Colistin-Resistant Acinetobacter Baumannii Bacteremia: A Serious Threat for Critically Ill Patients

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
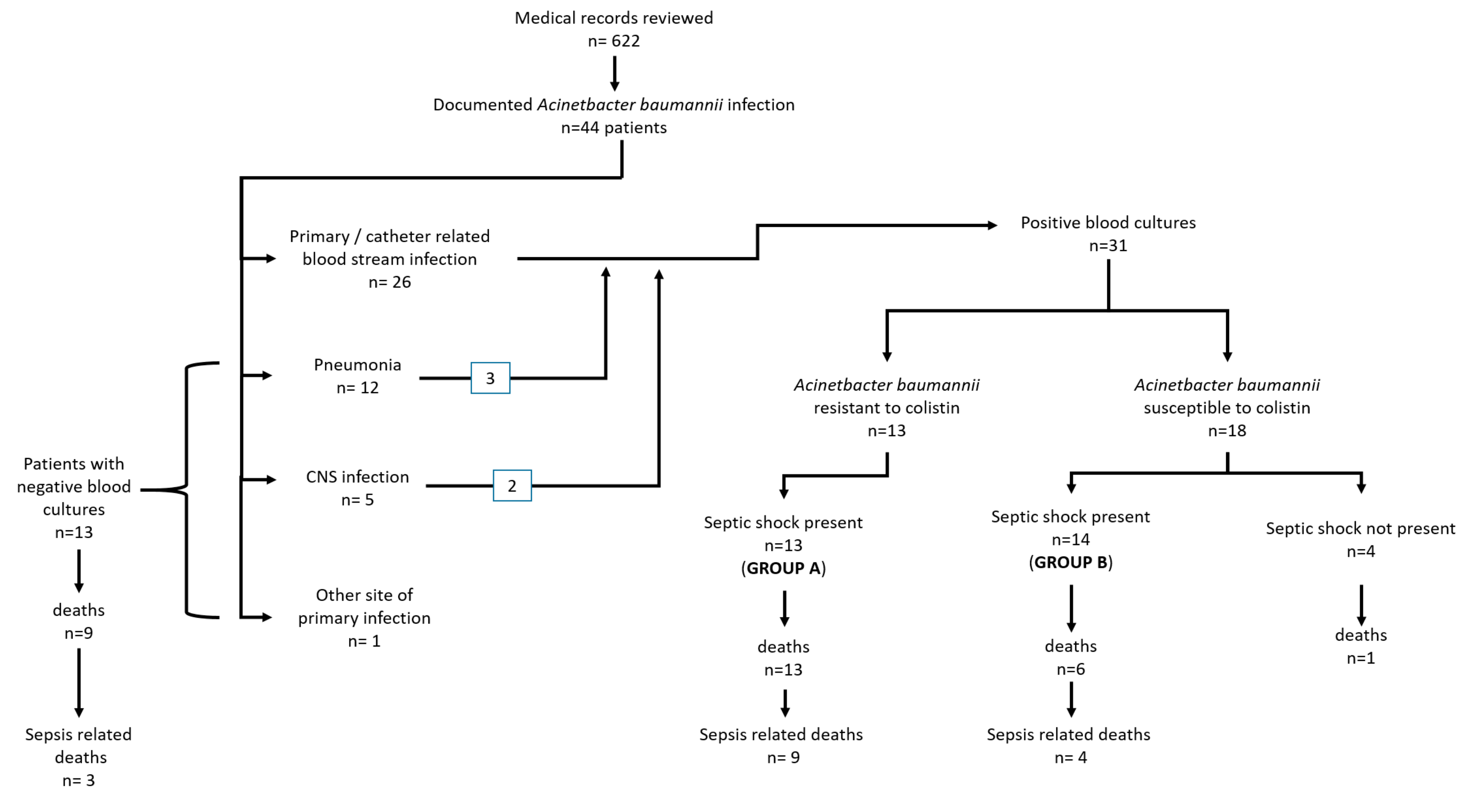
3.1. Patient Characteristics
3.2. Patients with Positive Blood Cultures Due to AΒ
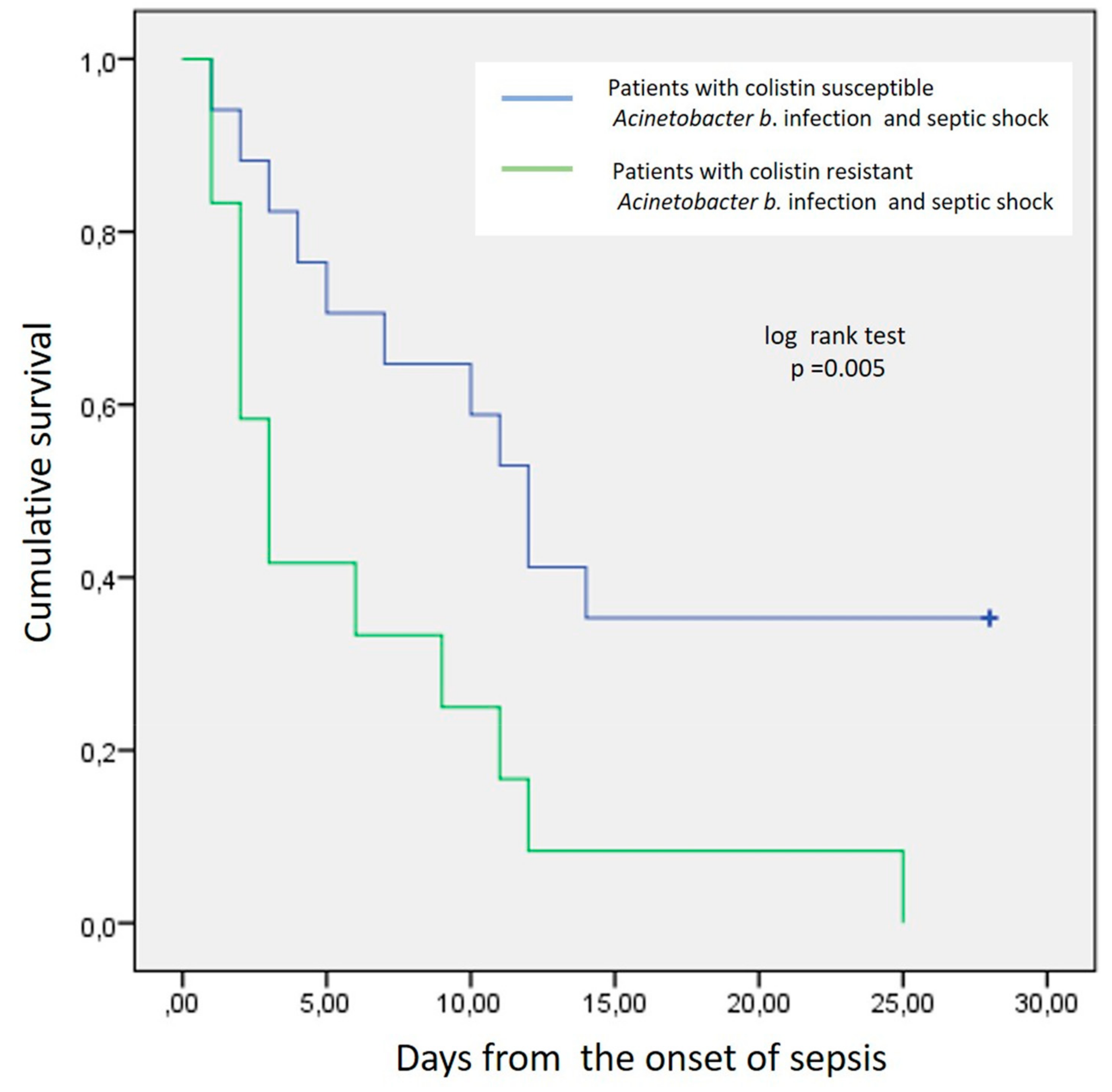
3.3. Patients’ Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thom, K.A.; Johnson, J.K.; Lee, M.S.; Harris, A.D. Environmental contamination because of multidrug-resistant Acinetobacter baumannii surrounding colonized or infected patients. Am. J. Infect. Control. 2011, 39, 711–715. [Google Scholar] [CrossRef]
- Rosa, R.M.; DePascale, D.; Cleary, T.; Fajardo-Aquino, Y.; Kett, D.H.; Munoz-Price, L.S. Differential environmental contamination with Acinetobacter baumannii based on the anatomic source of colonization. Am. J. Infect. Control. 2014, 42, 755–757. [Google Scholar] [CrossRef] [PubMed]
- Harding, C.M.; Hennon, S.W.; Feldman, M.F. Uncovering the mechanisms of Acinetobacter baumannii virulence. Nat. Rev. Genet. 2017, 16, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Maraki, S.; Mantadakis, E.; Mavromanolaki, V.E.; Kofteridis, D.; Samonis, G. A 5-year Surveillance Study on Antimicrobial Resistance of Acinetobacter baumannii Clinical Isolates from a Tertiary Greek Hospital. Infect. Chemother. 2016, 48, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.-C.; Chang, S.-C.; Wang, H.-Y.; Lai, J.-F.; Chen, P.-C.; Shiau, Y.-R.; Huang, I.-W.; Lauderdale, T.-L. Emergence of extensively drug-resistant Acinetobacter baumannii complex over 10 years: Nationwide data from the Taiwan Surveillance of Antimicrobial Resistance (TSAR) program. BMC Infect. Dis. 2012, 12, 200. [Google Scholar] [CrossRef]
- Su, C.-H.; Wang, J.-T.; Hsiung, C.A.; Chien, L.-J.; Chi, C.-L.; Yu, H.-T.; Chang, F.-Y.; Chang, S.-C. Increase of Carbapenem-Resistant Acinetobacter baumannii Infection in Acute Care Hospitals in Taiwan: Association with Hospital Antimicrobial Usage. PLoS ONE 2012, 7, 37788. [Google Scholar] [CrossRef]
- Perez, F.; Hujer, A.M.; Hujer, K.M.; Decker, B.K.; Rather, P.N.; Bonomo, R.A. Global Challenge of Multidrug-Resistant Acinetobacter baumannii. Antimicrob. Agents Chemother 2007, 51, 3471–3484. [Google Scholar] [CrossRef]
- Falagas, M.E.; Karveli, E.A.; Siempos, I.I.; Vardakas, K.Z. Acinetobacter infections: A growing threat for critically ill patients. Epidemiol. Infect. 2007, 136, 1009–1019. [Google Scholar] [CrossRef]
- Maragakis, L.L.; Perl, T.M.; Eliopoulos, G.M. Antimicrobial Resistance: Acinetobacter baumannii: Epidemiology, Antimicrobial Resistance, and Treatment Options. Clin. Infect. Dis. 2008, 46, 1254–1263. [Google Scholar] [CrossRef]
- Jean, S.-S.; Hsueh, P.-R.; Lee, W.-S.; Chang, H.-T.; Chou, M.-Y.; Chen, I.-S.; Wang, J.-H.; Lin, C.-F.; Shyr, J.-M.; Ko, W.-C.; et al. Nationwide surveillance of antimicrobial resistance among non-fermentative Gram-negative bacteria in Intensive Care Units in Taiwan: SMART programme data 2005. Int. J. Antimicrob. Agents 2009, 33, 266–271. [Google Scholar] [CrossRef]
- Ballouz, T.; Aridi, J.; Afif, C.; Irani, J.; Lakis, C.; Nasreddine, R.; Azar, E. Risk Factors, Clinical Presentation, and Outcome of Acinetobacter baumannii Bacteremia. Front. Microbiol. 2017, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-Y.; Chen, C.-L.; Wu, S.-R.; Huang, C.-W.; Chiu, C.-H. Risk Factors and Outcome Analysis of Acinetobacter baumannii Complex Bacteremia in Critical Patients. Crit. Care Med. 2014, 42, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.P.; Shih, S.-C.; Wang, N.-Y.; Wu, A.Y.; Sun, F.-J.; Chow, S.-F.; Chen, T.-L.; Yan, T.-R. Risk factors of mortality in patients with carbapenem-resistant Acinetobacter baumannii bacteremia. J. Microbiol. Immunol. Infect. 2016, 49, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Sunenshine, R.H.; Wright, M.-O.; Maragakis, L.L.; Harris, A.D.; Song, X.; Hebden, J.; Cosgrove, S.E.; Anderson, A.; Carnell, J.; Jernigan, D.B.; et al. Multidrug-resistant Acinetobacter Infection Mortality Rate and Length of Hospitalization. Emerg. Infect. Dis. 2007, 13, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Jung, J.Y.; Kang, Y.A.; Lim, J.E.; Kim, E.Y.; Lee, S.K.; Park, S.C.; Chung, K.S.; Park, B.H.; Kim, Y.S.; et al. Risk Factors for Occurrence and 30-Day Mortality for Carbapenem-Resistant Acinetobacter baumannii Bacteremia in an Intensive Care Unit. J. Korean Med Sci. 2012, 27, 939–947. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kim, S.I.; Hong, K.-W.; Kim, Y.R.; Park, Y.J.; Kang, M.-W. Risk Factors for Mortality in Patients with Carbapenem-Resistant Acinetobacter baumannii Bacteremia: Impact of Appropriate Antimicrobial Therapy. J. Korean Med Sci. 2012, 27, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Nowak, J.; Zander, E.; Stefanik, D.; Higgins, P.G.; Roca, I.; Vila, J.; McConnell, M.J.; Cisneros, J.M.; Seifert, H. MagicBullet Working Group WP4 High incidence of pandrug-resistant Acinetobacter baumannii isolates collected from patients with ventilator-associated pneumonia in Greece, Italy and Spain as part of the MagicBullet clinical trial. J. Antimicrob. Chemother. 2017, 72, 3277–3282. [Google Scholar] [CrossRef]
- Mavroidi, A.; Katsiari, M.; Palla, E.; Likousi, S.; Roussou, Z.; Nikolaou, C.; Platsouka, E.D. Investigation of Extensively Drug-Resistant blaOXA-23-Producing Acinetobacter baumannii Spread in a Greek Hospital. Microb. Drug Resist. 2017, 23, 488–493. [Google Scholar] [CrossRef]
- Lesho, E.; Yoon, E.-J.; Mc Gann, P.; Snesrud, E.; Kwak, Y.; Milillo, M.; Onmus-Leone, F.; Preston, L.; Clair, K.S.; Nikolich, M.; et al. Emergence of Colistin-Resistance in Extremely Drug-Resistant Acinetobacter baumannii Containing a Novel pmrCAB Operon During Colistin Therapy of Wound Infections. J. Infect. Dis. 2013, 208, 1142–1151. [Google Scholar] [CrossRef]
- López-Rojas, R.; McConnell, M.J.; Jiménez-Mejías, M.E.; Dominguez-Herrera, J.; Fernández-Cuenca, F.; Pachón, J. Colistin Resistance in a Clinical Acinetobacter baumannii Strain Appearing after Colistin Treatment: Effect on Virulence and Bacterial Fitness. Antimicrob. Agents Chemother. 2013, 57, 4587–4589. [Google Scholar] [CrossRef]
- Pelletier, M.R.; Casella, L.G.; Jones, J.W.; Adams, M.D.; Zurawski, D.; Hazlett, K.R.O.; Doi, Y.; Ernst, R.K. Unique Structural Modifications Are Present in the Lipopolysaccharide from Colistin-Resistant Strains of Acinetobacter baumannii. Antimicrob. Agents Chemother. 2013, 57, 4831–4840. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, J.A.; Ambe, L.A.; Casella, L.G.; Townsend, B.M.; Pelletier, M.R.; Ernst, R.K.; Shanks, R.M.Q.; Doi, Y. Activities of Vancomycin-Containing Regimens against Colistin-Resistant Acinetobacter baumannii Clinical Strains. Antimicrob. Agents Chemother. 2013, 57, 2103–2108. [Google Scholar] [CrossRef] [PubMed]
- Pogue, J.M.; Cohen, D.A.; Marchaim, D. Editorial commentary: Polymyxin-resistant Acinetobacter baumannii: Urgent action needed. Clin. Infect. Dis. 2015, 60, 1304–1307. [Google Scholar] [PubMed]
- Cai, Y.; Chai, D.; Wang, R.; Liang, B.; Bai, N. Colistin resistance of Acinetobacter baumannii: Clinical reports, mechanisms and antimicrobial strategies. J. Antimicrob. Chemother. 2012, 67, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, Z.A.; Hittle, L.E.; O’Hara, J.A.; Rivera, J.I.; Syed, A.; Shields, R.K.; Pasculle, A.W.; Ernst, R.K.; Doi, Y. Colistin-resistant Acinetobacter baumannii: Beyond carbapenem resistance. Clin. Infect. Dis. 2015, 60, 1295–1303. [Google Scholar] [CrossRef]
- Matthaiou, D.; Michalopoulos, A.; Rafailidis, P.I.; Karageorgopoulos, D.; Papaioannou, V.; Ntani, G.; Samonis, G.; Falagas, M.E. Risk factors associated with the isolation of colistin-resistant Gram-negative bacteria: A matched case-control study. Crit. Care Med. 2008, 36, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.M.; Teng, C.B.; Lye, D.; Apisarnthanarak, A. A Multicenter Case-Case Control Study for Risk Factors and Outcomes of Extensively Drug-Resistant Acinetobacter baumannii Bacteremia. Infect. Control. Hosp. Epidemiol. 2014, 35, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Mantzarlis, K.; Makris, D.; Zakynthinos, E. Risk factors for the first episode of Acinetobacter baumannii resistant to colistin infection and outcome in critically ill patients. J. Med Microbiol. 2020, 69, 35–40. [Google Scholar] [CrossRef]
- A Knaus, W.; A Draper, E.; Wagner, D.P.; E Zimmerman, J. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.-L.; De Mendonça, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kellum, J.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S.; et al. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; The Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup; et al. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock, 2012. Intensiv. Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef]
- Choi, S.-H.; Cho, E.B.; Chung, J.W.; Lee, M.-K. Changes in the early mortality of adult patients with carbapenem-resistant Acinetobacter baumannii bacteremia during 11 years at an academic medical center. J. Infect. Chemother. 2019, 25, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Bitew, A.; Molalign, T.; Chanie, M. Species distribution and antibiotic susceptibility profile of bacterial uropathogens among patients complaining urinary tract infections. BMC Infect. Dis. 2017, 17, 654. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Fu, Q.; Ye, H.; Liu, S. Risk factors for extensive drug-resistance and mortality in geriatric inpatients with bacteremia caused by Acinetobacter baumannii. Am. J. Infect. Control. 2015, 43, 857–860. [Google Scholar] [CrossRef]
- Tseng, Y.-C.; Wang, J.-T.; Wu, F.-L.L.; Chen, Y.-C.; Chie, W.-C.; Chang, S.-C. Prognosis of adult patients with bacteremia caused by extensively resistant Acinetobacter baumannii. Diagn. Microbiol. Infect. Dis. 2007, 59, 181–190. [Google Scholar] [CrossRef]
- Batirel, A.; Balkan, I.I.; Karabay, O.; Agalar, C.; Akalin, S.; Alici, O.; Alp, E.; Altay, F.A.; Altin, N.; Arslan, F.; et al. Comparison of colistin–carbapenem, colistin–sulbactam, and colistin plus other antibacterial agents for the treatment of extremely drug-resistant Acinetobacter baumannii bloodstream infections. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1311–1322. [Google Scholar] [CrossRef]
- Freire, M.; Garcia, D.D.O.; Garcia, C.; Bueno, M.C.; Camargo, C.; Magri, A.K.; Francisco, G.; Reghini, R.; Vieira, M.; Ibrahim, K.; et al. Bloodstream infection caused by extensively drug-resistant Acinetobacter baumannii in cancer patients: High mortality associated with delayed treatment rather than with the degree of neutropenia. Clin. Microbiol. Infect. 2016, 22, 352–358. [Google Scholar] [CrossRef]
- Aydın, M.; Ergonul, O.; Azap, A.; Bilgin, H.; Aydın, G.; Çavuş, S.A.; Demiroğlu, Y.Z.; Çalışkan, H.E.; Memikoğlu, O.; Menekşe, Ş.; et al. Rapid emergence of colistin resistance and its impact on fatality among healthcare-associated infections. J. Hosp. Infect. 2018, 98, 260–263. [Google Scholar] [CrossRef]
- Lertsrisatit, Y.; Santimaleeworagun, W.; Thunyaharn, S.; Traipattanakul, J. In vitro activity of colistin mono- and combination therapy against colistin-resistant Acinetobacter baumannii, mechanism of resistance, and clinical outcomes of patients infected with colistin-resistant A. baumannii at a Thai university hospital. Infect. Drug Resist. 2017, 10, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Katsiari, M.; Mavroidi, A.; Platsouka, E.; Nikolaou, C. Extensively drug-resistant Acinetobacter baumannii bacteraemia in a multidisciplinary intensive care unit during a 6-year period: Risk factors for fulminant sepsis. J. Glob. Antimicrob. Resist. 2018, 14, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Dickstein, Y.; Lellouche, J.; Amar, M.B.D.; Schwartz, D.; Nutman, A.; Daitch, V.; Yahav, D.; Leibovici, L.; Skiada, A.; Antoniadou, A.; et al. Treatment Outcomes of Colistin- and Carbapenem-resistant Acinetobacter baumannii Infections: An Exploratory Subgroup Analysis of a Randomized Clinical Trial. Clin. Infect. Dis. 2018, 69, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.; Nielsen, T.B.; Bonomo, R.A.; Pantapalangkoor, P.; Luna, B.; Spellberg, B. Clinical and Pathophysiological Overview ofAcinetobacterInfections: A Century of Challenges. Clin. Microbiol. Rev. 2016, 30, 409–447. [Google Scholar] [CrossRef] [PubMed]
- Song, J.Y.; Cheong, H.J.; Choi, W.S.; Heo, J.Y.; Noh, J.Y.; Kim, W.J. Clinical and microbiological characterization of carbapenem-resistant Acinetobacter baumannii bloodstream infections. J. Med. Microbiol. 2011, 60, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Xu, X.; Yao, J.; Deng, K.; Chen, S.; Shen, Z.; Yang, L.; Feng, G. Predictors of mortality in patients infected with carbapenem-resistant Acinetobacter baumannii: A systematic review and meta-analysis. Am. J. Infect. Control. 2019, 47, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Shorr, A.F.; Zilberberg, M.D.; Micek, S.T.; Kollef, M.H. Predictors of hospital mortality among septic ICU patients with Acinetobacter spp.bacteremia: A cohort study. BMC Infect. Dis. 2014, 14, 572. [Google Scholar] [CrossRef]
- Huang, S.-T.; Chiang, M.-C.; Kuo, S.-C.; Lee, Y.-T.; Chiang, T.-H.; Yang, S.-P.; Yin, T.-; Chen, T.-L.; Fung, C.-P. Risk factors and clinical outcomes of patients with carbapenem-resistant Acinetobacter baumannii bacteremia. J. Microbiol. Immunol. Infect. 2012, 45, 356–362. [Google Scholar] [CrossRef]
- Hernandez-Torres, A.; García-Vázquez, E.; Gómez, J.; Canteras, M.; Ruiz, J.; Yagüe, G. Multidrug and carbapenem-resistant Acinetobacter baumannii infections: Factors associated with mortality. Med. Clínica 2012, 138, 650–655. [Google Scholar] [CrossRef]
- Esterly, J.S.; Griffith, M.; Qi, C.; Malczynski, M.; Postelnick, M.J.; Scheetz, M.H. Impact of Carbapenem Resistance and Receipt of Active Antimicrobial Therapy on Clinical Outcomes of Acinetobacter baumannii Bloodstream Infections. Antimicrob. Agents Chemother. 2011, 55, 4844–4849. [Google Scholar] [CrossRef] [PubMed]
- Park, K.-H.; Shin, J.-H.; Lee, S.Y.; Kim, S.H.; Jang, M.O.; Kang, S.J.; Jung, S.-I.; Chung, E.-K.; Ko, K.S.; Jang, H.-C. The Clinical Characteristics, Carbapenem Resistance, and Outcome of Acinetobacter Bacteremia According to Genospecies. PLoS ONE 2013, 8, e65026. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Lee, E.J.; Kim, T.; Yu, S.N.; Park, K.-H.; Lee, M.S.; Park, S.Y.; Jeon, M.H.; Kim, T.H.; Choo, E.J.; et al. Early administration of appropriate antimicrobial agents to improve the outcome of carbapenem-resistant Acinetobacter baumannii complex bacteraemic pneumonia. Int. J. Antimicrob. Agents 2018, 51, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Lemos, E.; De La Hoz, F.; Einarson, T.; McGhan, W.; Quevedo, E.; Castañeda, C.; Kawai, K. Carbapenem resistance and mortality in patients with Acinetobacter baumannii infection: Systematic review and meta-analysis. Clin. Microbiol. Infect. 2014, 20, 416–423. [Google Scholar] [CrossRef]
- Da Silva, G.J.; Domingues, S. Interplay between Colistin Resistance, Virulence and Fitness in Acinetobacter baumannii. Antibiot. 2017, 6, 28. [Google Scholar] [CrossRef]
- Jones, C.L.; Singh, S.S.; Alamneh, Y.; Casella, L.G.; Ernst, R.K.; Lesho, E.P.; Waterman, P.E.; Zurawski, D.V. In Vivo Fitness Adaptations of Colistin-Resistant Acinetobacter baumannii Isolates to Oxidative Stress. Antimicrob. Agents Chemother. 2017, 61, e00598-16. [Google Scholar] [CrossRef]
- Bruhn, K.W.; Pantapalangkoor, P.; Nielsen, T.; Tan, B.; Junus, J.; Hujer, K.M.; Wright, M.S.; Bonomo, R.A.; Adams, M.D.; Chen, W.; et al. Host fate is rapidly determined by innate effector-microbial interactions during Acinetobacter baumannii bacteremia. J. Infect. Dis. 2014, 211, 1296–1305. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients’ Characteristics | |
|---|---|
| Age, years (mean ± SD) | 65.3 ± 17.6 |
| Sex-males (n, %) | 29 (65.9%) |
| APACHE II score (median, min–max) | 24 (13–40) |
| Diabetes mellitus (n, %) | 10 (22.7%) |
| Chronic heart failure (n, %) | 5 (11.3%) |
| Cardiovascular disease (n, %) | 8 (18.2%) |
| Chronic kidney disease (n, %) | 9 (20.5%) |
| Cirrhosis (n, %) | 3 (6.8%) |
| Chronic corticosteroid intake (n, %) | 7 (15.9%) |
| Cancer under therapy (n, %) | 3 (6.8%) |
| Immuno-suppressive therapy (n, %) | 4 (9.1%) |
| Cause of admission (n, %) | |
| Shock of any kind (n, %) | 10 (22.7%) |
| ARF, need for MV (n, %) | 16 (36.4%) |
| Coma (n, %) | 17 (38.6%) |
| Need for monitoring (n, %) | 1 (2.3%) |
| Parameter | |
|---|---|
| Blood culture positive (n, %) | 31 (70.5%) |
| Fulfil criteria for sepsis (n, %) | 39 (88.6%) |
| SOFA score 24 before (median, min–max) | 8 (3–18) |
| SOFA score on day 0 (median, min–max) | 11 (6–20) |
| Difference in SOFA (median, min–max) | 3 (2–10) |
| Fulfil criteria for septic shock (n, %) | 29 (65.9%) |
| Days from admission to sepsis, days (median, mix-max) | 21 (0–82) |
| Days from ICU admission to sepsis, days (median, min-max) | 12 (0–55) |
| Days from admission to positive blood cultures, days (median, mix-max) | 20 (3–82) |
| Days from admission to shock, days (median, mix-max) | 22 (0–82) |
| Duration of shock, days (median, mix-max) | 4 (1–14) |
| Lowest pH on day 0 (median, min-max) | 7.14 (6.8–7.44) |
| Levels of lactate on day 0 (median, min-max) | 3.4 (1–14) |
| PaO2/FiO2 ratio on day 0, (median, min-max) | 213 (41–463) |
| WBC count on day 0 (median, min-max) | 15,210 (900–46,100) |
| CRP on day 0 (median, min-max) | 185 (11–479) |
| Implications | |
| ARDS (n, %) | 15 (34.1%) |
| AKI (n, %) | 27 (61.4%) |
| CRRT (n, % | 14 (31.8%) |
| Septic myopathy (n, %) | 3 (6.8%) |
| DIC/thrombopenia (n, %) | 24 (54.5%) |
| Liver dysfunction (n, %) | 18 (40.1%) |
| Parameter | Patients with Colistin-Resistant A. baumannii Blood Stream Infection n = 13 | Patients with Colistin-Susceptible A. baumannii Blood Stream Infection n = 18 | p |
|---|---|---|---|
| Age, years (mean ± SD) | 67.6 ± 11.5 | 56.4 ± 19.9 | 0.07 |
| APACHE II score (median, min–max) | 28 (14–40) | 18 (13–40) | 0.01 |
| Charlson Comorbidity Index score (median, min–max) | 5 (3–10) | 4 (0–8) | 0.044 |
| Diabetes mellitus (n, %) | 2 (15.4%) | 3 (16.7%) | NS |
| Chronic heart failure (n, %) | 2 (15.4%) | 3 (16.7%) | NS |
| Chronic kidney disease (n, %) | 2 (15.4%) | 3 (16.7%) | NS |
| SOFA score 24 h before admission (median, min–max) | 9 (3–18) | 6 (3–12) | NS |
| SOFA score on day 0 (median, min–max) | 14 (6–20) | 11 (7–16) | NS |
| Difference in SOFA (median, min–max) | 2.5 (1–10) | 4 (4–4) | NS |
| Fulfil criteria for septic shock (n, %) | 13 (100%) | 14 (77.8%) | NS |
| Days from admission to sepsis, days (median, mix–max) | 14.5 (0–82) | 14 (3–38) | NS |
| Days from ICU admission to sepsis, days (median, min–max) | 10 (0–55) | 10.5 (0–31) | NS |
| Days from admission to positive blood cultures, days (median, mix–max) | 14 (5–82) | 15 (3–50) | NS |
| Days from admission to shock, days (median, mix–max) | 18 (0–82) | 12.5 (0–20) | NS |
| Duration of shock, days (median, mix–max) | 1 (0.5–14) | 5.5 (1–14) | 0.04 |
| Days from sepsis to death (median, mix–max) | 3 (1–25) | 4 (2–14) | 0.006 |
| Lowest pH on day 0 (median, min–max) | 7.03 (6.9–7.33) | 7.27 (7.11–7.44) | 0.03 |
| Levels of lactate on day 0 (median, min–max) | 2.8 (1–14) | 1.5 (0.8–8.8) | 0.0001 |
| Maximum levels of lactate during hospitalization (median, min–max) | 11.4 (1.4–26) | 1.7 (1–9.1) | 0.0001 |
| PaO2/FiO2 ratio on day 0, (median, min–max) | 198 (41–463) | 212 (105–385) | NS |
| WBC count on day 0 (median, min–max) | 14,500 (900–28,200) | 14,500 (2,700–46,100) | NS |
| CRP on day 0 (median, min–max) | 86.5 (11–430) | 172 (28–451) | NS |
| Implications | |||
| ARDS (n, %) | 5 (38.5%) | 4 (22.2%) | NS |
| AKI (n, %) | 12 (92.3%) | 6 (33.3%) | NS |
| Septic myopathy (n, %) | 0 | 2 (11.1) | - |
| DIC/thrombopenia (n, %) | 12 (92.3%) | 3 (16.7%) | 0.02 |
| Liver dysfunction (n, %) | 8 (61.5%) | 5 (27.8%) | NS |
| Mortality, overall | 13 (100%) | 7 (50%) | 0.001 |
| Sepsis-related mortality | 9 (69.2%) | 4 (22.2%) | 0.003 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papathanakos, G.; Andrianopoulos, I.; Papathanasiou, A.; Priavali, E.; Koulenti, D.; Koulouras, V. Colistin-Resistant Acinetobacter Baumannii Bacteremia: A Serious Threat for Critically Ill Patients. Microorganisms 2020, 8, 287. https://doi.org/10.3390/microorganisms8020287
Papathanakos G, Andrianopoulos I, Papathanasiou A, Priavali E, Koulenti D, Koulouras V. Colistin-Resistant Acinetobacter Baumannii Bacteremia: A Serious Threat for Critically Ill Patients. Microorganisms. 2020; 8(2):287. https://doi.org/10.3390/microorganisms8020287
Chicago/Turabian StylePapathanakos, Georgios, Ioannis Andrianopoulos, Athanasios Papathanasiou, Efthalia Priavali, Despoina Koulenti, and Vasilios Koulouras. 2020. "Colistin-Resistant Acinetobacter Baumannii Bacteremia: A Serious Threat for Critically Ill Patients" Microorganisms 8, no. 2: 287. https://doi.org/10.3390/microorganisms8020287
APA StylePapathanakos, G., Andrianopoulos, I., Papathanasiou, A., Priavali, E., Koulenti, D., & Koulouras, V. (2020). Colistin-Resistant Acinetobacter Baumannii Bacteremia: A Serious Threat for Critically Ill Patients. Microorganisms, 8(2), 287. https://doi.org/10.3390/microorganisms8020287