
HBcAb Positivity Is a Risk Factor for an Increased Detectability of HIV RNA after Switching to a Two-Drug Regimen Lamivudine-Based (2DR-3TC-Based) Treatment: Analysis of a Multicenter Italian Cohort

 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
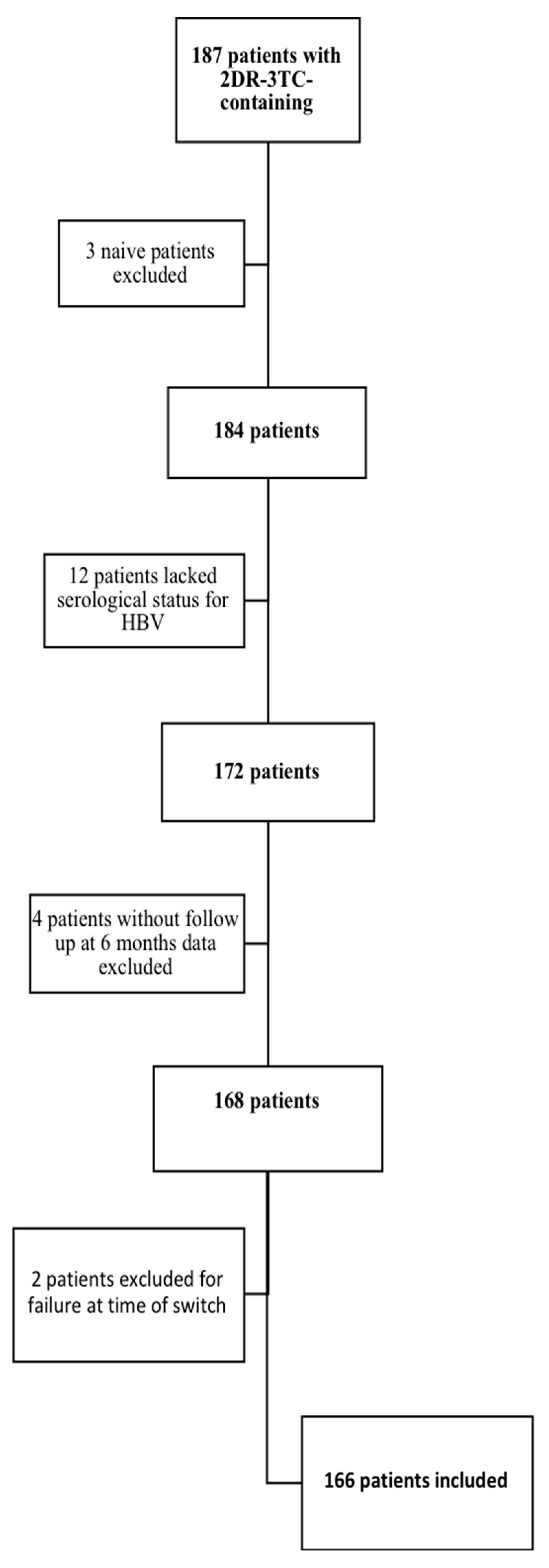
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Laboratory Testing for the Diagnosis of HBV and HIV Infections
2.4. HIV Viral Load Definitions
2.5. Endpoints
2.6. Statistical Methods
2.7. Ethic Statements
3. Results
3.1. Description of the Study Population
HIV Viral Load Values at the Different Time Points After Switching to the 2DR-3TC Regimen
3.2. Comparison of HIV Viral Load Values between HBcAb-Positive and HBcAb-Negative Patients
3.2.1. HIV Viral Load Values at the Different Time Assessments in the Two Groups before the 2DR-3TC Switch
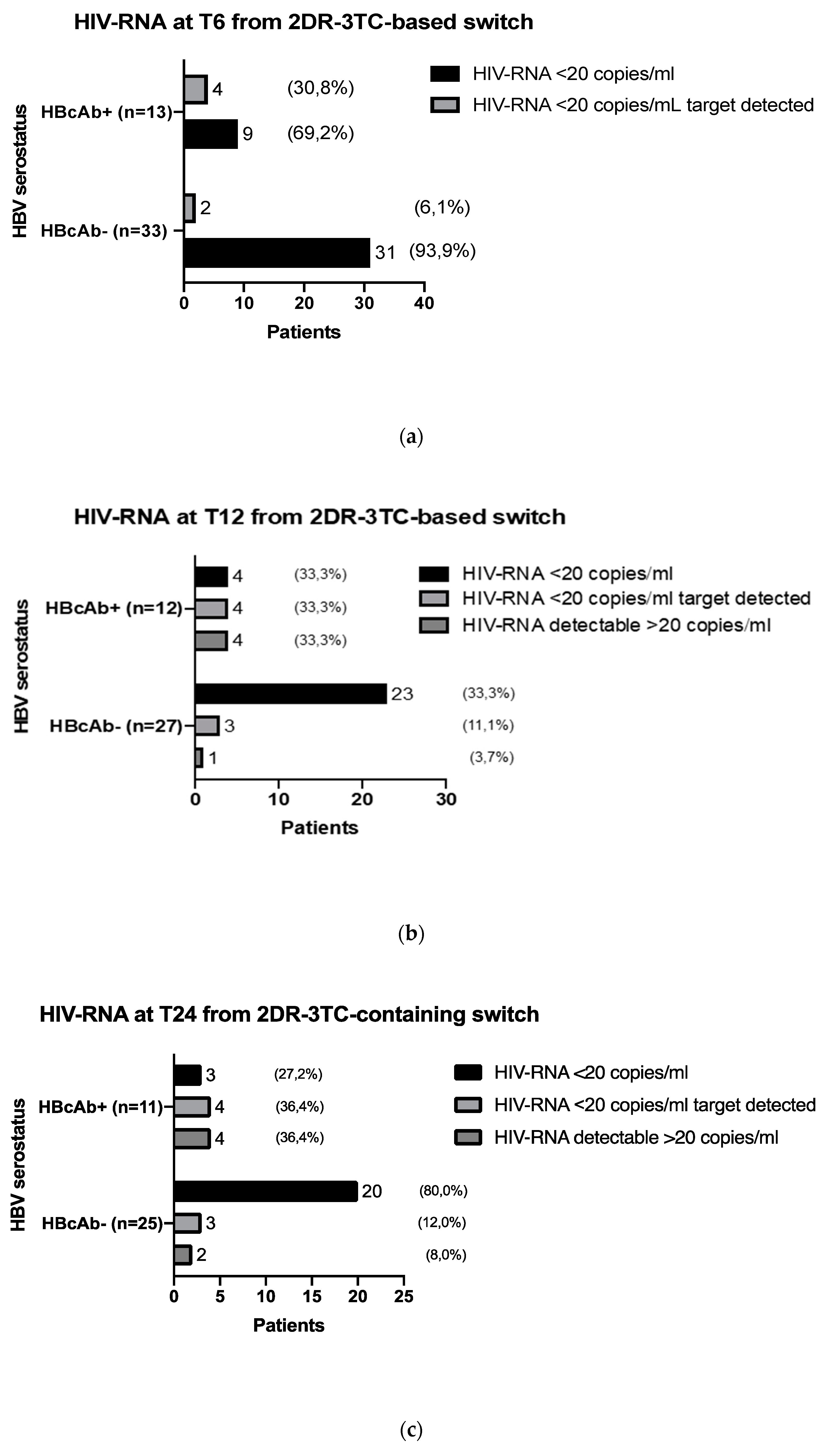
3.2.2. HIV Viral Load Values at the Different Time Assessments in the Two Groups after the 2DR-3TC Switch
3.2.3. HIV Viral Load Values in HBcAb -Positive and HBcAb -Negative Patients with HIV RNA Permanently Undetectable to All Assessments before 2DR-3TC Switching
3.2.4. Risk Factors for Signs of HIV-RNA Detectability 24 Months after the 2DR-3TC-Based Switch
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raimondo, G.; Locarnini, S.; Pollicino, T.; Levrero, M.; Zoulim, F.; Lok, A.S. Taormina Workshop on Occult HBV Infection Faculty Members. Update of the statements on biology and clinical impact of occult hepatitis B virus infection. J. Hepatol. 2019, 71, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Soriano, V.; Aguilera, A.; Gonzalez, R.; Gomez-Gallego, F.; Barea, L.; Treviño, M.; Corral, O. Occult hepatitis B and HIV infection. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1403–1407. [Google Scholar] [CrossRef]
- Ryan, K.; Anderson, M.; Gyurova, I.; Ambroggio, L.; Moyo, S.; Sebunya, T.; Makhema, J.; Marlink, R.; Essex, M.; Musonda, R.; et al. High Rates of Occult Hepatitis B Virus Infection in HIV-Positive Individuals Initiating Antiretroviral Therapy in Botswana. Open Forum Infect. Dis. 2017, 4, ofx195. [Google Scholar] [CrossRef]
- Saha, D.; Pal, A.; Sarkar, N.; Das, D.; Blackard, J.T.; Guha, S.K.; Saha, B.; Chakravarty, R. Occult hepatitis B virus infection in HIV positive patients at a tertiary healthcare unit in eastern India. PLoS ONE 2017, 12, e0179035. [Google Scholar] [CrossRef] [PubMed]
- Coffin, C.S.; Mulrooney-Cousins, P.M.; Osiowy, C.; van der Meer, F.; Nishikawa, S.; Michalak, T.I.; van Marle, G.; Gill, M.J. Virological characteristics of occult hepatitis B virus in a North American cohort of human immunodeficiency virus type 1-positive patients on dual active anti-HBV/HIV therapy. J. Clin. Virol. 2014, 60, 347–353. [Google Scholar] [CrossRef]
- Wandeler, G.; Gsponer, T.; Bihl, F.; Bernasconi, E.; Cavassini, M.; Kovari, H.; Schmid, P.; Battegay, M.; Calmy, A.; Egger, M.; et al. Swiss HIV Cohort Study. Hepatitis B virus infection is associated with impaired immunological recovery during antiretroviral therapy in the Swiss HIV cohort study. J. Infect. Dis. 2013, 208, 1454–1458. [Google Scholar] [CrossRef]
- Dore, G.J.; Cooper, D.A.; Pozniak, A.L.; DeJesus, E.; Zhong, L.; Miller, M.D.; Lu, B.; Cheng, A.K.; 903 Study Team; 907 Study Team. Efficacy of tenofovir disoproxil fumarate in antiretroviral therapy-naive and -experienced patients coinfected with HIV-1 and hepatitis B virus. J. Infect. Dis. 2004, 189, 1185–1192. [Google Scholar] [CrossRef]
- Nebbia, G.; Garcia-Diaz, A.; Ayliffe, U.; Smith, C.; Dervisevic, S.; Johnson, M.; Gilson, R.; Tedder, R.; Geretti, A.M. Predictors and kinetics of occult hepatitis B virus infection in HIV-infected persons. J. Med. Virol. 2007, 79, 1464–1471. [Google Scholar] [CrossRef] [PubMed]
- Altfeld, M.; Rockstroh, J.K.; Addo, M.; Kupfer, B.; Pult, I.; Will, H.; Spengler, U. Reactivation of hepatitis B in a long-term anti-HBs-positive patient with AIDS following lamivudine withdrawal. J. Hepatol. 1998, 29, 306–309. [Google Scholar] [CrossRef]
- Costantini, A.; Marinelli, K.; Biagioni, G.; Monachetti, A.; Ferreri, M.L.; Butini, L.; Montroni, M.; Manzin, A.; Bagnarelli, P. Molecular analysis of hepatitis B virus (HBV) in an HIV co-infected patient with reactivation of occult HBV infection following discontinuation of lamivudine-including antiretroviral therapy. BMC Infect. Dis. 2011, 11, 310. [Google Scholar] [CrossRef]
- Martin-Carbonero, L.; Soriano, V. New paradigms for treating hepatitis B in HIV/hepatitis B virus co-infected patients. J. Antimicrob. Chemother. 2010, 65, 379–382. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lukhwareni, A.; Gededzha, M.P.; Amponsah-Dacosta, E.; Blackard, J.T.; Burnett, R.J.; Selabe, S.G.; Kyaw, T.; Mphahlele, M.J. Impact of Lamivudine-Based Antiretroviral Treatment on Hepatitis B Viremia in HIV-Coinfected South Africans. Viruses 2020, 12, 634. [Google Scholar] [CrossRef] [PubMed]
- Malagnino, V.; Cerva, C.; Maffongelli, G.; Teti, E.; Foroghi Biland, L.; Cesta, N.; De Masi, M.; Stingone, C.; Armenia, D.; Svicher, V.; et al. HBcAb seropositivity is correlated with poor HIV viremia control in an Italian cohort of HIV/HBV-coinfected patients on first-line therapy. Sci. Rep. 2019, 9, 11942. [Google Scholar] [CrossRef] [PubMed]
- Morsica, G.; Ancarani, F.; Bagaglio, S.; Maracci, M.; Cicconi, P.; Cozzi Lepri, A.; Antonucci, G.; Bruno, R.; Santantonio, T.; Tacconi, L.; et al. HepaICONA and the ICONA Study Groups. Occult hepatitis B virus infection in a cohort of HIV-positive patients: Correlation with hepatitis C virus coinfection, virological and immunological features. Infection 2009, 37, 445–449. [Google Scholar] [CrossRef]
- Salpini, R.; Malagnino, V.; Piermatteo, L.; Mulas, T.; Alkhatib, M.; Scutari, R.; Teti, E.; Cerva, C.; Yu La Rosa, K.; Brugneti, M.; et al. Cryptic HBV Replicative Activity Is Frequently Revealed in Anti-HBc-Positive/HBsAg-Negative Patients with HIV Infection by Highly Sensitive Molecular Assays, and Can Be Predicted by Integrating Classical and Novel Serological HBV Markers. Microorganisms 2020, 8, 1819. [Google Scholar] [CrossRef] [PubMed]
- Marcuccilli, F.; Farchi, F.; Mirandola, W.; Ciccozzi, M.; Paba, P.; Bonanno, E.; Perno, C.F.; Ciotti, M. Performance evaluation of Anyplex™II HPV28 detection kit in a routine diagnostic setting: Comparison with the HPV Sign® Genotyping Test. J. Virol. Methods 2015, 217, 8–13. [Google Scholar] [CrossRef]
- Doyle, T.; Geretti, A.M. Low-level viraemia on HAART: Significance and management. Curr. Opin. Infect. Dis. 2012, 25, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Maggiolo, F.; Callegaro, A.; Cologni, G.; Bernardini, C.; Velenti, D.; Gregis, G.; Quinzan, G.; Soavi, L.; Iannotti, N.; Malfatto, E.; et al. Ultrasensitive assessment of residual low-level HIV viremia in HAART-treated patients and risk of virological failure. J. Acquir. Immune Defic. Syndr. 2012, 60, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Margot, N.; Koontz, D.; McCallister, S.; Mellors, J.W.; Callebaut, C. Measurement of plasma HIV-1 RNA below the limit of quantification (<20 copies/mL) of commercial assays with the integrase HIV RNA single-copy assay. J. Clin. Virol. 2018, 108, 50–52. [Google Scholar] [CrossRef]
- Fleming, J.; Mathews, W.C.; Rutstein, R.M.; Aberg, J.; Somboonwit, C.; Cheever, L.W.; Berry, S.A.; Gebo, K.A.; Moore, R.D. HIV Research Network. Low-level viremia and virologic failure in persons with HIV infection treated with antiretroviral therapy. AIDS 2019, 33, 2005–2012. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.-Y. Hepatitis B virus coinfection in human immunodeficiency virus-infected patients: A review. World J. Gastroenterol. 2014, 20, 14598. [Google Scholar] [CrossRef] [PubMed]
- Laprise, C.; de Pokomandy, A.; Baril, J.G.; Dufresne, S.; Trottier, H. Virologic failure following persistent low-level viremia in a cohort of HIV-positive patients: Results from 12 years of observation. Clin. Infect. Dis. 2013, 57, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Twu, J.S.; Chu, K.; Robinson, W.S. Hepatitis B virus X gene activates kappa B-like enhancer sequences in the long terminal repeat of human immunodeficiency virus 1. Proc. Natl. Acad. Sci. USA 1989, 86, 5168–5172. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gonzalo, M.; Carretero, M.; Rullas, J.; Lara-Pezzi, E.; Aramburu, J.; Berkhout, B.; Alcamí, J.; López-Cabrera, M. The hepatitis B virus X protein induces HIV-1 replication and transcription in synergy with T-cell activation signals: Functional roles of NF-kappaB/NF-AT and SP1-binding sites in the HIV-1 long terminal repeat promoter. J. Biol. Chem. 2001, 276, 35435–35443. [Google Scholar] [CrossRef] [PubMed]
- Maponga, T.G.; Andersson, M.I.; van Rensburg, C.J.; Arends, J.E.; Taljaard, J.; Preiser, W.; Glashoff, R.H. HBV and HIV viral load but not microbial translocation or immune activation are associated with liver fibrosis among patients in South Africa. BMC Infect. Dis. 2018, 18, 214. [Google Scholar] [CrossRef] [PubMed]
- Abdullahi, A.; Fopoussi, O.M.; Torimiro, J.; Atkins, M.; Kouanfack, C.; Geretti, A.M. Hepatitis B Virus (HBV) Infection and Re-activation During Nucleos(t)ide Reverse Transcriptase Inhibitor-Sparing Antiretroviral Therapy in a High-HBV Endemicity Setting. Open Forum Infect. Dis. 2018, 5, ofy251. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Population | n = 166 | |
|---|---|---|
| Sex ratio M:F (%F *) | 128:38 (22.9%) | |
| Age, years ** | 52.5 (42–59) | |
| Calendar year of HIV diagnosis ** | 2009 (2003–2013) | |
| Nadir CD4+, cell/mmc ** | 293 (172–414) | |
| HBcAb-positive * | 58 (34.9%) | |
| CD4+ cell/mmc at 2DR switch ** | 695 (547–880) | |
| Triple ART drug classes composition *: | ||
| Two NRTIs + PI | 65 (39.2%) | |
| Two NRTIs +NNRTI | 38 (22.9%) | |
| Two NRTIs + INI | 56 (33.7%) | |
| Other | 7 (4.2%) | |
| 2DR composition *: | ||
| 3TC + PI | 59 (35.5%) | |
| 3TC + DTG | 107 (64.5%) | |
| HIV-RNA copies/mL 24 months before 2DR switch *: | ||
| pts <20 copies/ml | 130 (78.3%) | |
| pts <20 copies/mL target detected | 36 (21.7%) | |
| HIV-RNA copies/mL 12 months before 2DR switch *: | ||
| pts <20 copies/ml | 133 (80.1%) | |
| pts <20 copies/mL target detected | 33 (19.8%) | |
| HIV RNA at 2DR switch *: | ||
| pts <20 copies/ml | 126 (75.9%) | |
| pts <20 copies/mL target detected | 36 (31.7%) | |
| Not available | 4 (2.4%) | |
| HIV RNA 6 months post-2DR switch * | ||
| pts <20 copies/ml | 129 (77.7%) | |
| pts <20 copies/mL target detected | 37 (22.3%) | |
| HIV RNA 12 months post-2DR switch *††: | ||
| pts <20 copies/ml | 74 (50.4%) | |
| pts <20 copies/mL target detected | 43 (29.9%) | |
| pts detectable >20 copies/ml | 27 (18.7%) | |
| HIV RNA 24 months post-2DR switch *‡: | ||
| pts <20 copies/ml | 53 (42.4%) | |
| pts <20 copies/mL target detected | 44 (35.2%) | |
| pts detectable >20 copies/ml | 28 (22.4%) | |
| Patients Characteristics | HBcAb-Positive (n = 58) | HBcAb-Negative (n = 108) | p-Value | |
|---|---|---|---|---|
| Sex ratio M:F (%F *) | 46:12 (20.7%) | 82:26 (24.1%) | 0.62 | |
| Age, years | 55 (51–61) | 49 (37–57) | 0.0007 | |
| Calendar year of HIV diagnosis ** | 2002 (1999–2010) | 2008 (2006–2014) | 0.0001 | |
| Nadir CD4+ cell/mmc ** | 251 (145–341) | 316 (201–446) | 0.047 | |
| History of therapeutic failure * | 12 (20.7%) | 12 (11.1%) | 0.26 | |
| Pre-2DR switch triple ART composition * | 0.023 | |||
| Two NRTIs + PI | 31 (53.4%) | 34 (31.5%) | ||
| Two NRTIs + NNRTI | 12 (20.7%) | 26 (24.1%) | ||
| Two NRTIs + INI | 12 (20.7%) | 44 (40.7%) | ||
| Other | 3 (5.2%) | 4 (3.7%) | ||
| Reason for switch | 0.44 | |||
| Therapeutic failure pre-switch | 1 (1.7%) | 2 (1.85) | ||
| Toxicity | 4 (6.8%) | 10 (9.2%) | ||
| Drug interaction | 7 (12.1%) | 17 (15.7%) | ||
| Pill burden | 3 (5.2%) | 9 (8.3%) | ||
| Pre-emptive switch | 43 (74.1%) | 70 (64.8%) | ||
| 2DR composition * | 0.51 | |||
| 3TC + PI | 24 (41.4%) | 35 (32.4%) | ||
| 3TC + DTG | 34 (58.6%) | 73 (67.6%) | ||
| CD4+ cell/mmc at 2DR switch ** | 660 (552–845) | 703 (543–894) | 0.58 | |
| HIV RNA 24 months pre-2DR switch * | 0.53 | |||
| pts <20 copies/mL | 47 (81%) | 83 (76.8%) | ||
| pts <20 copies/mL target detected | 11 (19%) | 25 (23.2%) | ||
| HIV RNA 12 months pre-2DR switch * | 0.31 | |||
| pts <20 copies/mL | 44 (75.9%) | 89 (82.4%) | ||
| pts <20 copies/mL target detected | 14 (24.1%) | 19 (17.6%) | ||
| HIV RNA at 2DR switch * | 0.87 | |||
| pts <20 copies/mL | 43 (74.1%) | 83 (76.8%) | ||
| pts <20 copies/mL target detected | 13 (22.4%) | 23 (21.3%) | ||
| Not available | 2 (1.8%) | 2 (3.4%) | ||
| HIV RNA 6 months post-2DR switch* | 0.047 | |||
| pts <20 copies/mL | 40 (69%) | 89 (82.4%) | ||
| pts <20 copies/mL target detected | 18 (31%) | 19 (17.6%) | ||
| HIV RNA 12 months post-2DR switch *†† | 0.001 | |||
| pts <20 copies/mL | 18 (34%) | 56 (61.5%) | ||
| pts <20 copies/mL target detected | 18 (34%) | 25 (27.5%) | ||
| pts detectable >20 copies/mL | 17 (32%) | 10 (11%) | ||
| CD4+ cell/mmc at 24 months post 2DR switch *‡ | 698 (592–932) | 771 (669–947) | 0.64 | |
| HIV RNA 24 months post-2DR switch *‡ | 0.003 | |||
| pts <20 copies/mL | 12 (26%) | 41 (51.9%) | ||
| pts <20 copies/mL target detected | 17 (37%) | 27 (34.2%) | ||
| pts detectable >20 copies/mL | 17 (37%) | 11 (13.9%) | ||
| Patients Characteristics | HBcAb-Positive (n = 13) | HBcAb-Negative (n = 33) | p-Value | |
|---|---|---|---|---|
| Sex ratio M:F (%F *) | 12:1 (7.7%) | 22:11 (33.3%) | 0.07 | |
| Age, years | 55 (52–59) | 46.5 (33.5–55.5) | 0.008 | |
| Calendar year of HIV diagnosis ** | 1999 (1996–2006) | 2009 (2007–2014) | 0.0005 | |
| Nadir CD4+ cell/mmc ** | 208 (155–290) | 355 (224–466) | 0.01 | |
| Pre-2DR switch triple ART composition * | 0.37 | |||
| Two NRTIs + PI | 7 (53.8%) | 12 (36.4%) | - | |
| Two NRTIs + NNRTI | 4 (30.7%) | 7 (21.2%) | - | |
| Two NRTIs + INI | 2 (15.4%) | 13 (39.4%) | - | |
| Other | 0 (0) | 1 (3%) | - | |
| 2DR Composition * | 0.7 | |||
| 3TC + PI | 6 (46.2%) | 11 (33.3%) | - | |
| 3TC + DTG | 7 (53.8%) | 22 (66.7%) | - | |
| CD4+ cell/mmc at 2DR switch ** | 671 (563–763) | 726 (514–885) | 0.01 | |
| HIV RNA at 2DR switch * | 0.26 | |||
| pts <20 copies/mL | 11 (84.6%) | 31 (93.9%) | - | |
| pts <20 copies/mL target detected | 1 (7.7%) | 2 (6.1%) | - | |
| Not available | 1 (7.7%) | 0 (0) | - | |
| HIV RNA 6 months post-2DR switch * | 0.025 | |||
| pts <20 copies/mL | 4 (30.7%) | 2 (6.1%) | - | |
| pts <20 copies/mL target detected | 9 (69.3%) | 31 (93.9%) | - | |
| HIV RNA 12 months post-2DR switch *†† | 0.004 | |||
| pts <20 copies/ml | 4 (33.3%) | 23 (85.2%) | - | |
| pts <20 copies/mL target detected | 4 (33.3%) | 3 (11.1%) | - | |
| pts detectable >20 copies/ml | 4 (33.3%) | 1 (3.7%) | - | |
| HIV RNA 24 months post-2DR switch *‡ | 0.009 | |||
| pts <20 copies/ml | 3 (27.2%) | 20 (80%) | - | |
| pts <20 copies/mL target detected | 4 (36.4%) | 3 (12%) | - | |
| pts detectable >20 copies/mL | 4 (36.4%) | 2 (8%) | - | |
| Variables | Univariate | Multivariate | ||
| OR (95% CI) | p-value | OR (95%) | p-value | |
| Age, years | 1.09 (1.05–1.13) | <0.0001 | 1.08 (1.04–1.13) | <0.0001 |
| Calendar year of HIV infection | 0.96 (0.91–1.07) | 0.10 | 1.03 (0.97–1.10) | 0.25 |
| Nadir CD4+ cell count,/mm3 | 0.99 (0.99–1) | 0.083 | 0.99 (0.99–1) | 0.67 |
| 2DR-3TC DTG containing | 0.93 (0.45–1.92) | 0.86 | 1.16 (0.46–2.9) | 0.74 |
| HBcAb positivity | 3.05 (1.38–6,75) | 0.006 | 2.7 (1.05–6.9) | 0.038 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malagnino, V.; Teti, E.; Compagno, M.; Coppola, L.; Salpini, R.; Svicher, V.; Basso, M.; Battagin, G.; Panese, S.; Rossi, M.C.; et al. HBcAb Positivity Is a Risk Factor for an Increased Detectability of HIV RNA after Switching to a Two-Drug Regimen Lamivudine-Based (2DR-3TC-Based) Treatment: Analysis of a Multicenter Italian Cohort. Microorganisms 2021, 9, 396. https://doi.org/10.3390/microorganisms9020396
Malagnino V, Teti E, Compagno M, Coppola L, Salpini R, Svicher V, Basso M, Battagin G, Panese S, Rossi MC, et al. HBcAb Positivity Is a Risk Factor for an Increased Detectability of HIV RNA after Switching to a Two-Drug Regimen Lamivudine-Based (2DR-3TC-Based) Treatment: Analysis of a Multicenter Italian Cohort. Microorganisms. 2021; 9(2):396. https://doi.org/10.3390/microorganisms9020396
Chicago/Turabian StyleMalagnino, Vincenzo, Elisabetta Teti, Mirko Compagno, Luigi Coppola, Romina Salpini, Valentina Svicher, Monica Basso, Giuliana Battagin, Sandro Panese, Maria Cristina Rossi, and et al. 2021. "HBcAb Positivity Is a Risk Factor for an Increased Detectability of HIV RNA after Switching to a Two-Drug Regimen Lamivudine-Based (2DR-3TC-Based) Treatment: Analysis of a Multicenter Italian Cohort" Microorganisms 9, no. 2: 396. https://doi.org/10.3390/microorganisms9020396
APA StyleMalagnino, V., Teti, E., Compagno, M., Coppola, L., Salpini, R., Svicher, V., Basso, M., Battagin, G., Panese, S., Rossi, M. C., Scaggiante, R., Zago, D., Iannetta, M., Parisi, S. G., Andreoni, M., & Sarmati, L. (2021). HBcAb Positivity Is a Risk Factor for an Increased Detectability of HIV RNA after Switching to a Two-Drug Regimen Lamivudine-Based (2DR-3TC-Based) Treatment: Analysis of a Multicenter Italian Cohort. Microorganisms, 9(2), 396. https://doi.org/10.3390/microorganisms9020396