats. J. Vet. Intern. Med. 2007, 21, 542–558. [Google Scholar] [CrossRef] [PubMed]
- Ramos, S.J.; Da Cunha, A.F.; Domingues, M.; Shelby, A.M.; Stout, R.W.; Acierno, M.J. Comparison of blood pressure measurements of anesthetized dogs obtained noninvasively with a cylindrical blood pressure cuff and an anatomically modified conical blood pressure cuff. Am. J. Vet. Res. 2016, 77, 59–64. [Google Scholar] [CrossRef] [PubMed]
- da Cunha, A.F.; Ramos, S.J.; Domingues, M.; Beaufrère, H.; Shelby, A.; Stout, R.; Acierno, M.J. Agreement between two oscillometric blood pressure technologies and invasively measured arterial pressure in the dog. Vet. Anaesth. Analg. 2016, 43, 199–203. [Google Scholar] [CrossRef]
- Vachon, C.; Belanger, M.C.; Burns, P.M. Evaluation of oscillometric and Doppler ultrasonic devices for blood pressure measurements in anesthetized and conscious dogs. Res. Vet. Sci. 2014, 97, 111–117. [Google Scholar] [CrossRef]
- Deflandre, C.J.; Hellebrekers, L.J. Clinical evaluation of the Surgivet V60046, a non invasive blood pressure monitor in anaesthetized dogs. Vet. Anaesth. Analg. 2008, 35, 13–21. [Google Scholar] [CrossRef]
- Haskins, S.C. Monitoring Anaesthetised Patients. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015. [Google Scholar]
- Skelding, A.; Valverde, A. Non–invasive blood pressure measurement in animals: Part 1—Techniques for measurement and validation of non-invasive devices. Can. Vet. J. 2020, 61, 368. [Google Scholar]
- Schauvliege, S. Chapter 7, Patient monitoring and monitoring equipment. In BSAVA Manual of Canine and Feline Anaesthesia and Analgesia, 3rd ed.; British Small Animal Veterinary Association: Quedgeley, UK, 2016; pp. 77–96. [Google Scholar]
- Garofalo, N.A.; Neto, F.J.T.; Alvaides, R.K.; de Oliveira, F.A.; Pignaton, W.; Pinheiro, R.T. Agreement between direct, oscillometric and Doppler ultrasound blood pressures using three different cuff positions in anesthetized dogs. Vet. Anaesth. Analg. 2012, 39, 324–334. [Google Scholar] [CrossRef]
- Seliškar, A.; Zrimšek, P.; Sredenšek, J.; Petrič, A.D. Comparison of high definition oscillometric and Doppler ultrasound devices with invasive blood pressure in anaesthetized dogs. Vet. Anaesth. Analg. 2013, 40, 21–27. [Google Scholar] [CrossRef]
- Bourazak, L.A.; Hofmeister, E.H. Bias, sensitivity, and specificity of Doppler ultrasonic flow detector measurement of blood pressure for detecting and monitoring hypotension in anesthetized dogs. J. Am. Vet. Med. Assoc. 2018, 253, 1433–1438. [Google Scholar] [CrossRef]
- Skelding, A.; Valverde, A. Review of non–invasive blood pressure measurement in animals: Part 2—Evaluation of the performance of non-invasive devices. Can. Vet. J. 2020, 61, 481. [Google Scholar] [PubMed]
- Trigg, S.A.; Abreu, D.; Bitton-Foronda, B.; Foley, F.C.; Gibson, A.L. Comparison of Systolic Blood Pressure Measurements by Auscultation and Visual Manometer Needle Jump. Int. J. Exerc. Sci. 2019, 12, 214–220. [Google Scholar] [PubMed]
- Stergiou, G.S.; Alpert, B.; Mieke, S.; Asmar, R.; Atkins, N.; Eckert, S.; Frick, G.; Friedman, B.; Graßl, T.; Ichikawa, T.; et al. A Universal Standard for the Validation of Blood Pressure Measuring Devices. Hypertension 2018, 71, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Acierno, M.J.; Brown, S.; Coleman, A.E.; Jepson, R.E.; Papich, M.; Stepien, R.L.; Syme, H.M. ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J. Jpn. Assoc. Vet. Nephrol. Urol. 2020, 12, 30–49. [Google Scholar] [CrossRef] [PubMed]
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. OpenEpi: Open Source Epidemiological Statistics for Public Health. Version 3.01. Available online: https://www.openepi.com/Menu/OE_Menu.htm (accessed on 18 September 2024).
- Geddes, L.; Combs, W.; Denton, W.; Whistler, S.; Bourland, J. Indirect mean arterial pressure in the anesthetized dog. Am. J. Physiol.-Heart Circ. Physiol. 1980, 238, H664–H666. [Google Scholar] [CrossRef]
- Lawrence, I.; Lin, K. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Chan, Y. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Portier, K.; Ida, K.K. The ASA Physical Status Classification: What Is the Evidence for Recommending Its Use in Veterinary Anesthesia?—A Systematic Review. Front. Vet. Sci. 2018, 5, 204. [Google Scholar] [CrossRef]
- Delegates AHo. ASA Physical Classification System. 2014. Available online: https://www.asahq.org/standards-and-practice-parameters/statement-on-asa-physical-status-classification-system (accessed on 18 September 2024).
- Cerejo, S.A.; Teixeira-Neto, F.J.; Garofalo, N.A.; Pimenta, E.L.; Zanuzzo, F.S.; Klein, A.V. Effects of cuff size and position on the agreement between arterial blood pressure measured by Doppler ultrasound and through a dorsal pedal artery catheter in anesthetized cats. Vet. Anaesth. Analg. 2020, 47, 191–199. [Google Scholar] [CrossRef]
- Chetboul, V.; Tissier, R.; Gouni, V.; de Almeida, V.; Lefebvre, H.P.; Concordet, D.; Jamet, N.; Sampedrano, C.C.; Serres, F.; Pouchelon, J.L. Comparison of Doppler ultrasonography and high-definition oscillometry for blood pressure measurements in healthy awake dogs. Am. J. Vet. Res. 2010, 71, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Moll, X.; Aguilar, A.; García, F.; Ferrer, R.; Andaluz, A. Validity and reliability of Doppler ultrasonography and direct arterial blood pressure measurements in anaesthetized dogs weighing less than 5 kg. Vet. Anaesth. Analg. 2018, 45, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.J.; Barletta, M. Agreement Between Doppler and Invasive Blood Pressure Monitoring in Anesthetized Dogs Weighing <5 kg. J. Am. Anim. Hosp. Assoc. 2015, 51, 300–305. [Google Scholar] [PubMed]
- Bosiack, A.P.; Mann, F.; Dodam, J.R.; Wagner-Mann, C.C.; Branson, K.R. Comparison of ultrasonic Doppler flow monitor, oscillometric, and direct arterial blood pressure measurements in ill dogs. J. Vet. Emerg. Crit. Care 2010, 20, 207–215. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Premedication | Induction | Maintenance | Adjunctive Infusion(s) | Blood Pressure Support—Infusion | Blood Pressure Support—Bolus |
|---|---|---|---|---|---|
| α-2 Agonist + Opioid (30) | Propofol or Alfaxalone (15) | Volatile anaesthetic (34) | Fentanyl (10) | Dopamine (7) | Glycopyrrolate (3) |
| α-2 Agonist (2) | Propofol or Alfaxalone and Midazolam (10) | Total Intravenous Anaesthesia: Propofol (1) | Dexmedetomidine (2) | Noradrenaline (6) | Ephedrine (4) |
| Acepromazine + Opioid + α-2 Agonist (1) | Propofol or Alfaxalone and Ketamine (7) | Ketamine and Fentanyl (4) | Dobutamine (2) | ||
| Opioid (2) | Propofol or Alfaxalone and Fentanyl (1) | Lidocaine (1) | |||
| Alfaxalone or Propofol and Midazolam and Fentanyl (2) | Ketamine (6) | ||||
| Fentanyl and Dexmedetomidine (2) | |||||
| Fentanyl & Ketamine and Dexmedetomidine (1) |
| Agreement | CCC (95% CI) | Mean Difference mmHg (95% LOAs) | ARPF Readings < 10 mmHg of iSAP (95% CI) | SNO Readings < 20 mmHg of iSAP (95% CI) |
|---|---|---|---|---|
| ARPF vs. iSAP (Average) | 0.40 (0.26–0.54) | −13.1 (−62.2–35.9) | 37.5% (28.6%–47.3%) | 54.8% (45.1%–64.2%) |
| ARPF vs. iSAP (timepoint 1) | 0.39 (0.14–0.64) | −18.4 (−77.4–40.7) | 31.4% (18.2%–48.5%) | 45.7% (30.1%–62.3%) |
| ARPF vs. iSAP (timepoint 2) | 0.37 (0.11–0.64) | −12.0 (−70.8–46.8) | 37.1% (22.8%–54.2%) | 57.1% (40.4–72.4) |
| ARPF vs. iSAP (timepoint 3) | 0.41 (0.15–0.67) | −12.1 (−54.2–30.0) | 44.1% (28.5%–61.0%) | 61.8% (44.5–76.4) |
| Agreement | CCC (95% CI) | Mean Difference mmHg (95% LOAs) | SNO Readings < 10 mmHg of iSAP (95% CI) | SNO Readings < 20 mmHg of iSAP (95% CI) |
|---|---|---|---|---|
| SNO vs. iSAP (Average) | 0.50 (0.36–0.64) | −9.7 (−51.3–31.9) | 38.3% (28.9–48.6) | 76.6% (66.9–84.1) |
| SNO vs. iSAP (timepoint 1) | 0.54 (0.30–0.78) | −6.7 (−46.9–33.5) | 39.4% (24.3–56.9) | 72.7% (55.1–85.3) |
| SNO vs. iSAP (timepoint 2) | 0.50 (0.27–0.74) | −13.2 (−56.2–29.8) | 40.6% (25.1–58.3) | 75.0% (57.1–87.1) |
| SNO vs. iSAP (timepoint 3) | 0.45 (0.17–0.72) | −9.3 (−51.1–32.5) | 34.5% (19.5–53.3) | 82.8 (64.4–92.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armour, M.; Michou, J.; Schofield, I.; Borland, K. Agreement of Doppler Ultrasound and Visual Sphygmomanometer Needle Oscillation with Invasive Blood Pressure in Anaesthetised Dogs. Animals 2024, 14, 2756. https://doi.org/10.3390/ani14192756
Armour M, Michou J, Schofield I, Borland K. Agreement of Doppler Ultrasound and Visual Sphygmomanometer Needle Oscillation with Invasive Blood Pressure in Anaesthetised Dogs. Animals. 2024; 14(19):2756. https://doi.org/10.3390/ani14192756
Chicago/Turabian StyleArmour, Marc, Joanne Michou, Imogen Schofield, and Karla Borland. 2024. "Agreement of Doppler Ultrasound and Visual Sphygmomanometer Needle Oscillation with Invasive Blood Pressure in Anaesthetised Dogs" Animals 14, no. 19: 2756. https://doi.org/10.3390/ani14192756
APA StyleArmour, M., Michou, J., Schofield, I., & Borland, K. (2024). Agreement of Doppler Ultrasound and Visual Sphygmomanometer Needle Oscillation with Invasive Blood Pressure in Anaesthetised Dogs. Animals, 14(19), 2756. https://doi.org/10.3390/ani14192756