
Beraprost Sodium for Pulmonary Hypertension in Dogs: Effect on Hemodynamics and Cardiac Function

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Protocol
2.3. Echocardiography
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics
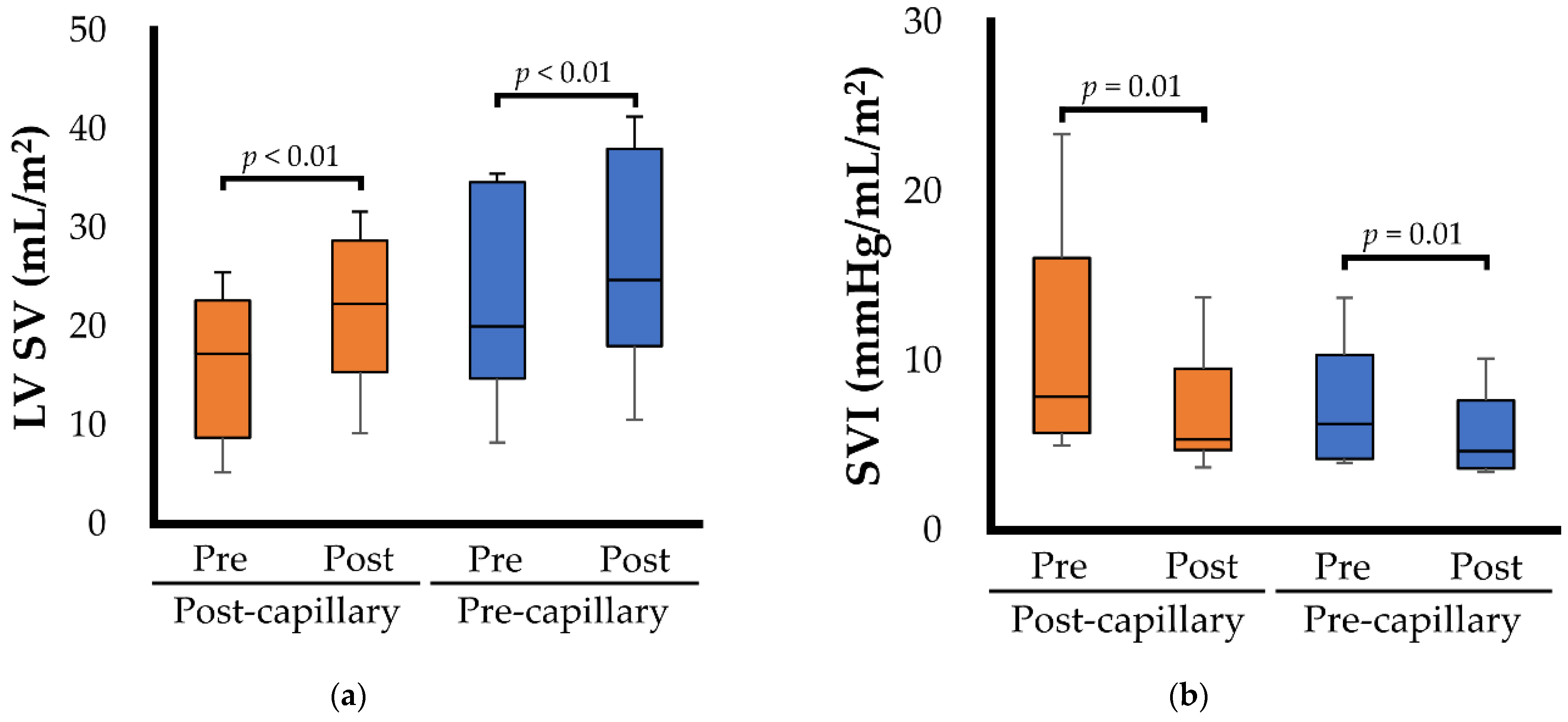
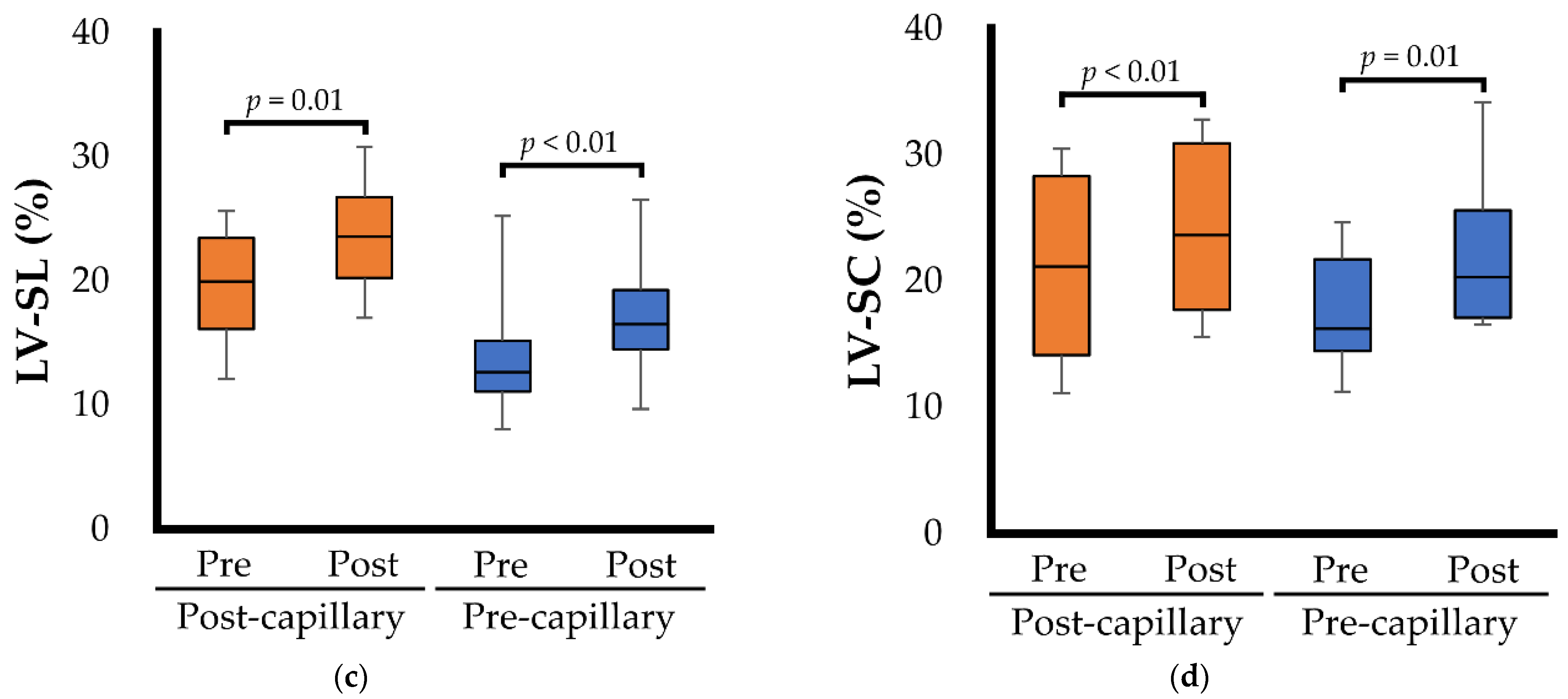
3.2. Echocardiographic Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reinero, C.; Visser, L.C.; Kellihan, H.B.; Masseau, I.; Rozanski, E.; Clercx, C.; Williams, K.; Abbott, J.A.; Borgarelli, M.; Scansen, B.A. ACVIM Consensus Statement Guidelines for the Diagnosis, Classification, Treatment, and Monitoring of Pulmonary Hypertension in Dogs. J. Vet. Intern. Med. 2020, 34, 549–573. [Google Scholar] [CrossRef] [PubMed]
- Borgarelli, M.; Abbott, J.A.; Braz-Ruivo, L.; Chiavegato, D.; Crosara, S.; Lamb, K.; Ljungvall, I.; Poggi, M.; Santilli, R.A.; Haggstrom, J. Prevalence and Prognostic Importance of Pulmonary Hypertension in Dogs with Myxomatous Mitral Valve Disease. J. Vet. Intern. Med. 2015, 29, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Jaffey, J.A.; Wiggen, K.; Leach, S.B.; Masseau, I.; Girens, R.E.; Reinero, C.R. Pulmonary Hypertension Secondary to Respiratory Disease and/or Hypoxia in Dogs: Clinical Features, Diagnostic Testing and Survival. Vet. J. 2019, 251, 105347. [Google Scholar] [CrossRef] [PubMed]
- Vezzosi, T.; Domenech, O.; Costa, G.; Marchesotti, F.; Venco, L.; Zini, E.; del Palacio, M.J.F.; Tognetti, R. Echocardiographic Evaluation of the Right Ventricular Dimension and Systolic Function in Dogs with Pulmonary Hypertension. J. Vet. Intern. Med. 2018, 32, 1541–1548. [Google Scholar] [CrossRef]
- Bach, J.F.; Rozanski, E.A.; MacGregor, J.; Betkowski, J.M.; Rush, J.E. Retrospective Evaluation of Sildenafil Citrate as a Therapy for Pulmonary Hypertension in Dogs. J. Vet. Intern. Med. 2006, 20, 1132–1135. [Google Scholar] [CrossRef]
- Akabane, R.; Sakatani, A.; Ogawa, M.; Nagakawa, M.; Miyakawa, H.; Miyagawa, Y.; Takemura, N. The Effect of Sildenafil on Pulmonary Haemodynamics in a Canine Model of Chronic Embolic Pulmonary Hypertension. Res. Vet. Sci. 2020, 133, 106–110. [Google Scholar] [CrossRef]
- Ueda, Y.; Johnson, L.R.; Ontiveros, E.S.; Visser, L.C.; Gunther-Harrington, C.T.; Stern, J.A. Effect of a Phosphodiesterase-5A (PDE5A) Gene Polymorphism on Response to Sildenafil Therapy in Canine Pulmonary Hypertension. Sci. Rep. 2019, 9, 6899. [Google Scholar] [CrossRef]
- Hoendermis, E.S.; Liu, L.C.Y.; Hummel, Y.M.; van der Meer, P.; de Boer, R.A.; Berger, R.M.F.; van Veldhuisen, D.J.; Voors, A.A. Effects of Sildenafil on Invasive Haemodynamics and Exercise Capacity in Heart Failure Patients with Preserved Ejection Fraction and Pulmonary Hypertension: A Randomized Controlled Trial. Eur. Heart J. 2015, 36, 2565–2573. [Google Scholar] [CrossRef]
- Redfield, M.M.; Chen, H.H.; Borlaug, B.A.; Semigran, M.J.; Lee, K.L.; Lewis, G.; Lewinter, M.M.; Rouleau, J.L.; Bull, D.A.; Mann, D.L.; et al. Effect of Phosphodiesterase-5 Inhibition on Exercise Capacity and Clinical Status in Heart Failure with Preserved Ejection Fraction a Randomized Clinical Trial. JAMA 2013, 309, 1268–1277. [Google Scholar] [CrossRef]
- Boilson, B.A.; Schirger, J.A.; Borlaug, B.A. Caveat Medicus! Pulmonary Hypertension in the Elderly: A Word of Caution. Eur. J. Heart Fail. 2010, 12, 89–93. [Google Scholar] [CrossRef]
- Koh, E.; Morimoto, S.; Jiang, B.; Inoue, T.; Nabata, T.; Kitano, S.; Yasuda, O.; Fukuo, K.; Ogihara, T. Effects of Beraprost Sodium, a Stable Analogue of Prostacyclin, on Hyperplasia, Hypertrophy and Glycosaminoglycan Synthesis of Rat Aortic Smooth Muscle Cells. Artery 1993, 20, 242–252. [Google Scholar] [PubMed]
- Akiba, T.; Miyazaki, M.; Toda, N. Vasodilator Actions of TRK-100, a New Prostaglandin I2 Analogue. Br. J. Pharmacol. 1986, 89, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Nishio, S.; Matsuura, H.; Kanai, N.; Fukatsu, Y.; Hirano, T.; Nishikawa, N.; Kameoka, K.; Umetsu, T. The in Vitro and Ex Vivo Antiplatelet Effect of TRK-100, a Stable Prostacyclin Analog, in Several Species. Jpn. J. Pharmacol. 1988, 47, 1–10. [Google Scholar] [CrossRef]
- Tamura, M.; Kurumatani, H.; Matsushita, T. Comparative Effects of Beraprost, a Stable Analogue of Prostacyclin, with PGE1, Nitroglycerin and Nifedipine on Canine Model of Vasoconstrictive Pulmonary Hypertension. Prostaglandins Leukot. Essent. Fat. Acids 2001, 64, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Yuchi, Y.; Saito, T.; Teshima, T.; Matsumoto, H.; Koyama, H. Investigation of Beraprost Sodium on Cardiac Function and Hemodynamics in Canine Models of Chronic Pulmonary Hypertension. Front. Vet. Sci. 2022, 9, 876178. [Google Scholar] [CrossRef]
- Yuchi, Y.; Suzuki, R.; Teshima, T.; Matsumoto, H.; Koyama, H. Utility of Tricuspid Annular Plane Systolic Excursion Normalized by Right Ventricular Size Indices in Dogs with Postcapillary Pulmonary Hypertension. J. Vet. Intern. Med. 2021, 35, 107–119. [Google Scholar] [CrossRef]
- Johnson, L.R.; Boon, J.A.; Orton, E.C. Clinical Characteristics of 53 Dogs with Doppler-Derived Evidence of Pulmonary Hypertension: 1992-1996. J. Vet. Intern. Med. Am. Coll. Vet. Intern. Med. 1999, 13, 440–447. [Google Scholar] [CrossRef]
- Visser, L.C.; Im, M.K.; Johnson, L.R.; Stern, J.A. Diagnostic Value of Right Pulmonary Artery Distensibility Index in Dogs with Pulmonary Hypertension: Comparison with Doppler Echocardiographic Estimates of Pulmonary Arterial Pressure. J. Vet. Intern. Med. 2016, 30, 543–552. [Google Scholar] [CrossRef]
- Takenaka, M.; Iio, A.; Sato, R.; Sakamoto, T.; Kurumatani, H. A Double-Blind, Placebo-Controlled, Multicenter, Prospective, Randomized Study of Beraprost Sodium Treatment for Cats with Chronic Kidney Disease. J. Vet. Intern. Med. 2018, 32, 236–248. [Google Scholar] [CrossRef]
- Cornell, C.C.; Kittleson, M.D.; della Torre, P.; Häggström, J.; Lombard, C.W.; Pedersen, H.D.; Vollmar, A.; Wey, A. Allometric Scaling of M-Mode Cardiac Measurements in Normal Adult Dogs. J. Vet. Intern. Med. 2004, 18, 311–321. [Google Scholar] [CrossRef]
- Visser, L.C.; Ciccozzi, M.M.; Sintov, D.J.; Sharpe, A.N. Echocardiographic Quantitation of Left Heart Size and Function in 122 Healthy Dogs: A Prospective Study Proposing Reference Intervals and Assessing Repeatability. J. Vet. Intern. Med. 2019, 33, 1909–1920. [Google Scholar] [CrossRef] [PubMed]
- Rishniw, M.; Caivano, D.; Dickson, D.; Vatne, L.; Harris, J.; Matos, J.N. Two-Dimensional Echocardiographic Left-Atrial-to-Aortic Ratio in Healthy Adult Dogs: A Reexamination of Reference Intervals. J. Vet. Cardiol. 2019, 26, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Schiller, N.B.; Shah, P.M.; Crawford, M.; DeMaria, A.; Devereux, R.; Feigenbaum, H.; Gutgesell, H.; Reichek, N.; Sahn, D.; Schnittger, I.; et al. Recommendations for Quantitation of the Left Ventricle by Two-Dimensional Echocardiography. J. Am. Soc. Echocardiogr. 1989, 2, 358–367. [Google Scholar] [CrossRef]
- Gustafson, D.L.; Bailey, D.B. Cancer Chemotherapy. In Withrow and MacEwen’s Small Animal Clinical Oncology; Vali, D.M., Douglas, T.H., Liptak, J.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 182–208. ISBN 978-0-323-59496-7. [Google Scholar]
- Schober, K.E.; Luis Fuentes, V.L. Effects of Age, Body Weight, and Heart Rate on Transmitral and Pulmonary Venous Flow in Clinically Normal Dogs. Am. J. Vet. Res. 2001, 62, 1447–1454. [Google Scholar] [CrossRef] [PubMed]
- Teshima, K.; Asano, K.; Sasaki, Y.; Kato, Y.; Kutara, K.; Edamura, K.; Hasegawa, A.; Tanaka, S. Assessment of Left Ventricular Function Using Pulsed Tissue Doppler Imaging in Healthy Dogs and Dogs with Spontaneous Mitral Regurgitation. J. Vet. Med. Sci. 2005, 67, 1207–1215. [Google Scholar] [CrossRef]
- Oyama, M.A.; Sisson, D.D.; Bulmer, B.J.; Constable, P.D. Echocardiographic Estimation of Mean Left Atrial Pressure in a Canine Model of Acute Mitral Valve Insufficiency. J. Vet. Intern. Med. 2004, 18, 667. [Google Scholar] [CrossRef]
- Visser, L.C.; Scansen, B.A.; Schober, K.E.; Bonagura, J.D. Echocardiographic Assessment of Right Ventricular Systolic Function in Conscious Healthy Dogs: Repeatability and Reference Intervals. J. Vet. Cardiol. 2015, 17, 83–96. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. Endorsed by the European Association of Echocardiography, a Registered Branch of the European Society of Cardiology, And. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef]
- Gentile-Solomon, J.M.; Abbott, J.A. Conventional Echocardiographic Assessment of the Canine Right Heart: Reference Intervals and Repeatability. J. Vet. Cardiol. 2016, 18, 234–247. [Google Scholar] [CrossRef]
- Visser, L.C.; Sintov, D.J.; Oldach, M.S. Evaluation of Tricuspid Annular Plane Systolic Excursion Measured by Two-Dimensional Echocardiography in Healthy Dogs: Repeatability, Reference Intervals, and Comparison with M-Mode Assessment. J. Vet. Cardiol. 2018, 20, 165–174. [Google Scholar] [CrossRef]
- Lewis, J.F.; Kuo, L.C.; Nelson, J.G.; Limacher, M.C.; Quinones, M.A. Pulsed Doppler Echocardiographic Determination of Stroke Volume and Cardiac Output: Clinical Validation of Two New Methods Using the Apical Window. Circulation 1984, 70, 425–431. [Google Scholar] [CrossRef]
- Suzuki, R.; Matsumoto, H.; Teshima, T.; Koyama, H. Clinical Assessment of Systolic Myocardial Deformations in Dogs with Chronic Mitral Valve Insufficiency Using Two-Dimensional Speckle-Tracking Echocardiography. J. Vet. Cardiol. 2013, 15, 41–49. [Google Scholar] [CrossRef]
- Suzuki, R.; Matsumoto, H.; Teshima, T.; Koyama, H. Effect of Age on Myocardial Function Assessed by Two-Dimensional Speckle-Tracking Echocardiography in Healthy Beagle Dogs. J. Vet. Cardiol. 2013, 15, 243–252. [Google Scholar] [CrossRef]
- Suzuki, R.; Yuchi, Y.; Kanno, H.; Saito, T.; Teshima, T.; Matsumoto, H.; Koyama, H. Pulmonary Vascular Resistance Estimated by Echocardiography in Dogs with Myxomatous Mitral Valve Disease and Pulmonary Hypertension Probability. Front. Vet. Sci. 2021, 8, 771726. [Google Scholar] [CrossRef]
- Yuchi, Y.; Suzuki, R.; Kanno, H.; Saito, T.; Teshima, T.; Matsumoto, H.; Koyama, H. Influence of Heart Rate on Right Ventricular Function Assessed by Right Heart Catheterization and Echocardiography in Healthy Anesthetized Dogs. BMC Vet. Res. 2022, 18, 166. [Google Scholar] [CrossRef]
- Yuchi, Y.; Suzuki, R.; Kanno, H.; Teshima, T.; Matsumoto, H.; Koyama, H. Right Ventricular Myocardial Adaptation Assessed by Two-Dimensional Speckle Tracking Echocardiography in Canine Models of Chronic Pulmonary Hypertension. Front. Vet. Sci. 2021, 8, 727155. [Google Scholar] [CrossRef]
- Yuchi, Y.; Suzuki, R.; Teshima, T.; Matsumoto, H.; Koyama, H. Right Ventricular Systolic and Diastolic Function Assessed by Two-Dimensional Speckle Tracking Echocardiography in Dogs with Myxomatous Mitral Valve Disease. J. Vet. Med. Sci. 2021, 83, 1918–1927. [Google Scholar] [CrossRef]
- Sun, D.; Yang, W.; Wang, Z.; Gao, B. Efficacy of Beraprost Sodium Combined with Sildenafil and Its Effects on Vascular Endothelial Function and Inflammation in Patients Experiencing Left Heart Failure Complicated with Pulmonary Arterial Hypertension. Med. Sci. Monit. 2021, 27, e928413-1–e928413-7. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Pre-Examination | Post-Examination |
|---|---|---|
| Age (year) | 13.2 (10.9–14.6) | 13.3 (10.9–14.7) |
| Sex (male/female) | 3/13 | |
| Body weight (kg) | 4.0 (3.2–6.7) | 4.0 (3.1–6.7) |
| BPS dose (µg/kg) | Range: 13.4–22.0 | |
| Dosing period (days) | Range: 7–21 | |
| Heart rate (bpm) | 125 (109–148) | 121 (107–138) |
| Systolic blood pressure (mmHg) | 136 (123–144) | 125 (114–141) |
| Mean blood pressure (mmHg) | 100 (86–111) | 98 (82–107) |
| PH severity (mild/moderate/severe) | 0/5/11 | 0/7/9 |
| RHF (n) | ||
| Pre-capillary PH | 3/8 (38%) | 2/8 (25%) |
| Post-capillary PH | 5/8 (63%) | 2/8 (25%) |
| Clinical signs suggestive of PH (n) | ||
| Syncope | 10/16 (63%) | 7/16 (44%) |
| Weakness | 13/16 (81%) | 9/16 (56%) |
| Respiratory distress at rest | 6/16 (38%) | 6/16 (38%) |
| Exercise intolerance | 11/16 (69%) | 8/16 (50%) |
| Medications | Post-Capillary PH | Pre-Capillary PH |
|---|---|---|
| Angiotensin-converting enzyme inhibitor (n) | 8/8 (100%) | 1/8 (13%) |
| Pimobendan (n) | 8/8 (100%) | 2/8 (25%) |
| Spironolactone (n) | 4/8 (50%) | 0/8 (0%) |
| Loop diuretics (n) | 6/8 (75%) | 0/8 (0%) |
| Calcium channel blocker (n) | 4/8 (50%) | 0/8 (0%) |
| Isosorbide dinitrate (n) | 6/8 (75%) | 0/8 (0%) |
| Sildenafil (n) | 3/8 (38%) | 2/8 (25%) |
| Antimicrobials (n) | 0/8 (0%) | 5/8 (63%) |
| Corticosteroid (n) | 0/8 (0%) | 5/8 (63%) |
| Antiplatelet drug (n) | 0/8 (0%) | 1/8 (13%) |
| Variables | Post-Capillary PH (n = 8) | Pre-Capillary PH (n = 8) | ||||
|---|---|---|---|---|---|---|
| Pre-Examination | Post-Examination | p | Pre-Examination | Post-Examination | p | |
| LA/Ao | 2.2 (1.7–2.9) | 2.4 (1.6–2.7) | 0.093 | 1.0 (1.0–1.2) | 1.1 (1.0–1.3) | 0.310 |
| LVIDDN (cm/kg0.294) | 2.1 (1.6–2.2) | 2.3 (1.6–2.4) | 0.211 | 1.1 (0.8–1.3) | 1.2 (0.9–1.4) | 0.327 |
| LVIDSN (cm/kg0.315) | 0.9 (0.9–1.1) | 1.0 (0.8–1.2) | 0.465 | 0.6 (0.5–0.6) | 0.6 (0.5–0.8) | 0.533 |
| Fractional shortening (%) | 48.3 (41.5–54.4) | 49.8 (41.5–57.4) | 0.579 | 45.3 (38.3–52.5) | 46.2 (42.9–53.9) | 0.150 |
| LVEDVI (mL/m2) | 79.0 (53.6–97.7) | 88.0 (54.5–105.2) | 0.130 | 28.2 (16.1–37.9) | 32.3 (19.7–39.0) * | 0.032 |
| LVESVI (mL/m2) | 27.9 (23.1–40.9) | 27.9 (20.5–38.1) | 0.251 | 13.0 (8.1–18.4) | 12.8 (10.5–14.5) | 0.515 |
| Ejection fraction (%) | 61.1 (51.0–65.3) | 64.6 (58.1–70.6) * | 0.004 | 51.6 (46.2–54.5) | 61.2 (48.2–64.0) * | 0.024 |
| E (m/s) | 1.2 (1.0–1.5) | 1.2 (0.8–1.3) | 0.354 | 0.6 (0.5–0.6) | 0.5 (0.5–0.6) | 0.594 |
| E/A | 1.3 (1.0–2.5) | 1.2 (0.8–1.5) | 0.362 | 0.8 (0.7–1.0) | 0.8 (0.8–0.9) | 0.407 |
| E/e’ | 18.5 (12.9–23.3) | 12.1 (10.1–18.0) | 0.230 | 13.4 (8.9–15.3) | 13.6 (11.1–14.7) | 0.906 |
| MR velocity (m/s) | 5.5 (5.2–5.8) | 5.9 (5.5–6.2) * | 0.047 | Not available | Not available | |
| Variables | Post-Capillary PH (n = 8) | Pre-Capillary PH (n = 8) | ||||
|---|---|---|---|---|---|---|
| Pre-Examination | Post-Examination | p | Pre-Examination | Post-Examination | p | |
| PA/Ao | 1.0 (1.0–1.1) | 1.0 (0.9–1.1) | 0.635 | 1.0 (1.0–1.1) | 1.0 (1.0–1.1) | 0.331 |
| RVEDA (cm2) | 2.9 (1.8–4.7) | 2.8 (1.8–3.6) | 0.371 | 3.4 (2.0–4.2) | 3.3 (2.3–4.0) | 0.221 |
| RVESA (cm2) | 1.4 (1.0–2.9) | 1.4 (0.9–1.7) | 0.111 | 2.2 (1.1–2.6) | 1.7 (1.1–2.3) | 0.050 |
| RV FACn (%/kg−0.097) | 46.4 (35.6–54.7) | 59.5 (55.9–63.0) * | 0.006 | 45.9 (39.4–50.5) | 48.5 (43.0–57.8) * | 0.034 |
| TAPSEn (mm/kg0.284) | 6.6 (6.3–8.1) | 7.4 (6.2–9.3) | 0.374 | 4.1 (3.0–5.2) | 5.0 (4.5–5.5) | 0.150 |
| RV s’ (cm/s) | 13.2 (8.4–16.2) | 11.6 (9.4–17.9) | 0.627 | 5.3 (4.9–7.6) | 7.3 (5.4–8.9) | 0.164 |
| TR velocity (m/s) | 4.1 (3.6–5.0) | 3.5 (3.1–4.9) * | 0.033 | 4.6 (4.5–5.2) | 4.2 (4.1–4.8) * | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, R.; Yuchi, Y.; Saito, T.; Yasumura, Y.; Teshima, T.; Matsumoto, H.; Koyama, H. Beraprost Sodium for Pulmonary Hypertension in Dogs: Effect on Hemodynamics and Cardiac Function. Animals 2022, 12, 2078. https://doi.org/10.3390/ani12162078
Suzuki R, Yuchi Y, Saito T, Yasumura Y, Teshima T, Matsumoto H, Koyama H. Beraprost Sodium for Pulmonary Hypertension in Dogs: Effect on Hemodynamics and Cardiac Function. Animals. 2022; 12(16):2078. https://doi.org/10.3390/ani12162078
Chicago/Turabian StyleSuzuki, Ryohei, Yunosuke Yuchi, Takahiro Saito, Yuyo Yasumura, Takahiro Teshima, Hirotaka Matsumoto, and Hidekazu Koyama. 2022. "Beraprost Sodium for Pulmonary Hypertension in Dogs: Effect on Hemodynamics and Cardiac Function" Animals 12, no. 16: 2078. https://doi.org/10.3390/ani12162078
APA StyleSuzuki, R., Yuchi, Y., Saito, T., Yasumura, Y., Teshima, T., Matsumoto, H., & Koyama, H. (2022). Beraprost Sodium for Pulmonary Hypertension in Dogs: Effect on Hemodynamics and Cardiac Function. Animals, 12(16), 2078. https://doi.org/10.3390/ani12162078