
Effects of Multimodal Analgesic Protocol, with Buprenorphine and Meloxicam, on Mice Well-Being: A Dose Finding Study

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
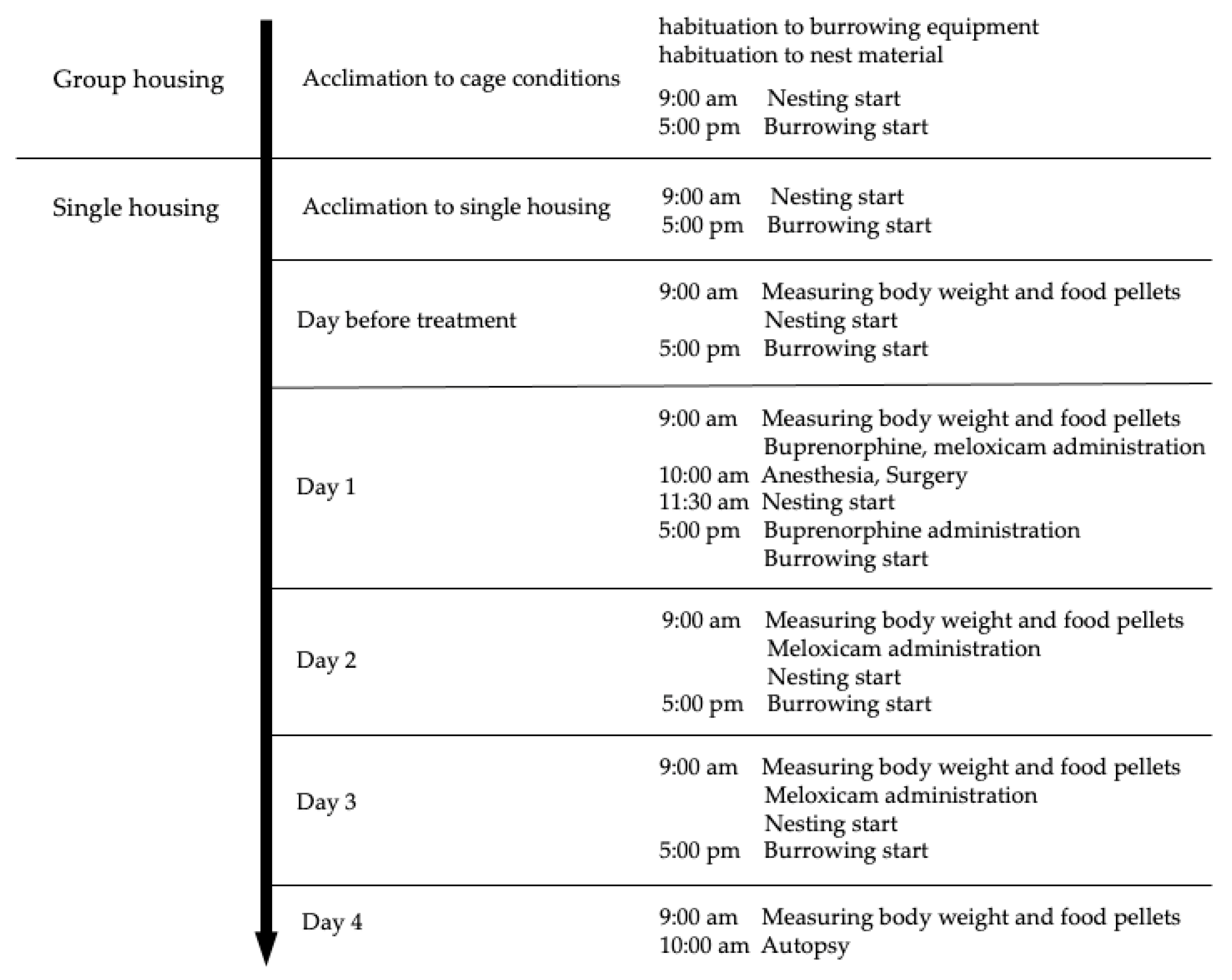
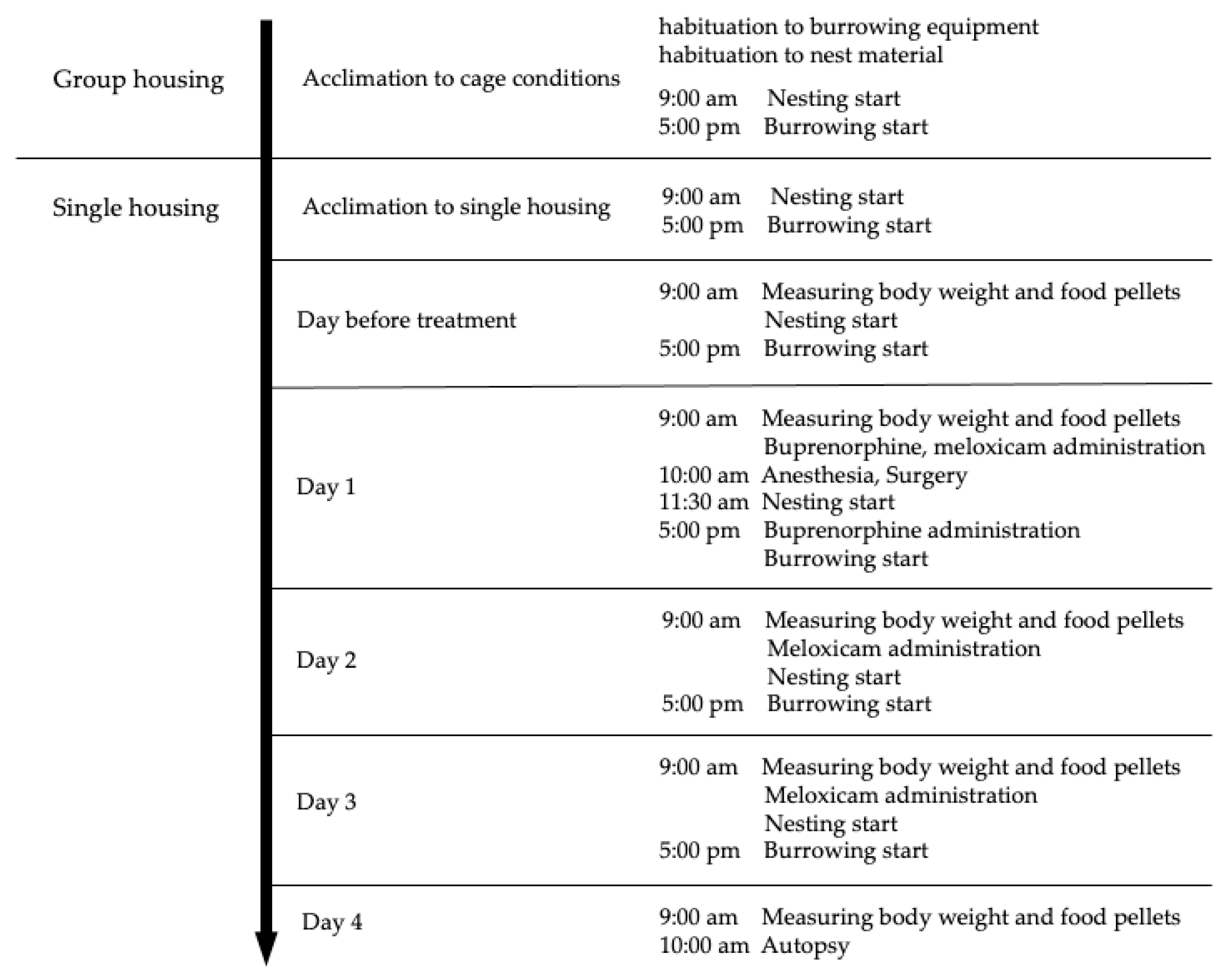
2.1. Animals and Experimental Setup
2.2. Surgery and Perioperative Care
2.3. Treatment Groups
2.4. Data Collection
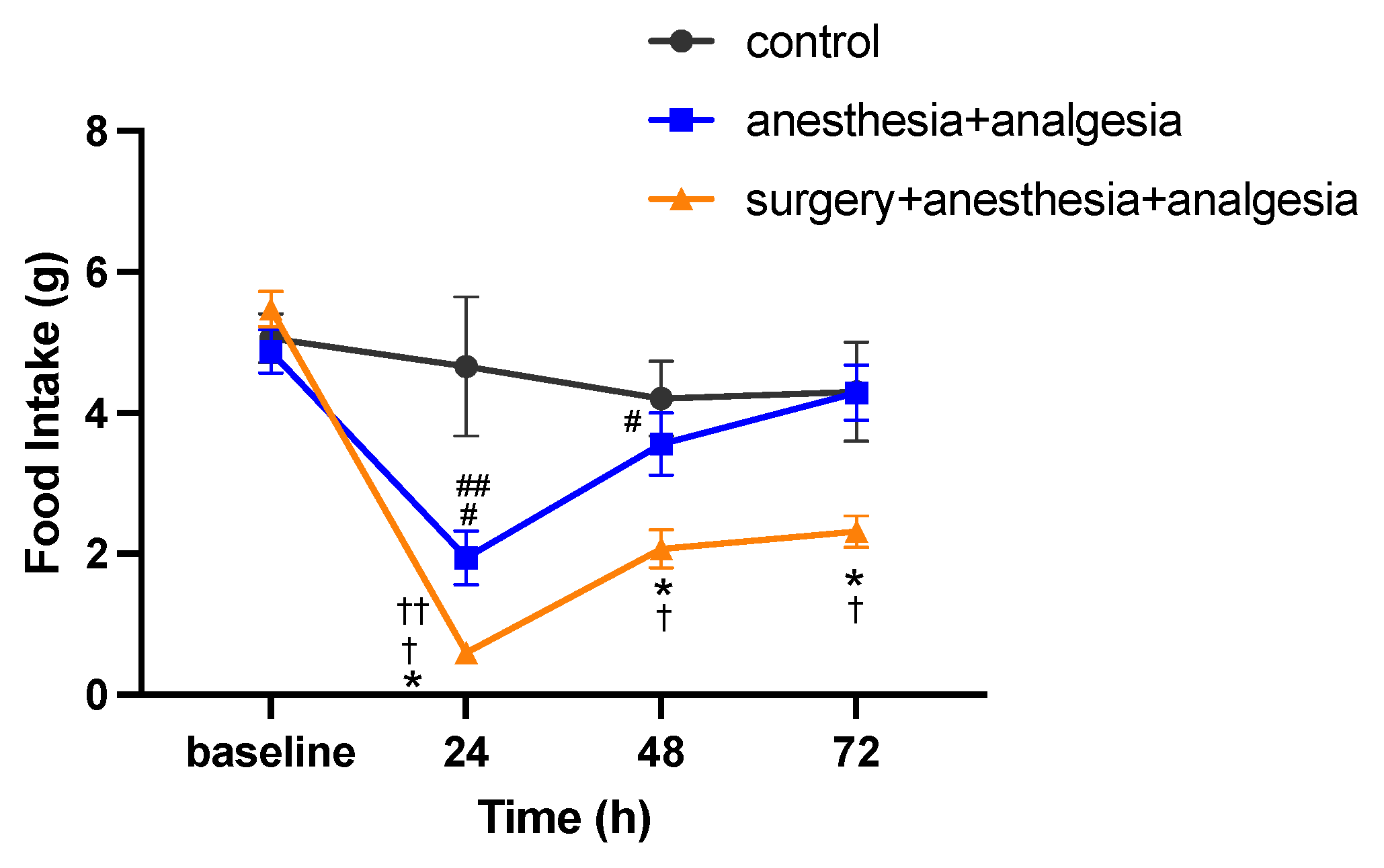
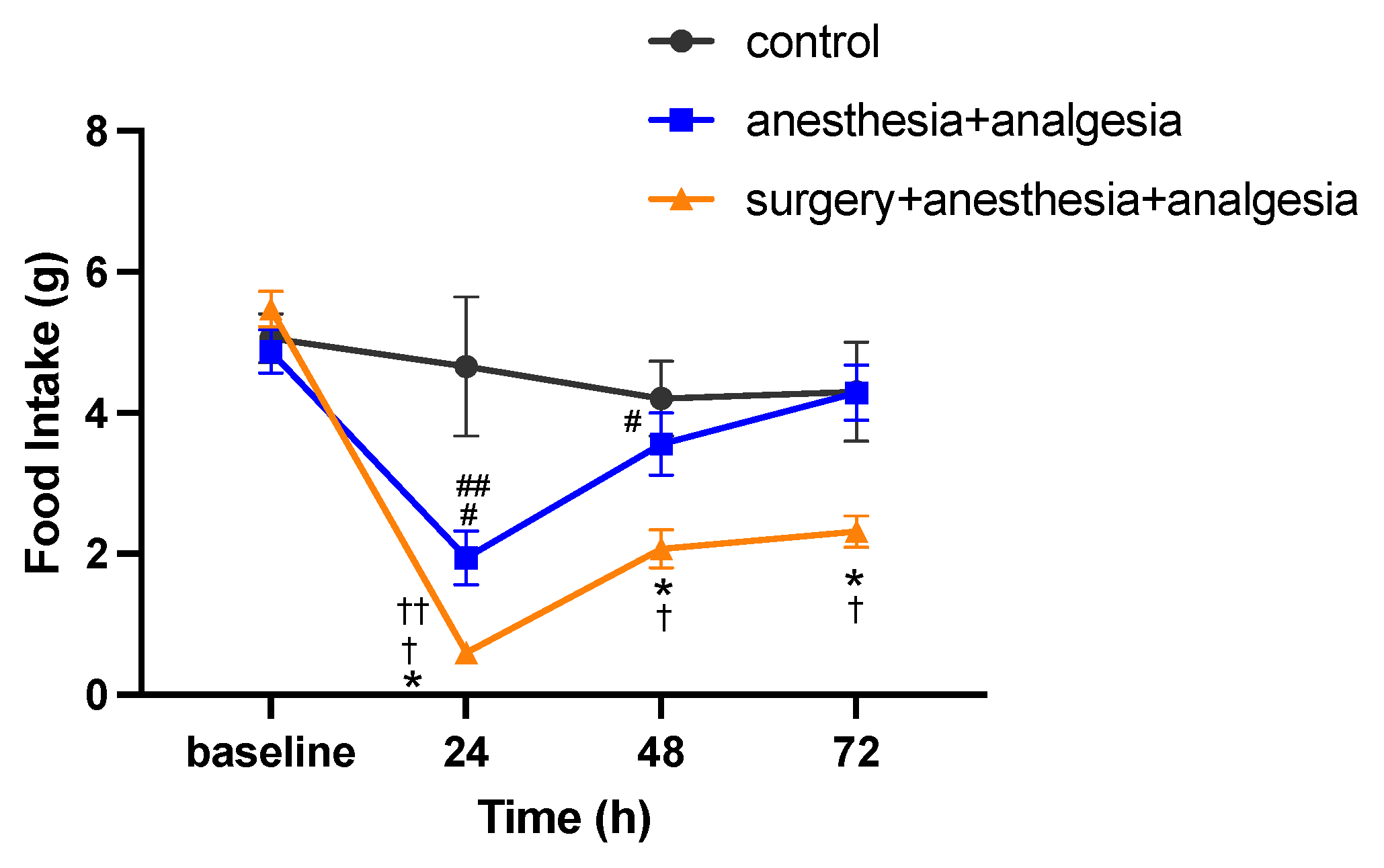
2.4.1. Food Intake
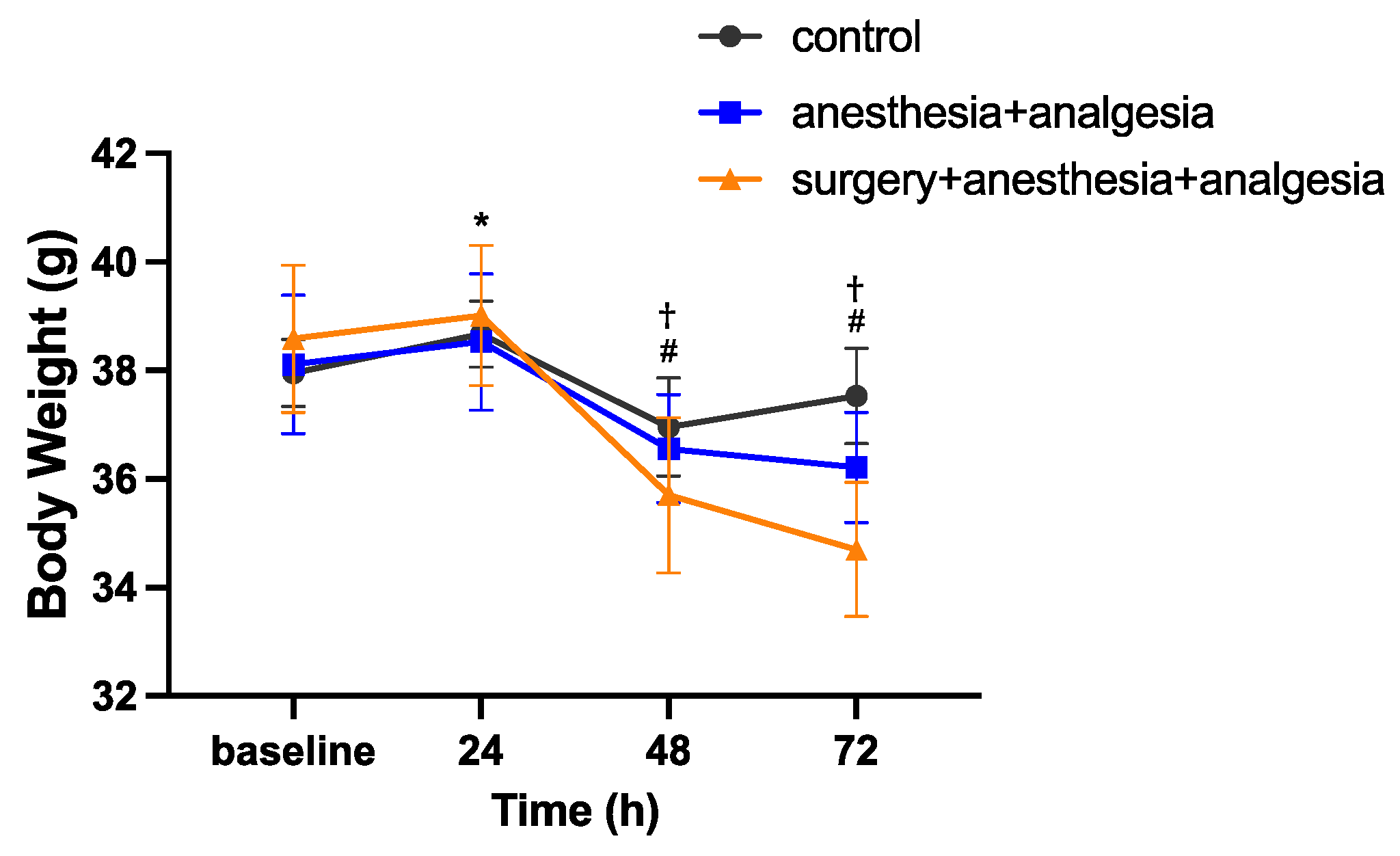
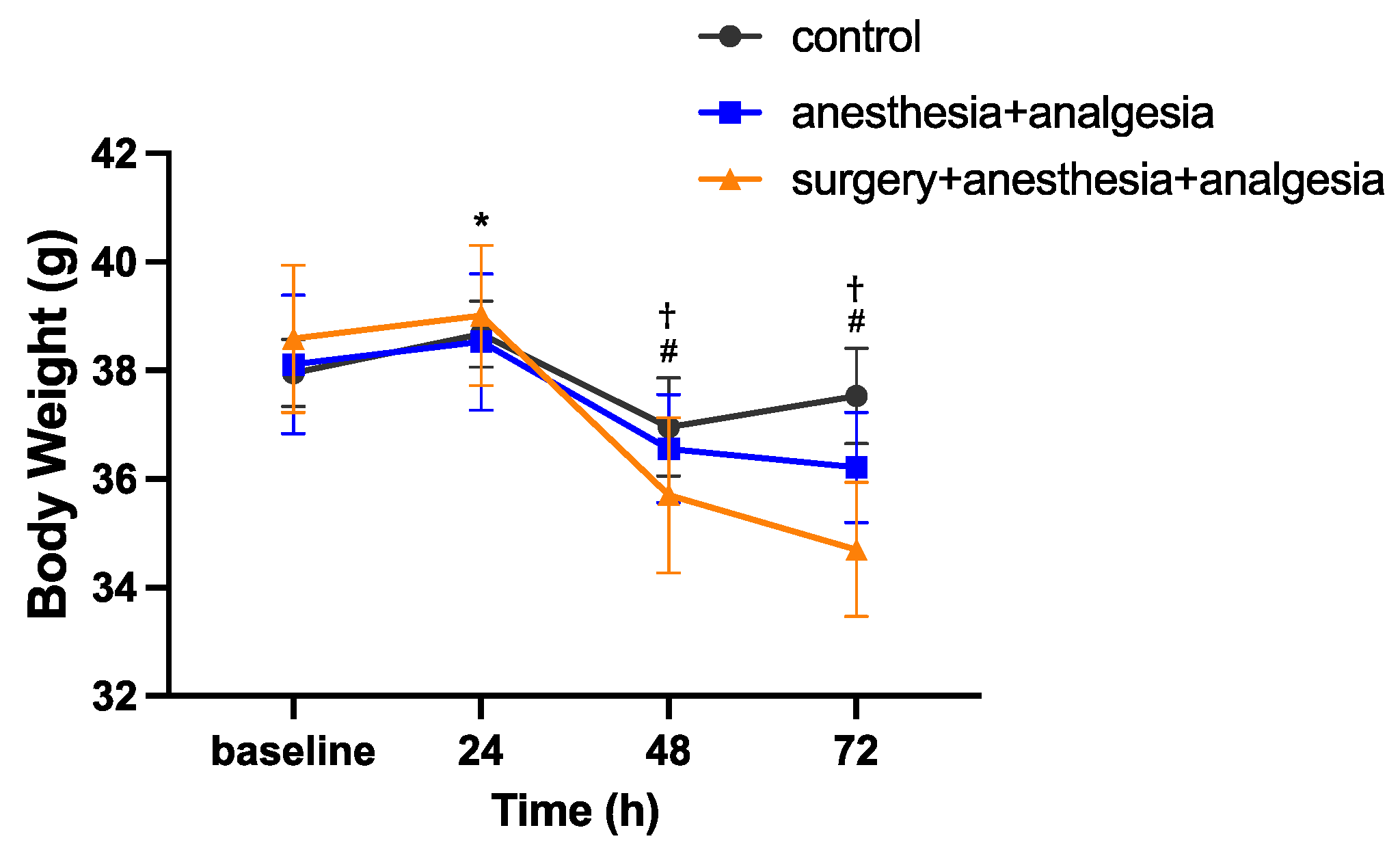
2.4.2. Body Weight
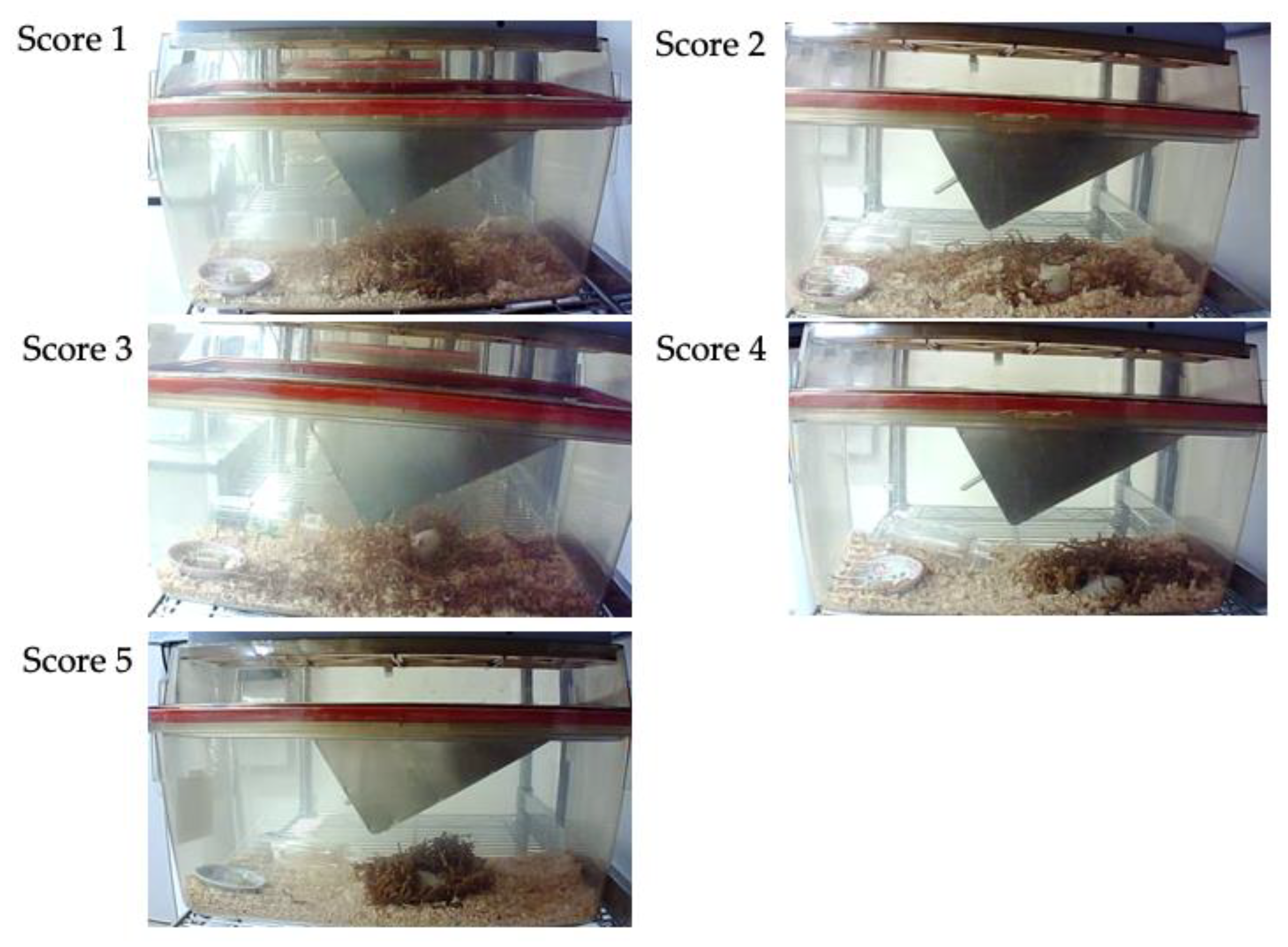
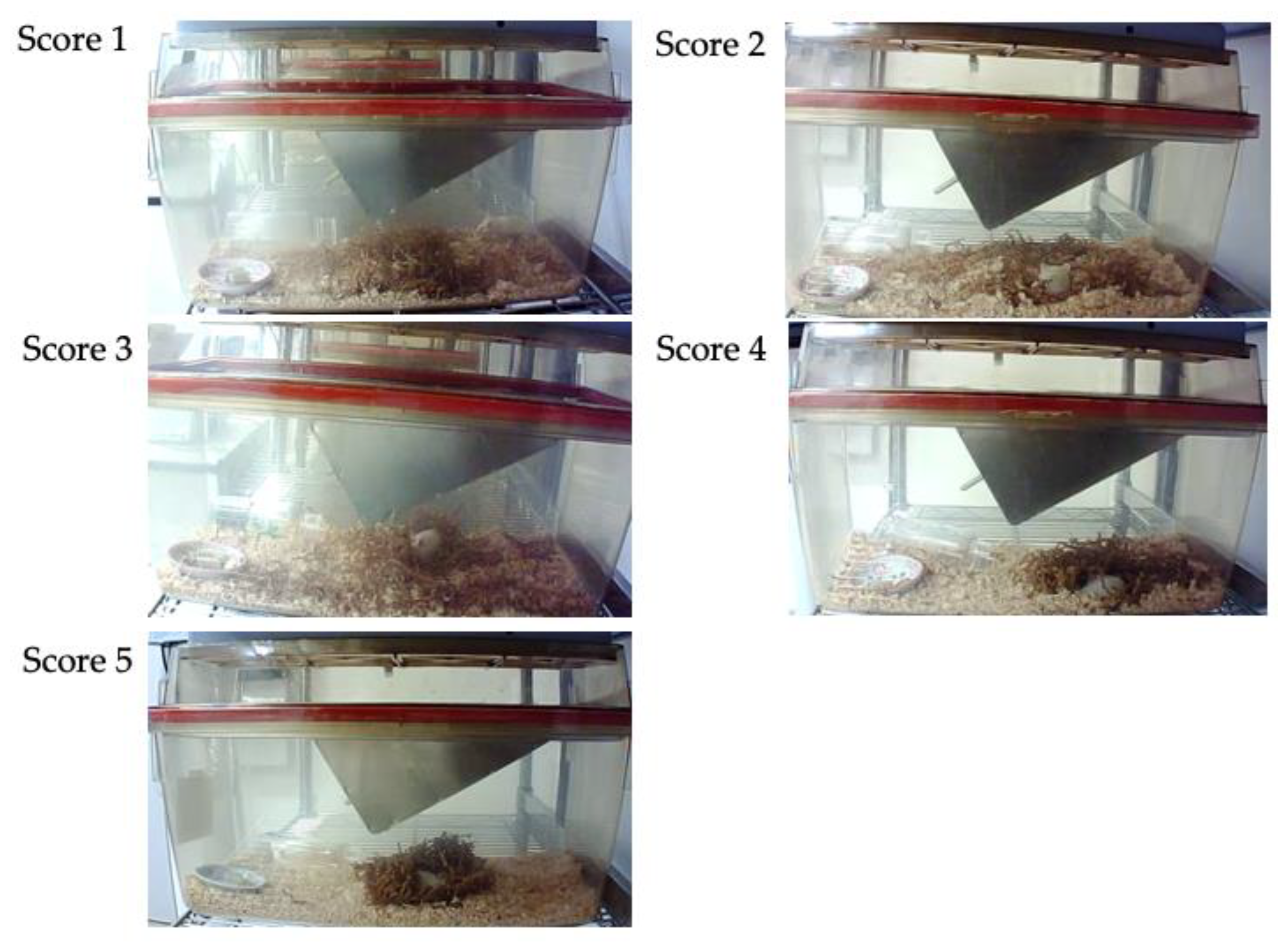
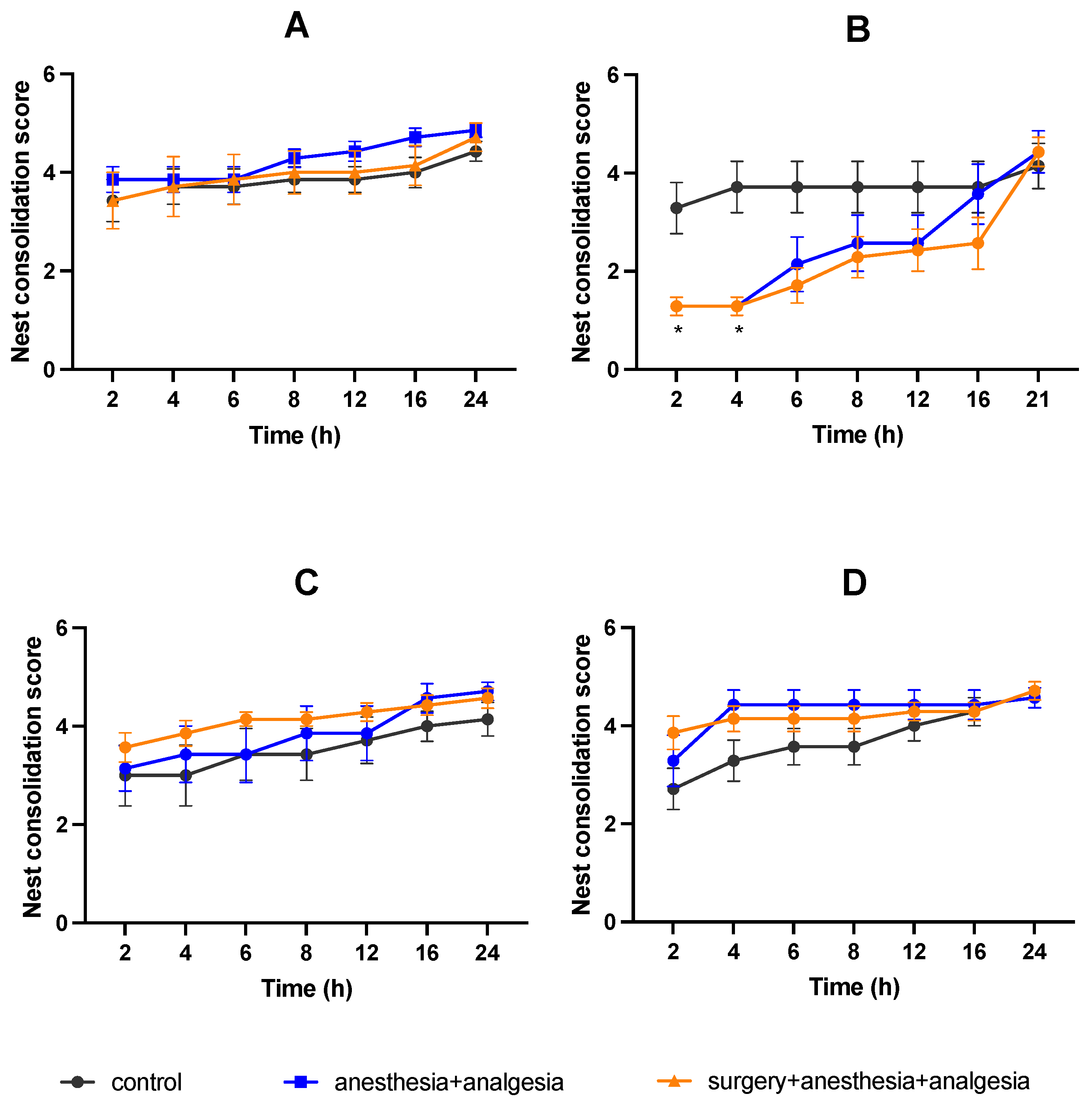
2.4.3. Nest Consolidating Behavior
2.4.4. Burrowing Behavior
2.4.5. Core Body Temperature
2.5. Histological Assessment of the Stomach and Duodenum
2.6. Statistical Analysis
3. Results
3.1. Changes in Food Intake
3.2. Changes in Body Weight
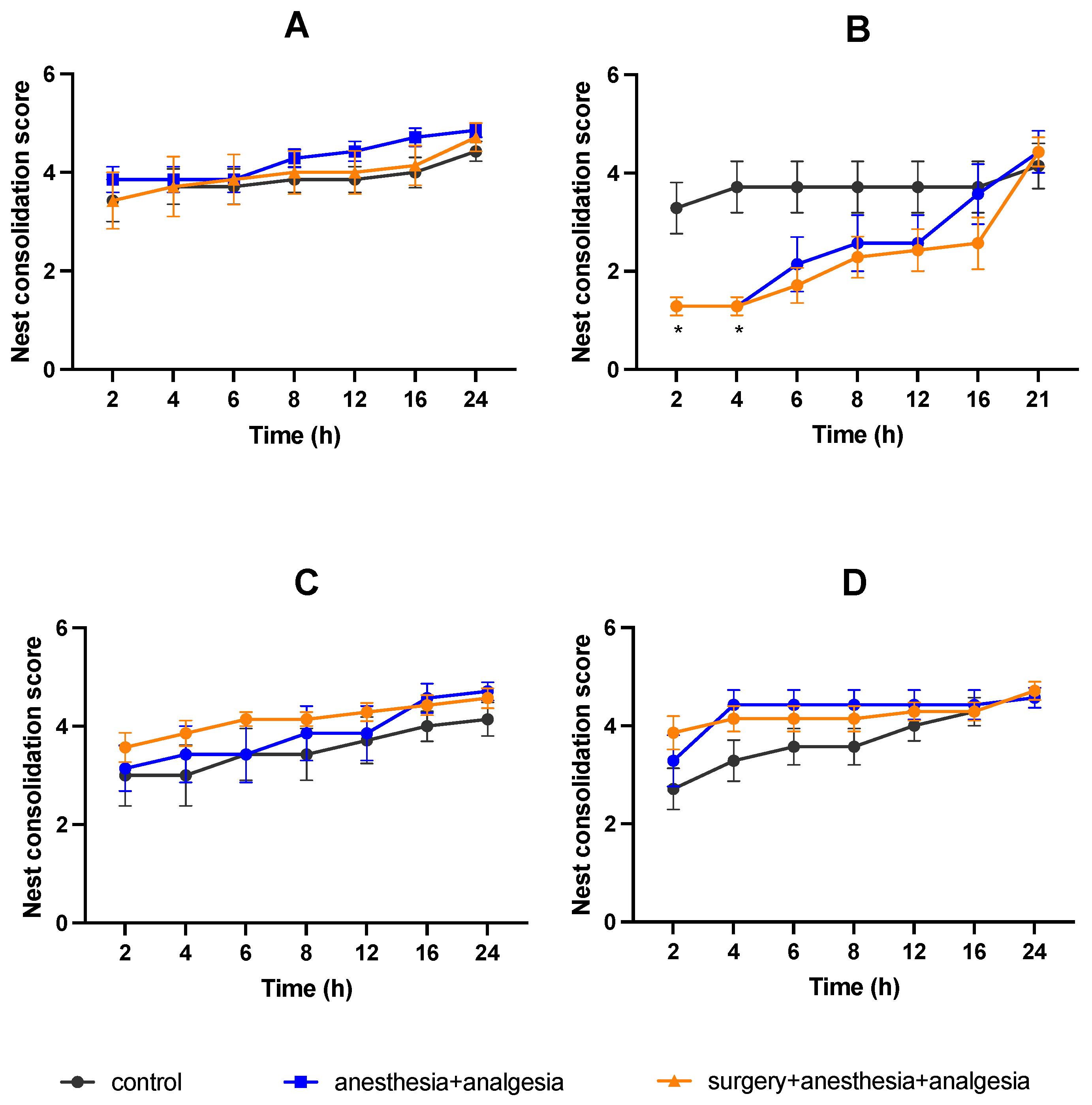
3.3. Nest Consolidating Behavior
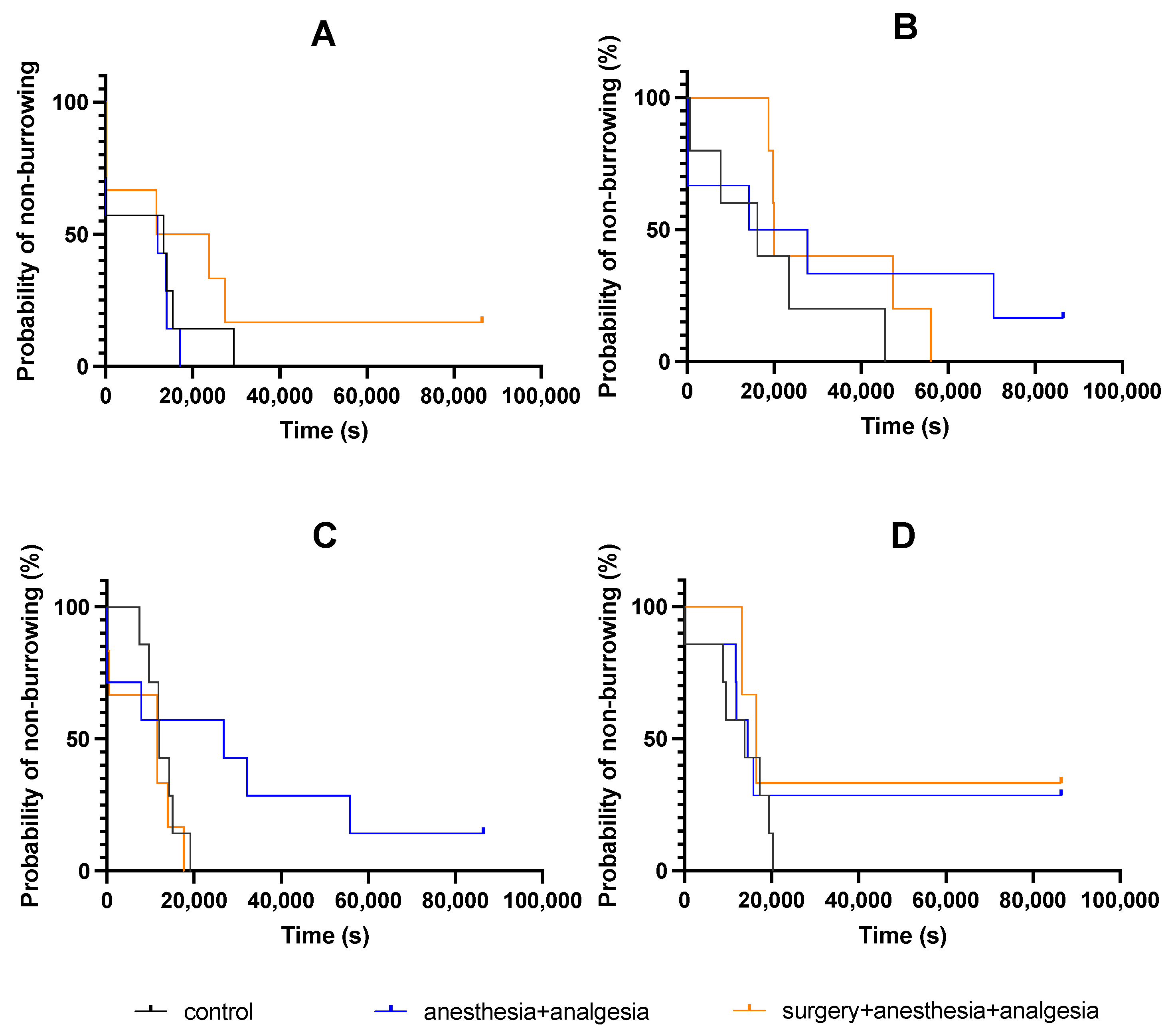
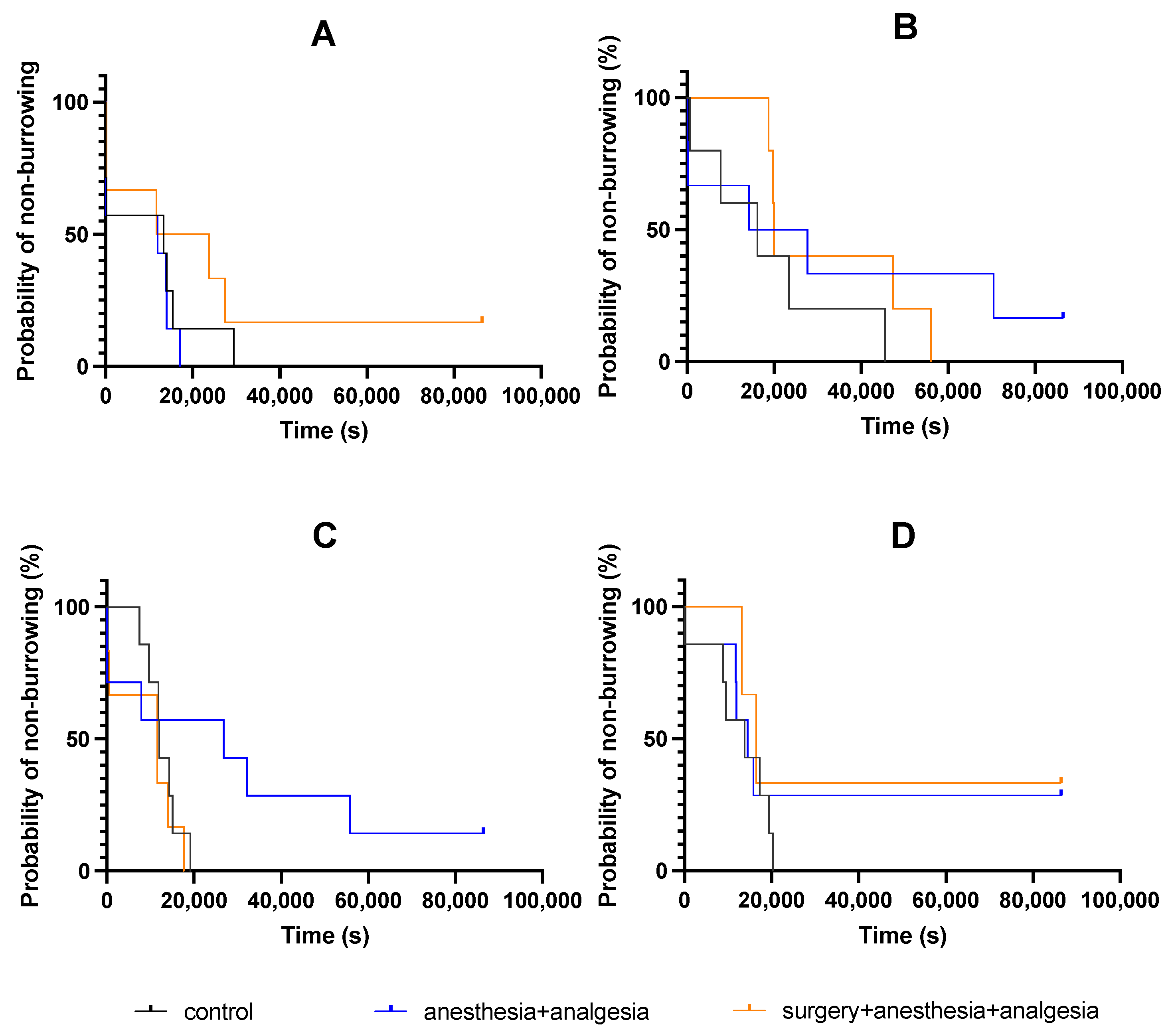
3.4. Burrowing Behavior
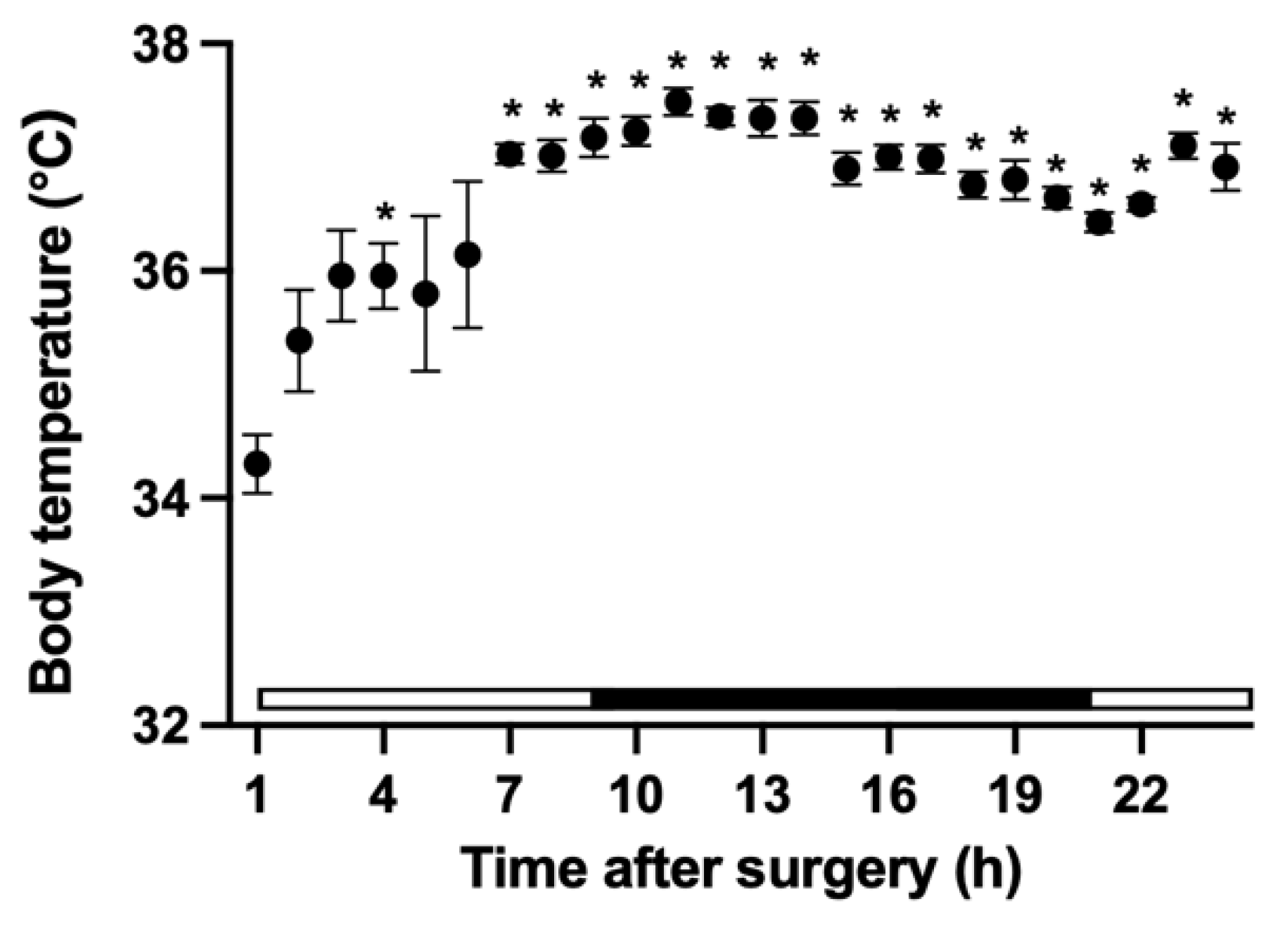
3.5. Changes in Core Body Temperature
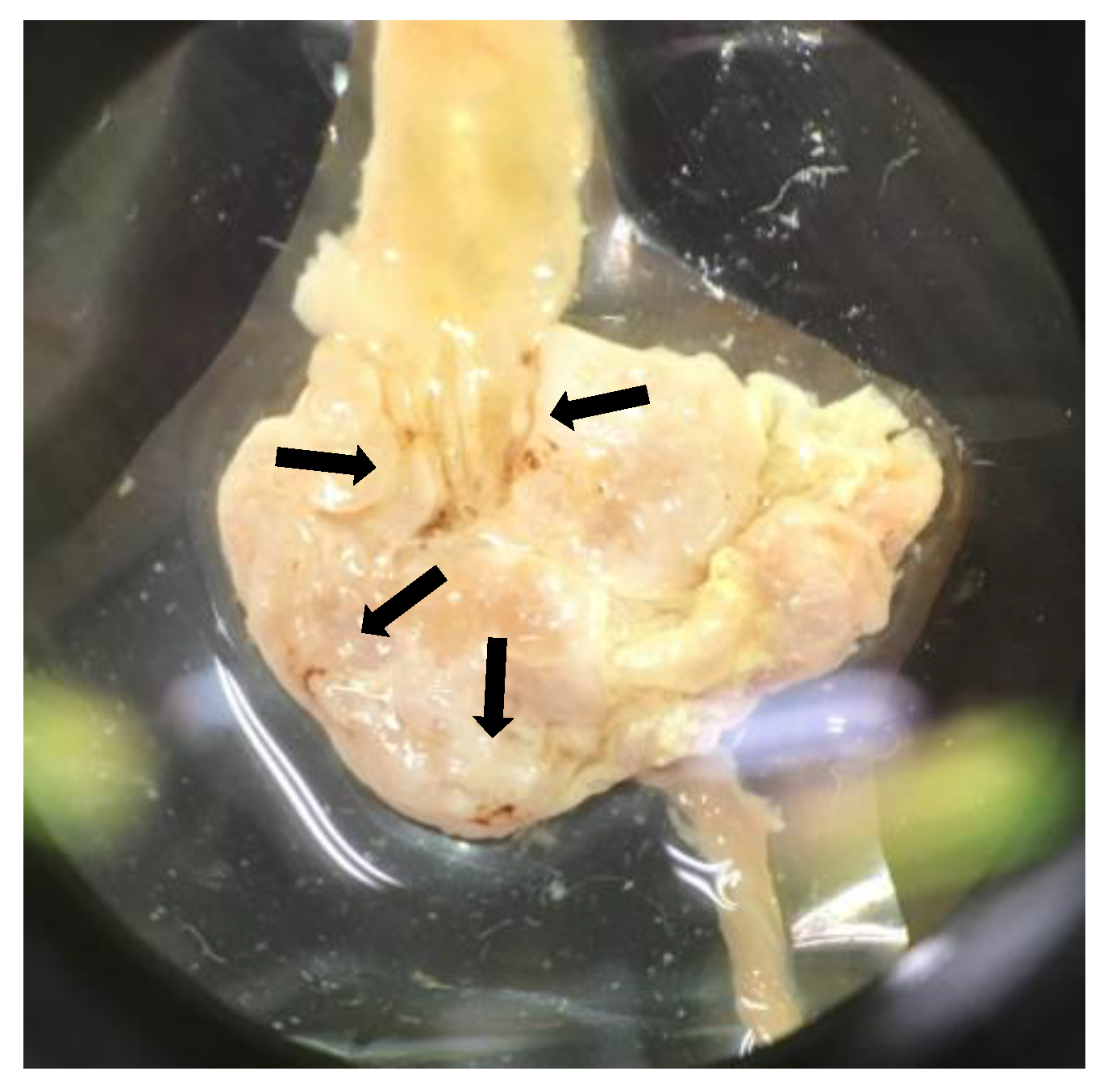
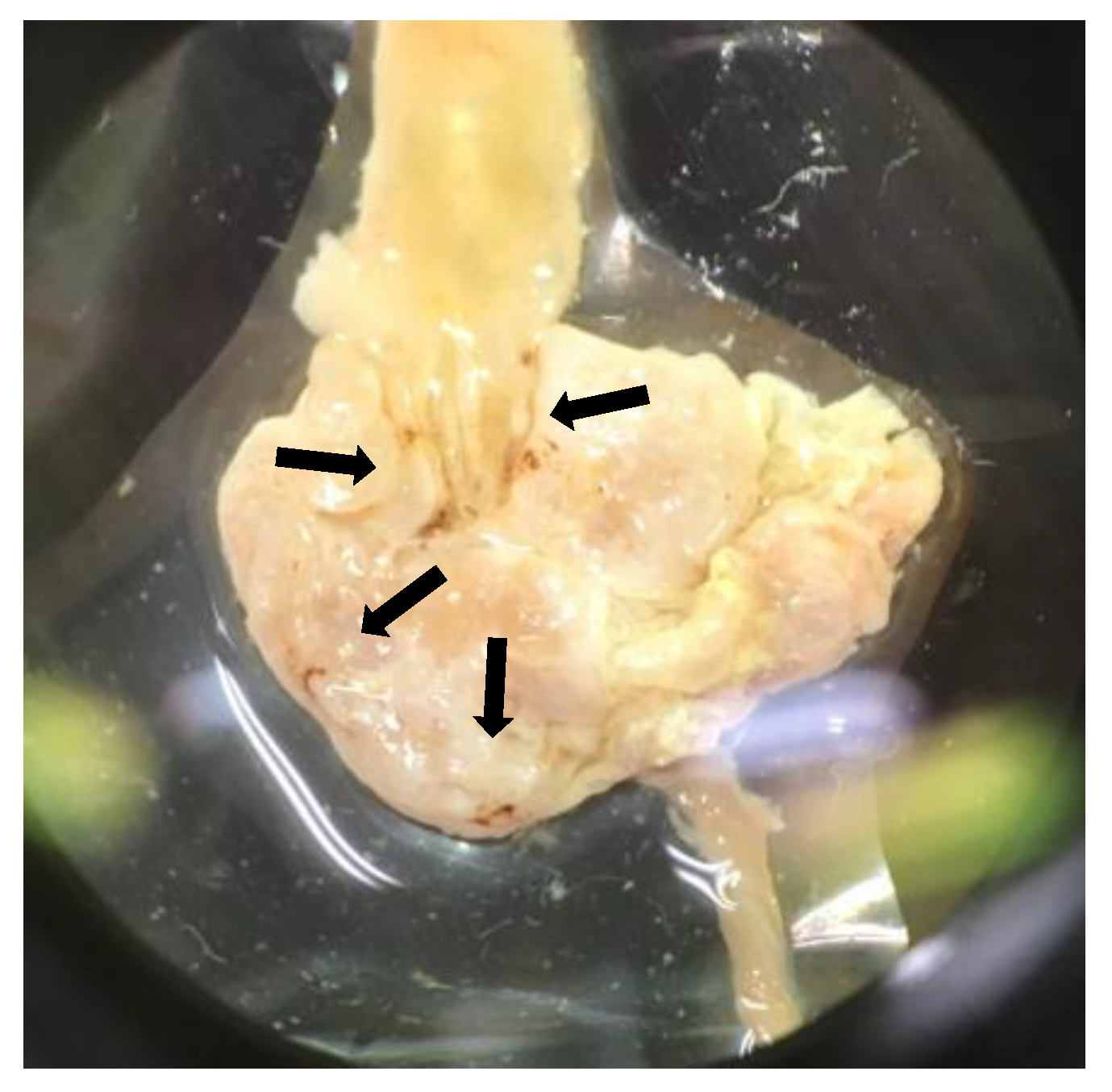
3.6. Autopsy Findings, and Histological Assessment of the Stomach and Duodenum
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Institute for Laboratory Animal Research. Veterinary Care. In Guide for the Care and Use of Laboratory Animals, 8th ed.; The National Academies Press: Washington, DC, USA, 2011; pp. 105–131. [Google Scholar]
- Jirkof, P. Side effects of pain and analgesia in animal experimentation. Lab. Anim. 2017, 46, 123–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellyer, P.W.; Robertson, S.A.; Fails, A.D. Pain and Its Management. In Veterinary Anesthesia and Analgesia, 4th ed.; Tranquilli, W.J., Thurmon, J.C., Grimm, K.A., Eds.; Blackwell Publishing: Ames, IA, USA, 2007; pp. 31–57. [Google Scholar]
- Dickinson, A.L.; Leach, M.C.; Flecknell, P.A. The analgesic effects of oral paracetamol in two strains of mice undergoing vasectomy. Lab. Anim. 2009, 43, 357–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver, V.L.; Thurston, S.E.; Lofgren, J.L. Using cageside measures to evaluate analgesic efficacy in mice (Mus musculus) after surgery. J. Am. Assoc. Lab. Anim. Sci. 2018, 57, 186–201. [Google Scholar]
- Beninson, J.A.; Lofgren, J.L.; Lester, P.A.; Hileman, M.M.; Berkowitz, D.J.; Myers, D.D. Analgesic efficacy and hematologic effects of robenacoxib in mice. J. Am. Assoc. Lab. Anim. Sci. 2018, 57, 258–267. [Google Scholar] [PubMed]
- Fernández-Dueñas, V.; Poveda, R.; Sánchez, S.; Ciruela, F. Synergistic interaction between fentanyl and a tramadol:Paracetamol combination on the inhibition of nociception in mice. J. Pharmacol. Sci. 2012, 118, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Farris, H.E. Effects of indomethacin and buprenorphine analgesia on the postoperative recovery of mice. J. Am. Assoc. Lab. Anim. Sci. 2008, 47, 8. [Google Scholar]
- Adamson, T.W.; Kendall, L.V.; Goss, S.; Grayson, K.; Tourna, C.; Palme, R.; Chen, J.Q.; Borowsky, A.D. Assessment of carprofen and buprenorphine on recovery of mice after surgical removal of the mammary fat pad. J. Am. Assoc. Lab. Anim. Sci. 2010, 49, 610–616. [Google Scholar]
- Tubbs, J.T.; Kissling, G.E.; Travlos, G.S.; Goulding, D.R.; Clark, J.A.; King-Herbert, A.P.; Blankenship-Paris, T.L. Effects of buprenorphine, meloxicam, and flunixin meglumine as postoperative analgesia in mice. J. Am. Assoc. Lab. Anim. Sci. 2011, 50, 185–191. [Google Scholar]
- Gaskill, B.N.; Karas, A.Z.; Garner, J.P.; Pritchett-Corning, K.R. Nest building as an indicator of health and welfare in laboratory mice. J. Vis. Exp. 2013, 82, 51012. [Google Scholar] [CrossRef] [Green Version]
- Jirkof, P. Burrowing and nest building behavior as indicators of well-being in mice. J. Neurosci. Methods 2014, 234, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Gjendal, K.; Ottesen, J.L.; Olsson, I.A.S.; Sørensen, D.B. Effect of Repeated Exposure to Isoflurane on Nest Building and Burrowing in Mice. J. Am. Assoc. Lab. Anim. Sci. 2020, 59, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Arras, M.; Rettich, A.; Cinelli, P.; Kasermann, H.P.; Burki, K. Assessment of post-laparotomy pain in laboratory mice by telemetric recording of heart rate and heart rate variability. BMC Vet. Res. 2007, 3, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jirkof, P.; Cesarovic, N.; Rettich, A.; Nicholls, F.; Seifert, B.; Arras, M. Burrowing behavior as an indicator of post-laparotomy pain in mice. Front. Behav. Neurosci. 2010, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deacon, R. Assessing burrowing, nest construction, and hoarding in mice. J. Vis. Exp. 2012, 59, 2607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryden, L.A.; Nicholson, J.R.; Doods, H.; Pekcec, A. Deficits in spontaneous burrowing behavior in the rat bilateral monosodium iodoacetate model of osteoarthritis: An objective measure of pain-related behavior and analgesic efficacy. Osteoarthr. Cartil. 2015, 23, 1605–1612. [Google Scholar] [CrossRef] [Green Version]
- Okayama, T.; Goto, T.; Toyoda, A. Assessing nest-building behavior of mice using a 3D depth camera. J. Neurosci. Methods 2015, 251, 151–157. [Google Scholar] [CrossRef]
- Hess, S.E.; Rohr, S.; Dufour, B.D.; Gaskill, B.N.; Pajor, E.A.; Garner, J.P. Home improvement: C57BL/6J mice given more naturalistic nesting materials build better nests. J. Am. Assoc. Lab. Anim. Sci. 2008, 47, 25–31. [Google Scholar]
- Jirkof, P.; Cesarovic, N.; Rettich, A.; Fleischmann, T.; Arras, M. Individual housing of female mice: Influence on postsurgical behaviour and recovery. Lab. Anim. 2012, 46, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Jirkof, P.; Tourvieille, A.; Cinelli, P.; Arras, M. Buprenorphine for pain relief in mice: Repeated injections vs sustained-release depot formulation. Lab. Anim. 2015, 49, 177–187. [Google Scholar] [CrossRef]
- Roughan, J.V.; Flecknell, P.A. Buprenorphine: A reappraisal of its antinociceptive effects and therapeutic use in alleviating post-operative pain in animals. Lab. Anim. 2002, 36, 322–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goecke, J.C.; Awad, H.; Lawson, J.C.; Boivin, G.P. Evaluating postoperative analgesics in mice using telemetry. Comp. Med. 2005, 55, 37–44. [Google Scholar] [PubMed]
- Kendall, L.V.; Wegenast, D.J.; Smith, B.J.; Dorsey, K.M.; Kang, S.; Lee, N.Y.; Hess, A.M. Efficacy of sustained-release buprenorphine in an experimental laparotomy model in female mice. J. Am. Assoc. Lab. Anim. Sci. 2016, 55, 66–73. [Google Scholar] [PubMed]
- Wright-Williams, S.L.; Courade, J.P.; Richardson, C.A.; Roughan, J.V.; Flecknell, P.A. Effects of vasectomy surgery and meloxicam treatment on faecal corticosterone levels and behaviour in two strains of laboratory mouse. Pain 2007, 130, 108–118. [Google Scholar] [CrossRef]
- Hohlbaum, K.; Bert, B.; Dietze, S.; Palme, R.; Fink, H.; Thöne-Reineke, C. Severity classification of repeated isoflurane anesthesia in C57BL/6JRj mice-Assessing the degree of distress. PLoS ONE 2017, 12, 1–21. [Google Scholar] [CrossRef]
- Sarfaty, A.E.; Zeiss, C.J.; Willis, A.D.; Harris, J.M.; Smith, P.C. Concentration-dependent toxicity after subcutaneous administration of meloxicam to C57BL/6N mice (Mus musculus). J. Am. Assoc. Lab. Anim. Sci. 2018, 58, 802–809. [Google Scholar] [CrossRef]
- Parker, J.M.; Austin, J.; Wilkerson, J.; Carbone, L. Effects of multimodal analgesia on the success of mouse embryo transfer surgery. J. Am. Assoc. Lab. Anim. Sci. 2011, 50, 466–470. [Google Scholar]
- Miranda, H.F.; Pinardi, G. Lack of effect of naltrindole on the spinal synergism of morphine and non-steroidal anti-inflammatory drugs (NSAIDS). J. Physiol. Pharmacol. 2009, 60, 71–76. [Google Scholar]
- Le, A.H.; Bonachea, L.A.; Cargill, S.L. Meloxicam and buprenorphine treatment after ovarian transplantation does not affect estrous cyclicity and follicular integrity in aged CBA/J mice. PLoS ONE 2014, 9, e106013. [Google Scholar] [CrossRef]
- Matsumiya, L.C.; Sorge, R.E.; Sotocinal, S.G.; Tabaka, J.M.; Wieskopf, J.S.; Zaloum, A.; King, O.D.; Mogil, J.S. Using the mouse grimace scale to reevaluate the efficacy of postoperative analgesics in laboratory mice. J. Am. Assoc. Lab. Anim. Sci. 2012, 51, 42–49. [Google Scholar]
- Pham, T.M.; Hagman, B.; Codita, A.; Van Loo, P.L.P.; Strömmer, L.; Baumans, V. Housing environment influences the need for pain relief during post-operative recovery in mice. Physiol. Behav. 2010, 99, 663–668. [Google Scholar] [CrossRef]
- Van Loo, P.L.P.; Kuin, N.; Sommer, R.; Avsaroglu, H.; Pham, T.; Baumans, V. Impact of “living apart together” on postoperative recovery of mice compared with social and individual housing. Lab. Anim. 2007, 41, 441–455. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Control | Anesthesia + Analgesia | Anesthesia + Analgesia + Surgery | |
|---|---|---|---|---|
| Day 1 | Medetomidine | Water for injection (IP) | 0.2 mg/kg (IP) | 0.2 mg/kg (IP) |
| Atipamezole | Water for injection (IP) | 1 mg/kg (IP) | 1 mg/kg (IP) | |
| Isoflurane | – | 1.5–2.5% | 1.5–2.5% | |
| Buprenorphine | Water for injection | 0.1 mg/kg (SC) 2 times | 0.1 mg/kg (SC) 2 times | |
| Meloxicam | Water (PO) | 5 mg/kg (PO) | 5 mg/kg (PO) | |
| Bupivacaine | – | – | 0.5% (drop) | |
| Day 2 | Meloxicam | Water for injection (IP) | 5 mg/kg (PO) | 5 mg/kg (PO) |
| Day 3 | Meloxicam | Water for injection (IP) | 5 mg/kg (PO) | 5 mg/kg (PO) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furumoto, K.; Ogita, K.; Kamisaka, T.; Kawasumi, A.; Takata, K.; Maeta, N.; Itoi, T.; Nohara, M.; Saeki, K.; Kanda, T. Effects of Multimodal Analgesic Protocol, with Buprenorphine and Meloxicam, on Mice Well-Being: A Dose Finding Study. Animals 2021, 11, 3420. https://doi.org/10.3390/ani11123420
Furumoto K, Ogita K, Kamisaka T, Kawasumi A, Takata K, Maeta N, Itoi T, Nohara M, Saeki K, Kanda T. Effects of Multimodal Analgesic Protocol, with Buprenorphine and Meloxicam, on Mice Well-Being: A Dose Finding Study. Animals. 2021; 11(12):3420. https://doi.org/10.3390/ani11123420
Chicago/Turabian StyleFurumoto, Kayo, Kumi Ogita, Tomomi Kamisaka, Asami Kawasumi, Koushi Takata, Noritaka Maeta, Takamasa Itoi, Masakatsu Nohara, Kaori Saeki, and Teppei Kanda. 2021. "Effects of Multimodal Analgesic Protocol, with Buprenorphine and Meloxicam, on Mice Well-Being: A Dose Finding Study" Animals 11, no. 12: 3420. https://doi.org/10.3390/ani11123420
APA StyleFurumoto, K., Ogita, K., Kamisaka, T., Kawasumi, A., Takata, K., Maeta, N., Itoi, T., Nohara, M., Saeki, K., & Kanda, T. (2021). Effects of Multimodal Analgesic Protocol, with Buprenorphine and Meloxicam, on Mice Well-Being: A Dose Finding Study. Animals, 11(12), 3420. https://doi.org/10.3390/ani11123420