
Priorities for Research into the Impact of Canine Surgical Sterilisation Programmes for Free-Roaming Dogs: An International Priority Setting Partnership


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The James Lind Alliance Priority Setting Partnership Process Initiation
2.1.1. Steering Group
2.1.2. Participants
2.1.3. Scope
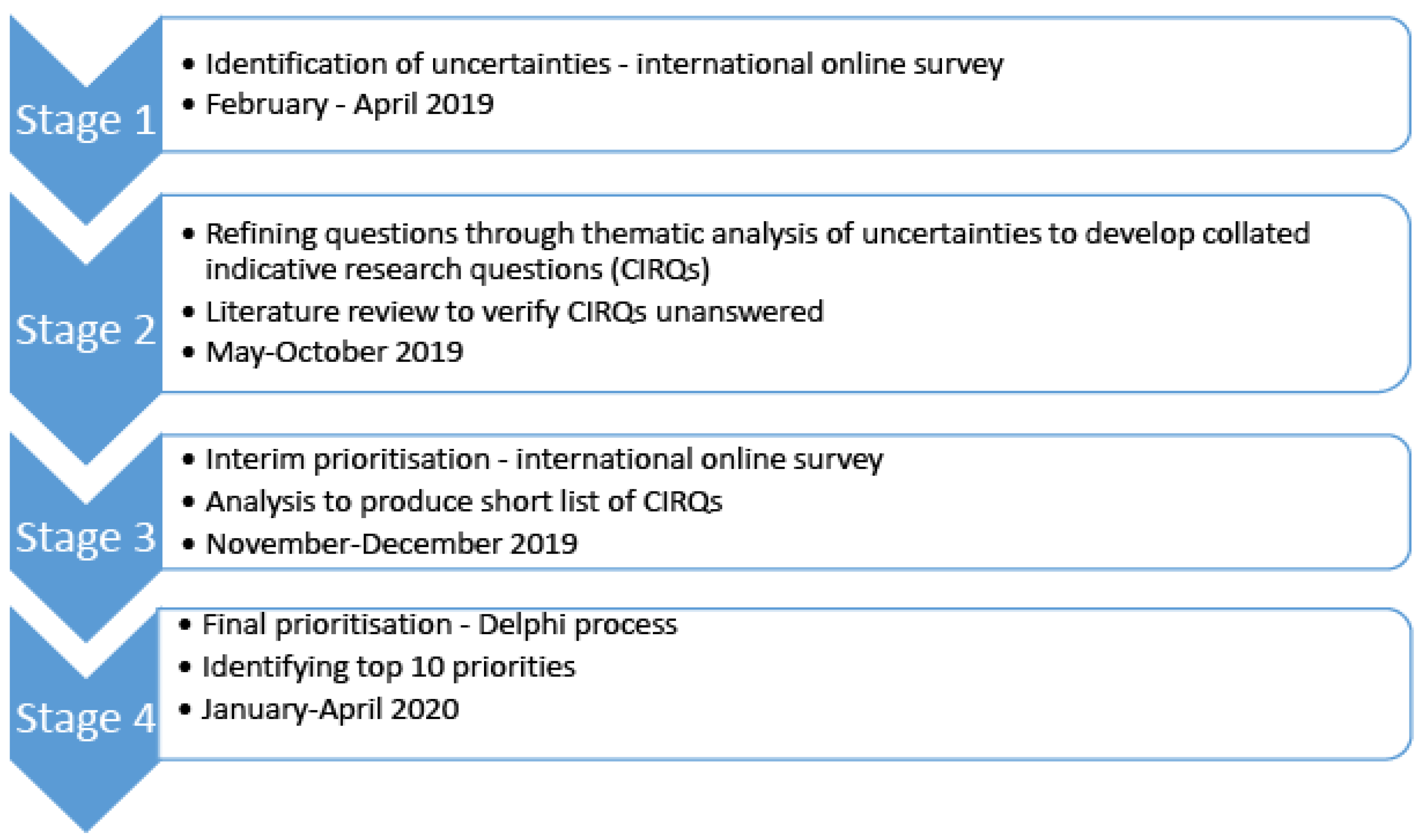
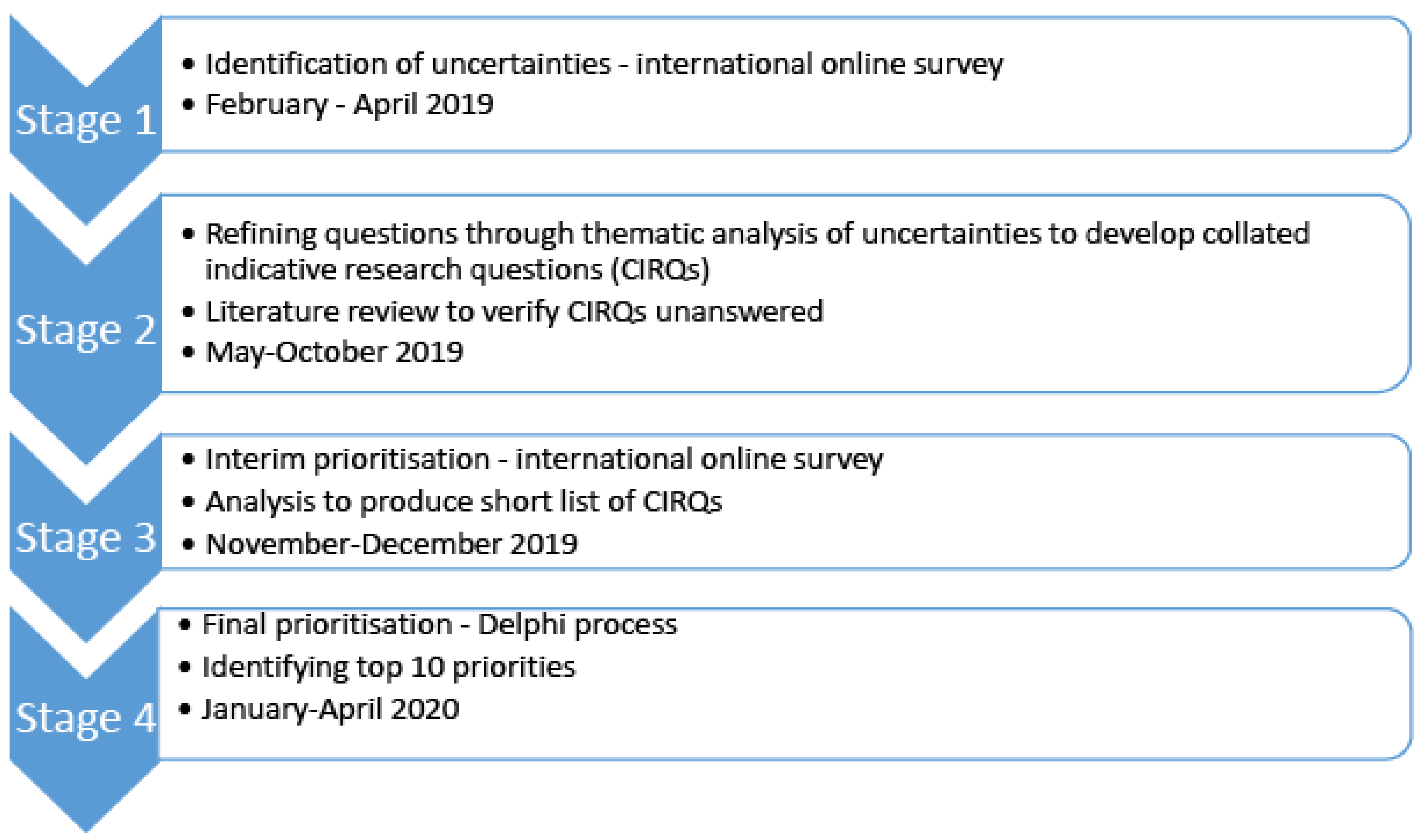
2.2. Stage 1: Identification of Uncertainties
2.3. Stage 2: Refining Questions and Literature Review
2.4. Stage 3: Interim Prioritisation
2.5. Stage 4: Final Prioritisation
3. Results
3.1. Participant Demographics
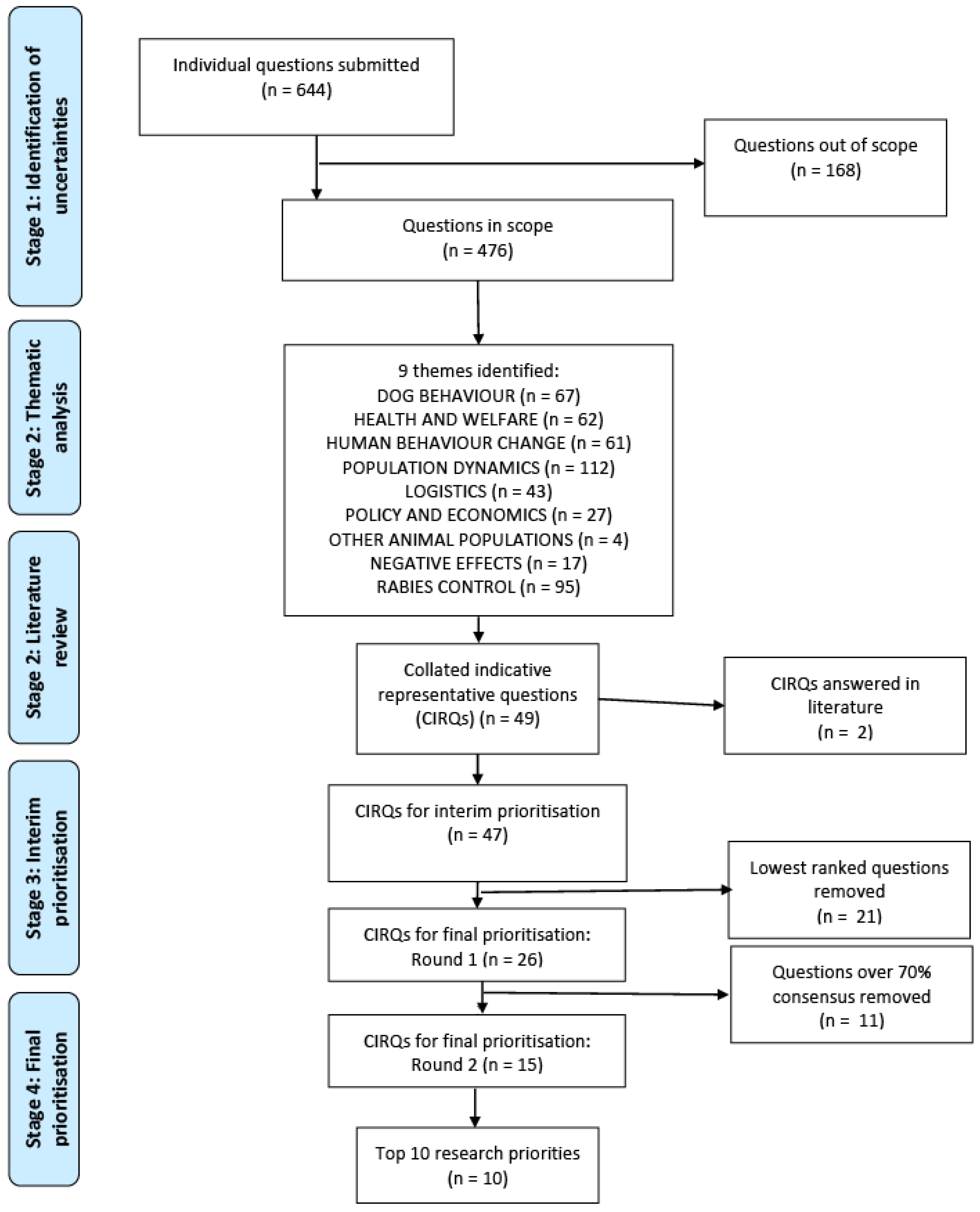
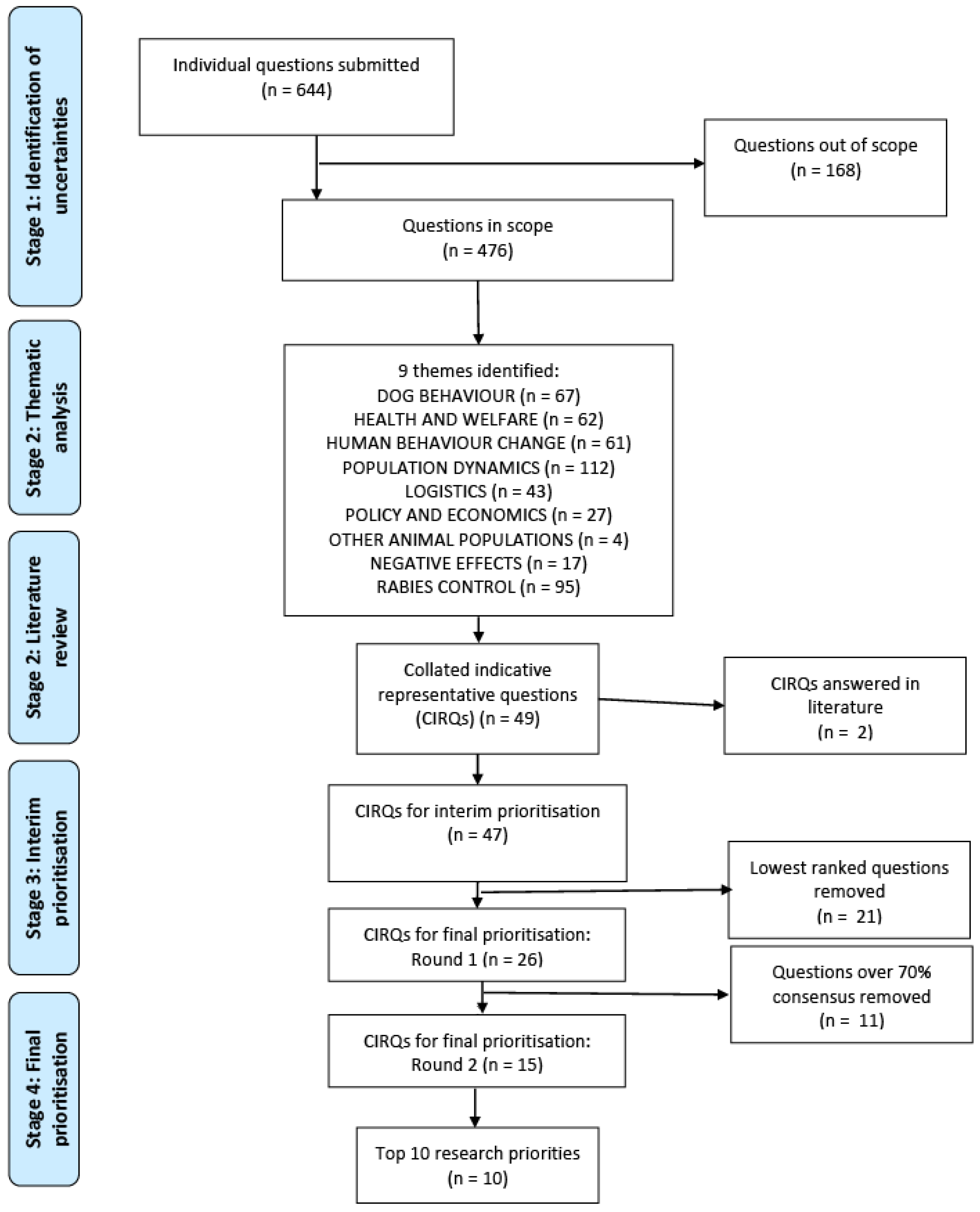
3.2. Stage 1: Identification of Uncertainties
3.3. Stage 2: Refining Questions and Literature Review
3.4. Stage 3: Interim Prioritisation
3.5. Stage 4: Final Prioritisation
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Companion Animal Management Coalition (ICAM). Humane Dog Population Management Guidance: 2019 Update. 2019. Available online: https://www.icam-coalition.org/wp-content/uploads/2019/09/2019-ICAM-DPM-guidance-Interactive-updated-15-Oct-2019.pdf (accessed on 30 June 2021).
- Hiby, E.; Atema, K.N.; Brimley, R.; Hammond-Seaman, A.; Jones, M.; Rowan, A.; Fogelberg, E.; Kennedy, M.; Balaram, D.; Nel, L. Scoping review of indicators and methods of measurement used to evaluate the impact of dog population management interventions. BMC Vet. Res. 2017, 13, 143. [Google Scholar] [CrossRef]
- Smith, L.M.; Hartmann, S.; Munteanu, A.M.; Dalla Villa, P.; Quinnell, R.J.; Collins, L.M. The Effectiveness of Dog Population Management: A Systematic Review. Animals 2019, 9, 1020. [Google Scholar] [CrossRef] [Green Version]
- Collinson, A.; Bennett, M.; Brennan, M.L.; Dean, R.S.; Stavisky, J. Evaluating the role of surgical sterilisation in canine rabies control: A systematic review of impact and outcomes. PLoS Negl. Trop. Dis. 2020, 14, e0008497. [Google Scholar] [CrossRef] [PubMed]
- Belsare, A.; Vanak, A.T. Modelling the challenges of managing free-ranging dog populations. Sci. Rep. 2020, 10, 18874. [Google Scholar] [CrossRef]
- Taylor, L.H.; Wallace, R.M.; Balaram, D.; Lindenmayer, J.M.; Eckery, D.C.; Mutonono-Watkiss, B.; Parravani, E.; Nel, L.H. The Role of Dog Population Management in Rabies Elimination—A Review of Current Approaches and Future Opportunities. Front. Vet. Sci. 2017, 4, 109. [Google Scholar] [CrossRef] [PubMed]
- Crowe, S.; Fenton, M.; Hall, M.; Cowan, K.; Chalmers, I. Patients’, clinicians’ and the research communities’ priorities for treatment research: There is an important mismatch. Res. Involv. Engagem. 2015, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Laurance, W.F.; Koster, H.; Grooten, M.; Anderson, A.B.; Zuidema, P.A.; Zwick, S.; Zagt, R.J.; Lynam, A.J.; Linkie, M.; Anten, N.P.R. Making conservation research more relevant for conservation practitioners. Biol. Conserv. 2012, 153, 164–168. [Google Scholar] [CrossRef]
- Brett, J.; Staniszewska, S.; Mockford, C.; Herron-Marx, S.; Hughes, J.; Tysall, C.; Suleman, R. Mapping the impact of patient and public involvement on health and social care research: A systematic review. Health Expect. 2014, 17, 637–650. [Google Scholar] [CrossRef]
- Alliance, J.L. The James Lind Alliance Guidebook (Version 8). 2018. Available online: https://www.jla.nihr.ac.uk/jla-guidebook/ (accessed on 30 June 2021).
- Tallon, D.; Chard, J.; Dieppe, P. Relation between agendas of the research community and the research consumer. Lancet 2000, 355, 2037–2040. [Google Scholar] [CrossRef]
- Chalmers, I.; Essali, A.; Rezk, E.; Crowe, S. Is academia meeting the needs of non-academic users of the results of research? Lancet 2012, 380, S43. [Google Scholar] [CrossRef]
- Chalmers, I.; Glasziou, P. Avoidable waste in the production and reporting of research evidence. Lancet 2009, 374, 86–89. [Google Scholar] [CrossRef]
- Dean, R.S. Identification of Research Priorities of Veterinary Surgeons and Cat Owners with Regard to the Treatment of Chronic Kidney Disease (CKD) in Cats. Master’s Thesis, University of Oxford, Oxford, UK, 2014. [Google Scholar]
- Tatum, R.C.; McGowan, C.M.; Dean, R.S.; Ireland, J.L. Equine pituitary pars intermedia dysfunction: Identifying research priorities for diagnosis, treatment and prognosis through a priority setting partnership. PLoS ONE 2021, 16, e0244784. [Google Scholar] [CrossRef]
- Bacon, H.; Vancia, V.; Walters, H.; Waran, N. Canine trap-neuter-return: A critical review of potential welfare issues. Anim. Welf. 2017, 26, 281–292. [Google Scholar] [CrossRef]
- Tong, A.; Synnot, A.; Crowe, S.; Hill, S.; Matus, A.; Scholes-Robertson, N.; Oliver, S.; Cowan, K.; Nasser, M.; Bhaumik, S.; et al. Reporting guideline for priority setting of health research (REPRISE). BMC Med. Res. Methodol. 2019, 19, 243. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Rattanavipapong, W.; Thavorncharoensap, M.; Youngkong, S.; Genuino, A.J.; Anothaisintawee, T.; Chaikledkaew, U.; Meeyai, A. The impact of transmission dynamics of rabies control: Systematic review. Vaccine 2019, 37 (Suppl. 1), A154–A165. [Google Scholar] [CrossRef]
- Zinsstag, J.; Schelling, E.; Waltner-Toews, D.; Tanner, M. From “one medicine” to “one health” and systemic approaches to health and well-being. Prev. Vet. Med. 2011, 101, 148–156. [Google Scholar] [CrossRef] [Green Version]
- International Companion Animal Management Coalition (ICAM). Are We Making a Difference? A Guide to Monitoring and Evaluating Dog Population Management Interventions. 2015. Available online: http://www.icam-coalition.org/downloads/ICAM_Guidance_Document.pdf (accessed on 30 June 2021).
- Reed, K.; Upjohn, M.M. Better Lives for Dogs: Incorporating Human Behaviour Change into a Theory of Change to Improve Canine Welfare Worldwide. Front. Vet. Sci. 2018, 5, 93. [Google Scholar] [CrossRef]
- Reece, J.F.; Chawla, S.K. Control of rabies in Jaipur, India, by the sterilisation and vaccination of neighbourhood dogs. Vet. Rec. 2006, 159, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Totton, S.C.; Wandeler, A.I.; Zinsstag, J.; Bauch, C.T.; Ribble, C.S.; Rosatte, R.C.; McEwen, S.A. Stray dog population demographics in Jodhpur, India following a population control/rabies vaccination program. Prev. Vet. Med. 2010, 97, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Riley, T.; Lovett, R.; Thandrayen, J.; Cumming, B.; Thurber, K.A. Evaluating Impacts of a One Health Approach to Companion Animal Health and Management in a Remote Aboriginal Community in the Northern Territory, Australia. Animals 2020, 10, 1790. [Google Scholar] [CrossRef]
- Santos Baquero, O.; Akamine, L.A.; Amaku, M.; Ferreira, F. Defining priorities for dog population management through mathematical modeling. Prev. Vet. Med. 2016, 123, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Hiby, E.; Hiby, L. Direct Observation of Dog Density and Composition during Street Counts as a Resource Efficient Method of Measuring Variation in Roaming Dog Populations over Time and between Locations. Animals 2017, 7, 57. [Google Scholar] [CrossRef] [Green Version]
- Macpherson, C.; Meslin, F.; Wandeler, A. Dogs, Zoonoses and Public Health, 2nd ed.; CABI Publishing: New York, NY, USA, 2013. [Google Scholar]
- Reece, J.; Chawla, S.; Hiby, A. Decline in human dog-bite cases during a street dog sterilisation programme in Jaipur, India. Vet. Rec. 2013, 172, 473. [Google Scholar] [CrossRef]
- Ma, G.C.; Withers, A.-M.; Spencer, J.; Norris, J.M.; Ward, M.P. Evaluation of a Dog Population Management Intervention: Measuring Indicators of Impact. Animals 2020, 10, 1061. [Google Scholar] [CrossRef] [PubMed]
- Davlin, S.L.; Vonville, H.M. Canine rabies vaccination and domestic dog population characteristics in the developing world: A systematic review. Vaccine 2012, 30, 3492–3502. [Google Scholar] [CrossRef] [PubMed]
- Hampson, K.; Dushoff, J.; Cleaveland, S.; Haydon, D.T.; Kaare, M.; Packer, C.; Dobson, A. Transmission dynamics and prospects for the elimination of canine rabies. PLoS Biol. 2009, 7, e53. [Google Scholar] [CrossRef]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [Green Version]
- Oakley, A.; Strange, V.; Bonell, C.; Allen, E.; Stephenson, J. Process evaluation in randomised controlled trials of complex interventions. BMJ 2006, 332, 413–416. [Google Scholar] [CrossRef] [Green Version]
- Pawson, R.; Tilley, N. Realistic Evaluation; Sage: London, UK, 1997. [Google Scholar]
- Gurusamy, K.S.; Walmsley, M.; Davidson, B.R.; Frier, C.; Fuller, B.; Madden, A.; Masson, S.; Morley, R.; Safarik, I.; Tsochatzis, E.A.; et al. Top research priorities in liver and gallbladder disorders in the UK. BMJ Open 2019, 9, e025045. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.C.; Sandford, B.A. The Delphi technique: Making sense of consensus. Pract. Assess. Res. Eval. 2007, 12, 10. [Google Scholar]

{kind=link}
{kind=link}
| Initial Survey (n = 110) % | Interim Prioritisation (n = 107) % | Final Prioritisation | |||
|---|---|---|---|---|---|
| Round 1 (n = 44) % | Round 2 (n = 36) % | ||||
| Geographical region of residence | Africa | 15 | 18 | 11 | 6 |
| North America | 14 | 8 | 11 | 11 | |
| Latin America and the Caribbean | 15 | 9 | 16 | 17 | |
| Asia | 28 | 34 | 32 | 39 | |
| Oceania | 9 | 7 | 11 | 8 | |
| Europe | 20 | 24 | 18 | 19 | |
| Role | Vet | 62 | 51 | 39 | 36 |
| Vet nurse/technician | 10 | 7 | 11 | 11 | |
| Programme manager (non-veterinary) | 22 | 23 | 32 | 33 | |
| CAHW 1/AHT 2 | - | 5 | - | - | |
| Researcher | 3 | 6 | 16 | 17 | |
| Other | 4 | 7 | 2 | 3 | |
| Organisation | NGO | 75 | 71 | 80 | 78 |
| IGO 3 | 3 | 1 | - | - | |
| Government (national, state) | 18 | 15 | 5 | 6 | |
| Academic/research institute | 3 | 12 | 14 | 14 | |
| Other | 2 | 1 | 2 | 3 | |
| Main aim | Animal health | 26 | 22 | 21 | 19 |
| Human health/Public health | 9 | 3 | 2 | 3 | |
| Public health (veterinary) | 18 | 22 | 18 | 17 | |
| Animal welfare | 39 | 44 | 50 | 50 | |
| Education/training | 2 | 5 | 5 | 6 | |
| Community engagement | 2 | 1 | - | - | |
| Other | 4 | 5 | 5 | 6 | |
| Key Theme | Subtheme | Example Questions |
|---|---|---|
| Dog behaviour | Aggression | Do sterilised street dogs bite humans less? |
| Roaming | Do sterilised free-roaming dogs roam less? | |
| Reproductive behaviour | Does a focus on sterilising females have an impact on behaviour of males? | |
| Social structure/behaviour | Will a sterilised dog be accepted back into its pack after release? | |
| Dog health and welfare | Longevity | Average lifespan sterilised free-roaming dogs vs. unsterilised? |
| Specific health conditions | What is the impact of sterilisation in preventing TVT 1? | |
| Body condition score | Do sterilised street dogs have a higher body condition score than non-sterilised dogs? | |
| Human behaviour change | Barriers and facilitators to participation | How do we better engage with the community stakeholders prior to the project inception to ensure there is full community buy in and involvement? |
| Perception of FRDs | Does sterilisation change how people feel about their dogs (increased value)? | |
| Behaviours towards FRDs | Does this lead to a stronger human-animal bond—improved/more care provided by owners? | |
| Population dynamics | Population size | Do sterilisation programs reduce the size of dog populations? What percentage of dogs in a given population of dogs need to be sterilised to keep a dog population stable—no growth? |
| Population turnover | Do sterilisation programs reduce the birth rate (puppies born per 1000 dogs in population per year)? Does sterilising a specific dog population prevent other dogs entering this zone? | |
| Logistics | Targeting dogs for sterilisation | Who should be the priority for sterilisation and why—young females, adult females, young males, adult males—is this order correct? |
| Inaccessible dogs | Is neutering only targeting dogs that are friendly and easy to catch—hence the skittish ones are breeding? | |
| Geographical considerations | In which dog population group is surgical sterilisation most effective (rural vs. urban)? | |
| One off/intermittent | Are pop up spay/neuter clinics effective? Do they help to reduce street dog population sizes? How regular do these clinics need to be do be effective? | |
| Training component | Is there a measurable improvement (or increase) in local veterinary care (either qualifies veterinarians or para-vet personnel)? | |
| Policy and economics | Cost-effectiveness | What are the financial impacts for a government to convert from catch and kill to TNR 2? |
| Changes in policy | Do these programs change government support/intervention attitudes that then enable increased funding to continue such humane programs (vs. mass animal control such as poison baits) long term? | |
| Stakeholder expectations | Do the realistic expected outcomes of most dog population management interventions match the desired outcomes of stakeholders? | |
| Other animal populations | Other domestic animal populations | Do dog population management programs affect the size of the cat population? |
| Wildlife | Is sterilisation an effective means to reduce free-ranging dog impact on wildlife? | |
| Negative effects | Short term (i.e., directly related to surgery) | What is the surgical complication rate of sterilised free-roaming dogs? |
| Long term | Do free-roaming dogs suffer any long-term negative effects of being caught for a sterilisation programme, e.g., greater fear of or aggression towards humans, or difficulty integrating back into their group? | |
| Rabies control | Human behaviour change | Would people bring their animals to clinic just for surgery or just for vacc or do they perceive one is better than another? |
| Indirect effects | Could sterilisation programs reduce the rate of decline of vaccination coverage in the period between mass rabies vaccination campaigns, and thus allow for an increase in the period between these campaigns? | |
| Direct effects | Does sterilisation change contact rate between dogs? And therefore reduce rabies risk? | |
| Logistics | How long does an area that has had a ABC/AR 3 intervention of over 70% of the dogs stay rabies free if there is no re-vaccination of the dogs (as per data sheet)? |
| Final Ranking | Question | Theme | Aggregate Score |
|---|---|---|---|
| 1 | In order to affect the size of a dog population, what proportion of the population needs to be sterilised and over what time period? | Population dynamics | 279 |
| 2 | How do sterilisation programmes (of different sizes and durations) affect the size of dog populations? | Population dynamics | 221 |
| 3 | Does a sterilisation programme cause a change in dog population turnover (in terms of birth, death and migration rates)? | Population dynamics | 178 |
| 4 | Do areas with sterilisation programmes have a lower rate of dog bites in people than areas without sterilisation programmes? | Dog behaviour | 175 |
| 5 | Do areas with sterilisation and vaccination programmes have a lower incidence of rabies in dogs and humans than areas with vaccination only programmes (that achieve the same level of vaccination coverage)? | Rabies control | 171 |
| 6 | What are the effects of one-off or intermittent sterilisation (with or without vaccination) programmes in comparison to consistent programmes in an area? What frequency is optimal? | Logistics | 163 |
| 7 | What effect does targeting of female dogs only have on the impact of sterilisation programmes? | Logistics | 122 |
| 8 | Do sterilisation programmes affect community behaviour (human–dog interactions) towards free-roaming dogs? | Human behaviour change | 119 |
| 9 | Do sterilisation programmes affect community perception towards free-roaming dogs? | Human behaviour change | 94 |
| 10 | Does sterilisation have any direct effects on rabies transmission, e.g., in terms of behavioural changes? | Rabies control | 87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collinson, A.; Brennan, M.L.; Dean, R.S.; Stavisky, J. Priorities for Research into the Impact of Canine Surgical Sterilisation Programmes for Free-Roaming Dogs: An International Priority Setting Partnership. Animals 2021, 11, 2250. https://doi.org/10.3390/ani11082250
Collinson A, Brennan ML, Dean RS, Stavisky J. Priorities for Research into the Impact of Canine Surgical Sterilisation Programmes for Free-Roaming Dogs: An International Priority Setting Partnership. Animals. 2021; 11(8):2250. https://doi.org/10.3390/ani11082250
Chicago/Turabian StyleCollinson, Abi, Marnie L. Brennan, Rachel S. Dean, and Jenny Stavisky. 2021. "Priorities for Research into the Impact of Canine Surgical Sterilisation Programmes for Free-Roaming Dogs: An International Priority Setting Partnership" Animals 11, no. 8: 2250. https://doi.org/10.3390/ani11082250
APA StyleCollinson, A., Brennan, M. L., Dean, R. S., & Stavisky, J. (2021). Priorities for Research into the Impact of Canine Surgical Sterilisation Programmes for Free-Roaming Dogs: An International Priority Setting Partnership. Animals, 11(8), 2250. https://doi.org/10.3390/ani11082250