
Primary Cutaneous Nocardiosis (Lymphangitic Type) in an Immunocompetent Patient: A Case Report

 , , , and
, , , and 
{kind=link}
{kind=link}
Abstract
1. Introduction
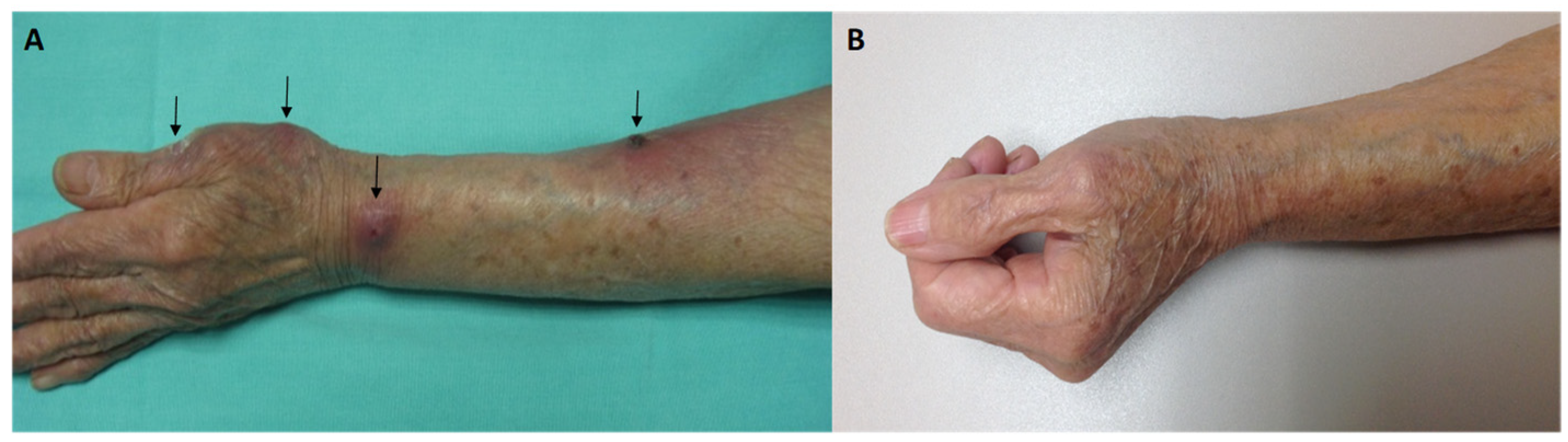
2. Case Report
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, J.W. Nocardiosis: Updates and clinical overview. Mayo Clin. Proc. 2012, 87, 403–407. [Google Scholar] [CrossRef]
- You, Y.; Chen, W.; Zhong, B.; Song, Z.; Yang, X. Disseminated nocardiosis caused by Nocardia elegans: A case report and review of the literature. Infection 2018, 46, 705–710. [Google Scholar] [CrossRef]
- Kumar, T.S.; Scott, J.X.; Viswanathan, S. Cervicofacial nocardiosis in an immunocompetent child. Acta Paediatr. 2005, 94, 1342–1343. [Google Scholar] [CrossRef]
- Ercibengoa, M.; Vicente, D.; Arranz, L.; Ugarte, A.; Marimon, J. Primary cutaneous Nocardia brasiliensis in a Spanish child. Clin. Lab. 2018, 64, 1769–1772. [Google Scholar] [CrossRef]
- Fatahi-Bafghi, M. Nocardiosis from 1888 to 2017. Microb. Pathog. 2018, 114, 369–384. [Google Scholar] [CrossRef]
- Agterof, M.; van der Bruggen, T.; Tersmette, M.; ter Borg, E.; van den Bosch, J.; Biesma, D. Nocardiosis: A case series and a mini review of clinical and microbiological features. Neth. J. Med. 2007, 65, 199–202. [Google Scholar]
- Sonneville, R.; Ruimy, R.; Benzonana, N. An update on bacterial brain abscess in immunocompetent patients. Clin. Microbiol. Infect. 2017, 23, 614–620. [Google Scholar] [CrossRef]
- Mazzaferri, F.; Cordioli, M.; Segato, E. Nocardia infection over 5 years (2011–2015) in an Italian tertiary care hospital. New Microbiol. 2018, 41, 136–140. [Google Scholar]
- Dodiuk-Gad, R.; Cohen, E.; Ziv, M.; Goldstein, L.H.; Chazan, B.; Shafer, J.; Sprecher, H.; Elias, M.; Keness, Y.; Rozenman, D. Cutaneous nocardiosis: Report of two cases and review of the literature. Int. J. Dermatol. 2010, 49, 1380–1385. [Google Scholar] [CrossRef]
- Hu, M.; Bao, F.; Zhang, F. Primary Cutaneous Nocardiosis. JAMA Dermatol. 2024, 160, 1237–1238. [Google Scholar] [CrossRef]
- Ambrosioni, J.; Lew, D.; Garbino, J. Nocardiosis: Updated clinical review and experience at a tertiary center. Infection. 2010, 38, 89–97. [Google Scholar] [CrossRef]
- Sharmila, P.; Manjyot, M.G.; Avani, A.; Kaleem, J. Primary cutaneous nocardiosis with craniocerebral extension: A case report. Dermatol. Online J. 2010, 15, 8. [Google Scholar]
- Fukuda, H.; Saotome, A.; Usami, N.; Urushibata, O.; Mukai, H. Lymphocutaneous type of nocardiosis caused by Nocardia brasiliensis: A case report and review of primary cutaneous nocardiosis caused by N. brasiliensis reported in Japan. J. Dermatol. 2008, 35, 346–353. [Google Scholar] [CrossRef]
- Iotti, L.R.; de Frutos, M.; Lorenzo-Vidal, B.; Eiros, J.M. Nocardiosis diseminada [Disseminated nocardiosis]. Rev. Esp. Quimioter. 2024, 37, 180–182. [Google Scholar] [CrossRef]
- Besteiro, B.; Coutinho, D.; Fragoso, J.; Figueiredo, C.; Nunes, S.; Azevedo, C.; Teixeira, T.; Selaru, A.; Abreu, G.; Malheiro, L. Nocardiosis: A single-center experience and literature review. Braz. J. Infect. Dis. 2023, 27, 102806. [Google Scholar] [CrossRef]
- Duggal, S.D.; Chugh, T.D. Nocardiosis: A Neglected Disease. Med. Princ. Pract. 2020, 29, 514–523. [Google Scholar] [CrossRef]
- Brown-Elliot, B.A.; Brown, J.M.; Conville, P.S.; Wallace, R.J., Jr. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin. Microbiol. Rev. 2006, 19, 259–282. [Google Scholar] [CrossRef]
- Ameen, M.; Arenas, R.; Vasquez del Mercado, E.; Fernandez, R.; Torres, E.; Zacarias, R. Efficacy of imipenem therapy for Nocardia actinomycetomas refractory to sulfonamides. J. Am. Acad. Dermatol. 2010, 62, 239–246. [Google Scholar] [CrossRef]
- Pujol-Montcus, J.A.; Pastor-Jane, L.; Simo-Esque, M.; Diaz, M.L.; Turegano-Fuentes, P. Primary cutaneous nocardiosis caused by Nocardia transvalensis in an immunocompetent patient. J. Am. Acad. Dermatol. 2011, 64, P2313. [Google Scholar] [CrossRef]
- Ramos-E-Silva, M.; Lopes, R.S.; Trope, B.M. Cutaneous nocardiosis: A great imitator. Clin. Dermatol. 2020, 38, 152–159. [Google Scholar] [CrossRef]
- Songo, A.; Jacquier, H.; Danjean, M.; Compain, F.; Dorchène, D.; Edoo, Z.; Woerther, P.L.; Arthur, M.; Lebeaux, D. Analysis of two Nocardia brasiliensis class A β-lactamases (BRA-1 and BRS-1) and related resistance to β-lactam antibiotics. Glob. Antimicrob. Resist. 2025, 42, 135–141. [Google Scholar] [CrossRef]
- Muñoz, J.; Mirelis, B.; Aragón, L.M.; Gutiérrez, N.; Sánchez, F.; Español, M.; Esparcia, O.; Gurguí, M.; Domingo, P.; Coll, P. Clinical and microbiological features of nocardiosis 1997–2003. J. Med. Microbiol. 2007, 56, 545–550. [Google Scholar] [CrossRef]
- Li, S.; Xu, X.; Wu, M.; Zhu, J.; Cen, P.; Ding, J.; Wu, S.; Jin, J. Lymphocutaneous nocardiosis caused by Nocardia brasiliensis in an immunocompetent patient: A case report. J. Int. Med. Res. 2020, 48, 300060519897690. [Google Scholar] [CrossRef]
- Chu, L.; Xu, X.; Ran, Y. Primary cutaneous nocardiosis caused by Nocardia brasiliensis following a wasp sting. Clin. Exp. Dermatol. 2017, 42, 416–419. [Google Scholar] [CrossRef]
- Martínez-Ortega, J.I.; Franco-Gonzalez, S.; Ramirez Cibrian, A.G. An immune-based therapeutical approach in an elderly patient with fixed cutaneous sporotrichosis. Cureus 2024, 16, e53192. [Google Scholar] [CrossRef]
- Smego, R.A., Jr.; Castiglia, M.; Asperilla, M.O. Lymphocutaneous syndrome. A review of non-sporothrix causes. Medicine 1999, 78, 38–63. [Google Scholar] [CrossRef]
- Zhao, P.; Zhang, X.; Du, P.; Li, G.; Li, L.; Li, Z. Susceptibility profiles of Nocardia spp. to antimicrobial and antituberculotic agents detected by a microplate Alamar Blue assay. Sci. Rep. 2017, 7, 43660. [Google Scholar] [CrossRef]
- Traxler, R.M.; Bell, M.E.; Lasker, B.; Headd, B.; Shieh, W.J.; McQuiston, J.R. Updated review on Nocardia species: 2006–2021. Clin. Microbiol. Rev. 2022, 35, e0002721. [Google Scholar] [CrossRef]
- Conville, P.S.; Brown-Elliott, B.A.; Smith, T.; Zelazny, A.M. The Complexities of Nocardia Taxonomy and Identification. J. Clin. Microbiol. 2017, 56, e01419-17. [Google Scholar] [CrossRef]
- Liu, Y.; Wu, S.Y.; Deng, J.; Zhuang, K.W.; Tang, Y.; Wu, N.; Zhang, W.L.; Liao, Q.F.; Xiao, Y.L.; Kang, M. Application of MALDI-TOF mass spectrometry for identification of Nocardia species. BMC Microbiol. 2024, 24, 358. [Google Scholar] [CrossRef]
- Margalit, I.; Lebeaux, D.; Tishler, O.; Goldberg, E.; Bishara, J.; Yahav, D.; Coussement, J. How do I manage nocardiosis? Clin. Microbiol. Infect. 2021, 27, 550–558. [Google Scholar] [CrossRef]
- Bonifaz, A.; García-Sotelo, R.S.; Lumbán-Ramirez, F.; Vázquez-González, D.; Inclán-Reyes, J.I.; Sierra-Garduño, M.E.; Araiza, J.; Chandler, D. Update on actinomycetoma treatment: Linezolid in the treatment of actinomycetomas due to Nocardia spp. and Actinomadura madurae resistant to conventional treatments. Expert. Rev. Anti. Infect. Ther. 2025, 23, 79–89. [Google Scholar] [CrossRef]
- Xu, X.; Liu, Z.; Xia, X. Acute primary cutaneous nocardiosis. Am. J. Trop. Med. Hyg. 2024, 110, 848–849. [Google Scholar] [CrossRef]
- Wang, C.; Sun, Q.; Yan, J.; Liao, X.; Long, S.; Zheng, M.; Zhang, Y.; Yang, X.; Shi, G.; Zhao, Y.; et al. The species distribution and antimicrobial resistance profiles of Nocardia species in China: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2023, 17, e0011432. [Google Scholar] [CrossRef]
- Attias, N.H.; Schlaeffer-Yosef, T.; Zahavi, I.; Hasson, N.; Ari, Y.B.; Darawsha, B.; Levitan, I.; Goldberg, E.; Landes, M.; Litchevsky, V.; et al. Shorter vs. standard-duration antibiotic therapy for nocardiosis: A multi-center retrospective cohort study. Infection 2024. [Google Scholar] [CrossRef]
- Silva, R.A.; Young, R.; Sridhar, J.; Nocardia Study Group. Nocardia choroidal abscess: Risk factors, treatment strategies, and visual outcomes. Retina 2015, 35, 2137–2146. [Google Scholar] [CrossRef]
- Acevedo, C.T.; Imkamp, F.; Marques Maggio, E.; Brugger, S.D. Primary cutaneous nocardiosis of the head and neck in an immunocompetent patient. BMJ Case Rep. 2021, 14, e241217. [Google Scholar] [CrossRef]
- Ji, Y.; Su, F.; Hong, X.; Chen, M.; Zhu, Y.; Cheng, D.; Ge, Y. Successful treatment with amoxicillin-clavulanic acid: Cutaneous nocardiosis caused by Nocardia brasiliensis. J. Dermatolog. Treat. 2023, 34, 2229467. [Google Scholar] [CrossRef]
- Pai, S.; Pai, K.; Sharma, S. Cutaneous nocardiosis: An underdiagnosed pathogenic infection. BMJ Case Rep. 2015, 2015, bcr2014208713. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguilar-Molina, H.; Toussaint-Caire, S.; Arenas, R.; Xicohtencatl-Cortes, J.; Martínez-Chavarría, L.C.; Hernández-Castro, R.; Rodriguez-Cerdeira, C. Primary Cutaneous Nocardiosis (Lymphangitic Type) in an Immunocompetent Patient: A Case Report. Microorganisms 2025, 13, 1022. https://doi.org/10.3390/microorganisms13051022
Aguilar-Molina H, Toussaint-Caire S, Arenas R, Xicohtencatl-Cortes J, Martínez-Chavarría LC, Hernández-Castro R, Rodriguez-Cerdeira C. Primary Cutaneous Nocardiosis (Lymphangitic Type) in an Immunocompetent Patient: A Case Report. Microorganisms. 2025; 13(5):1022. https://doi.org/10.3390/microorganisms13051022
Chicago/Turabian StyleAguilar-Molina, Hilayali, Sonia Toussaint-Caire, Roberto Arenas, Juan Xicohtencatl-Cortes, Luary C. Martínez-Chavarría, Rigoberto Hernández-Castro, and Carmen Rodriguez-Cerdeira. 2025. "Primary Cutaneous Nocardiosis (Lymphangitic Type) in an Immunocompetent Patient: A Case Report" Microorganisms 13, no. 5: 1022. https://doi.org/10.3390/microorganisms13051022
APA StyleAguilar-Molina, H., Toussaint-Caire, S., Arenas, R., Xicohtencatl-Cortes, J., Martínez-Chavarría, L. C., Hernández-Castro, R., & Rodriguez-Cerdeira, C. (2025). Primary Cutaneous Nocardiosis (Lymphangitic Type) in an Immunocompetent Patient: A Case Report. Microorganisms, 13(5), 1022. https://doi.org/10.3390/microorganisms13051022