
Hymenoptera Venom Immunotherapy in Dogs: Safety and Clinical Efficacy
 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
- Moderate or severe anaphylactic reaction, following an observed or suspected bee and/or wasp sting (grading system is shown in Table 1).
- A positive bee- and/or wasp-specific IgE serology or skin test.
2.2. Anaphylaxis Grading Scale
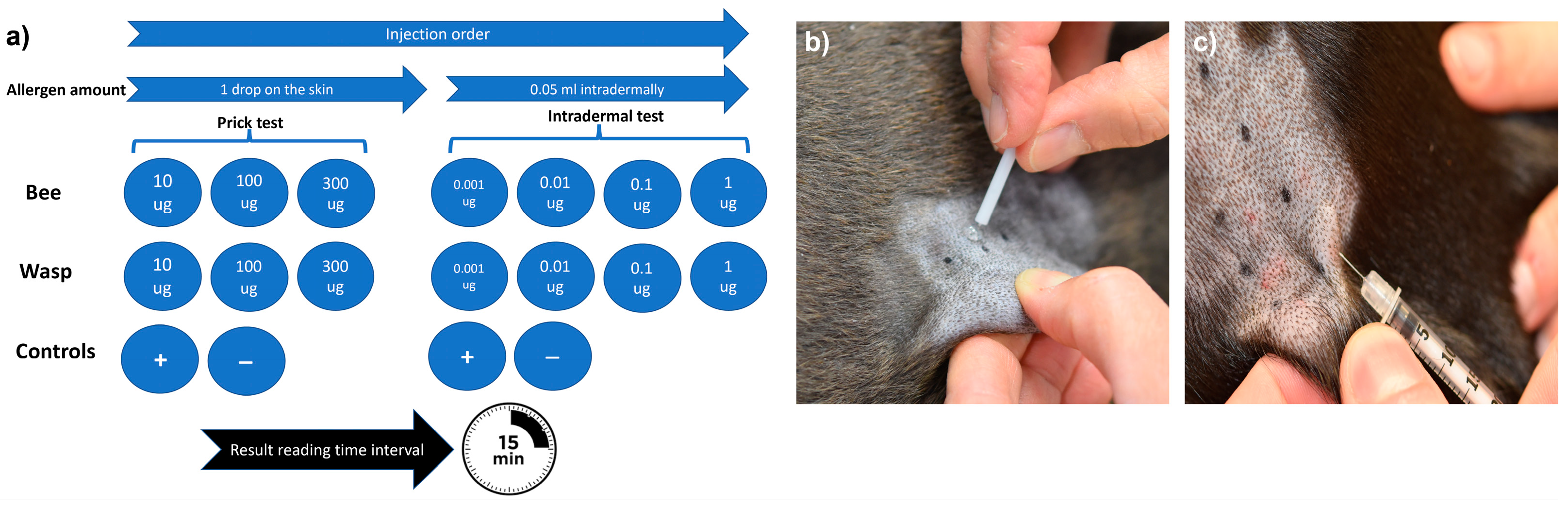
2.3. Allergy Testing
2.4. Allergen Selection for VIT
2.5. Protocol(s) for VIT
2.6. Safety and Efficacy Evaluation
2.7. Endpoints and Statistics
3. Results
3.1. Demographic and Clinical Data
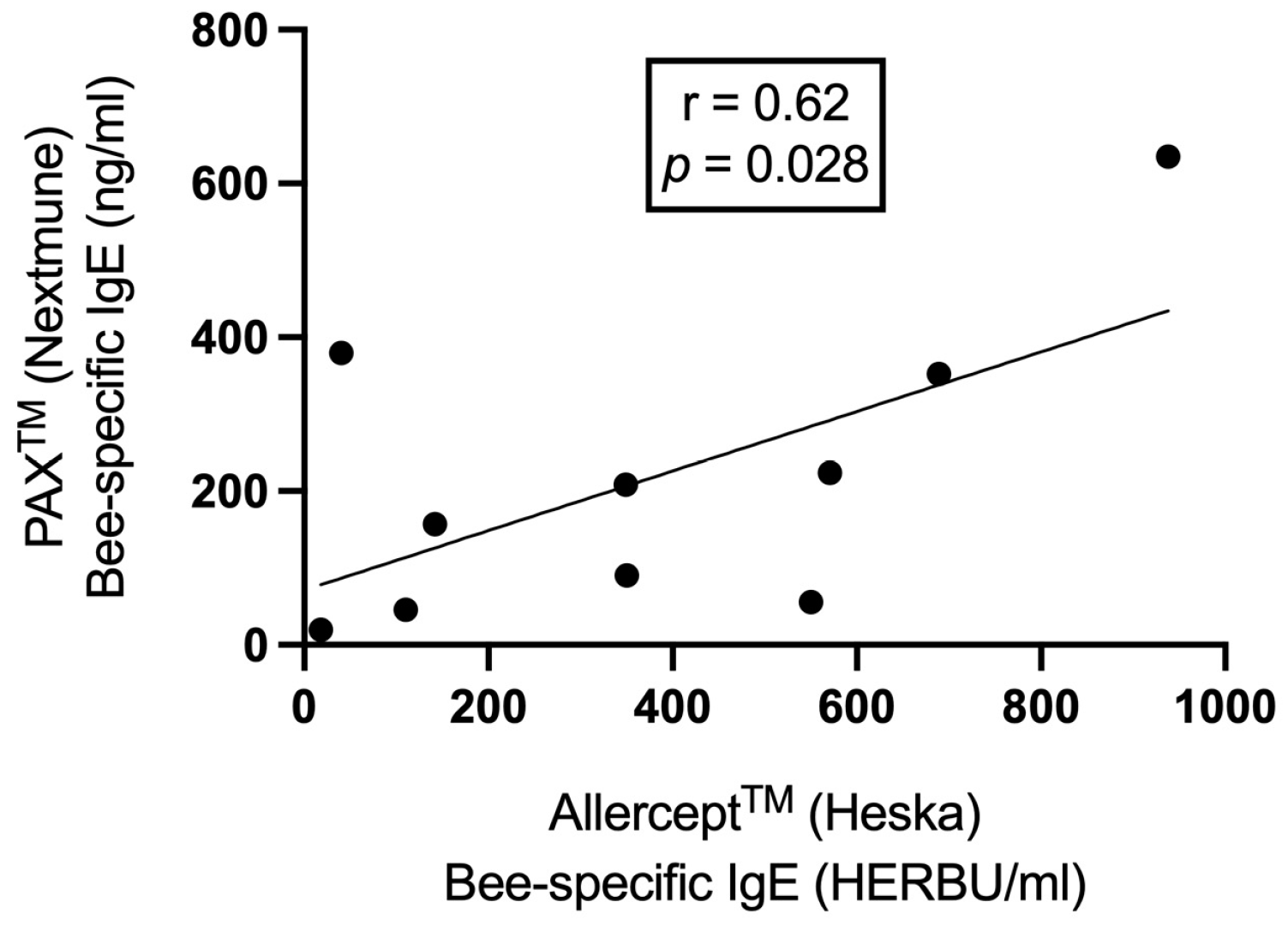
3.2. Data from In Vitro and In Vivo Allergic Testing
3.3. Data on Venom Immunotherapy Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bilo, B.M.; Bonifazi, F. Epidemiology of insect-venom anaphylaxis. Curr. Opin. Allergy Clin. Immunol. 2008, 8, 330–337. [Google Scholar] [CrossRef]
- Jennings, A.; Duggan, E.; Perry, I.J.; Hourihane, J.O.B. Epidemiology of allergic reactions to hymenoptera stings in Irish school children. Pediatr. Allergy Immunol. 2010, 21, 1166–1170. [Google Scholar] [CrossRef] [PubMed]
- Rostaher, A. Bienen-und Wespengiftallergien bei Hunden–Von der Akutbehandlung bis zur Desensibilisierung. Kleintier Konkret 2018, 21, 13–19. [Google Scholar] [CrossRef][Green Version]
- Rostaher, A.; Hofer-Inteeworn, N.; Kümmerle-Fraune, C.; Fischer, N.M.; Favrot, C. Triggers, risk factors and clinico-pathological features of urticaria in dogs—A prospective observational study of 24 cases. Vet. Dermatol. 2017, 28, 39–46. [Google Scholar] [CrossRef]
- Antonicelli, L.; Bilo, M.B.; Bonifazi, F. Epidemiology of Hymenoptera allergy. Curr. Opin. Allergy Clin. Immunol. 2002, 2, 341–346. [Google Scholar] [CrossRef]
- Elremeli, M.; Bulsara, M.K.; Daniels, M.; Boyle, R.J. Venom immunotherapy for preventing allergic reactions to insect stings. Cochrane Database Syst. Rev. 2012, 10, CD008838. [Google Scholar]
- Pumphrey, R.S. Lessons for management of anaphylaxis from a study of fatal reactions. Clin. Exp. Allergy 2000, 30, 1144–1150. [Google Scholar] [CrossRef]
- Adams, K.E.; Tracy, J.M.; Golden, D.B. Anaphylaxis to Stinging Insect Venom. Immunol. Allergy Clin. N. Am. 2022, 42, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Golden, D.B.; Kagey-Sobotka, A.; Norman, P.S.; Hamilton, R.G.; Lichtenstein, L.M. Outcomes of Allergy to Insect Stings in Children, with and without Venom Immunotherapy. N. Engl. J. Med. 2004, 351, 668–674. [Google Scholar] [CrossRef]
- Hunt, K.J.; Valentine, M.D.; Sobotka, A.K.; Benton, A.W.; Amodio, F.J.; Lichtenstein, L.M. A Controlled Trial of Immunotherapy in Insect Hypersensitivity. N. Engl. J. Med. 1978, 299, 157–161. [Google Scholar] [CrossRef]
- Sturm, G.J.; Varga, E.M.; Roberts, G.; Mosbech, H.; Bilò, M.B.; Akdis, C.A.; Antolín-Amérigo, D.; Cichocka-Jarosz, E.; Gawlik, R.; Jakob, T.; et al. EAACI guidelines on allergen immunotherapy: Hymenoptera venom allergy. Allergy 2018, 73, 744–764. [Google Scholar] [CrossRef]
- Bilo, B.M.; Rueff, F.; Mosbech, H.; Bonifazi, F.; Oude-Elberink, J.N.G.; Eaaci Interest Grp Insect Venom the EAACI Interest Group on Insect Venom Hypersensitivity. Diagnosis of Hymenoptera venom allergy. Allergy 2005, 60, 1339–1349. [Google Scholar] [CrossRef]
- Hoffman, D.R.; Jacobson, R.S. Allergens in hymenoptera venom XII: How much protein is in a sting? Ann. Allergy 1984, 52, 276–278. [Google Scholar]
- Goldberg, A.; Confino-Cohen, R. Bee venom immunotherapy—How early is it effective? Allergy 2010, 65, 391–395. [Google Scholar] [CrossRef]
- Lerch, E.; Muller, U.R. Long-term protection after stopping venom immunotherapy: Results of re-stings in 200 patients. J. Allergy Clin. Immunol. 1998, 101, 606–612. [Google Scholar] [CrossRef]
- Ruëff, F.; Vos, B.; Oude Elberink, J.; Bender, A.; Chatelain, R.; Dugas-Breit, S.; Horny, H.-P.; Küchenhoff, H.; Linhardt, A.; Mastnik, S.; et al. Predictors of clinical effectiveness of Hymenoptera venom immunotherapy. Clin. Exp. Allergy 2014, 44, 736–746. [Google Scholar] [CrossRef]
- Apostolopoulos, N.; Mayer, U. Hymenoptera venom immunotherapy without human serum albumin as a stabilizer in a canine patient. Vet. Rec. Case Rep. 2021, 9, e13. [Google Scholar] [CrossRef]
- Boord, M. Venomous Insect Hypersensitivity. In Veterinary Allergy Somerset, 1st ed.; Chapter 29; Noli, C., Foster, A.P., Rosenkrantz, W., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2014; pp. 191–194. [Google Scholar]
- Bryden, S. Venom allergy in dogs: A multicentre retrospective study. Proc. Aust. Coll. Vet. Sci. Dermatol. Chapter Sci. Week 2009. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://ripehosting.blob.core.windows.net/anzcvs-prod-media/2372/acvs-dermatology-chapter-proceedings-2009-bryden-venom-allergy.pdf (accessed on 17 September 2023).
- Ewing, T.S.; Dong, C.; Boord, M.J.; Fang, Y. Adverse events associated with venomous insect immunotherapy and clinical outcomes in 82 dogs (2002–2020). Vet. Dermatol. 2021, 33, 40-e14. [Google Scholar] [CrossRef] [PubMed]
- Rostaher, A.; Mueller, R.S.; Meile, L.; Favrot, C.; Fischer, N.M. Venom immunotherapy for Hymenoptera allergy in a dog. Vet. Dermatol. 2021, 32, 206-e252. [Google Scholar] [CrossRef]
- Moore, A.; Burrows, A.K.; Rosenkrantz, W.S.; Ghubash, R.M.; Hosgood, G. Modified rush venom immunotherapy in dogs with Hymenoptera hypersensitivity. Vet. Dermatol. 2023. [Google Scholar] [CrossRef]
- Stedman, K.; Lee, K.; Hunter, S.; Rivoire, B.; McCall, C.; Wassom, D. Measurement of canine IgE using the alpha chain of the human high affinity IgE receptor. Vet. Immunol. Immunopathol. 2001, 78, 349–355. [Google Scholar] [CrossRef]
- Hensel, P.; Santoro, D.; Favrot, C.; Hill, P.; Griffin, C. Canine atopic dermatitis: Detailed guidelines for diagnosis and allergen identification. BMC Vet. Res. 2015, 11, 196. [Google Scholar] [CrossRef]
- Gouel-Chéron, A.; Harpan, A.; Mertes, P.-M.; Longrois, D. Management of anaphylactic shock in the operating room. La Presse Médicale 2016, 45, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Rueff, F.; Przybilla, B. Stichprovokation. Indik. Und Durchführung. Hautarzt 2014, 65, 796–801. [Google Scholar] [CrossRef]
- Novak, N.; Mete, N.; Bussmann, C.; Maintz, L.; Bieber, T.; Akdis, M.; Zumkehr, J.; Jutel, M.; Akdis, C. Early suppression of basophil activation during allergen-specific immuno-therapy by histamine receptor 2. J. Allergy Clin. Immunol. 2012, 130, 1153–1158.e1152. [Google Scholar] [CrossRef]
- Confino-Cohen, R.; Melamed, S.; Goldberg, A. Debilitating beliefs, emotional distress and quality of life in patients given immunotherapy for insect sting allergy. Clin. Exp. Allergy 1999, 29, 1626–1631. [Google Scholar] [CrossRef] [PubMed]
- Oude Elberink, J.N.; de Monchy, J.G.; van der Heide, S.; Guyatt, G.H.; Dubois, A.E. Venom immunotherapy improves health-related quality of life in patients allergic to yellow jacket venom. J. Allergy Clin. Immun. 2002, 110, 174–182. [Google Scholar] [CrossRef]
- Eitel, T.; Zeiner, K.N.; Assmus, K.; Ackermann, H.; Zoeller, N.; Meissner, M.; Kaufmann, R.; Kippenberger, S.; Valesky, E.M. Impact of specific immunotherapy and sting challenge on the quality of life in patients with hymenoptera venom allergy. World Allergy Organ. J. 2021, 14, 100536. [Google Scholar] [CrossRef]
- Fischer, J.; Teufel, M.; Feidt, A.; Giel, K.E.; Zipfel, S.; Biedermann, T. Tolerated wasp sting challenge improves health-related quality of life in patients allergic to wasp venom. J. Allergy Clin. Immunol. 2013, 132, 489–490. [Google Scholar] [CrossRef] [PubMed]
- Elberink, J.N.O.; Van der Heide, S.; Guyatt, G.H.; Dubois, A.E. Analysis of the burden of treatment in patients receiving an EpiPen for yellow jacket anaphylaxis. J. Allergy Clin. Immun. 2006, 118, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Findeis, S.; Craig, T. The relationship between insect sting allergy treatment and patient anxiety and depression. Allergy Asthma Proc. 2014, 35, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Luzar, A.D.; Korošec, P.; Košnik, M.; Zidarn, M.; Rijavec, M. Hymenoptera Venom Immunotherapy: Immune Mechanisms of Induced Protection and Tolerance. Cells 2021, 10, 1575. [Google Scholar] [CrossRef]
- Navas, A.; Ruiz-Leon, B.; Serrano, P.; Martí, M.; Espinazo, M.L.; Blanco, N.; Molina, J.; Alonso, C.; Jurada, A.; Moreno-Aguilar, C. Natural and Induced Tolerance to Hymenoptera Venom: A Single Mech-anism? Toxins 2022, 14, 426. [Google Scholar] [CrossRef]
- Aßmus, K.; Meissner, M.; Kaufmann, R.; Valesky, E.M. Benefits and limitations of sting challenge in hymenoptera venom allergy. Allergol. Sel. 2021, 5, 45–50. [Google Scholar] [CrossRef]
- Rueff, F.; Przybilla, B. Sting challenge: Indications and execution. Hautarzt 2014, 65, 796–801. [Google Scholar] [PubMed]
- Muller, U.; Hari, Y.; Berchtold, E. Premedication with antihistamines may enhance efficacy of specific-allergen immunotherapy. J. Allergy Clin. Immunol. 2001, 107, 81–86. [Google Scholar] [CrossRef]
- Brockow, K.; Kiehn, M.; Riethmüller, C.; Vieluf, D.; Berger, J.; Ring, J. Efficacy of antihistamine pretreatment in the prevention of adverse reactions to Hymenoptera immunotherapy: A prospective, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 1997, 100, 458–463. [Google Scholar] [CrossRef]
- Wang, K.Y.; Friedman, D.F.; DaVeiga, S.P. Immediate hypersensitivity reaction to human serum albumin in a child undergoing plasmapheresis. Transfusion 2019, 59, 1921–1923. [Google Scholar] [CrossRef]
- Stoevesandt, J.; Hofmann, B.; Hain, J.; Kerstan, A.; Trautmann, A. Single venom-based immunotherapy effectively protects patients with double positive tests to honey bee and Vespula venom. Allergy Asthma Clin. Immunol. 2013, 9, 33. [Google Scholar] [CrossRef]
- Blank, S.; Bilò, M.B.; Grosch, J.; Schmidt-Weber, C.B.; Ollert, M.; Jakob, T. Marker allergens in Hymenoptera venom allergy—Characteristics and potential use in precision medicine. Allergo J. Int. 2021, 30, 26–38. [Google Scholar] [CrossRef]
- Sturm, G.J.; Kranzelbinder, B.; Schuster, C.; Sturm, E.M.; Bokanovic, D.; Vollmann, J.; Crailsheim, K.; Hemmer, W.; Aberer, W. Sensitization to Hymenoptera venoms is common, but systemic sting reactions are rare. J. Allergy Clin. Immunol. 2014, 133, 1635–1643.e1. [Google Scholar] [CrossRef]
- Hollstein, M.M.; Matzke, S.S.; Lorbeer, L.; Forkel, S.; Fuchs, T.; Lex, C.; Buhl, T. Intracutaneous Skin Tests and Serum IgE Levels Cannot Predict the Grade of Anaphylaxis in Patients with Insect Venom Allergies. J. Asthma Allergy 2022, 15, 907–918. [Google Scholar] [CrossRef] [PubMed]
- Sahiner, U.M.; Durham, S.R. Hymenoptera Venom Allergy: How Does Venom Immunotherapy Prevent Anaphylaxis from Bee and Wasp Stings? Front. Immunol. 2019, 10, 1969. [Google Scholar] [CrossRef]
- Strohmeier, B.; Aberer, W.; Bokanovic, D.; Komericki, P.; Sturm, G.J. Simultaneous intradermal testing with hymenoptera venoms is safe and more efficient than sequential testing. Allergy 2013, 68, 542–544. [Google Scholar] [CrossRef] [PubMed]
- Feindor, M.; Heath, M.D.; Hewings, S.J.; Carreno Velazquez, T.L.; Blank, S.; Grosch, J.; Jakob, T.; Schmid-Grendelmeier, P.; Klimmek, L.; Glden, D.B.K.; et al. Venom Immunotherapy: From Proteins to Product to Patient Protection. Toxins 2021, 13, 616. [Google Scholar] [CrossRef]
- Alessandrini, A.E.; Berra, D.; Rizzini, F.L.; Mauro, M.; Melchiorre, A.; Rossi, F.; Spezia, D.; Stanizzi, R.; Ricciardi, L.; Burastero, S.E. Flexible approaches in the design of subcutaneous immunotherapy protocols for Hymenoptera venom allergy. Ann. Allergy Asthma Immunol. 2006, 97, 92–97. [Google Scholar] [CrossRef]
- Pospischil, I.; Kagerer, M.; Cozzio, A.; Angelova-Fischer, I.; Guenova, E.; Ballmer-Weber, B.; Hoetzenecker, W. Comparison of the safety profiles of three different Hymenoptera venom immunotherapy protocols—A retrospective two-center study of 143 patients. Exp. Dermatol. 2021, 30, E3. [Google Scholar]
- Golden, D.B.K.; Valentine, M.D.; Kagey-Sobotka, A.; Lichtenstein, L.M. Regimens of Hymenoptera Venom Immunotherapy. Ann. Intern. Med. 1980, 92, 620–624. [Google Scholar] [CrossRef]
- Confino-Cohen, R.; Rosman, Y.; Goldberg, A. Rush Venom Immunotherapy in Children. J. Allergy Clin. Immunol. Pract. 2017, 5, 799–803. [Google Scholar] [CrossRef]
- Ruëff, F.; Przybilla, B.; Biló, M.B.; Müller, U.; Scheipl, F.; Aberer, W.; Birnbaum, J.; Bodzenta-Lukaszyk, A.; Bonifazi, F.; Bucher, C.; et al. Predictors of side effects during the buildup phase of venom immunotherapy for Hymenoptera venom allergy: The importance of baseline serum tryptase. J. Allergy Clin. Immunol. 2010, 126, 105–111.e5. [Google Scholar] [CrossRef] [PubMed]
- Roumana, A.; Pitsios, C.; Vartholomaios, S.; Kompoti, E.; Kontou-Fili, K. The safety of initiating Hymenoptera immunotherapy at 1 mu g of venom extract. J. Allergy Clin. Immun. 2009, 124, 379–381. [Google Scholar] [CrossRef]
- Simioni, L.; Vianello, A.; Bonadonna, P.; Marcer, G.; Severino, M.; Pagani, M.; Morlin, L.; Crivellaro, M.; Passalacqua, G. Efficacy of venom immunotherapy given every 3 or 4 months: A prospective comparison with the conventional regimen. Ann. Allergy Asthma Immunol. 2013, 110, 51–54. [Google Scholar] [CrossRef]
- Rueff, F.; Wenderoth, A.; Przybilla, B. Patients still reacting to a sting challenge while receiving conventional Hy-menoptera venom immunotherapy are protected by increased venom doses. J. Allergy Clin. Immunol. 2001, 108, 1027–1032. [Google Scholar] [CrossRef]
- Golden, D.B.; Kwiterovich, K.A.; Kagey-Sobotka, A.; Valentine, M.D.; Lichtenstein, L.M. Discontinuing venom immunotherapy: Outcome after five years. J. Allergy Clin. Immunol. 1996, 97, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Keating, M.; Kagey-Sobotka, A.; Hamilton, R.; Yunginger, J. Clinical and immunologic follow-up of patients who stop venom immunotherapy. J. Allergy Clin. Immunol. 1991, 88, 339–348. [Google Scholar] [CrossRef]
- Golden, D.B.; Kwiterovich, K.A.; Kagey-Sobotka, A.; Lichtenstein, L.M. Discontinuing venom immunotherapy: Extended observations. J. Allergy Clin. Immunol. 1998, 101, 298–305. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Grade | Organ System Involved | Clinical Findings |
|---|---|---|
| 1—mild | Skin | Generalized erythema, urticaria and/or angioedema |
| 2—moderate | Gastrointestinal, respiratory ± skin | Dyspnea, stridor, wheeze, nausea, vomiting and/or abdominal pain ± above findings |
| 3—severe | Respiratory, cardiovascular, neurological ± skin ± gastrointestinal, respiratory | Cyanosis, pallor, SpO2 < 92%, hypotension (systolic blood pressure < 90 mmHg), collapse, loss of consciousness and/or incontinence ± above findings |
| Injection No. | Allergen Amount (µg) | Concentration (µg/mL) | Injection Volume (mL) | Observation Time (Minutes) | |
|---|---|---|---|---|---|
| Day 1 | 1 | 0.1 | 1 | 0.1 | 20 |
| 2 | 1 | 10 | 0.1 | 20 | |
| 3 | 10 | 100 | 0.1 | 20 | |
| 4 | 20 | 100 | 0.2 | 20 | |
| 5 | 30 | 100 | 0.3 | 20 | |
| 6 | 40 | 100 | 0.4 | 20 | |
| Day 7 | 7 | 50 | 100 | 0.5 | 20 |
| 8 | 50 | 100 | 0.5 | 20 |
| Signalment at VIT Initiation | Clinical Data Related to the Sting Event | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dog No | Breed | Age (Years) | Sex | Castration Status | Weight (kg) | No. of Sting Episodes | No. of Anaphylaxis Episodes | Age 1st Sting (Years) | Age 1st Anaphylaxis Episode (Years) | Reaction Severity (1st Sting) | Reaction Severity (Last Sting) |
| 1 | Boxer | 3.0 | female | intact | 28.6 | 2 | 2 | 0.75 | 2.8 | 2 | 3 |
| 2 | Toy poodle | 2.0 | male | intact | 3 | 1 | 1 | 1.75 | 1.75 | 3 | N/A |
| 3 | Dachshund | 4.0 | female | spayed | 5.8 | 2 | 2 | 3.9 | 4 | 2 | 3 |
| 4 | Dachshund | 1.0 | female | spayed | 5.2 | 2 | 2 | 0.75 | 0.8 | 2 | 3 |
| 5 | Entlebucher Sennenhund | 1.0 | female | spayed | 18.3 | 1 | 1 | 1 | 1 | 3 | N/A |
| 6 | Yorkshire Terrier | 2.2 | female | spayed | 4.1 | 2 | 2 | 1 | 1.2 | 2 | 3 |
| 7 | Cross-breed | 7.4 | male | castrated | 10.5 | 1 | 1 | 7 | 7 | 3 | N/A |
| 8 | Malinois | 3.1 | female | spayed | 25.1 | 3 | 2 | 1.1 | 1.3 | 1 | 2 |
| 9 | Doberman | 0.8 | male | intact | 31.2 | 1 | 1 | 0.6 | 0.6 | 3 | N/A |
| 10 | Beagle | 8.0 | female | spayed | 13.9 | 3 | 3 | 4 | 4 | 3 | 3 |
| Dog No. | Bee Allergens | Wasp Allergens | Insect Identification by Owner | Time Interval Sting to Testing | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Prick | IDT | Serology | Prick | IDT | Serology | |||||
| Positive at Following Concentrations (µg/mL) | Allercept (HERBU/mL) | PAX (ng/mL) | Positive at Following Concentrations (µg/mL) | Allercept (HERBU/mL) | PAX (ng/mL) | |||||
| 1 | Neg. | 1 | 142 | 156.67 | Neg. | Neg. | 116 | 28.02 | Bee | 4 weeks |
| 2 | 100–300 | 1 | 350 | 90.54 | Neg. | Neg. | 84 | 27.2 | Bee | 3 weeks |
| 3 | Neg. | Neg. | 938 | 634.7 | Neg. | Neg. | 45 | 23.62 | Bee | 10 days |
| 4 | Neg. | 0.01–1 | 349 | 208.14 | Neg. | 0.01–1 | 16 | 32.22 | Bee | 5 weeks |
| 5 | Neg. | 0.01–1 | 110 | 45.77 | Neg. | 0.01–1 | 16 | 27.82 | Bee | 6 weeks |
| 6 | 10–300 | 1 | 40 | 379.62 | Neg. | Neg. | 2 | 25.26 | Bee | 1 year |
| 7 | 300 | 0.1–1 | 550 | 55.95 | Neg. | 0.1–1 | 36 | 27.33 * | Bee | 4 months |
| 8 | Neg. | 0.01–1 | 689 | 352 | Neg. | Neg. | 23 | 27 | Bee | 2 months |
| 9 | Neg. | Neg. | 18 | 19.81 | Neg. | 1 | 18 | 25.45 | Wasp | 4 weeks |
| 10 | Neg. | 0.01–1 | 571 | 223.44 | Neg. | 1 | 427 | 66.02 | Bee and wasp | 1 year |
| Dog No. | PAX Results in Bee-Allergic Dogs | |||||
|---|---|---|---|---|---|---|
| Bee Extract | Bee Allergen Components | |||||
| Api m | nApi m 1 | rApi m 2 | rApi m 3 | rApi m 5 | rApi m 10 | |
| 1 | 156.67 | 227.91 | 82.79 | 31.33 | 20.66 | 577.49 |
| 2 | 90.54 | 132.83 | 633.33 | 110.07 | 19.11 | 633.33 |
| 3 | 634.7 | 722.22 | 111.15 | 804.65 | 18.3 | 1478.85 |
| 4 | 208.14 | 592.32 | 853.02 | 987.17 | 21.57 | 1061.81 |
| 5 | 45.77 | 42.55 | 33.8 | 24.04 | 19.35 | 167.46 |
| 6 | 379.62 | 958.41 | 20.35 | 82.96 | 19.52 | 23.18 |
| 7 | 55.95 | 55.95 | 57.91 | 128.53 | 18.81 | 133.62 |
| 8 | 352 | 386 | 344 | 60 | 22 | 1657 |
| 10 | 223.44 | 356 | 234.32 | 467.19 | 19.23 | 1018.54 |
| Dog No. | VIT Allergen Source | Premedication with Cetirizine | Side Effects VIT | Re-Stings | VIT Follow-Up (Days) | |||
|---|---|---|---|---|---|---|---|---|
| Induction Phase | Maintenance Phase | Re-Sting No. | Clinical Signs | VIT Duration at First Re-Sting (Days) | ||||
| 1 | Bee * | Yes | No | No | 1 | No | 360 | 620 |
| 2 | Bee | Yes | No | No | 1 | No | 269 | 614 |
| 3 | Bee | Yes | No | No | 1 | Local angioedema | 176 | 375 |
| 4 | Bee | Yes | No | No | 0 | Not stung | N/A | 312 |
| 5 | Bee | Yes | No | No | 0 | Not stung | N/A | 312 |
| 6 | Bee | Yes | No | No | 1 | No | 182 | 409 |
| 7 | Bee | Yes | No | No | 0 | Not stung | N/A | 202 |
| 8 | Bee | No | Mild pruritus | No | 1 | No | 12 | 90 |
| 9 | Wasp | No | Mild pruritus | No | 1 | No | 30 | 291 |
| 10 | Bee * and wasp | No | No | No | 1 | No | 307 | 702 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rostaher, A.; Fischer, N.M.; Vigani, A.; Steblaj, B.; Martini, F.; Brem, S.; Favrot, C.; Kosnik, M. Hymenoptera Venom Immunotherapy in Dogs: Safety and Clinical Efficacy. Animals 2023, 13, 3002. https://doi.org/10.3390/ani13193002
Rostaher A, Fischer NM, Vigani A, Steblaj B, Martini F, Brem S, Favrot C, Kosnik M. Hymenoptera Venom Immunotherapy in Dogs: Safety and Clinical Efficacy. Animals. 2023; 13(19):3002. https://doi.org/10.3390/ani13193002
Chicago/Turabian StyleRostaher, Ana, Nina Maria Fischer, Alessio Vigani, Barbara Steblaj, Franco Martini, Salina Brem, Claude Favrot, and Mitja Kosnik. 2023. "Hymenoptera Venom Immunotherapy in Dogs: Safety and Clinical Efficacy" Animals 13, no. 19: 3002. https://doi.org/10.3390/ani13193002
APA StyleRostaher, A., Fischer, N. M., Vigani, A., Steblaj, B., Martini, F., Brem, S., Favrot, C., & Kosnik, M. (2023). Hymenoptera Venom Immunotherapy in Dogs: Safety and Clinical Efficacy. Animals, 13(19), 3002. https://doi.org/10.3390/ani13193002