
Outcome of Acquired Fanconi Syndrome Associated with Ingestion of Jerky Treats in 30 Dogs
 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
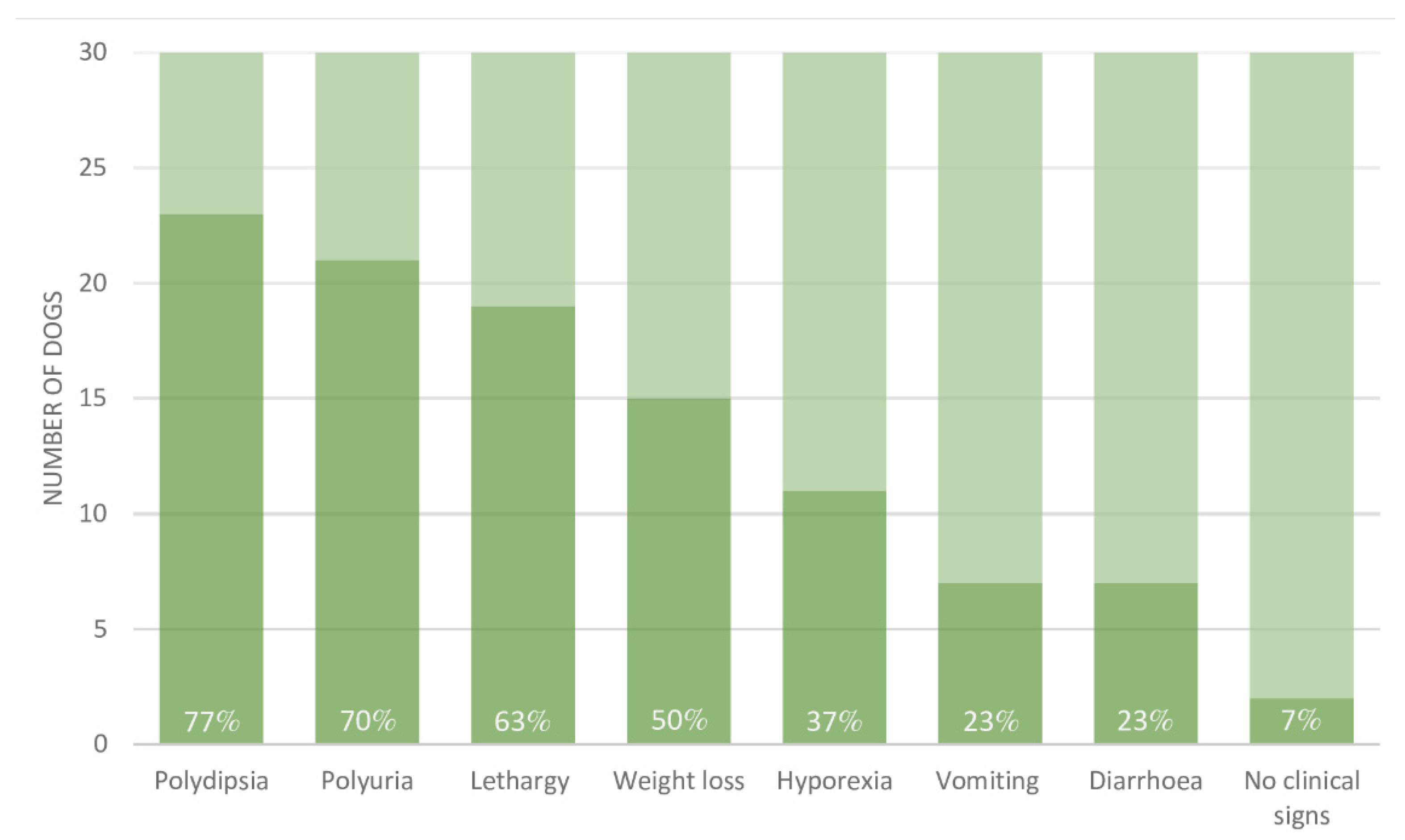
3.2. Clinical Signs
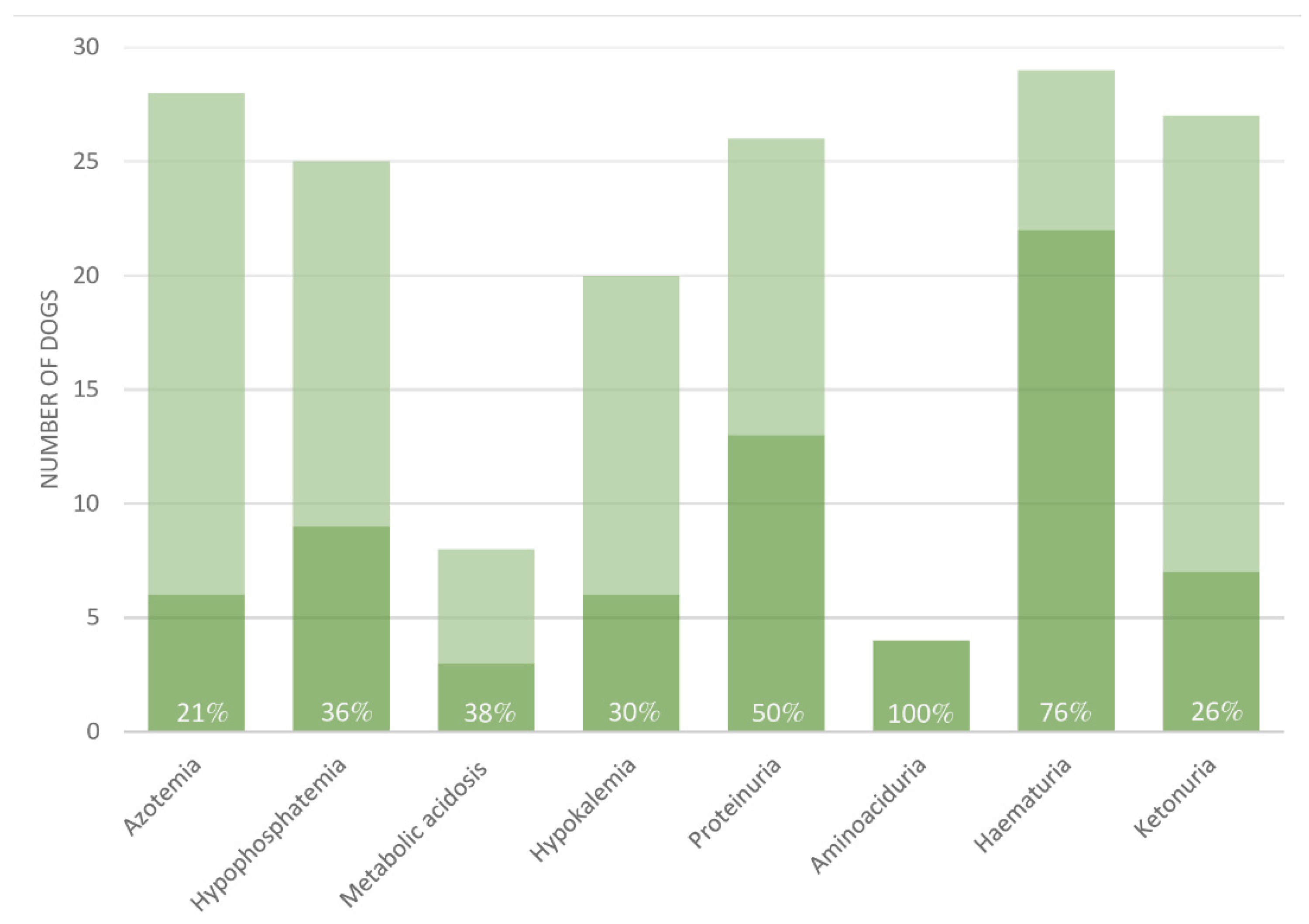
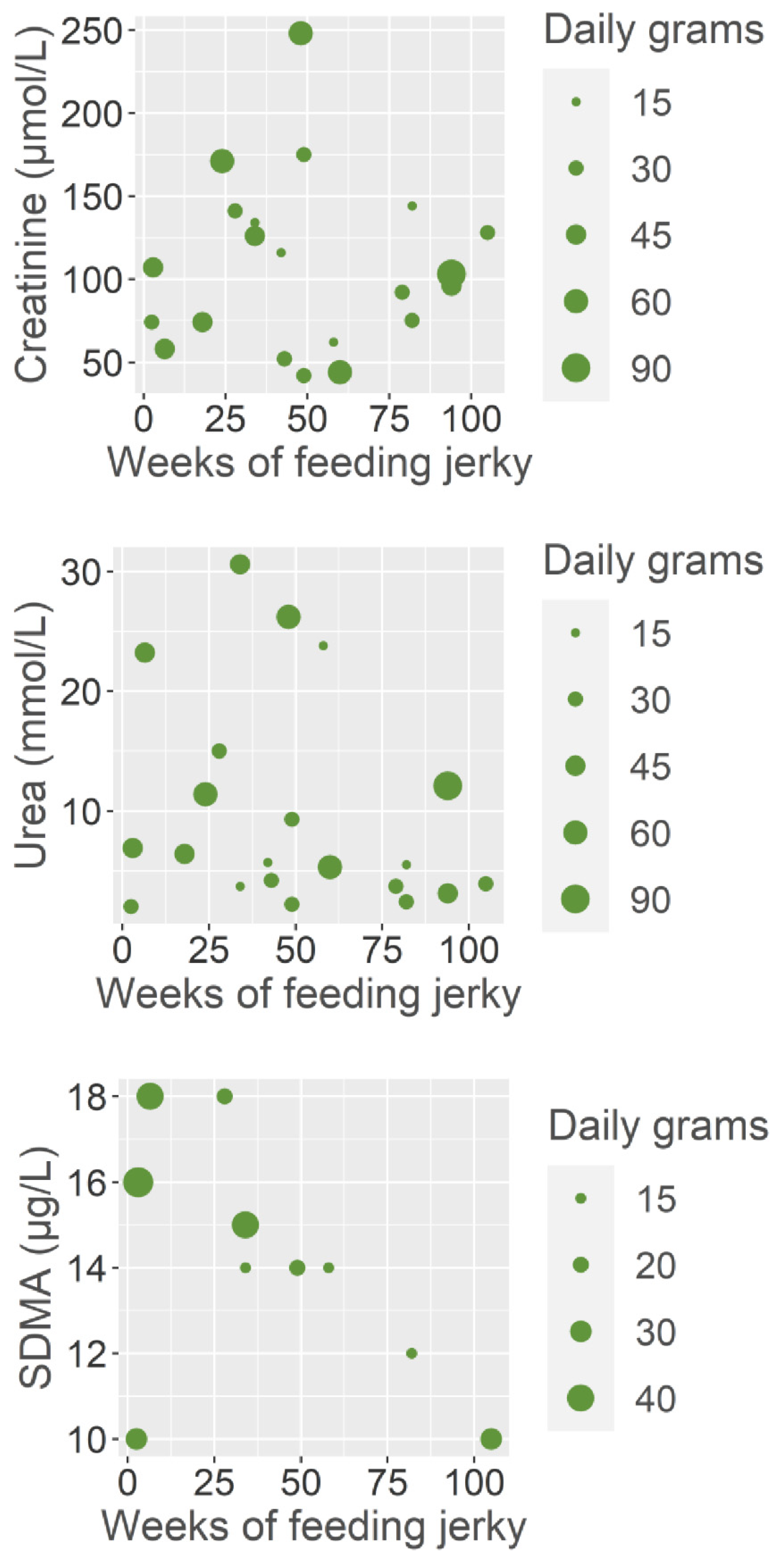
3.3. Para-Clinical Signs
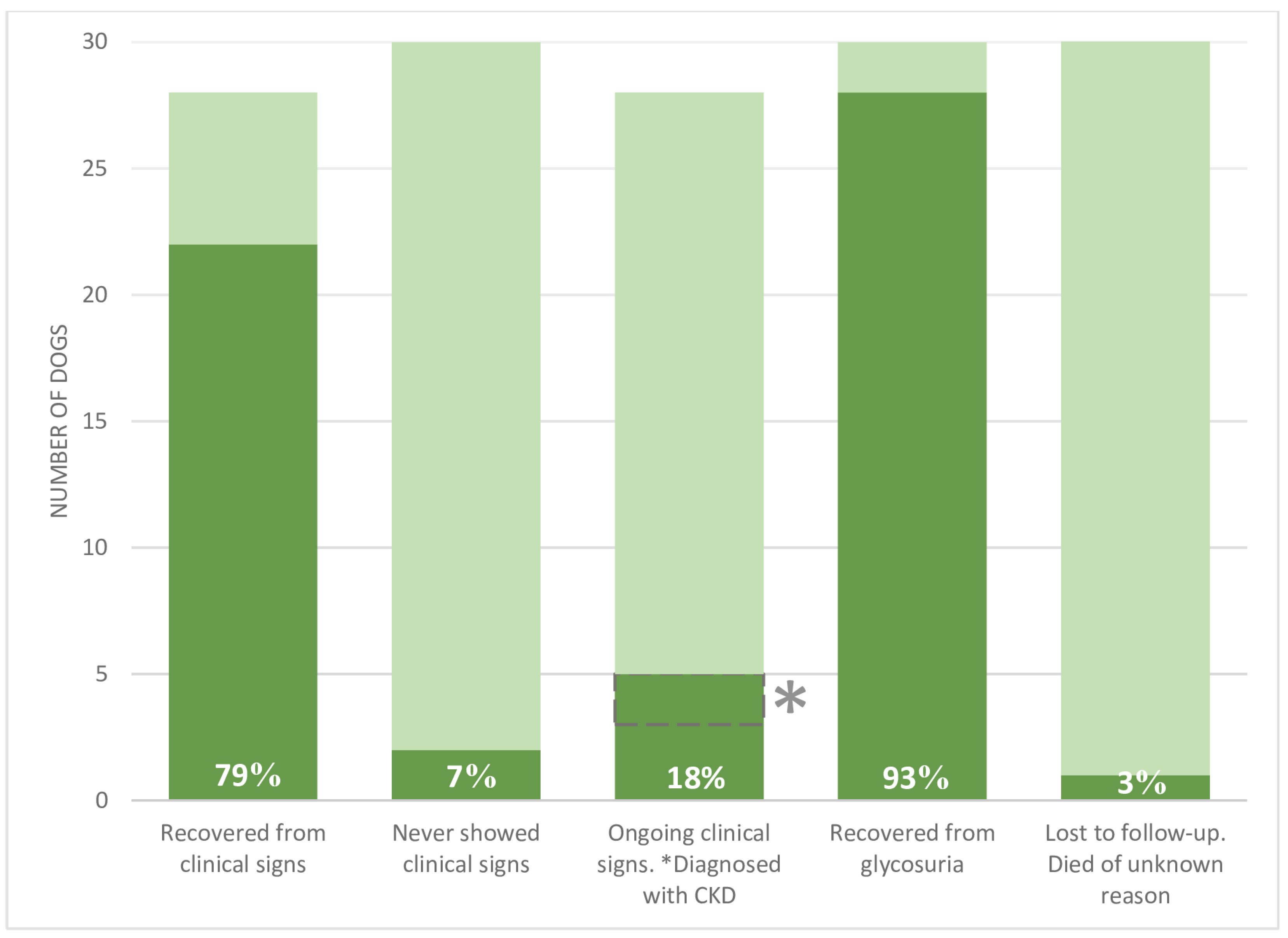
3.4. Treatment and Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Foreman, J.W. Fanconi Syndrome. Pediatric Clin. N. Am. 2019, 66, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.E. Renal Tubular Reabsorption and Secretion. In Guyton and Hall Textbook of Medical Physiology, 13th ed.; Elsevier: Philadelphia, PA, USA, 2016; pp. 347–369, Chapter 28. [Google Scholar]
- Bovée, K.C.; Joyce, T.; Blazer-Yost, B.; Goldschmidt, M.S.; Segal, S. Characterization of Renal Defects in Dogs with a Syndrome Similar to the Fanconi Syndrome in Man. J. Am. Vet. Med. Assoc. 1979, 174, 1094–1099. [Google Scholar] [PubMed]
- Easley, J.R.; Breitschwerdt, E.B. Glucosuria Associated with Renal Tubular Dysfunction in Three Basenji Dogs. J. Am. Vet. Med. Assoc. 1976, 168, 938–943. [Google Scholar] [PubMed]
- Yearley, J.H.; Hancock, D.D.; Mealey, K.L. Survival Time, Lifespan, and Quality of Life in Dogs with Idiopathic Fanconi Syndrome. J. Am. Vet. Med. Assoc. 2004, 225, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Finco, D.R. Familial Renal Disease in Norwegian Elkhound Dogs: Physiologic and Biochemical Examinations. Am. J. Vet. Res. 1976, 37, 87–91. [Google Scholar] [PubMed]
- Bommer, N.X.; Brownlie, S.E.; Morrison, L.R.; Chandler, M.L.; Simpson, J.W. Fanconi Syndrome in Irish Wolfhound Siblings. J. Am. Anim. Hosp. Assoc. 2018, 54, 173–178. [Google Scholar] [CrossRef]
- Mackenzie, C.P.; Van Den Broek, A. The Fanconi Syndrome in a Whippet. J. Small Anim. Pract. 1982, 23, 469–474. [Google Scholar] [CrossRef]
- McEwan, N.A.; Macartney, L. Fanconi’s Syndrome in a Yorkshire Terrier. J. Small Anim. Pract. 1987, 28, 737–742. [Google Scholar] [CrossRef]
- Langlois, D.K.; Smedley, R.C.; Schall, W.D.; Kruger, J.M. Acquired Proximal Renal Tubular Dysfunction in 9 Labrador Retrievers with Copper-Associated Hepatitis (2006–2012). J. Vet. Intern. Med. 2013, 27, 491–499. [Google Scholar] [CrossRef]
- King, J. Proximal Tubular Nephropathy in Two Dogs Diagnosed with Lead Toxicity. Aust. Vet. J. 2016, 94, 280–284. [Google Scholar] [CrossRef]
- Settles, E.L.; Schmidt, D. Fanconi Syndrome in a Labrador Retriever. J. Vet. Intern. Med. 1994, 8, 390–393. [Google Scholar] [CrossRef]
- Freeman, L.M.; Breitschwerdt, E.B.; Keene, B.W.; Hansen, B. Fanconi’s Syndrome in a Dog with Primary Hypoparathyroidism. J. Vet. Intern. Med. 1994, 8, 349–354. [Google Scholar] [CrossRef]
- Brown, S.A.; Rakich, P.M.; Barsanti, J.A.; Finco, D.R.; Kickbush, C. Fanconi Syndrome and Acute Renal Failure Associated with Gentamicin Therapy in a Dog. J. Am. Anim. Hosp. Assoc. 1986, 22, 635–640. [Google Scholar]
- Bark, H.; Park, R. Fanconi Syndrome Associated with Amoxicillin Therapy in the Dog. Canine Pract. (Santa Barbara Calif. 1990) (USA) 1995, 20, 19–22. [Google Scholar]
- Schuller, S.; Francey, T.; Hartmann, K.; Hugonnard, M.; Kohn, B.; Nally, J.E.; Sykes, J. European Consensus Statement on Leptospirosis in Dogs and Cats. J. Small Anim. Pract. 2015, 56, 159–179. [Google Scholar] [CrossRef]
- Sykes, J.E.; Hartmann, K.; Lunn, K.F.; Moore, G.E.; Stoddard, R.A.; Goldstein, R.E. 2010 ACVIM Small Animal Consensus Statement on Leptospirosis: Diagnosis, Epidemiology, Treatment, and Prevention. J. Vet. Intern. Med. 2011, 25, 1–13. [Google Scholar] [CrossRef]
- Barton, J.C.; Mäntylä Noble, P.-J.; O’Connell, E.M. Acute Kidney Injury Manifesting as Renal Tubular Acidosis with Proximal and Distal Renal Tubular Dysfunction in a Dog with Acute Pancreatitis. J. Vet. Emerg. Crit. Care (San Antonio) 2022, 32, 524–531. [Google Scholar] [CrossRef]
- Center for Veterinary Medicine FDA Investigates Animal Illnesses Linked to Jerky Pet Treats. Available online: https://www.fda.gov/animal-veterinary/outbreaks-and-advisories/fda-investigates-animal-illnesses-linked-jerky-pet-treats (accessed on 26 August 2022).
- Center for Veterinary Medicine CVM Updates—FDA Provides Update on Jerky Pet Treat Investigation. Available online: https://www.nasc.cc/news/fda-provides-update-jerky-pet-treat-investigation/ (accessed on 17 November 2022).
- Sheridan, R.; Mirabile, J.; Hafler, K. Determination of Six Illegal Antibiotics in Chicken Jerky Dog Treats. J. Agric. Food Chem. 2014, 62, 3690–3696. Available online: https://pubs.acs.org/doi/full/10.1021/jf405458m (accessed on 27 August 2022). [CrossRef]
- Thompson, M.; Fleeman, L.; Kessell, A.; Steenhard, L.; Foster, S. Acquired Proximal Renal Tubulopathy in Dogs Exposed to a Common Dried Chicken Treat: Retrospective Study of 108 Cases (2007–2009). Aust. Vet. J. 2013, 91, 368–373. [Google Scholar] [CrossRef]
- Hooper, A.N.; Roberts, B.K. Fanconi Syndrome in Four Non–Basenji Dogs Exposed to Chicken Jerky Treats. J. Am. Anim. Hosp. Assoc. 2011, 47, e178–e187. [Google Scholar] [CrossRef]
- Major, A.; Schweighauser, A.; Hinden, S.E.; Francey, T. Transient Fanconi Syndrome with Severe Polyuria and Polydipsia in a 4-Year Old Shih Tzu Fed Chicken Jerky Treats. Schweiz. Arch. Tierheilkd 2014, 156, 593–598. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Igase, M.; Baba, K.; Shimokawa Miyama, T.; Noguchi, S.; Mizuno, T.; Okuda, M. Acquired Fanconi Syndrome in a Dog Exposed to Jerky Treats in Japan. J. Vet. Med. Sci. 2015, 77, 1507–1510. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yabuki, A.; Iwanaga, T.; Giger, U.; Sawa, M.; Kohyama, M.; Yamatoy, O. Acquired Fanconi Syndrome in Two Dogs Following Long-Term Consumption of Pet Jerky Treats in Japan: Case Report. J. Vet. Med. Sci. 2017, 79, 818–821. [Google Scholar] [CrossRef]
- Bates, N.; Sharman, M.; Lam, A.; Kent, A.; Walker, D.; Smith, V.; Carmichael, N. Reporting Cases of Fanconi Syndrome in Dogs in the UK. Vet. Rec. 2016, 178, 510. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, N.; Lee, J.; Giger, U. Fanconi Syndrome in Dog in the UK. Vet. Rec. 2014, 174, 357. [Google Scholar] [CrossRef]
- Hooijberg, E.H.; Furman, E.; Leidinger, J.; Brandstetter, D.; Hochleitner, C.; Sewell, A.C.; Leidinger, E.; Giger, U. Transient Renal Fanconi Syndrome in a Chihuahua Exposed to Chinese Chicken Jerky Treats. Tierarztl. Prax Ausg K Kleintiere Heimtiere 2015, 43, 188–192. [Google Scholar] [CrossRef]
- Schaalo, S.; Miklis, A.; Schlüter, C.; Neiger, R. Acquired transient Fanconi syndrome after feeding jerky treats in dogs—A case series. Tierarztl. Prax Ausg K Kleintiere Heimtiere 2021, 49, 300–308. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: https://www.r-project.org/ (accessed on 19 October 2022).
- Hall, J.A.; Yerramilli, M.; Obare, E.; Yerramilli, M.; Almes, K.; Jewell, D.E. Serum Concentrations of Symmetric Dimethylarginine and Creatinine in Dogs with Naturally Occurring Chronic Kidney Disease. J. Vet. Intern. Med. 2016, 30, 794–802. [Google Scholar] [CrossRef]
- Nabity, M.B.; Lees, G.E.; Boggess, M.M.; Yerramilli, M.; Obare, E.; Yerramilli, M.; Rakitin, A.; Aguiar, J.; Relford, R. Symmetric Dimethylarginine Assay Validation, Stability, and Evaluation as a Marker for the Early Detection of Chronic Kidney Disease in Dogs. J. Vet. Intern. Med. 2015, 29, 1036–1044. [Google Scholar] [CrossRef]
- Le Sueur, A.N.V.; Geraldes, S.S.; Melchert, A.; Takahira, R.K.; Coyne, M.; Murphy, R.; Szlosek, D.; Guimarães-Okamoto, P.T.C. Symmetric Dimethylarginine Concentrations in Dogs with International Renal Interest Society Stage 4 Chronic Kidney Disease Undergoing Intermittent Hemodialysis. J. Vet. Intern. Med. 2019, 33, 2635–2643. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Origin | Number of Dogs | Azotaemia | Metabolic Acidosis | Hypokalaemia | Hypo-Phosphatemia | Glycosuria | Aminoaciduria | Proteinuria | Ketonuria | Haematuria |
|---|---|---|---|---|---|---|---|---|---|---|
| USA, 2011 [23] | 4 | 25% | 100% | 100% | 25% | 100% | 100% | 100% | 50% | 75% |
| Australia, 2013 [22] | 108 | 27% | 77% | 45% | 37% | 100% | 100% | 87% | 25% | 77% |
| Switzerland, 2014 [24] | 1 | + | + | + | + | NA | + | + | - | |
| UK, 2016 [27] | 11 | - | NA | NA | NA | + | + | - | NA | NA |
| UK, 2014 [28] | 1 | - | - | - | - | + | + | - | - | - |
| Austria, 2015 [29] | 1 | - | NA | NA | + | + | + | + | - | + |
| Japan, 2015 [25] | 1 | + | + | + | NA | + | + | + | NA | - |
| Japan, 2017 [26] | 2 | - | 50% | 50% | 50% | 100% | 100% | 50% | 50% | - |
| Germany, 2021 [30] | 6 | 83% | NA | 33% | 0% | 100% | 100% | 67% | NA | 50% |
| Dog ID | Clinical Signs | Glycosuria | Subsequent CKD * (+/−) | Last Follow-Up |
|---|---|---|---|---|
| 1 | Ongoing 68 wks | Resolved 9 wks | + | 68 wks |
| 4 | Ongoing 35 wks | Resolved 22 wks | + | 35 wks |
| 18 | Ongoing 8 wks | Unknown | − | 8 wks |
| 23 | Ongoing 72 wks | Resolved (unknown time) | − | 72 wks |
| 32 | Ongoing 9 wks | Resolved 4 wks | − | 9 wks |
| 2 | Recovered 20 wks | Ongoing 20 wks | − | 20 wks |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nybroe, S.; Bjørnvad, C.R.; Hansen, C.F.H.; Andersen, T.S.L.; Kieler, I.N. Outcome of Acquired Fanconi Syndrome Associated with Ingestion of Jerky Treats in 30 Dogs. Animals 2022, 12, 3192. https://doi.org/10.3390/ani12223192
Nybroe S, Bjørnvad CR, Hansen CFH, Andersen TSL, Kieler IN. Outcome of Acquired Fanconi Syndrome Associated with Ingestion of Jerky Treats in 30 Dogs. Animals. 2022; 12(22):3192. https://doi.org/10.3390/ani12223192
Chicago/Turabian StyleNybroe, Stinna, Charlotte R. Bjørnvad, Camilla F. H. Hansen, Tenna S. L. Andersen, and Ida N. Kieler. 2022. "Outcome of Acquired Fanconi Syndrome Associated with Ingestion of Jerky Treats in 30 Dogs" Animals 12, no. 22: 3192. https://doi.org/10.3390/ani12223192
APA StyleNybroe, S., Bjørnvad, C. R., Hansen, C. F. H., Andersen, T. S. L., & Kieler, I. N. (2022). Outcome of Acquired Fanconi Syndrome Associated with Ingestion of Jerky Treats in 30 Dogs. Animals, 12(22), 3192. https://doi.org/10.3390/ani12223192