
Knowledge, Perception, and Attitude of Veterinarians About Q Fever from South Spain

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Material and Methods
2.1. Study Population and Sampling
2.2. Study Questionnaire
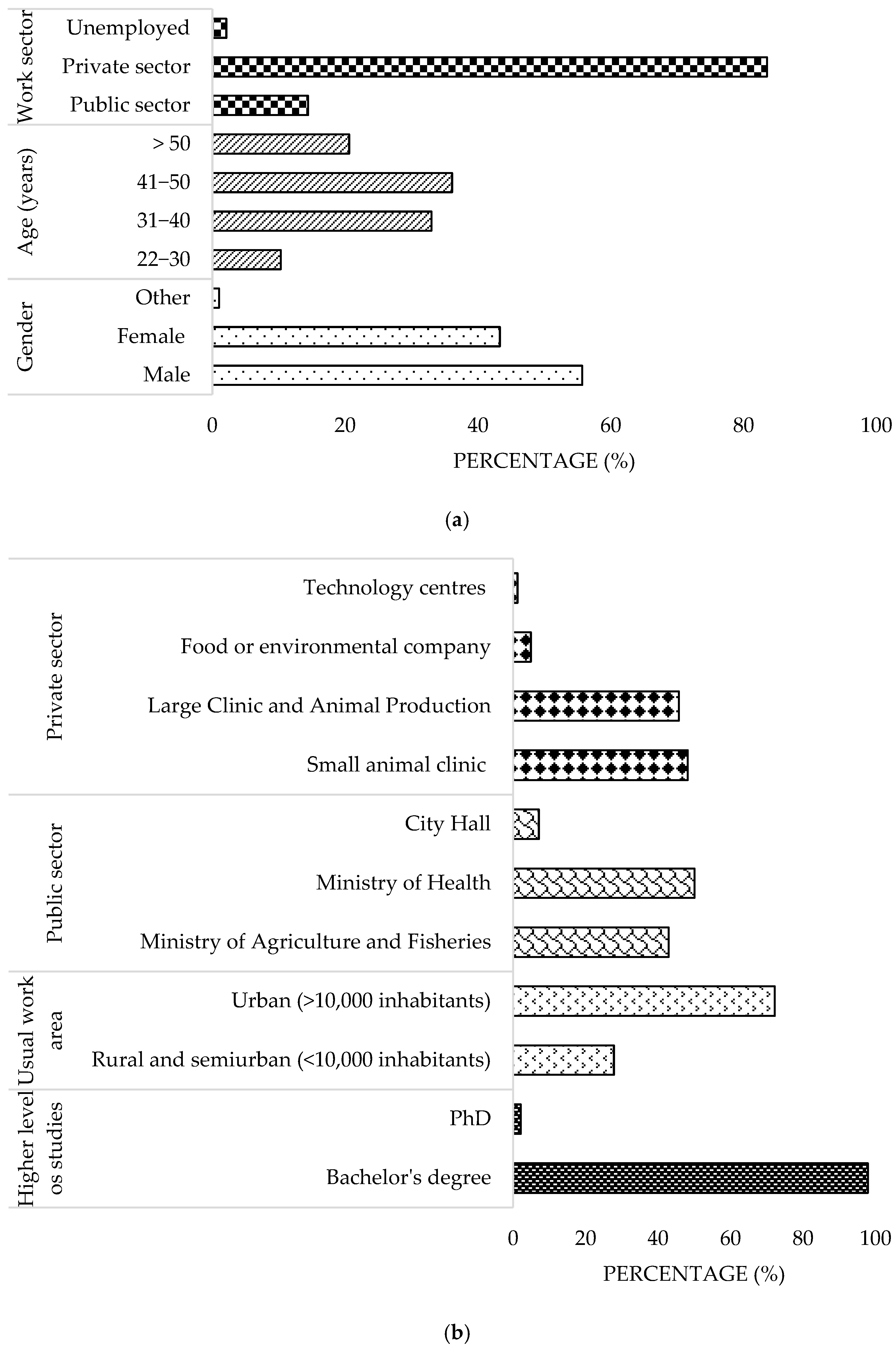
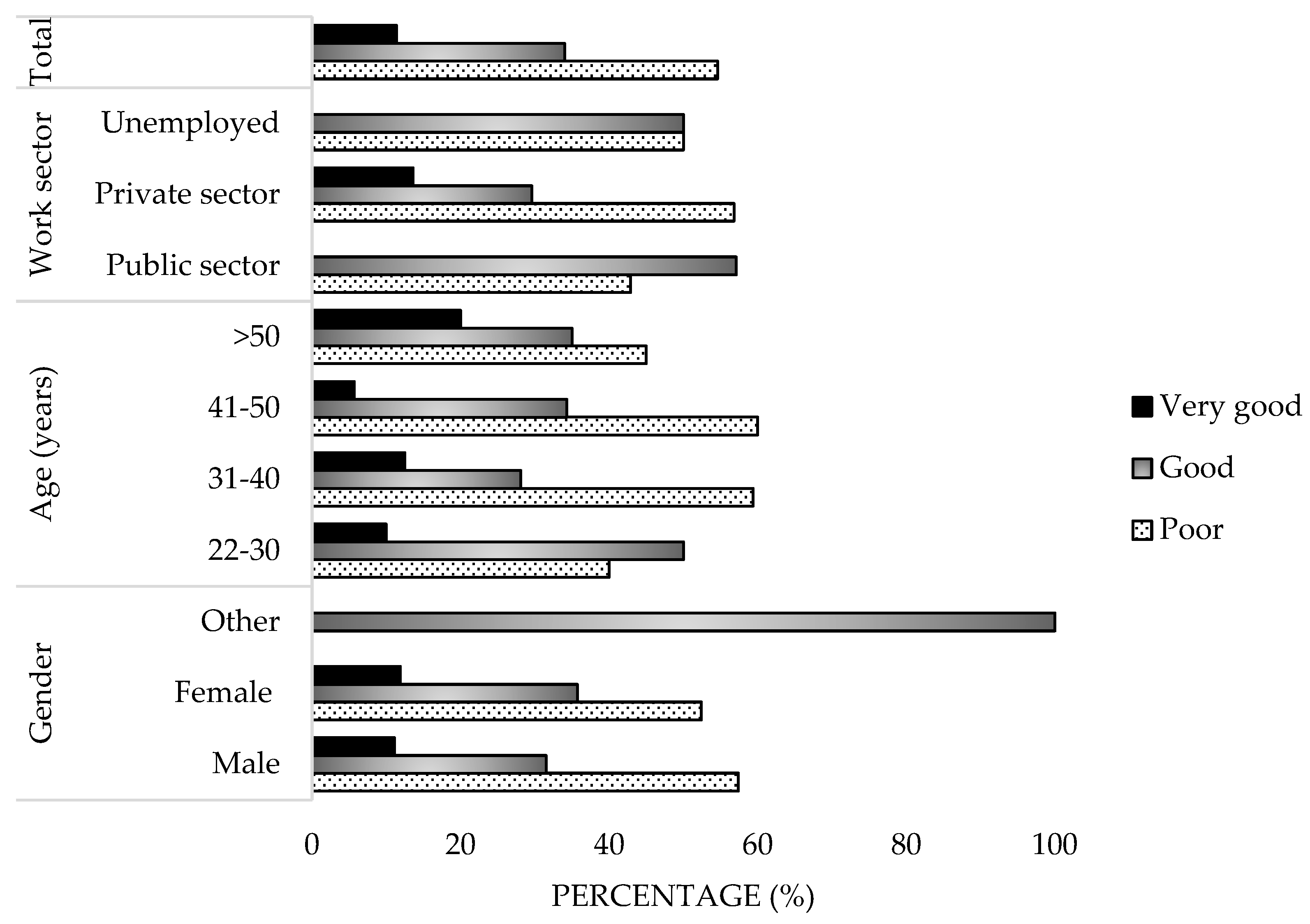
- Demographic data (10 items): personal details of the respondent (gender, age, highest level of education, current employment status, professional field, and work location).
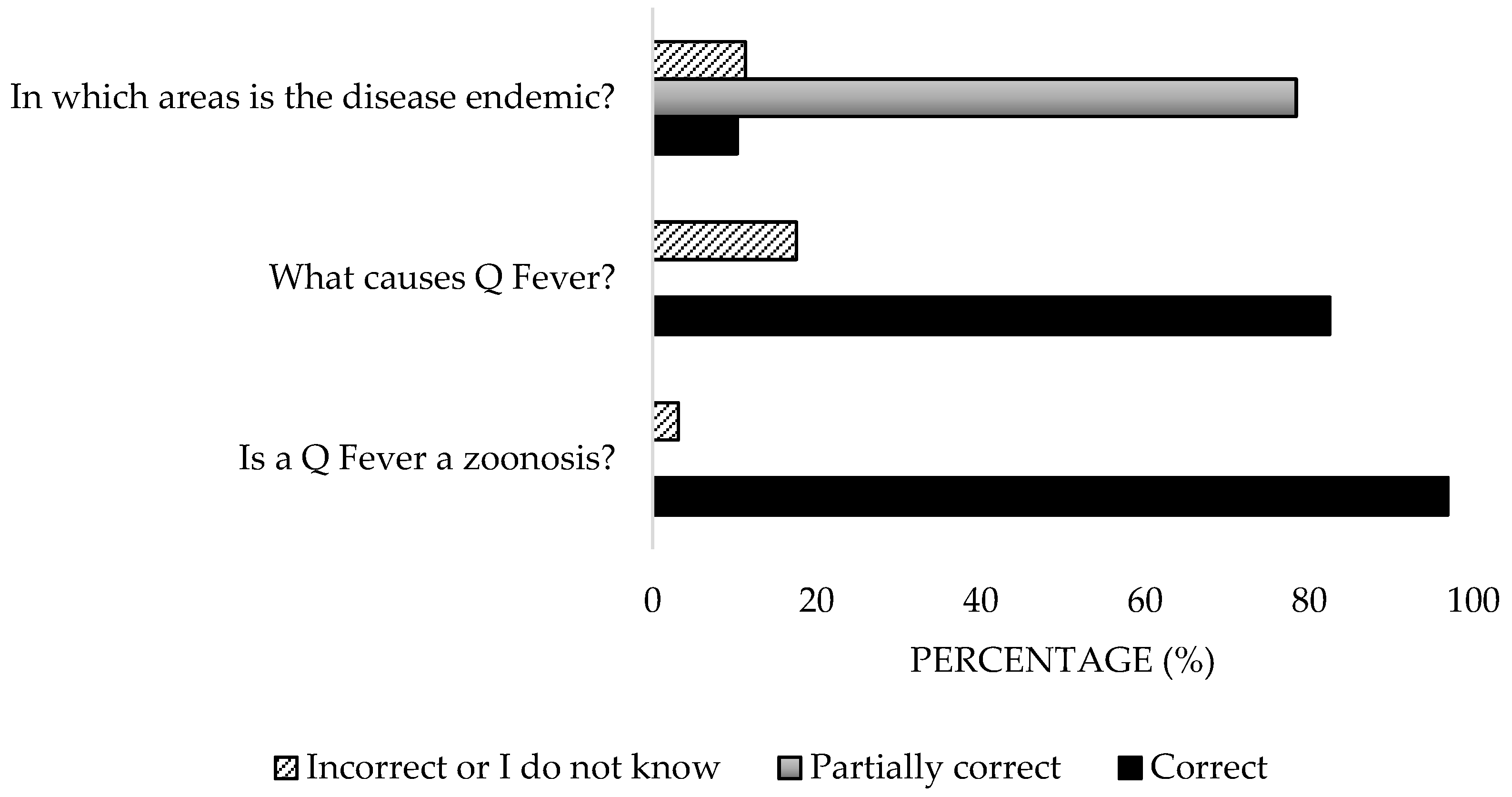
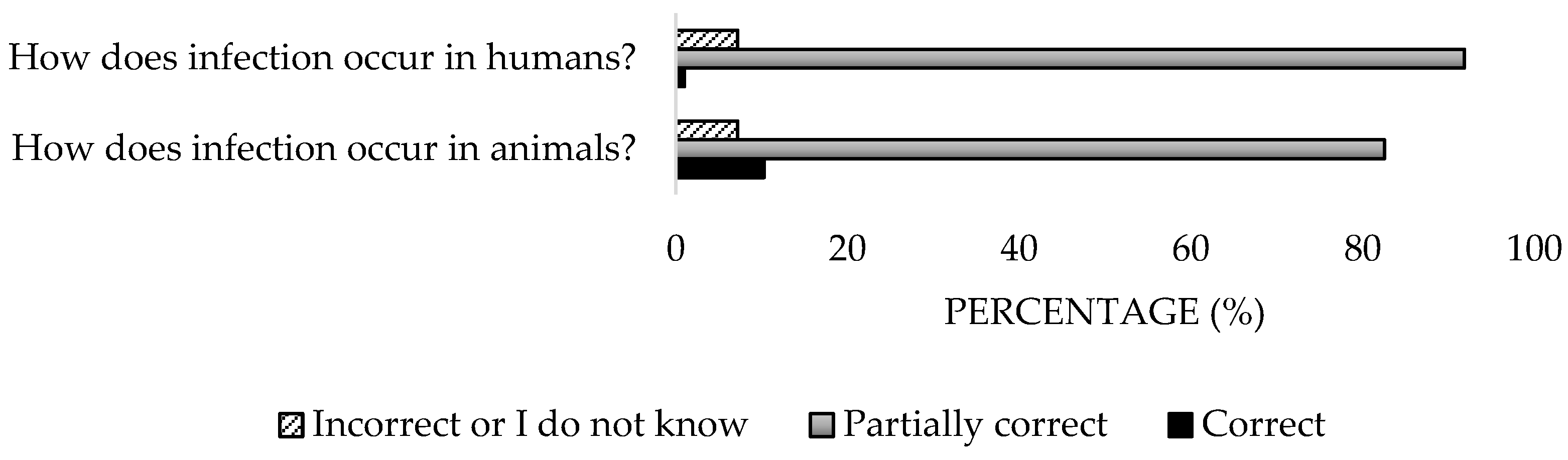
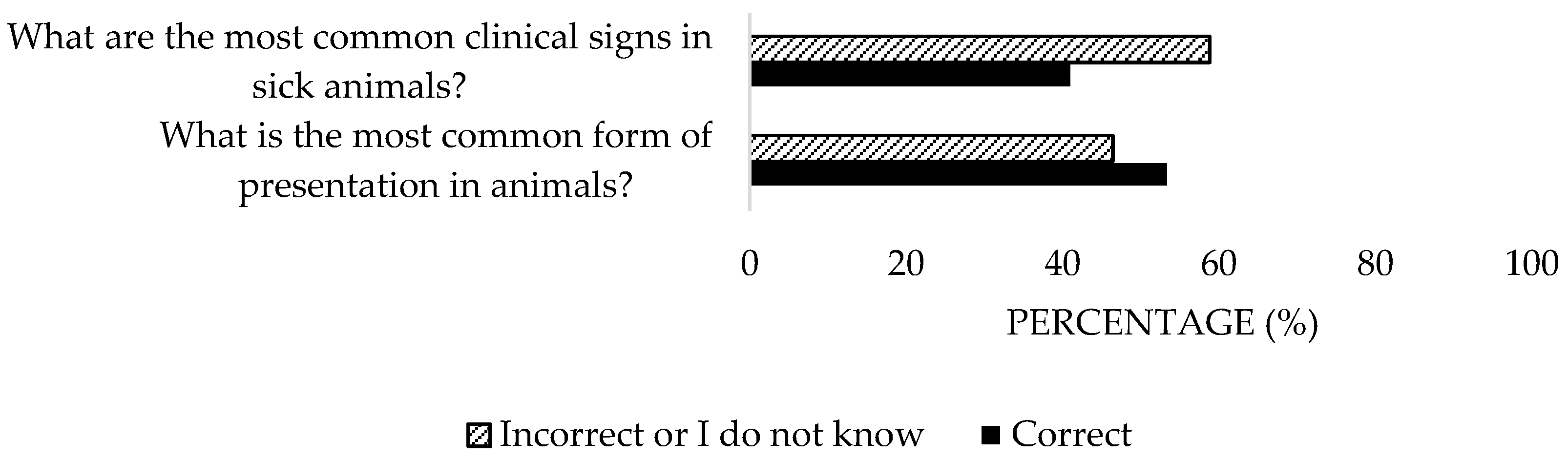
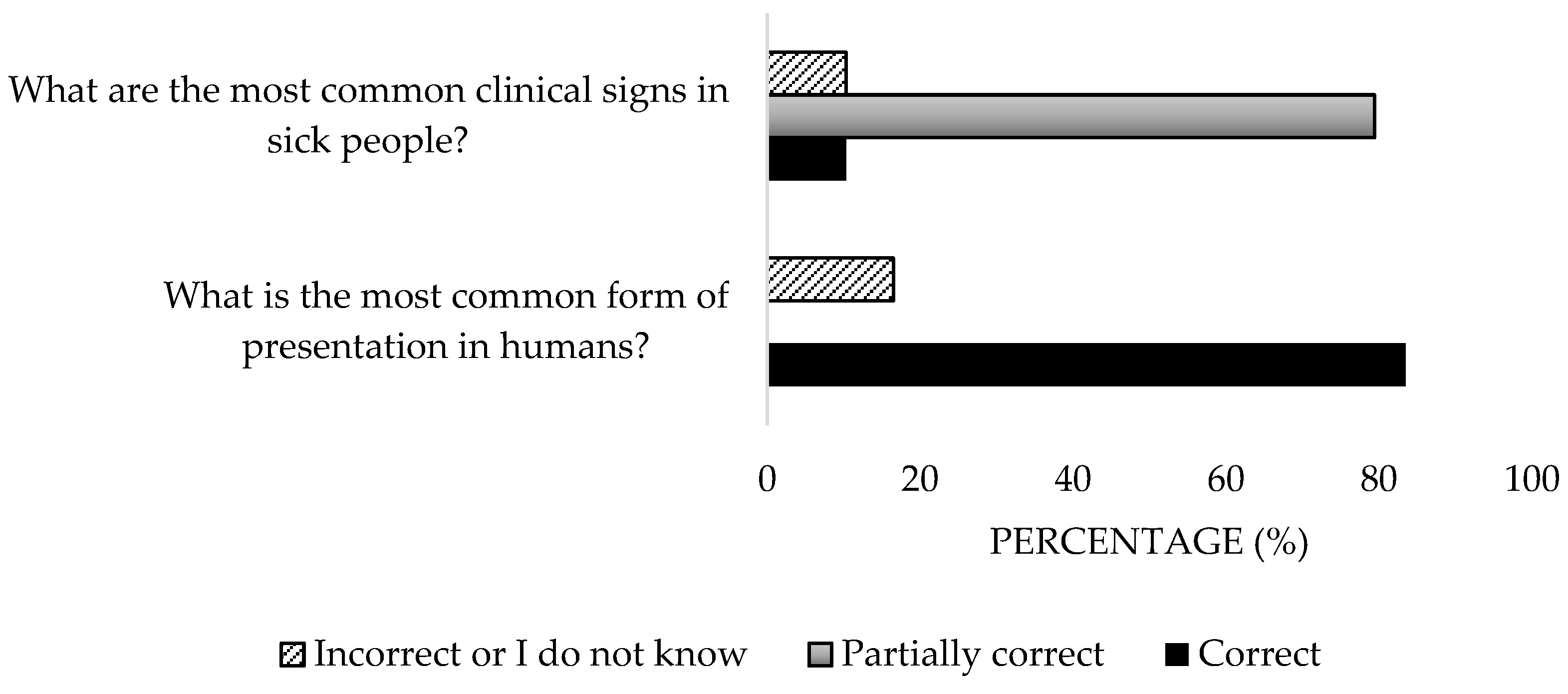
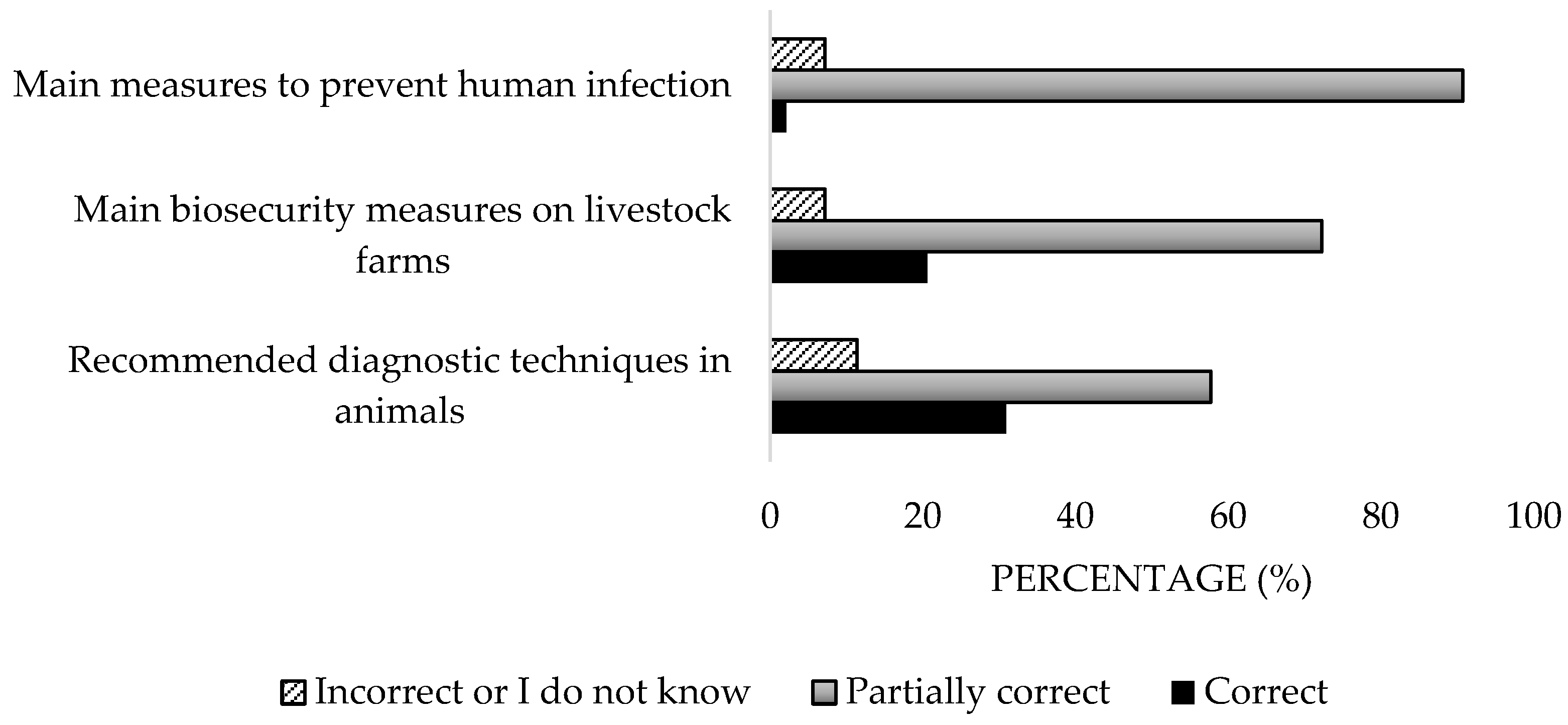
- General knowledge of the disease (14 items): etiology, epidemiology, clinical features, diagnosis, and prophylaxis.
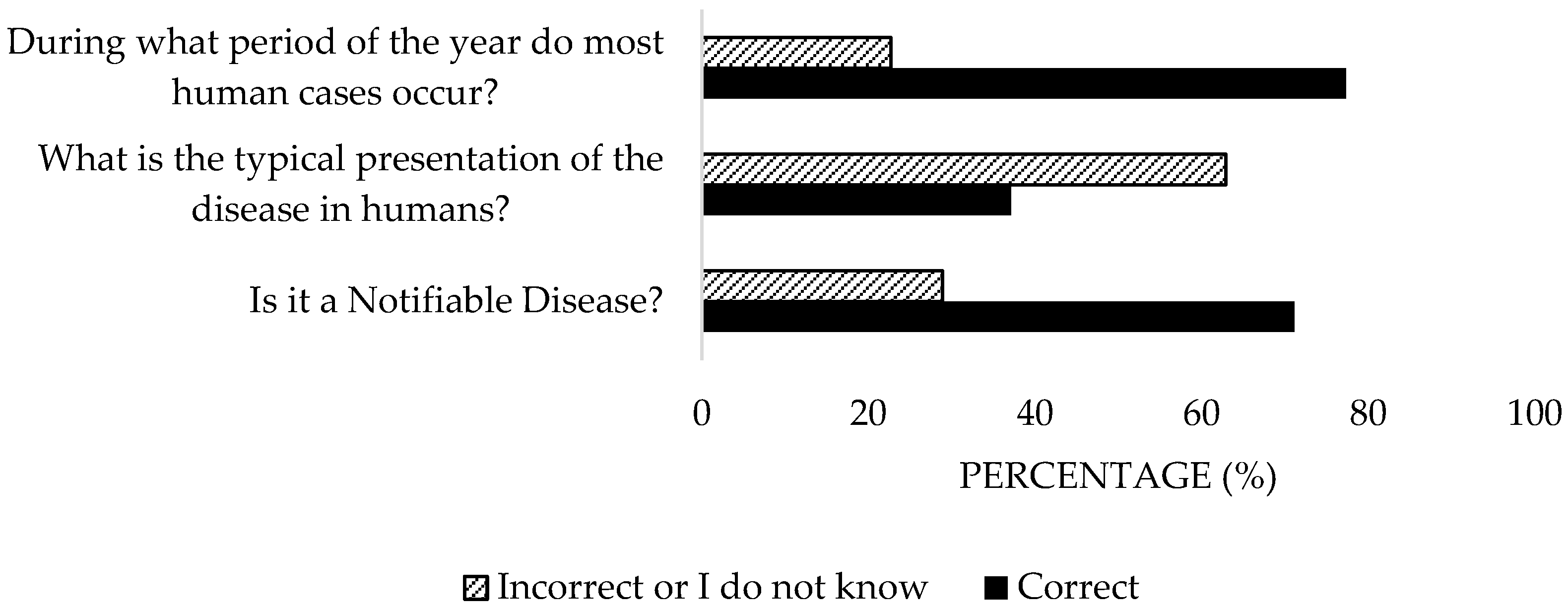
- Specific knowledge about the disease in Spain (3 items): aimed at assessing respondents’ understanding of presentation forms, seasonal presentation, and the mandatory reporting of cases.
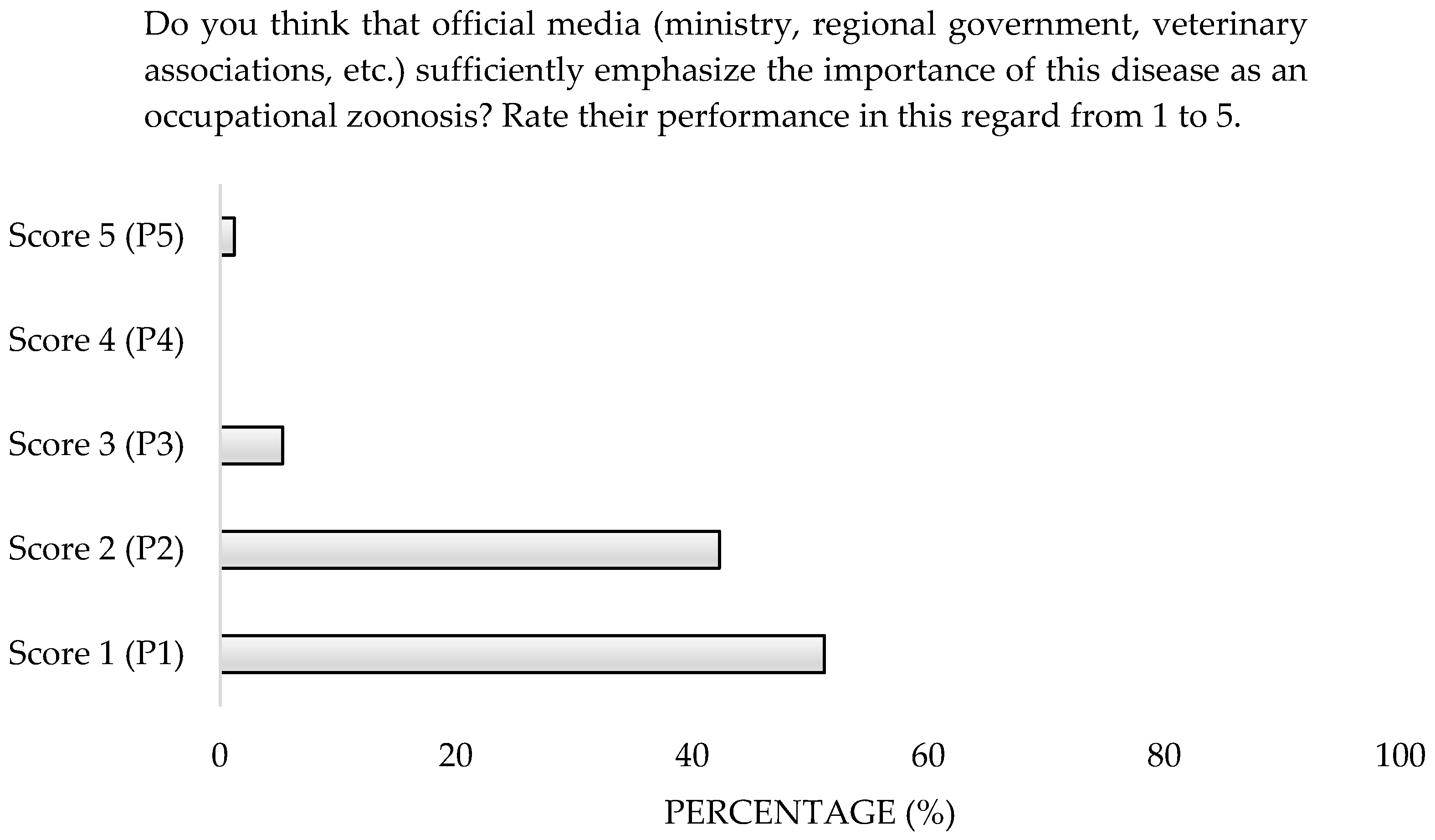
- Perception of Q Fever (4 items): multiple-choice, single-choice, and numerical rating scale (NRS from 1 to 5 points, with 1 representing the minimum value and 5 the maximum value regarding the availability of reliable information about Q Fever provided by official sources, such as the Ministries of Health and Agriculture.) questions, designed to evaluate participants’ opinions on their training, the quality of information sources, and the occupational zoonotic risk posed by this disease.
- Attitude toward Q Fever (7 items): single-choice and multiple-choice questions, aimed at evaluating attitudes toward the use of personal protective equipment (PPE) and preventive measures, vaccination, early diagnosis, and continued training about the disease.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation (WHO). One Health 2023. Available online: https://www.who.int/es/news-room/fact-sheets/detail/one-health (accessed on 30 April 2025).
- Zinsstag, J.; Schelling, E.; Waltner-Toews, D.; Tanner, M. From “One Medicine” to “One Health” and Systemic Approaches to Health and Well-Being. Prev. Vet. Med. 2011, 101, 148–156. [Google Scholar] [CrossRef]
- Sánchez, A.; Prats-Van Der Ham, M.; Tatay-Dualde, J.; García-Galán, A.; de la Fe, C.; Corrales, J.C.; Contreras, A. Zoonosis Y Salud Laboral En La Profesión Veterinaria [Zoonoses and Occupational Health in the Veterinary Profession]. Rev. Española De Salud Pública 2018, 92, e201812086. [Google Scholar] [PubMed] [PubMed Central]
- Arricau-Bouvery, N.; Rodolakis, A. Is Q Fever an Emerging or Re-emerging Zoonosis? Vet. Res. 2005, 36, 327–349. [Google Scholar] [CrossRef]
- Dupuis, G.; Petite, J.; Péter, O.; Vouilloz, M. An Important Outbreak of Human Q Fever in a Swiss Alpine Valley. Int. J. Epidemiol. 1987, 16, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Centro Europeo Para La Prevención Y El Control De Las Enfermedades (ECDC). Informe Epidemiológico Anual De Fiebre Q; ECDC: Solna, Sweden, 2019.
- Federation of Veterinarians of Europe (FVE). Survey of the Veterinary Profession in Europe 2023. Available online: https://fve.org/cms/wp-content/uploads/FVE-Survey-2023_updated-v3.pdf (accessed on 30 April 2025).
- Babudieri, B.; Moscovici, C. Experimental and Natural Infection of Birds by Coxiella burnetti. Nature 1952, 169, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Arellano, J.L.; Rodríguez, C.; Gutiérrez, C.; Rivero, B. Epidemiology of Q Fever in Spain. Rev. Española De Quimioter. 2018, 31, 386–405. [Google Scholar] [PubMed] [PubMed Central]
- Castro-Scholten, S.; Caballero-Gómez, J.; Martínez, R.; Nadales-Martín, B.J.; Cano-Terriza, D.; Jiménez-Martín, D.; Remesar, S.; Jiménez-Ruiz, S.; Gómez-Guillamón, F.; García-Bocanegra, I. Occurrence of Coxiella burnetii in Wild Lagomorphs and Their Ticks in Spanish Mediterranean Ecosystems. Zoonoses Public Health 2024, 71, 549–559. [Google Scholar] [CrossRef]
- Astorga, R.J.; Reguillo, L.; Hernández, M.; Cardoso-Toset, F.; Tarradas, C.; Maldonado, A.; Gómez- Laguna, J. Serosurvey On Schmallenberg Virus and Selected Ovine Reproductive Pathogens in Culled Ewes from Southern Spain. Transbound. Emerg. Dis. 2014, 61, 4–11. [Google Scholar] [CrossRef]
- Astorga, R.J.; Carvajal, A.; Maldonado, A.; Gordon, S.V.; Salas, R.; Gómez-Villamón, F.; Sánchez-Baro, A.; López-Sebastián, A. Influence of Cohabitation Between Domestic Goat (Capra aegagrus hircus) and Iberian Ibex (Capra pyrenaica hispanica) on Seroprevalence of Infectious Diseases. Europ. J. Wild. Dis. 2014, 60, 387–390. [Google Scholar] [CrossRef]
- Sidi-Boumedine, K.; Rousset, E.; Henning, K.; Ziller, M.; Niemczuck, K.; Roest, H.I.J.; Thiéry, R. Development of Harmonised Schemes for the Monitoring and Reporting of Q-Fever in Animals in the European Union. EFSA Support. Publ. 2010, 7, 48E. [Google Scholar] [CrossRef]
- Porter, S.R.; Czaplicki, G.; Mainil, J.; Guattéo, R.; Saegerman, C. Q Fever: Current State of Knowledge and Perspectives of Research of a Neglected Zoonosis. Int. J. Microbiol. 2011, 2011, 248418. [Google Scholar] [CrossRef] [PubMed]
- Van den Brom, R.; Van Engelen, E.; Roest, H.I.; Van der Hoek, W.; Vellema, P. Coxiella burnetii Infections in Sheep or Goats: An Opinionated Review. Vet. Microbiol. 2015, 181, 119–129. [Google Scholar] [CrossRef]
- Fariñas, M.T.; Collado, C.M. Infección Por Coxiella burnetii (Fiebre Q) [Infection by Coxiella burnetii (Q Fever)]. Enfermedades Infecc. Y Microbiol. Clínica 2010, 28, 29–32. [Google Scholar] [CrossRef]
- World Organization for Animal Health (WOAH). Manual of Terrestrial Animals 2018. Available online: https://www.oie.int/app/uploads/2021/03/3-01-16-q-fever-1.pdf (accessed on 30 April 2025).
- Boarbi, S.; Mori, M.; Rousset, E.; Sidi-Boumedine, K.; Van Esbroeck, M.; Fretin, D. Prevalence and Molecular Typing of Coxiella burnetii in Bulk Tank Milk in Belgian Dairy Goats, 2009–2013. Vet. Microbiol. 2014, 170, 117–124. [Google Scholar] [CrossRef]
- Valencia, M.D.S.; Rodríguez, C.O.; Punet, O.G.; Giral, I.D. Seroprevalencia De La Fiebre Q Y Factores De Riesgo Asociados En Estudiantes De La Facultad De Veterinaria De Zaragoza, España. Eur. J. Epidemiol. 2000, 16, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Meadows, S.L.; Jones-Bitton, A.; McEwen, S.A.; Jansen, J.; Patel, S.N.; Filejski, C.; Menzies, P. Prevalence and Risk Factors for Coxiella burnetii Seropositivity in Small Ruminant Veterinarians and Veterinary Students in Ontario, Canada. Can. Vet. J. 2017, 58, 397–399. [Google Scholar] [PubMed] [PubMed Central]
- Baker, W.S.; Gray, G.C. A Review of Published Reports Regarding Zoonotic Pathogen Infection in Veterinarians. J. Am. Vet. Med. Assoc. 2009, 234, 1271–1278. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Gac. Sanit. 2009, 23, 158.e1–158.e28. [Google Scholar] [CrossRef]
- Real Decreto 50/2024; Por El Que Se Modifican los Estatutos Generales de la Organización Colegial Veterinaria Española, Aprobados Por El Real Decreto 126/2013, De 22 De Febrero. 3 de Febrero de 2024. D.O. No. 2044. Available online: https://www.boe.es/eli/es/rd/2024/01/16/50 (accessed on 30 April 2025).
- Ministerio de Trabajo Y Economía Social (MITES). Guía De Buenas Prácticas Para Zoonosis De Origen Laboral (NTP411) 2018. Available online: https://www.insst.es/documentacion/colecciones-tecnicas/ntp-notas-tecnicas-de-prevencion/12-serie-ntp-numeros-401-a-435-ano-1997/ntp-411-zoonosis-de-origen-laboral (accessed on 30 April 2025).
- Filippitzi, M.E.; Goumperis, T.; Robinson, T.; Saegerman, C. Microbiological Zoonotic Emerging Risks, Transmitted Between Livestock Animals and Humans (2007–2015). Transbound. Emerg. Dis. 2017, 64, 1059–1070. [Google Scholar] [CrossRef] [PubMed]
- Epp, T.; Waldner, C. Occupational Health Hazards in Veterinary Medicine: Zoonoses and Other Biological Hazards. La Rev. Vet. Can. 2012, 53, 144–150. [Google Scholar] [PubMed] [PubMed Central]
- Jackson, J.; Villarroel, A. A Survey of the Risk of Zoonoses for Veterinarians. Zoonoses Public Health 2012, 59, 193–201. [Google Scholar] [CrossRef]
- Contreras, V.; González, M.; Guzmán, C.; Máttar, S. Fiebre Q: Una Zoonosis Olvidada En Colombia. Rev. Médica De Risaralda 2013, 19, 137–146. Available online: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0122-06672013000200007&lng=en (accessed on 30 April 2025).
- Instituto Nacional De Estadística (INE). Informe Sectorial De La Profesión Veterinaria En España 2020. Available online: https://www.ine.es/prodyser/pubweb/anuario20/anu20_completo.pdf (accessed on 30 April 2025).
- Bañuls, P.; Galán-Relaño, Á.; Romero-Salmoral, A.; Gómez-Gascón, L.; Tarradas, C.; Astorga Márquez, R.J.; Luque, I.; Huerta, B. Knowledge, Perception and Attitude About Crimean-Congo Haemorrhagic Fever (CCHF) Among Veterinary Students and Professionals of Spain. Comp. Immunol. Microbiol. Infect. Dis. 2024, 115, 102260. [Google Scholar] [CrossRef]
- Crist, S.D.; Kopsco, H.; Miller, A.; Gronemeyer, P.; Mateus-Pinilla, N.; Smith, R.L. Knowledge, Attitudes, and Practices of Veterinary Professionals Towards Ticks and Tick-Borne Diseases in Illinois. One Health 2022, 14, 100391. [Google Scholar] [CrossRef]
- Buhariwalla, F.; Cann, B.; Marrie, T.J. A Dog-Related Outbreak of Q Fever. Clin. Infect. Dis. 1996, 23, 753–755. [Google Scholar] [CrossRef]
- Sellens, E.; Norris, J.M.; Dhand, N.K.; Heller, J.; Hayes, L.; Gidding, H.F.; Willaby, H.; Wood, N.; Bosward, K.L. Q Fever Knowledge, Attitudes and Vaccination Status of Australia’s Veterinary Workforce in 2014. PLoS ONE 2016, 11, e0146819. [Google Scholar] [CrossRef] [PubMed]
- Winter, F.; Campe, A. Q Fever Expertise Among Human and Veterinary Health Professionals in Germany—A Stakeholder Analysis of Knowledge Gaps. PLoS ONE 2022, 17, e0264629. [Google Scholar] [CrossRef] [PubMed]
- Center for Food Security and Public Health (CFSPH) of Iowa State University. Q Fever; Center for Food Security and Public Health (CFSPH): Ames, IA, USA, 2007. [Google Scholar]
- Real Decreto 779/2023. Por El Que Se Establece La Comunicación De Enfermedades De Los Animales De Declaración Obligatoria y Se Regula Su Notificación. 25 de Octubre de 2023. D.O. No. 21844. Available online: https://www.boe.es/eli/es/rd/2023/10/10/779/con (accessed on 30 April 2025).
- Ministerio de Agricultura, Pesca Y Alimentación (MAPA). Informe De Zoonosis 2022. Available online: https://www.mapa.gob.es/es/ganaderia/temas/sanidad-animal-higiene-ganadera/informezoonosis2022_tcm30-684580.pdf (accessed on 30 April 2025).
- Whelan, J.; Schimmer, B.; Schneeberger, P.; Meekelenkamp, J.; Ijff, A.; Van Der Hoek, W.; van Beest Holle, D.R. Fiebre Q En Trabajadores De Sacrificio, Países Bajos, 2009–2010. Emerg. Infect. Dis. 2011, 17, 1719–1723. [Google Scholar] [CrossRef] [PubMed]
- Khamassi-Khbou, M.; Daaloul-Jedidi, M.; Bouaicha-Zaafouri, F.; Benzarti, M.H. Coronaviruses in Farm Animals: Epidemiology and Public Health Implications. Vet. Med. Sci. 2021, 7, 322–347. [Google Scholar] [CrossRef]
- Biosecurity Working Group. Biosecurity Standard Operating Procedures (SOP) Applied to the Faculty of Veterinary Medicine of the University of Liège (FVM) 2019. Available online: https://www2.fmv.ulg.ac.be/actualites/Biosecurity_Manual_Final_6Jan10.pdf (accessed on 30 April 2025).
- Fariñas-Guerrero, F.; Astorga-Márquez, R.J. Zoonosis Transmitidas Por Animales De Compañía. Una Guía De Consulta Para El Profesional Sanitario. Zaragoza (España); Amazing Books: Zaragoza, Spain, 2019; ISBN 978-84-17403-32-4. [Google Scholar]
- Vega-García, S.; Astorga-Márquez, R.J. Virus Del Nilo Occidental. ¿Estamos Preparados? Una Perspectiva One Health; Editorial Amazing Books: Zaragoza, Spain, 2020; ISBN 978-84-17403-75-1. [Google Scholar]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Pérez, F.; Astorga-Márquez, R.J.; Galán-Relaño, Á.; Tarradas-Iglesias, C.; Luque-Moreno, I.; Gómez-Gascón, L.; De Luque-Ibáñez, J.A.; Huerta-Lorenzo, B. Knowledge, Perception, and Attitude of Veterinarians About Q Fever from South Spain. Microorganisms 2025, 13, 1759. https://doi.org/10.3390/microorganisms13081759
Pérez-Pérez F, Astorga-Márquez RJ, Galán-Relaño Á, Tarradas-Iglesias C, Luque-Moreno I, Gómez-Gascón L, De Luque-Ibáñez JA, Huerta-Lorenzo B. Knowledge, Perception, and Attitude of Veterinarians About Q Fever from South Spain. Microorganisms. 2025; 13(8):1759. https://doi.org/10.3390/microorganisms13081759
Chicago/Turabian StylePérez-Pérez, Francisco, Rafael Jesús Astorga-Márquez, Ángela Galán-Relaño, Carmen Tarradas-Iglesias, Inmaculada Luque-Moreno, Lidia Gómez-Gascón, Juan Antonio De Luque-Ibáñez, and Belén Huerta-Lorenzo. 2025. "Knowledge, Perception, and Attitude of Veterinarians About Q Fever from South Spain" Microorganisms 13, no. 8: 1759. https://doi.org/10.3390/microorganisms13081759
APA StylePérez-Pérez, F., Astorga-Márquez, R. J., Galán-Relaño, Á., Tarradas-Iglesias, C., Luque-Moreno, I., Gómez-Gascón, L., De Luque-Ibáñez, J. A., & Huerta-Lorenzo, B. (2025). Knowledge, Perception, and Attitude of Veterinarians About Q Fever from South Spain. Microorganisms, 13(8), 1759. https://doi.org/10.3390/microorganisms13081759