
Part II of Finnish Agility Dog Survey: Agility-Related Injuries and Risk Factors for Injury in Competition-Level Agility Dogs

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
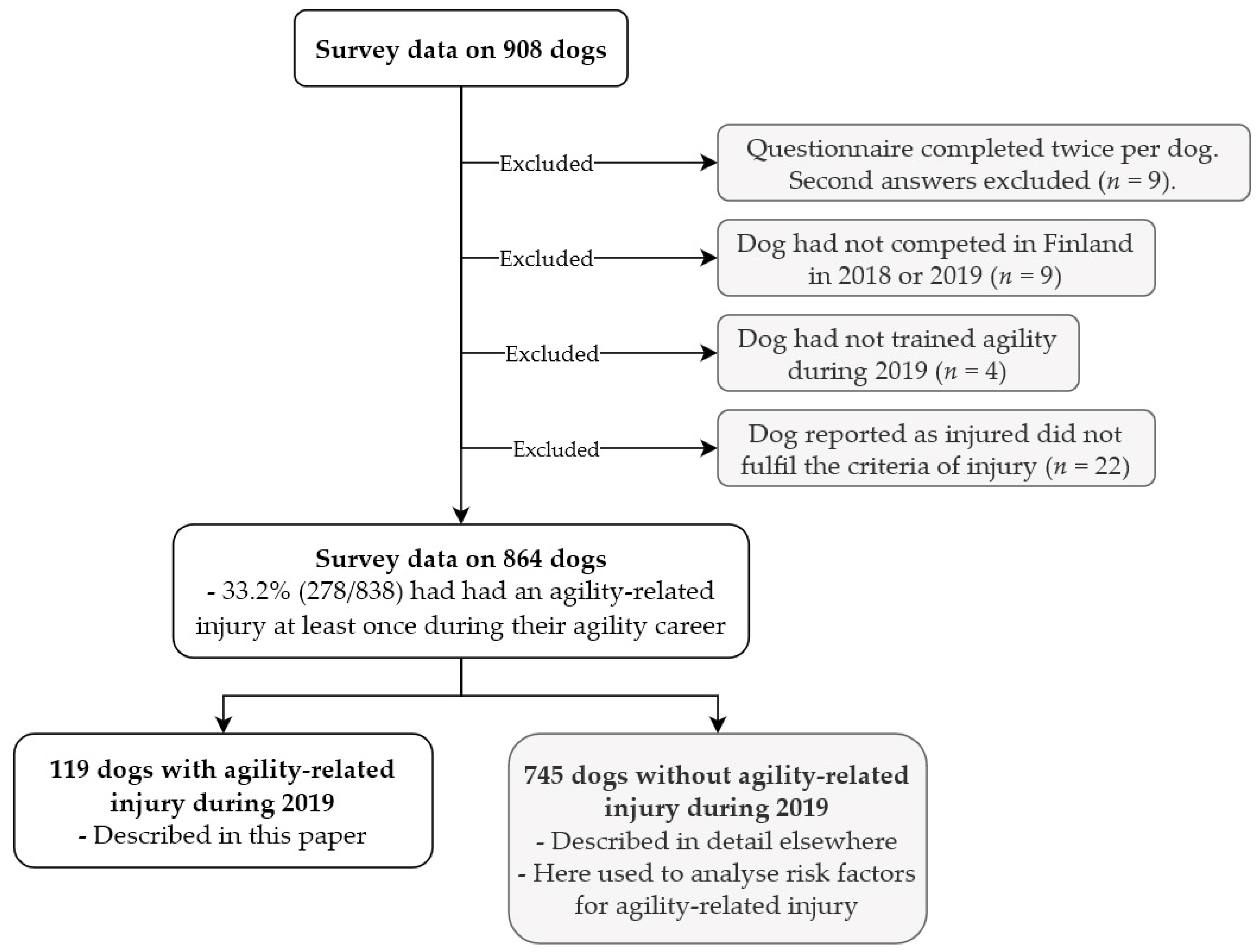
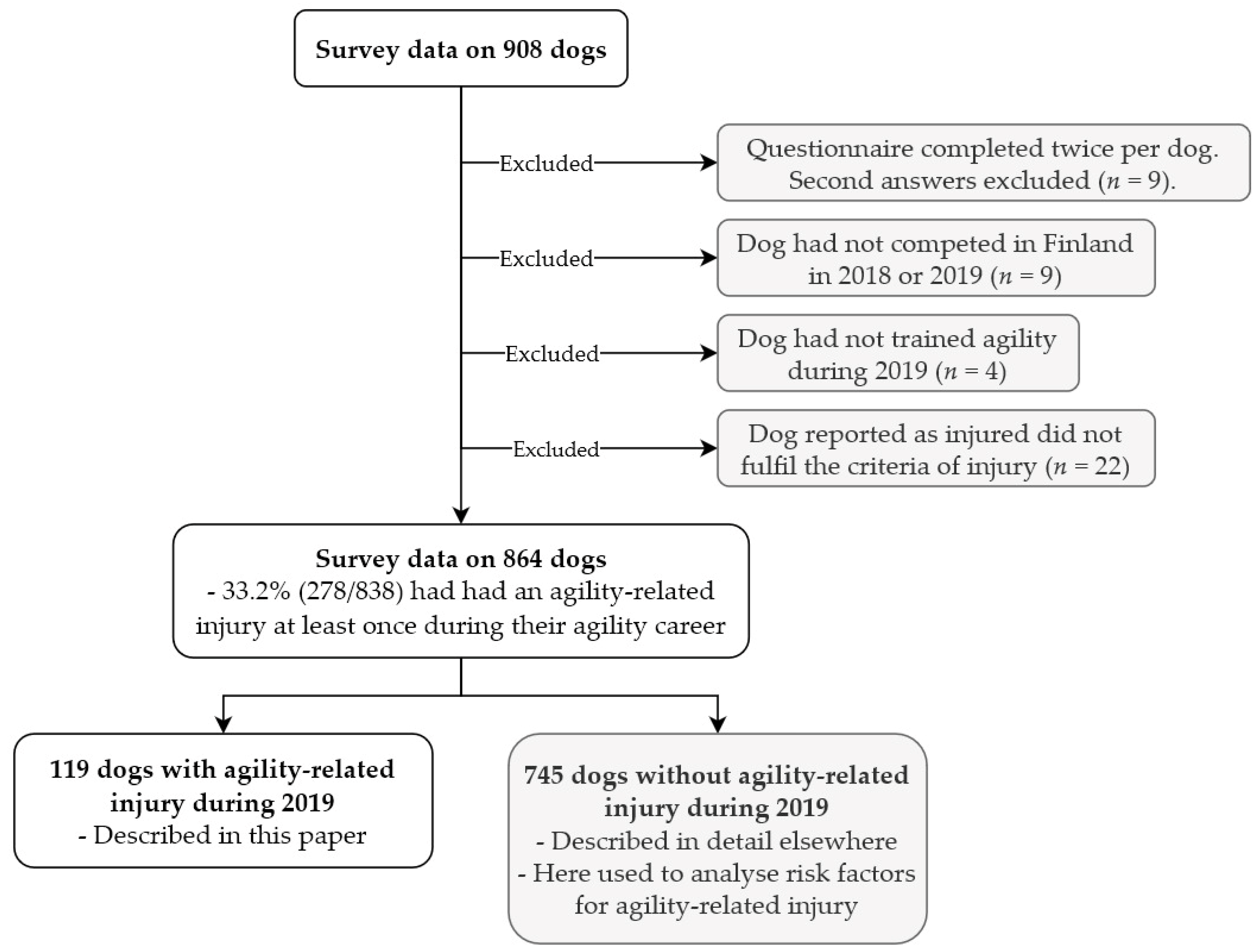
2.1. Dogs and Respondents
2.2. Questionnaire
2.3. Competition Result Database
2.4. Data Curation
2.5. Data Analysis and Statistical Methods
3. Results
3.1. Dogs and Respondents
Dog’s and Main Handler’s Experience in Agility
3.2. Context of the Injury
3.2.1. Training- and Competition-Related Injuries
3.2.2. Obstacle-Related Injuries
3.2.3. Field Surface
3.3. Description of Injury
3.3.1. Anatomical Location
3.3.2. Type of Injury
3.3.3. Clinical Signs
3.3.4. Treatment and Recovery
3.4. Training, Competition, and Management Prior to Injury
3.4.1. Agility Training
3.4.2. Competition
3.4.3. Field Surface
3.4.4. Time off from Agility
3.4.5. Warm-up and Cool-down Routines
3.4.6. Musculoskeletal Care and Conditioning
3.4.7. Daily Exercise
3.5. Health History
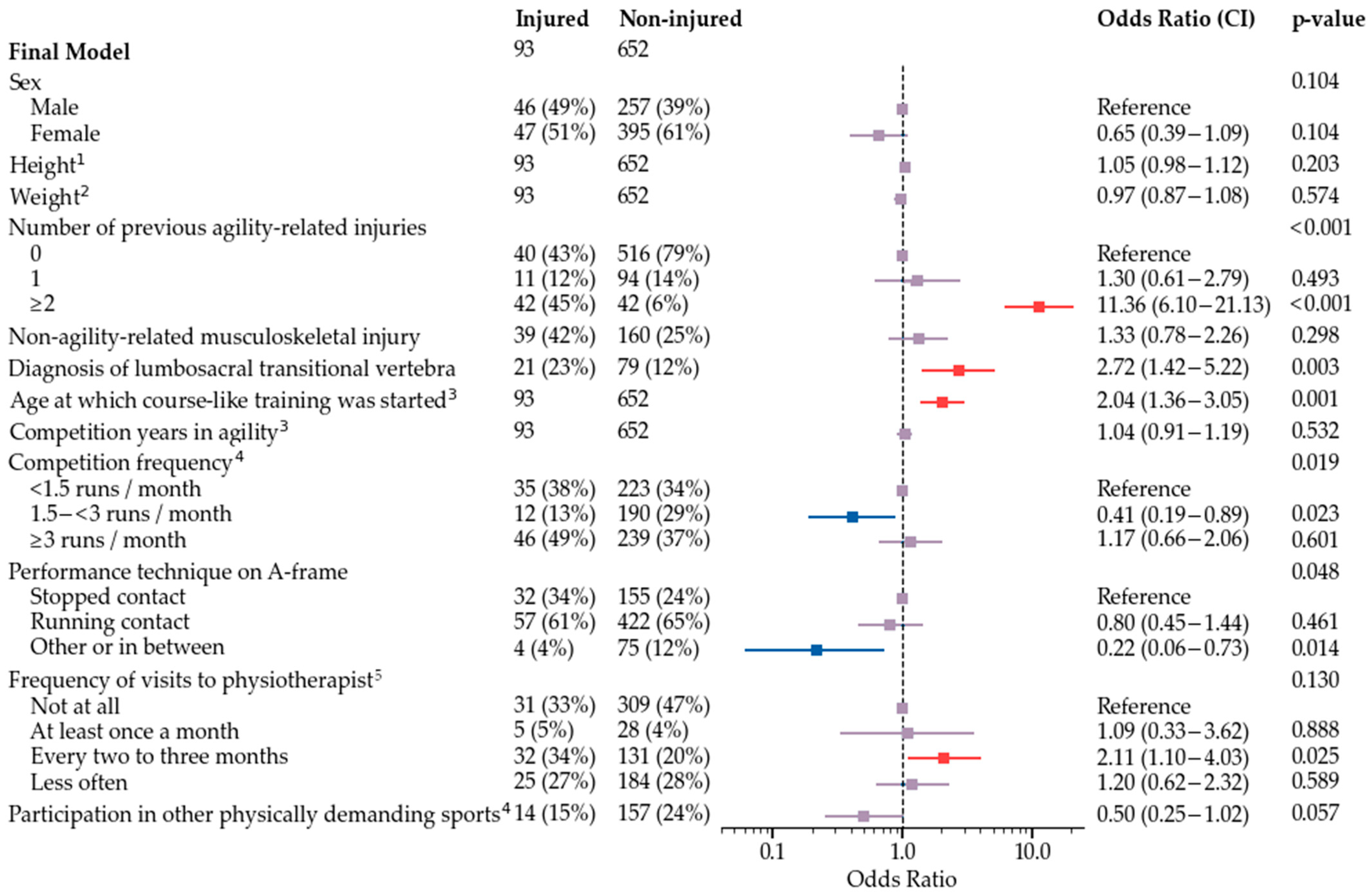
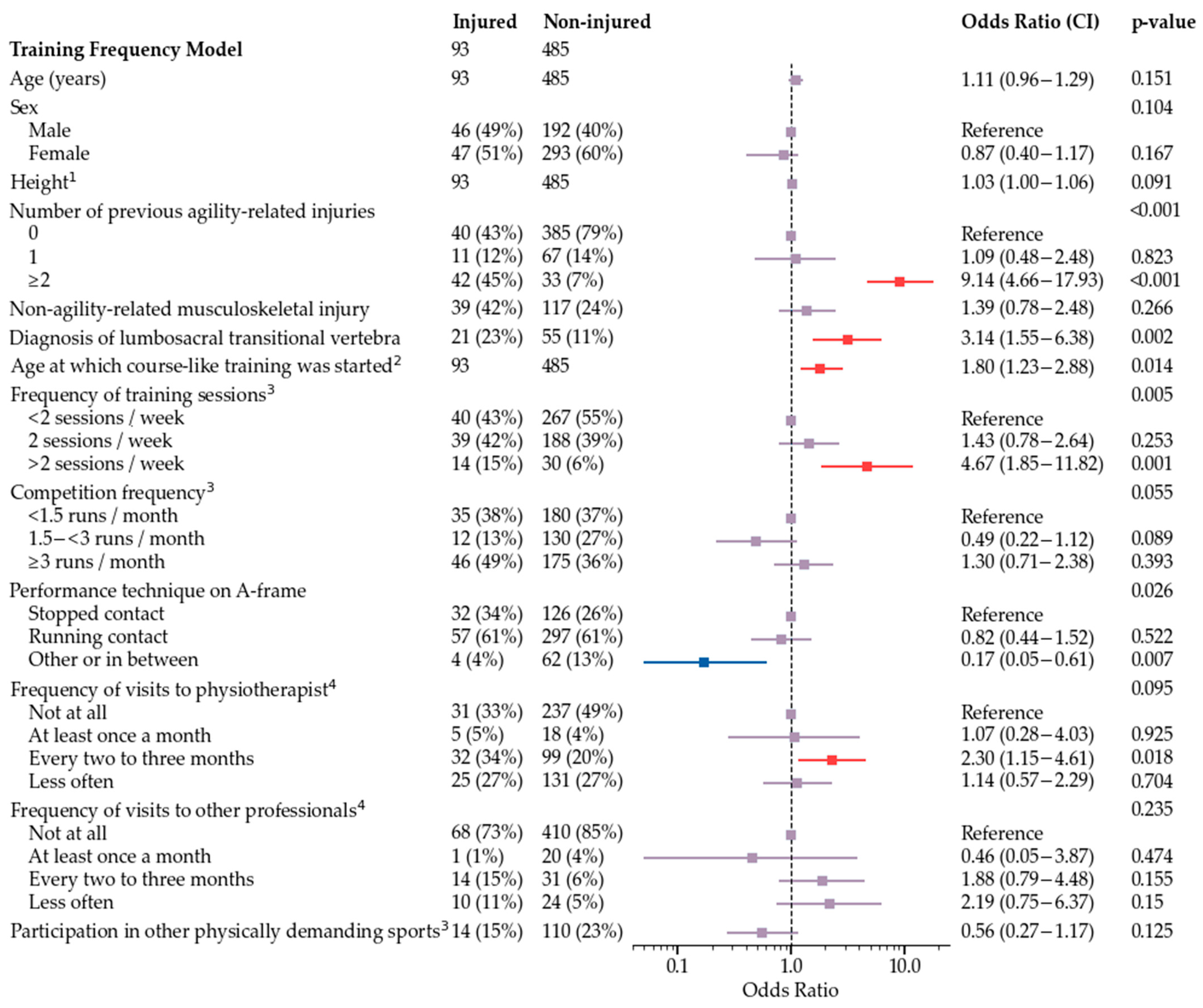
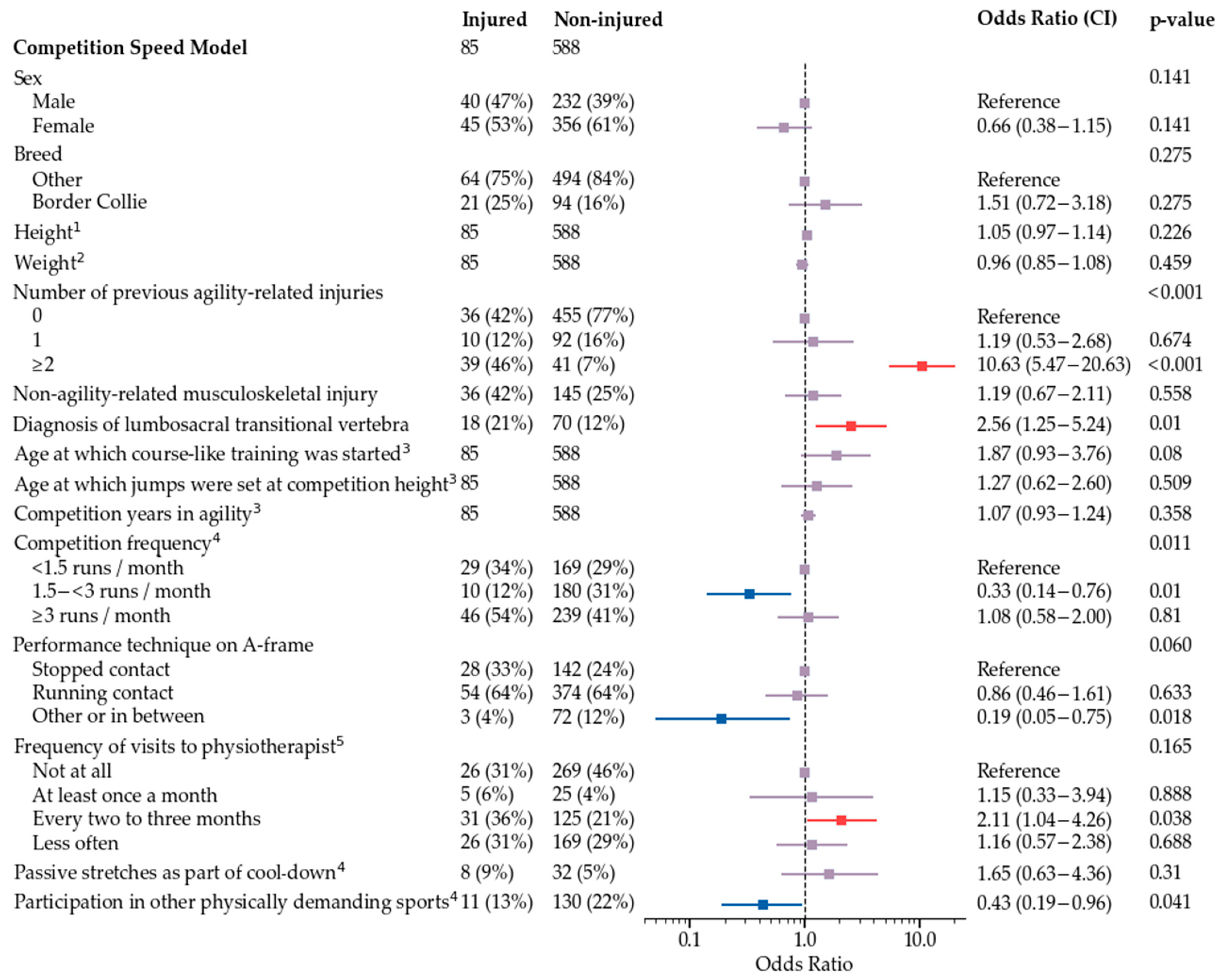
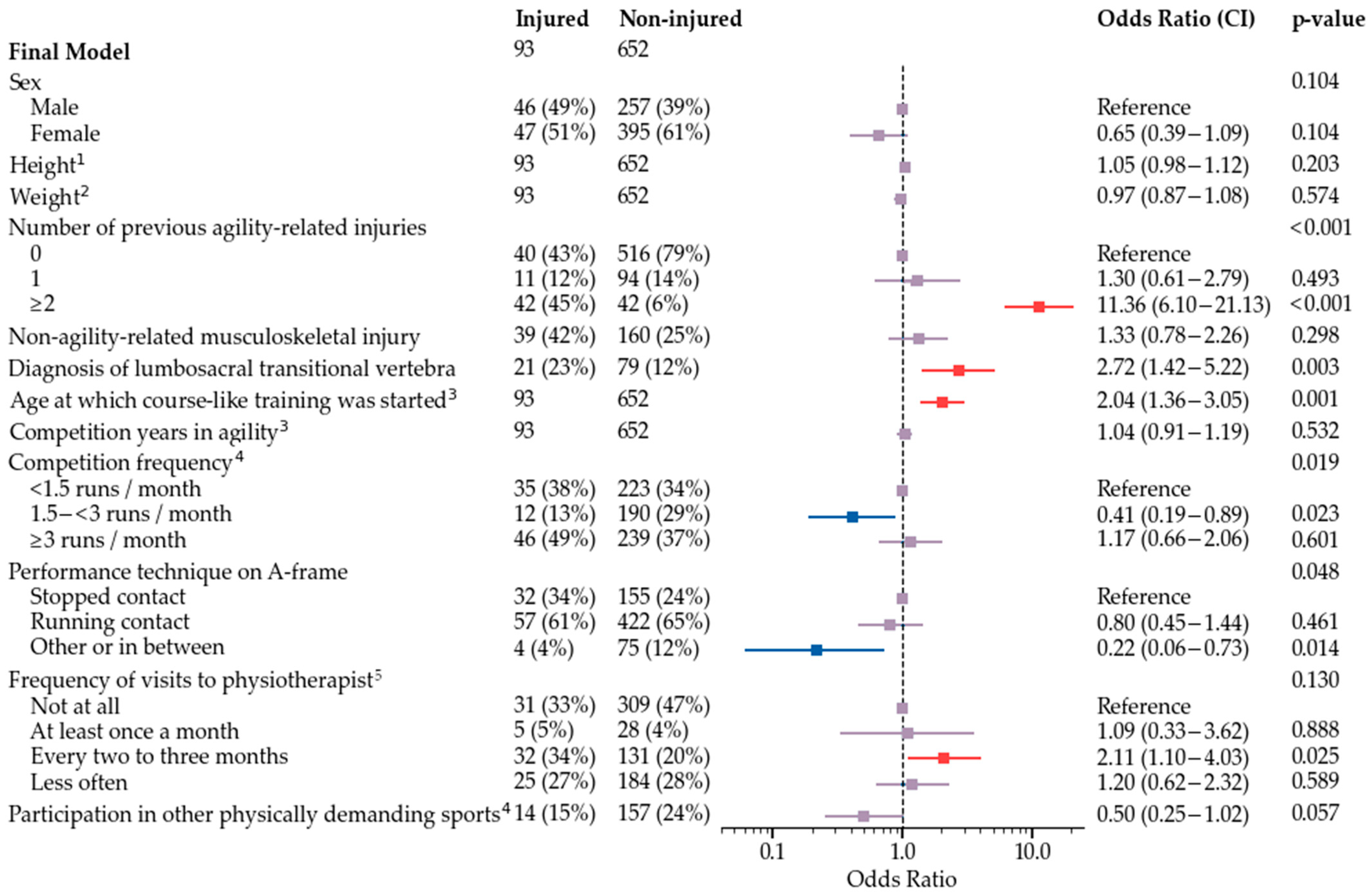
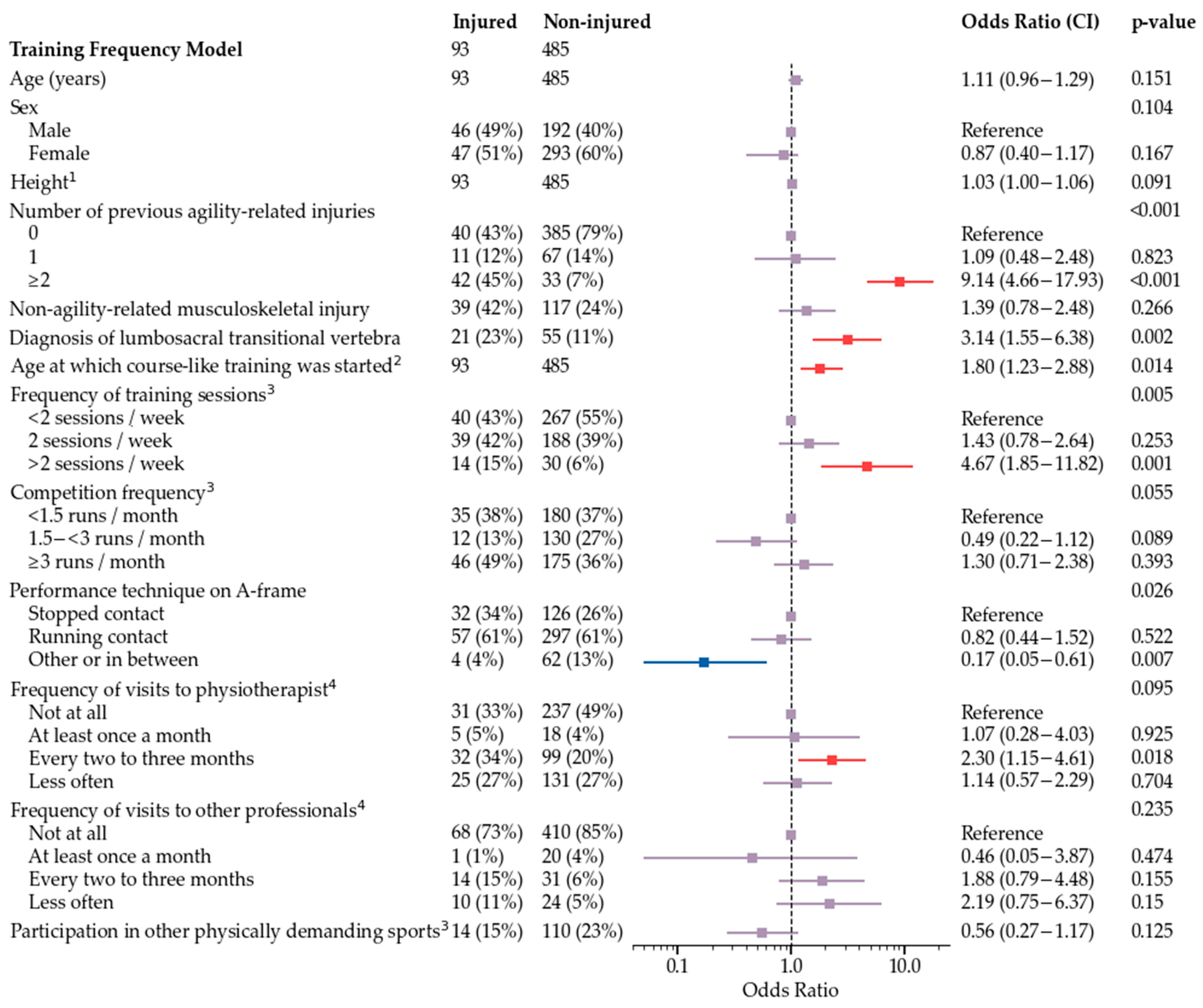
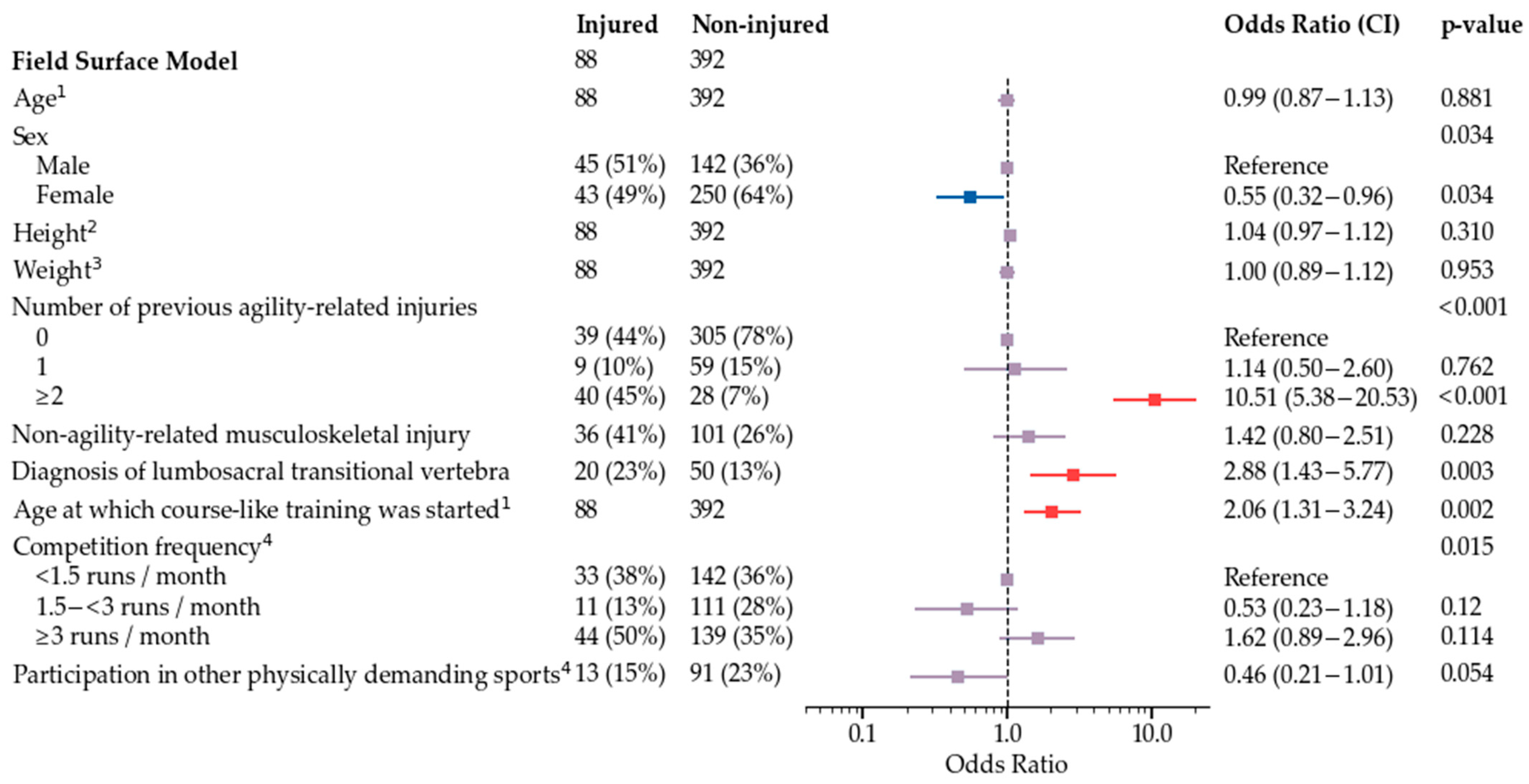
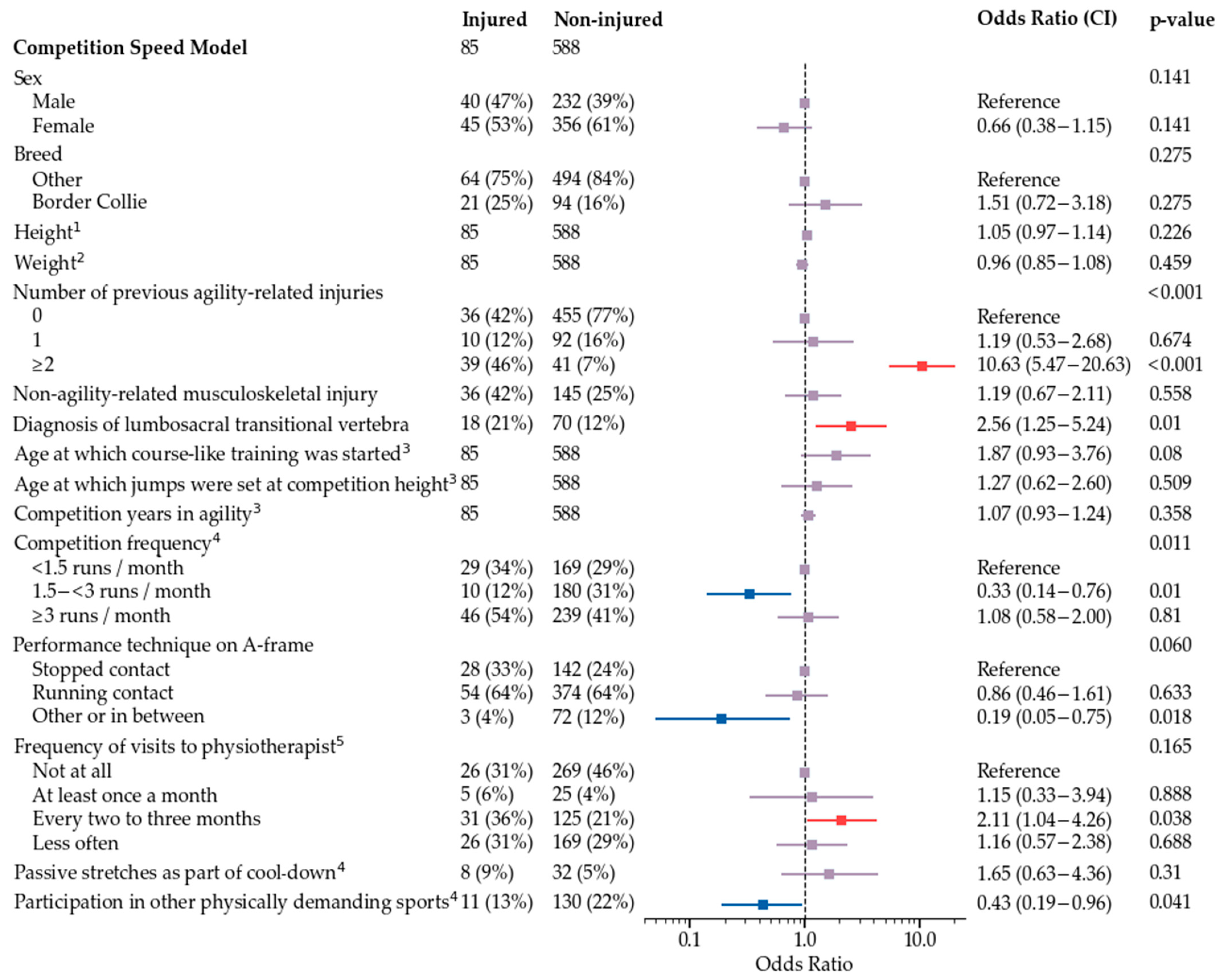
3.6. Potential Risk Factors for Agility-Related Injury during 2019
4. Discussion
4.1. Injury Rate
4.2. Obstacle-Related Injuries
4.3. Anatomical Location and Treatment
4.4. Risk Factors
4.5. Study Design and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Finnish Agility Association (Helsinki, Finland). National Competition Results from 2018 and 2019. 2020. [Google Scholar]
- Cullen, K.L.; Dickey, J.P.; Bent, L.R.; Thomason, J.J.; Moëns, N.M.M. Internet-Based Survey of the Nature and Perceived Causes of Injury to Dogs Participating in Agility Training and Competition Events. J. Am. Vet. Med. Assoc. 2013, 243, 1010–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, Z.Y.; Fields, S.; Comstock, R.D. Epidemiology of Injury among Handlers and Dogs Competing in the Sport of Agility. J. Phys. Act. Health 2014, 11, 1032–1040. [Google Scholar] [CrossRef]
- Levy, I.; Hall, C.; Trentacosta, N.; Percival, M. A Preliminary Retrospective Survey of Injuries Occurring in Dogs Participating in Canine Agility. Vet. Comp. Orthop. Traumatol. 2009, 22, 321–324. [Google Scholar]
- Evanow, J.A.; VanDeventer, G.; Dinallo, G.; Mann, S.; Frye, C.W.; Wakshlag, J.J. Internet Survey of Participant Demographics and Risk Factors for Injury in Competitive Agility Dogs. VCOT Open 2021, 4, e92–e98. [Google Scholar] [CrossRef]
- Inkilä, L.; Hyytiäinen, H.; Hielm-Björkman, A.; Junnila, J.; Bergh, A.; Boström, A. Part I of Finnish Agility Dog Survey: Training and Management of Competition-Level Agility Dogs. Animals 2021, 12, 212. [Google Scholar] [CrossRef]
- Cullen, K.L.; Dickey, J.P.; Bent, L.R.; Thomason, J.J.; Moëns, N.M.M. Survey-Based Analysis of Risk Factors for Injury among Dogs Participating in Agility Training and Competition Events. J. Am. Vet. Med. Assoc. 2013, 243, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Markley, A.P.; Shoben, A.B.; Kieves, N.R. Internet-Based Survey of the Frequency and Types of Orthopedic Conditions and Injuries Experienced by Dogs Competing in Agility. J. Am. Vet. Med. Assoc. 2021, 259, 1001–1008. [Google Scholar] [CrossRef]
- Sellon, D.C.; Martucci, K.; Wenz, J.R.; Marcellin-Little, D.J.; Powers, M.; Cullen, K.L. A Survey of Risk Factors for Digit Injuries among Dogs Training and Competing in Agility Events. J. Am. Vet. Med. Assoc. 2018, 252, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Alcock, J.; Birch, E.; Boyd, J. Effect of Jumping Style on the Performance of Large and Medium Elite Agility Dogs. Comp. Exerc. Physiol. 2015, 11, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Pinto, K.R.; Chicoine, A.L.; Romano, L.S.; Otto, S.J.G. An Internet Survey of Risk Factors for Injury in North American Dogs Competing in Flyball. Can. Vet. J. 2021, 62, 253–260. [Google Scholar]
- Kilpailusääntö (Competition Regulations of Finnish Agility Association). Available online: http://www.agilityliitto.fi/site/assets/files/7831/agilitysaannosto_-_voimassaoleva_2021.pdf (accessed on 10 October 2021).
- Isaksen, K.E.; Linney, L.; Williamson, H.; Cave, N.J.; Norman, E.J.; Cogger, N. TeamMate: A Longitudinal Study of New Zealand Working Farm Dogs. II. Occurrence of Musculoskeletal Abnormalities. Front. Vet. Sci. 2020, 7, 624. [Google Scholar] [CrossRef]
- Houlton, J.E.F. A Survey of Gundog Lameness and Injuries in Great Britain in the Shooting Seasons 2005/2006 and 2006/2007. Vet. Comp. Orthop. Traumatol. 2008, 21, 231–237. [Google Scholar] [CrossRef]
- Palmer, A.L.; Rogers, C.W.; Stafford, K.J.; Gal, A.; Bolwell, C.F. A Retrospective Descriptive Analysis of Race-Day Injuries of Greyhounds in New Zealand. Aust. Vet. J. 2021, 99, 255–262. [Google Scholar] [CrossRef]
- Montalbano, C.; Gamble, L.-J.; Walden, K.; Rouse, J.; Mann, S.; Sack, D.; Wakshlag, L.G.; Shmalberg, J.W.; Wakshlag, J.J. Internet Survey of Participant Demographics and Risk Factors for Injury in Flyball Dogs. Front. Vet. Sci. 2019, 6, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcellin-Little, D.J.; Levine, D.; Taylor, R. Rehabilitation and Conditioning of Sporting Dogs. Vet. Clin. N. Am. Small Anim. 2005, 35, 1427–1439. [Google Scholar] [CrossRef] [PubMed]
- McCauley, L.; van Dyke, J.B. Therapeutic Exercise. In Canine Sports Medicine and Rehabilitation, 2nd ed.; Zink, C., van Dyke, J.B., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2018; p. 184. [Google Scholar]
- Emery, C.A.; Pasanen, K. Current Trends in Sport Injury Prevention. Best. Pract. Res. Clin. Rheumatol. 2019, 33, 3–15. [Google Scholar] [CrossRef]
- FCI Agility Obstacle Guidelines. Available online: http://www.fci.be/medias/AGI-REG-OBS-2018-en-7609.pdf (accessed on 10 October 2021).
- Söhnel, K.; Rode, C.; de Lussanet, M.H.E.; Wagner, H.; Fischer, M.S.; Andrada, E. Limb Dynamics in Agility Jumps of Beginner and Advanced Dogs. J. Exp. Biol. 2020, 223, jeb202119. [Google Scholar] [CrossRef]
- Jaegger, G.; Marcellin-little, D.J.; Levine, D. Reliability of Goniometry in Labrador Retrievers. Am. J. Vet. Res. 2002, 63, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Appelgrein, C.; Glyde, M.R.; Hosgood, G.; Dempsey, A.R.; Wickham, S. Reduction of the A-Frame Angle of Incline Does Not Change the Maximum Carpal Joint Extension Angle in Agility Dogs Entering the A-Frame. Vet. Comp. Orthop. Traumatol. 2018, 31, 77–82. [Google Scholar]
- Castilla, A.; Knotek, B.; Vitt, M.; Gordon-Evans, W. Carpal Extension Angles in Agility Dogs Exiting the A-Frame and Hurdle Jumps. Vet. Comp. Orthop. Traumatol. 2020, 33, 142–146. [Google Scholar] [CrossRef]
- Thomas, T.M. Comparison of Measurements Obtained by Use of an Electrogoniometer and a Universal Plastic Goniometer for the Assessment of Joint Motion in Dogs Todd. Am. J. Vet. Res. 2006, 67, 1974–1979. [Google Scholar] [CrossRef]
- Birch, E.; Carter, A.; Boyd, J. An Examination of Jump Kinematics in Dogs over Increasing Hurdle Heights. Comp. Exerc. Physiol. 2016, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Cullen, K.L.; Dickey, J.P.; Brown, S.H.M.; Nykamp, S.G.; Bent, L.R.; Thomason, J.J.; Moens, N.M.M. The Magnitude of Muscular Activation of Four Canine Forelimb Muscles in Dogs Performing Two Agility-Specific Tasks. BMC Vet. Res. 2017, 13, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Zink, C.; Carr, B.J. Conditioning and Retraining the Canine Athlete. In Canine Sports Medicine and Rehabilitation, 2nd ed.; Zink, C., van Dyke, J.B., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2018; pp. 228, 259–260. [Google Scholar]
- Logan, A.A.; Nielsen, B.D. Training Young Horses: The Science behind the Benefits. Animals 2021, 11, 463. [Google Scholar] [CrossRef]
- Eckard, T.G.; Padua, D.A.; Hearn, D.W.; Pexa, B.S.; Frank, B.S. The Relationship Between Training Load and Injury in Athletes: A Systematic Review Key Points. Sports Med. 2018, 48, 1929–1961. [Google Scholar] [CrossRef]
- Griffin, A.; Kenny, I.C.; Comyns, T.M.; Lyons, M. The Association between the Acute:Chronic Workload Ratio and Injury and Its Application in Team Sports: A Systematic Review. Sports Med. 2019, 50, 561–580. [Google Scholar] [CrossRef]
- Flückiger, M.A.; Damur-Djuric, N.; Hässig, M.; Morgan, J.P.; Steffen, F. A Lumbosacral Transitional Vertebrae in the Dog Predisposes to Cauda Equina Syndrome. Vet. Radiol. Ultrasound 2006, 47, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Lappalainen, A.K.; Salomaa, R.; Junnila, J.; Snellman, M.; Laitinen-Vapaavuori, O. Alternative Classification and Screening Protocol for Transitional Lumbosacral Vertebra in German Shepherd Dogs. Acta Vet. Scand. 2012, 54, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gradner, G.; Bockstahler, B.; Peham, C.; Henninger, W.; Podbregar, I. Kinematic Study of Back Movement in Clinically Sound Malinois Dogs with Consideration of the Effect of Radiographic Changes in the Lumbosacral Junction. Vet. Surg. 2007, 36, 472–481. [Google Scholar] [CrossRef]
- Post, E.G.; Trigsted, S.M.; Riekena, J.W.; Hetzel, S.; McGuine, T.A.; Brooks, M.A.; Bell, D.R. The Association of Sport Specialization and Training Volume with Injury History in Youth Athletes. Am. J. Sports Med. 2017, 45, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.R.; Post, E.G.; Biese, K.; Bay, C.; McLeod, T.V. Sport Specialization and Risk of Overuse Injuries: A Systematic Review with Meta-Analysis. Pediatrics 2018, 142, e20180657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myer, G.D.; Jayanthi, N.; Difiori, J.P.; Faigenbaum, A.D.; Kiefer, A.W.; Logerstedt, D.; Micheli, L.J. Sport Specialization, Part I: Does Early Sports Specialization Increase Negative Outcomes and Reduce the Opportunity for Success in Young Athletes? Sports Health 2015, 7, 437–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; Mccrory, P. Consensus Statement on Injury Definitions and Data Collection Procedures in Studies of Football (Soccer) Injuries. Br. J. Sports Med. 2006, 40, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Orchard, J.W.; Ranson, C.; Olivier, B.; Dhillon, M.; Gray, J.; Langley, B.; Mansingh, A.; Moore, I.S.; Murphy, I.; Patricios, J.; et al. International Consensus Statement on Injury Surveillance in Cricket: A 2016 Update. Br. J. Sports Med. 2016, 50, 1245–1251. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Variable |
|---|---|
| Injury | Agility-related injury during 2019 (yes/no) Number of agility-related injuries during 2019 Date of the latest agility-related injury |
| Context of the injury | During competition or training If training: first or second half of the training session If competition: number of runs before the injury on that day During obstacle performance (yes/no) 1 If obstacle-associated: Which obstacle, collision (yes/no), fall (yes/no), slipping during obstacle performance (yes/no) Slipping in between obstacles (yes/no) When injury was noticed (during or after agility) Surface of the agility field |
| Description of the injury | Anatomical location 2 Type of the injury Clinical signs |
| Treatment | Veterinary care (yes/no) If veterinary care was sought: the time of diagnosis in relation to injury Treatments |
| Recovery | Recovery time to normal exercise Recovery time to performance level prior to injury |
| Number of Runs | Number of Dogs | Proportion of Dogs with Competition-Related Injury |
|---|---|---|
| 0 | 8/34 | 23.5% |
| 1 | 16/34 | 47.1% |
| 2 | 5/34 | 14.7% |
| 3 | 5/34 | 14.7% |
| Obstacle | Number of Dogs | Proportion of Dogs with Obstacle-Related Injury |
|---|---|---|
| Bar jump | 23/63 | 36.5% |
| Dogwalk | 11/63 | 17.5% |
| A-frame | 10/63 | 15.9% |
| Open tunnel | 10/63 | 15.9% |
| Weave poles | 4/63 | 6.3% |
| Seesaw | 2/63 | 3.2% |
| Spread jump | 1/63 | 1.6% |
| Tire | 1/63 | 1.6% |
| Long jump | 1/63 | 1.6% |
| Field Surface | Number of Dogs | Proportion of Dogs |
|---|---|---|
| Artificial turf with rubber filling | 39/111 | 35.1% |
| Dirt or sand | 25/111 | 22.5% |
| Artificial turf without filling | 21/111 | 18.9% |
| Artificial turf with cork filling | 14/111 | 12.6% |
| Artificial turf with sand filling | 6/111 | 5.4% |
| Natural grass | 5/111 | 4.5% |
| Rubber mat | 1/111 | 0.9% |
| Anatomical Location | Number of Dogs | Proportion of Dogs |
|---|---|---|
| Back | 23/119 | 19.3% |
| Brachium | 19/119 | 16.0% |
| Scapular region | 16/119 | 13.4% |
| Shoulder | 15/119 | 12.6% |
| Pelvis | 14/119 | 11.8% |
| Thigh | 13/119 | 10.9% |
| Ribcage | 12/119 | 10.1% |
| Digit (front limb) | 12/119 | 10.1% |
| Carpus | 11/119 | 9.2% |
| Nail of a front limb | 11/119 | 9.2% |
| Neck | 10/119 | 8.4% |
| Treatment | Number of Dogs | Proportion of Dogs |
|---|---|---|
| Exercise restriction | 91/118 | 77.1% |
| Medical treatment | 55/118 | 46.6% |
| Physiotherapy | 50/118 | 42.4% |
| Rehabilitation/conditioning as part of physiotherapy | 25/118 | 21.2% |
| Osteopathy | 15/118 | 12.7% |
| Massage | 14/118 | 11.9% |
| Laser therapy | 13/118 | 11.0% |
| Wound care | 11/118 | 9.3% |
| Other therapies 1 | 9/118 | 7.6% |
| Taping | 8/118 | 6.8% |
| Acupuncture | 8/118 | 6.8% |
| Surgery | 6/118 | 5.1% |
| Craniosacral therapy | 5/118 | 4.2% |
| Splint or cast | 4/118 | 3.4% |
| Cryotherapy | 4/118 | 3.4% |
| Severity | Number of Dogs | Proportion of Dogs |
|---|---|---|
| Minor (<3 weeks) | 26/99 | 26.3% |
| Moderate (3 to <8 weeks) | 29/99 | 29.3% |
| Severe (≥8 weeks, with return to agility) | 33/99 | 33.3% |
| Career ending | 11/99 | 11.1% |
| Item | Warm-Up (n = 118) | Cool-Down (n = 118) |
|---|---|---|
| Exercising on leash | 93.2% (n = 110/118) | 92.4% (109/118) |
| Exercising off leash | 61.0% (n = 72/118) | 55.9% (66/118) |
| Walking | 61.9% (n = 73/118) | 70.3% (83/118) |
| Running | 72.9% (n = 86/118) | 50.8% (60/118) |
| Sprinting | 35.6% (n = 42/118) | 1.7% (2/118) |
| Tricks | 69.5% (n = 82/118) | 4.2% (5/118) |
| Tug play | 31.4% (n = 37/118) | 2.5% (3/118) |
| Active stretches | 31.4% (n = 37/118) | 4.2% (5/118) |
| Passive stretches | 13.6% (n = 16/118) | 10.2% (12/118) |
| Habituation to the field surface | 32.2% (n = 38/118) | Not applicable |
| Obstacle performances as part of warm-up | 20.3% (n = 24/118) | Not applicable |
| Other 1 | 1.7% (n = 2/118) | 3.4% (4/118) |
| Professional | At Least Once a Month | Every Two to Three Months | Less Often | Not at All |
|---|---|---|---|---|
| Massage therapist | 16.1% (n = 19/118) | 30.5% (n = 36/118) | 19.5% (n = 23/118) | 33.9% (n = 40/118) |
| Physiotherapist | 6.8% (n = 8/118) | 31.4% (n = 37/118) | 27.1% (n = 32/118) | 34.7% (n = 41/118) |
| Osteopath | 1.7% (n = 2/118) | 14.4% (n = 17/118) | 20.3% (n = 24/118) | 63.6% (n = 75/118) |
| Other | 1.7% (n = 2/118) | 16.1% (n = 19/118) | 9.3% (n = 11/118) | 72.9% (n = 86/118) |
| Diagnosis | Number of Dogs | Proportion of Dogs |
|---|---|---|
| Lumbosacral transitional vertebra | 26/119 | 21.8% |
| Hip dysplasia | 16/119 | 13.4% |
| Other muscle injury | 5/116 | 4.3% |
| Fracture | 5/119 | 4.2% |
| Patellar luxation | 4/119 | 3.4% |
| Disease of the elbow | 3/119 | 2.5% |
| Carpal sprain | 2/118 | 1.7% |
| Sprain of toe | 2/118 | 1.7% |
| Injury of biceps tendon or muscle | 2/118 | 1.7% |
| Other tendon injury | 2/118 | 1.7% |
| Osteochondrosis/osteochondritis dissecans | 2/119 | 1.7% |
| Injury of supraspinatus muscle or tendon | 1/118 | 0.8% |
| Shoulder instability/medial shoulder syndrome | 1/119 | 0.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inkilä, L.; Hyytiäinen, H.K.; Hielm-Björkman, A.; Junnila, J.; Bergh, A.; Boström, A. Part II of Finnish Agility Dog Survey: Agility-Related Injuries and Risk Factors for Injury in Competition-Level Agility Dogs. Animals 2022, 12, 227. https://doi.org/10.3390/ani12030227
Inkilä L, Hyytiäinen HK, Hielm-Björkman A, Junnila J, Bergh A, Boström A. Part II of Finnish Agility Dog Survey: Agility-Related Injuries and Risk Factors for Injury in Competition-Level Agility Dogs. Animals. 2022; 12(3):227. https://doi.org/10.3390/ani12030227
Chicago/Turabian StyleInkilä, Leena, Heli K. Hyytiäinen, Anna Hielm-Björkman, Jouni Junnila, Anna Bergh, and Anna Boström. 2022. "Part II of Finnish Agility Dog Survey: Agility-Related Injuries and Risk Factors for Injury in Competition-Level Agility Dogs" Animals 12, no. 3: 227. https://doi.org/10.3390/ani12030227
APA StyleInkilä, L., Hyytiäinen, H. K., Hielm-Björkman, A., Junnila, J., Bergh, A., & Boström, A. (2022). Part II of Finnish Agility Dog Survey: Agility-Related Injuries and Risk Factors for Injury in Competition-Level Agility Dogs. Animals, 12(3), 227. https://doi.org/10.3390/ani12030227