
The Epidemiology of Meningitis in Infants under 90 Days of Age in a Large Pediatric Hospital


 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
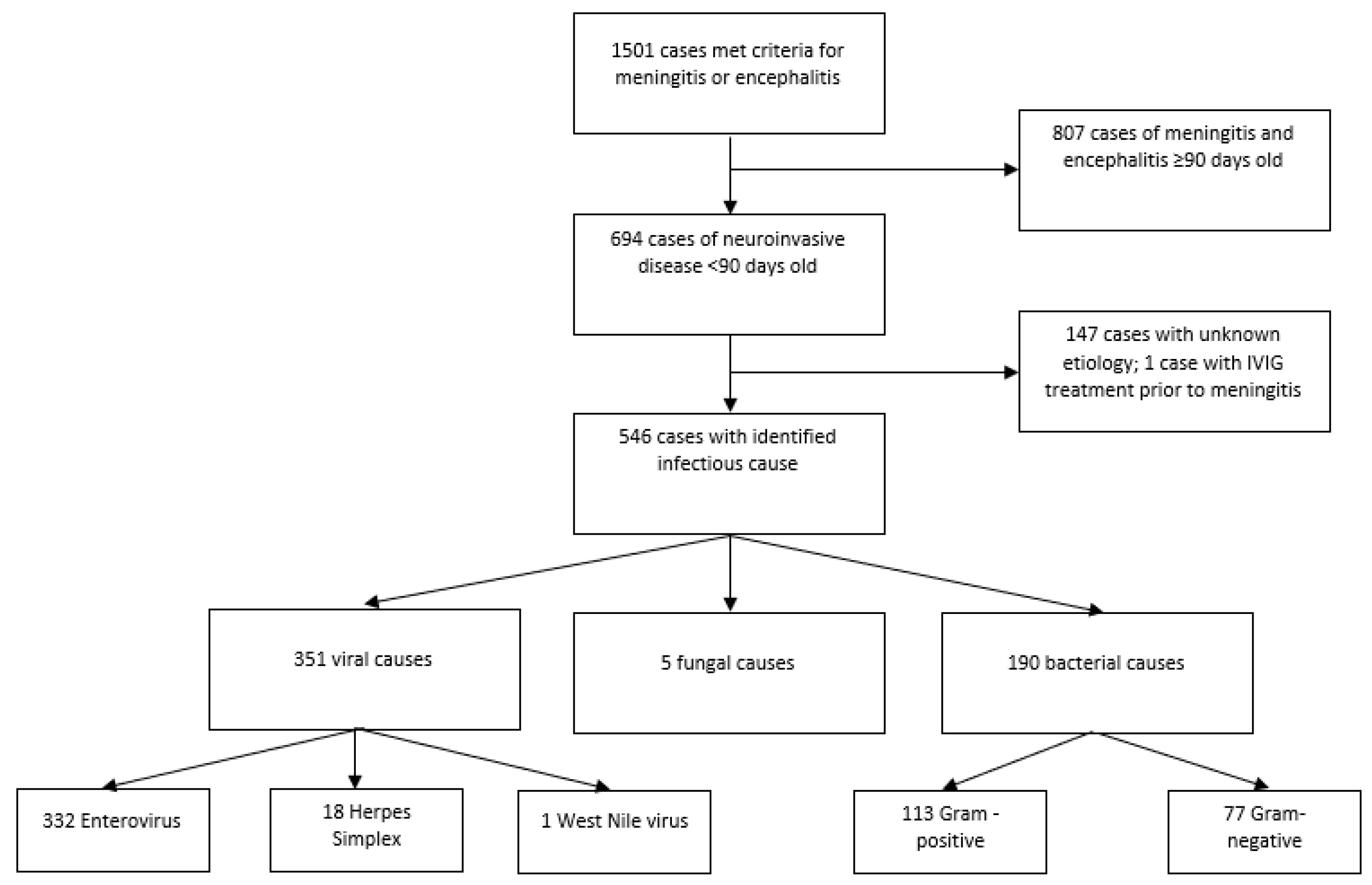
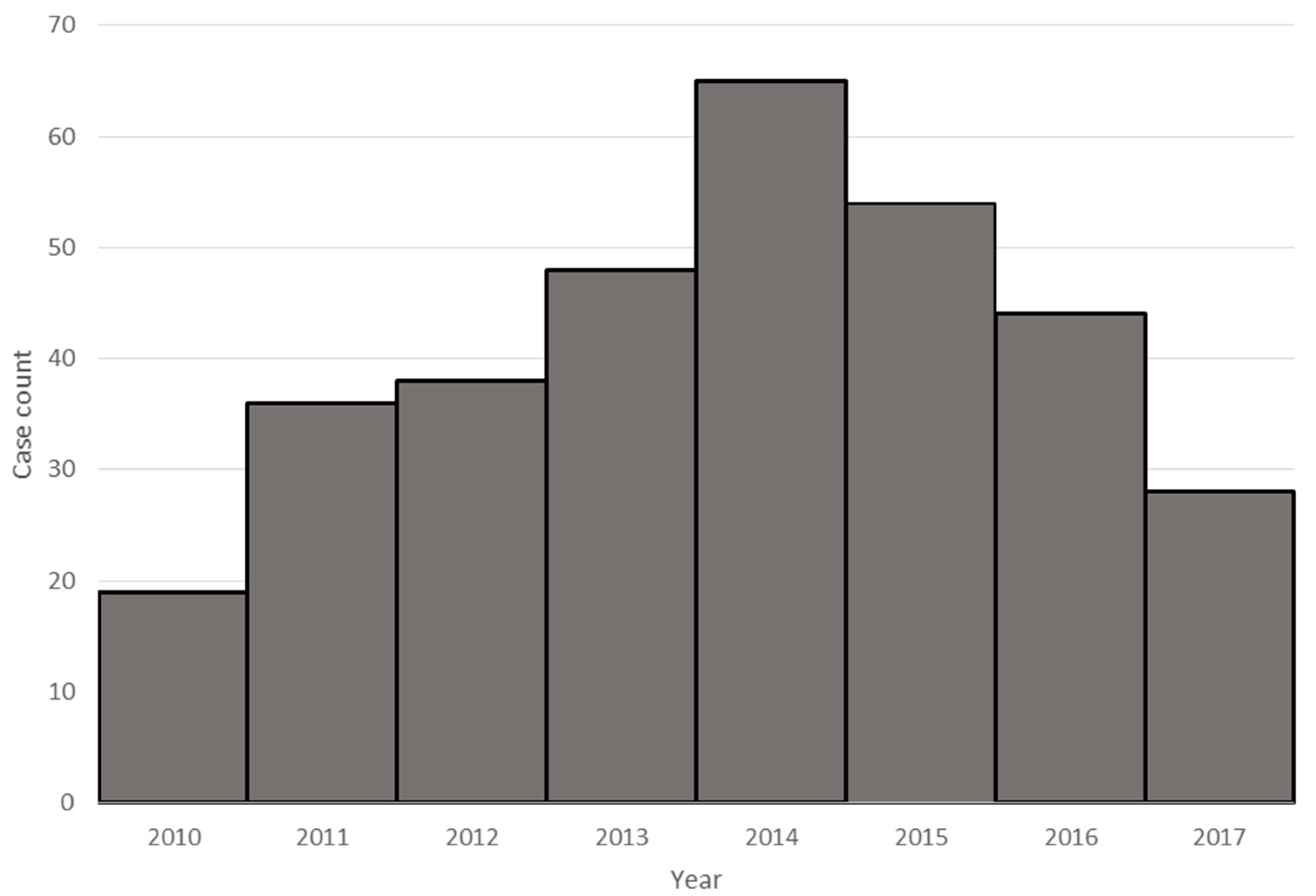
3. Results
3.1. Viral Infections
3.2. Group B Streptococcus
3.3. Escherichia coli
3.4. Gram-Negative Organisms Other Than E. coli
3.5. Gram-Positive Organisms Other Than GBS and Fungi
3.6. Antimicrobial Resistance
3.7. Risk Factors for Meningitis
3.8. Fatal Cases
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hasbun, R.; Wootton, S.H.; Rosenthal, N.; Balada-Llasat, J.M.; Chung, J.; Duff, S.; Bozzette, S.; Zimmer, L.; Ginocchio, C.C. Epidemiology of Meningitis and Encephalitis in Infants and Children in the United States, 2011–2014. Pediatr. Infect. Dis. J. 2019, 38, 37–41. [Google Scholar] [CrossRef]
- Cherry, J.D.; Demmler-Harrison, G.; Kaplan, S.L.; Steinbach, W.J.; Hotez, P.J. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases, 7th ed.; Saunders/Elsevier: Philadelphia, PA, USA, 2014. [Google Scholar]
- Rotbart, H.A. Enteroviral Infections of the Central Nervous System. Clin. Infect. Dis. 1995, 20, 971–981. [Google Scholar] [CrossRef]
- Lee, B.E.; Dele Davies, H. Aseptic meningitis. Curr. Opin. Infect. Dis. 2007, 20, 272–277. [Google Scholar] [CrossRef]
- Murphy, T.V.; White, K.E.; Pastor, P.; Gabriel, L.; Medley, F.; Granoff, D.M.; Osterholm, M.T. Declining incidence of Haemophilus influenzae type b disease since introduction of vaccination. JAMA 1993, 269, 246–248. [Google Scholar] [CrossRef] [PubMed]
- Thigpen, M.C.; Whitney, C.G.; Messonnier, N.E.; Zell, E.R.; Lynfield, R.; Hadler, J.L.; Harrison, L.H.; Farley, M.M.; Reingold, A.; Bennett, N.M.; et al. Bacterial Meningitis in the United States, 1998–2007. N. Engl. J. Med. 2011, 364, 2016–2025. [Google Scholar] [CrossRef]
- Gaschignard, J.; Levy, C.; Romain, O.; Cohen, R.; Bingen, E.; Aujard, Y.; Boileau, P. Neonatal Bacterial Meningitis: 444 Cases in 7 Years. Pediatr. Infect. Dis. J. 2011, 30, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Okike, I.O.; Johnson, A.P.; Henderson, K.L.; Blackburn, R.M.; Muller-Pebody, B.; Ladhani, S.N.; Anthony, M.; Ninis, N.; Heath, P.T. Incidence, etiology, and outcome of bacterial meningitis in infants aged <90 days in the United kingdom and Republic of Ireland: Prospective, enhanced, national population-based surveillance. Clin. Infect. Dis. 2014, 59, e150–e157. [Google Scholar] [CrossRef] [PubMed]
- Ouchenir, L.; Renaud, C.; Khan, S.; Bitnun, A.; Boisvert, A.-A.; McDonald, J.; Bowes, J.; Brophy, J.; Barton, M.; Ting, J.; et al. The Epidemiology, Management, and Outcomes of Bacterial Meningitis in Infants. Pediatrics 2017, 140, e20170476. [Google Scholar] [CrossRef]
- MacNeil, J.R.; Cohn, A.C.; Farley, M.; Mair, R.; Baumbach, J.; Bennett, N.; Gershman, K.; Harrison, L.H.; Lynfield, R.; Petit, S.; et al. Current Epidemiology and Trends in Invasive Haemophilus influenzae Disease—United States, 1989–2008. Clin. Infect. Dis. 2011, 53, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Verani, J.R.; McGee, L.; Schrag, S.J. Prevention of perinatal group B streptococcal disease—Revised guidelines from CDC, 2010. MMWR. Recomm. Rep. 2010, 59, 1–36. [Google Scholar]
- Collignon, P. Resistant Escherichia coli—We are what we eat. Clin. Infect. Dis. 2009, 49, 202–204. [Google Scholar] [CrossRef]
- Chambers, H.F.; DeLeo, F.R. Waves of resistance: Staphylococcus aureus in the antibiotic era. Nat. Rev. Genet. 2009, 7, 629–641. [Google Scholar] [CrossRef]
- CDC/NHSN Surveillance Definitions for Specific Types of Infections; National Healthcare Safety Network: Atlanta, GA, USA, 2018.
- Arboviral Encephalitis or Meningitis 2001 Case Definition. Available online: https://wwwn.cdc.gov/nndss/conditions/arboviral-encephalitis-or-meningitis/case-definition/2001/ (accessed on 10 January 2021).
- Bharath, V.; Eckert, K.; Kang, M.; Chin-Yee, I.H.; Hsia, C.C. Incidence and natural history of intravenous immunoglobulin-induced aseptic meningitis: A retrospective review at a single tertiary care center. Transfusion 2015, 55, 2597–2605. [Google Scholar] [CrossRef] [PubMed]
- Beneteau, A.; Levy, C.; Foucaud, P.; Béchet, S.; Cohen, R.; Raymond, J.; Dommergues, M.-A. Childhood meningitis caused by Streptococcus bovis group: Clinical and biologic data during a 12-year period in France. Pediatr. Infect. Dis. J. 2015, 34, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, M.K.; Phares, C.R.; Lynfield, R.; Thomas, A.R.; Arnold, K.E.; Craig, A.S.; Mohle-Boetani, J.; Gershman, K.; Schaffner, W.; Petit, S.; et al. Evaluation of Universal Antenatal Screening for Group B Streptococcus. N. Engl. J. Med. 2009, 360, 2626–2636. [Google Scholar] [CrossRef] [PubMed]
- Perinatal group B streptococcal disease after universal screening recommendations—United States, 2003–2005. In Morbidity and Mortality Weekly Report; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2007; pp. 701–705.
- Jawa, G.; Hussain, Z.; Da Silva, O. Recurrent Late-Onset Group B Streptococcus Sepsis in a Preterm Infant Acquired by Expressed Breastmilk Transmission: A Case Report. Breastfeed. Med. 2013, 8, 134–136. [Google Scholar] [CrossRef]
- Zimmermann, P.; Gwee, A.; Curtis, N. The controversial role of breast milk in GBS late-onset disease. J. Infect. 2017, 74, S34–S40. [Google Scholar] [CrossRef]
- Seale, A.C.; Bianchi-Jassir, F.; Russell, N.J.; Kohli-Lynch, M.; Tann, C.J.; Hall, J.; Madrid, L.; Blencowe, H.; Cousens, S.; Baker, C.J.; et al. Estimates of the Burden of Group B Streptococcal Disease Worldwide for Pregnant Women, Stillbirths, and Children. Clin. Infect. Dis. 2017, 65 (Suppl. 2), S200–S219. [Google Scholar] [CrossRef]
- Spiel, M.H.; Hacker, M.R.; Haviland, M.J.; Mulla, B.; Roberts, E.; Dodge, L.E.; Young, B.C. Racial disparities in intrapartum group B Streptococcus colonization: A higher incidence of conversion in African American women. J. Perinatol. 2019, 39, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Newton, E.R.; Butler, M.C.; Shain, R.N. Sexual behavior and vaginal colonization by group B streptococcus among minority women. Obstet. Gynecol. 1996, 88 Pt 1, 577–582. [Google Scholar] [CrossRef]
- Schuchat, A. Epidemiology of Group B Streptococcal Disease in the United States: Shifting Paradigms. Clin. Microbiol. Rev. 1998, 11, 497–513. [Google Scholar] [CrossRef]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K.; Mathews, T.J. Births: Final Data for 2015. Natl Vital Stat. Rep. 2017, 66, 1. [Google Scholar] [PubMed]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K.; Drake, P. Births: Final Data for 2017. Natl Vital Stat. Rep. 2018, 67, 1–50. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics and Clinical Findings | Enterovirus and West Nile Virus n= 333 | HSV n = 18 | GBS n = 60 | Staphylococcus Species n = 18 | Gram-Positive Others n = 35 | E. coli n = 37 | Gram Negative Others n = 40 | Fungal n= 5 | Unknown n = 147 |
|---|---|---|---|---|---|---|---|---|---|
| Male (%) | 186 (56) | 10 (56) | 28 (47) | 12 (66) | 18 (51) | 25 (68) | 24 (60) | 4 (80) | 87 (59) |
| Race/ethnicity | |||||||||
| White (%) | 135 (41) | 8 (44) | 14 (23) | 7 (39) | 5 (14) | 10 (27) | 16 (40) | 3 (60) | 49 (33) |
| Hispanic (%) | 129 (39) | 5 (28) | 28 (47) | 6 (33) | 17 (49) | 17 (46) | 10 (25) | 1 (20) | 66 (45) |
| Black (%) | 36 (11) | 4 (22) | 15 (25) | 5 (28) | 11 (31) | 6 (16) | 7 (18) | 1 (20) | 20 (14) |
| Other (%) | 33 (10) | 1 (6) | 3 (5) | 0 | 2 (6) | 4 (11) | 7 (18) | 0 | 12 (8) |
| Private insurance (%) | 165 (50) | 5 (28) | 17 (28) | 8 (44) | 19 (54) | 13 (35) | 17 (43) | 3 (60) | 57 (39) |
| Age | |||||||||
| <7 days | 18 (5) | 5 (28) | 10 (17) | 3 (17) | 10 (29) | 9 (24) | 10 (25) | 3 (60) | 17 (12) |
| 7–13 days (%) | 33 (10) | 3 (17) | 9 (15) | 2 (11) | 1 (3) | 3 (8) | 3 (8) | 1 (20) | 14 (10) |
| 14–20 days (%) | 36 (11) | 5 (28) | 4 (7) | 3 (17) | 5 (14) | 5 (14) | 7 (18) | 1 (20) | 7 (5) |
| 20–27 days (%) | 59 (18) | 2 (11) | 6 (10) | 2 (11) | 1 (3) | 4 (11) | 5 (13) | 0 | 15 (10) |
| >28 days (%) | 187 (56) | 3 (17) | 31 (52) | 8 (44) | 18 (51) | 16 (43) | 15 (38) | 0 | 94 (64) |
| CSF Findings | |||||||||
| Median CSF leukocytes (range) | 202 (1–7099) | 36.5 (0–247) | 1185 (5–24,900) | 119 (2–1290) | 915 (1–13,726) | 831 (16–161,500) | 129 (7–7350) | 549 (35–1063) | 227 (8–3848) |
| Percent neutrophils | 26 (0–95) | 4 (0–83) | 76.5 (3–97) | 43.5 (0–85) | 80 (0–98) | 70.5 (2–97) | 58.5 (7–95) | 75.5 (71–80) | 29 (0–93) |
| Protein mg/dL | 81 (21–6000) | 112.5 (59–1702) | 263.5 (51–6000) | 172 (58–1397) | 146.5 (54–2412) | 261 (46–3587) | 193 (43–1498) | 317 (72–1134) | 90 (16–1456) |
| Glucose mg/dL | 41 (27–112) | 37 (20–102) | 26.5 (20–98) | 36 (20–96) | 42 (20–126) | 35 (20–121) | 40 (20–97) | 47 (20–55) | 42 (20–83) |
| Death (%) | 0 | 1 (6) | 6 (10) | 2 (11) | 0 | 2 (5) | 3 (8) | 0 | 0 |
| Enterovirus and West Nile Virus n= 333 | HSV n = 18 | GBS n = 60 | Staphylococcus Species n = 18 | Other Gram-Positive n = 35 | E. coli n = 37 | Other Gram-Negative n = 40 | Fungal n = 5 | Un-known n = 147 | IVIG n = 1 |
|---|---|---|---|---|---|---|---|---|---|
| Enterovirus (332) | HSV-1 (4) | GBS (60) | Staphylococcus aureus (8) | Gram-positive bacteria, no species (13) | E. coli (37) | Enterobacter cloacae (7) | Candida albicans (5) | ||
| West Nile virus (1) | HSV-2 (14) | Staphylococcus epidermidis (8) | Streptococcus gallolyticus (9) | Klebsiella pneumoniae (7) | |||||
| Staphylococcus warneri (1) | Enterococcus faecalis (6) | Salmonella enterica (6) | |||||||
| Staphylococcus hominis (1) | Streptococcus pneumoniae (3) | Acinetobacter baumannii (3) | |||||||
| Streptococcus mitis (2) | Serratia marcescens (3) | ||||||||
| Clostridium species (1) | Gram-negative rods, no species (2) | ||||||||
| Streptococcus infantarius (1) | Neisseria meningitidis (2) | ||||||||
| Proteus mirabilis (2) | |||||||||
| Citrobacter braakii (1) | |||||||||
| Citrobacter freundii (1) | |||||||||
| Haemophilus influenzae (1) | |||||||||
| Klebsiella oxytoca (1) | |||||||||
| Pantoea species (1) | |||||||||
| Pseudomonas aeruginosa (1) | |||||||||
| Pseudomonas fluorescens (1) | |||||||||
| Morganella morganii (1) | |||||||||
| Early (0–7 Days) (n = 10) | Late (>7 Days) (n = 50) | |
|---|---|---|
| Maternal screen | 9 | 35 |
| Positive for GBS | 1 (11%) | 14 (40%) |
| Negative for GBS | 8 (89%) | 21 (60%) |
| GBS prophylaxis | 2 (22%) | 10 (20%) |
| Concurrent bacteremia | 8 (89%) | 35 (69%) |
| Death | 1 (11%) | 5 (10%) |
| Resistance Spectra (Total) | Ampicillin | 3rd Generation Cephalosporin | Gentamicin | Piperacillin | Ciprofloxacin | 4th Generation Cephalosporin (Cefepime) |
|---|---|---|---|---|---|---|
| E. coli (37) | 23/35 (66%) | 2/34 (6%) | 3/33 (9%) | 16/27 (59%) | 5/30 (20%) | 0/5 |
| Other Gram-negative (38) | 9/16 (56%) | 8/35 (23%) | 1/30 (3%) | 12/24 (50%) | 0/22 | 0/1 |
| Early Preterm (≤34 Weeks Gestation) (n = 68) | Late Preterm (35–36 Weeks Gestation) (n = 47) | Full Term (37+ Weeks) (n = 579) | |
|---|---|---|---|
| Viral | 6 (9%) | 23 (49%) | 322 (56%) |
| Enterovirus and other viruses * | 4 (6%) | 20 (43%) | 309 (53%) |
| HSV | 2 (3%) | 3 (6%) | 13 (2%) |
| Bacterial | 55 (81%) | 13 (28%) | 123 (21%) |
| Streptococcus agalactiae | 13 (19%) | 2 (4%) | 45 (8%) |
| Staphylococcus species | 8 (12%) | 1 (2%) | 9 (2%) |
| Other Gram-positive ** | 8 (12%) | 2 (4%) | 25 (4%) |
| E. coli | 11 (16%) | 5 (11%) | 21 (4%) |
| Other Gram-negative ** | 15 (22%) | 3 (6%) | 22 (4%) |
| Fungal | 4 (6%) | 1 (2%) | 0 |
| Unknown | 3 (4%) | 10 (21%) | 134 (23%) |
| Other *** | 0 (0%) | 0 (0%) | 1 (0.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erickson, T.A.; Munoz, F.M.; Troisi, C.L.; Nolan, M.S.; Hasbun, R.; Brown, E.L.; Murray, K.O. The Epidemiology of Meningitis in Infants under 90 Days of Age in a Large Pediatric Hospital. Microorganisms 2021, 9, 526. https://doi.org/10.3390/microorganisms9030526
Erickson TA, Munoz FM, Troisi CL, Nolan MS, Hasbun R, Brown EL, Murray KO. The Epidemiology of Meningitis in Infants under 90 Days of Age in a Large Pediatric Hospital. Microorganisms. 2021; 9(3):526. https://doi.org/10.3390/microorganisms9030526
Chicago/Turabian StyleErickson, Timothy A., Flor M. Munoz, Catherine L. Troisi, Melissa S. Nolan, Rodrigo Hasbun, Eric L. Brown, and Kristy O. Murray. 2021. "The Epidemiology of Meningitis in Infants under 90 Days of Age in a Large Pediatric Hospital" Microorganisms 9, no. 3: 526. https://doi.org/10.3390/microorganisms9030526
APA StyleErickson, T. A., Munoz, F. M., Troisi, C. L., Nolan, M. S., Hasbun, R., Brown, E. L., & Murray, K. O. (2021). The Epidemiology of Meningitis in Infants under 90 Days of Age in a Large Pediatric Hospital. Microorganisms, 9(3), 526. https://doi.org/10.3390/microorganisms9030526