_Di_Marco.png)
A Potential Link Between Oral Microbiota and Female Reproductive Health



Abstract
1. Introduction
2. Oral Health and Pregnancy Outcomes
3. Oral Dysbiosis and Fertility Disorders
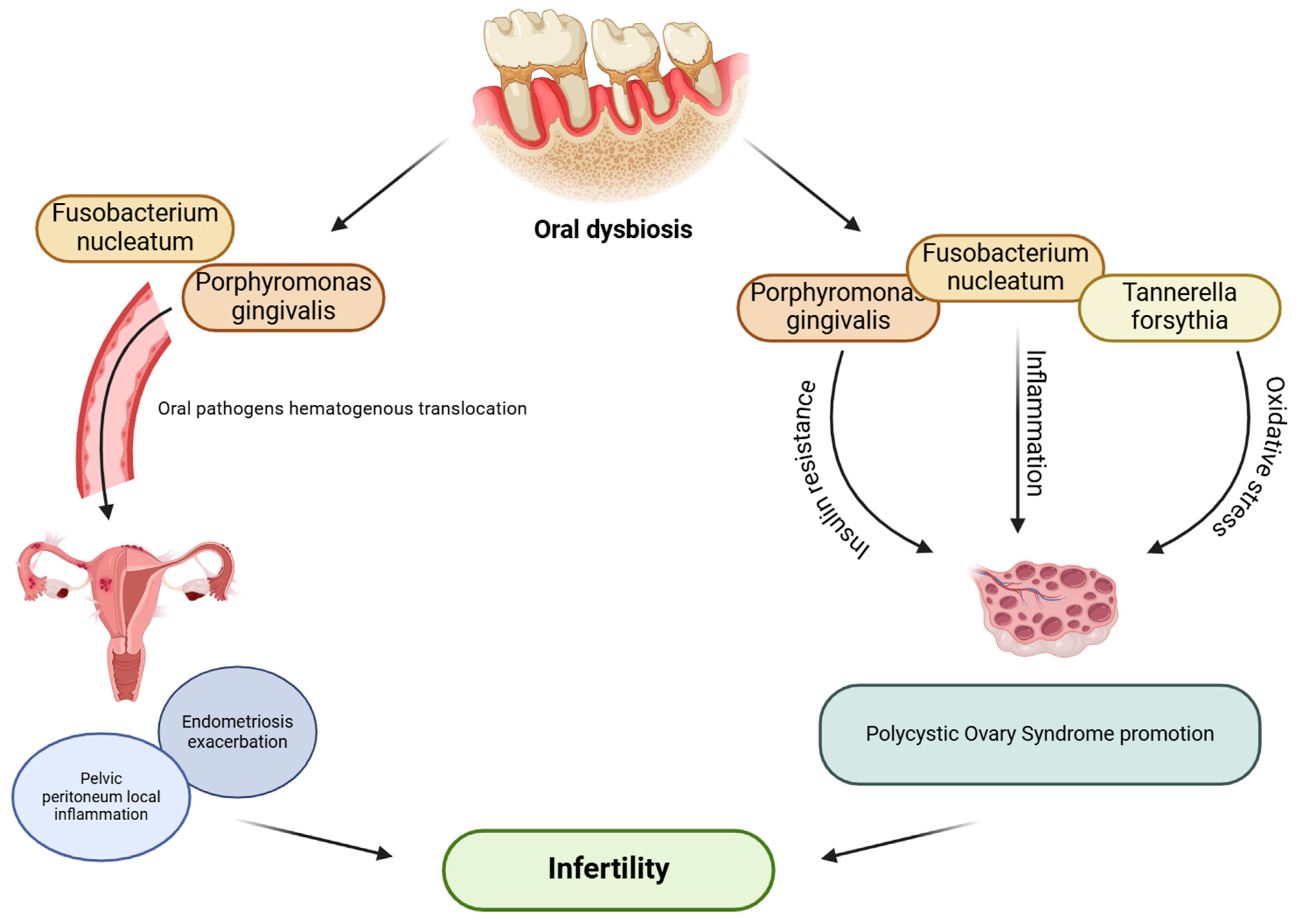
3.1. Polycystic Ovary Syndrome
3.2. Endometriosis
4. Probiotics Administration in Fertility Disorders
5. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.R.; Yu, W.-H.; Lakshmanan, A.; Wade, W.G. The Human Oral Microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [PubMed]
- Kaan, A.M.M.; Kahharova, D.; Zaura, E. Acquisition and Establishment of the Oral Microbiota. Periodontol. 2000 2021, 86, 123–141. [Google Scholar] [CrossRef] [PubMed]
- Radaic, A.; Kapila, Y.L. The Oralome and Its Dysbiosis: New Insights into Oral Microbiome-Host Interactions. Comput. Struct. Biotechnol. J. 2021, 19, 1335–1360. [Google Scholar] [CrossRef]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. D efining the Normal Bacterial Flora of the Oral Cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef]
- Gibbons, R.J.; Houte, J.V. Bacterial adherence in oral microbial ecology. Annu. Rev. Microbiol. 1975, 29, 19–42. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L. Microbial Complexes in Subgingival Plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Smith, C.; Martin, L.; Haffajee, J.A.; Uzel, N.G.; Goodson, J.M. Use of Checkerboard DNA–DNA Hybridization to Study Complex Microbial Ecosystems. Oral Microbiol. Immunol. 2004, 19, 352–362. [Google Scholar] [CrossRef]
- Socransky, S.S.; Manganiello, S.D. The Oral Microbiota of Man from Birth to Senility. J. Periodontol. 1971, 42, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, K.; Chen, T.; Paster, B. A Practical Guide to the Oral Microbiome and Its Relation to Health and Disease. Oral Dis. 2017, 23, 276–286. [Google Scholar] [CrossRef]
- Sun, J.; Buys, N. Effects of Probiotics Consumption on Lowering Lipids and CVD Risk Factors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann. Med. 2015, 47, 430–440. [Google Scholar] [CrossRef]
- Genco, R.J.; Borgnakke, W.S. Risk Factors for Periodontal Disease. Periodontol. 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- Slots, J. Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis in Periodontal Disease: Introduction. Periodontol. 2000 1999, 20, 7–13. [Google Scholar] [CrossRef]
- Kinney, J.S.; Morelli, T.; Braun, T.; Ramseier, C.A.; Herr, A.E.; Sugai, J.V.; Shelburne, C.E.; Rayburn, L.A.; Singh, A.K.; Giannobile, W.V. Saliva/Pathogen Biomarker Signatures and Periodontal Disease Progression. J. Dent. Res. 2011, 90, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhao, Y.; Lalsiamthara, J.; Peng, Y.; Qi, L.; Deng, S.; Wang, Q. Current Research Progress on Prevotella Intermedia and Associated Diseases. Crit. Rev. Microbiol. 2024, 1–18, epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A. Virulence Mechanisms of Tannerella Forsythia: Virulence Mechanisms of Tannerella Forsythia. Periodontol. 2000 2010, 54, 106–116. [Google Scholar] [CrossRef]
- Mohanty, R.; Asopa, S.; Joseph, M.D.; Singh, B.; Rajguru, J.; Saidath, K.; Sharma, U. Red Complex: Polymicrobial Conglomerate in Oral Flora: A Review. J. Fam. Med. Prim. Care 2019, 8, 3480. [Google Scholar] [CrossRef]
- Tanner, A.C.R.; Kressirer, C.A.; Rothmiller, S.; Johansson, I.; Chalmers, N.I. The Caries Microbiome: Implications for Reversing Dysbiosis. Adv. Dent. Res. 2018, 29, 78–85. [Google Scholar] [CrossRef]
- Becker, M.R.; Paster, B.J.; Leys, E.J.; Moeschberger, M.L.; Kenyon, S.G.; Galvin, J.L.; Boches, S.K.; Dewhirst, F.E.; Griffen, A.L. Molecular Analysis of Bacterial Species Associated with Childhood Caries. J. Clin. Microbiol. 2002, 40, 1001–1009. [Google Scholar] [CrossRef]
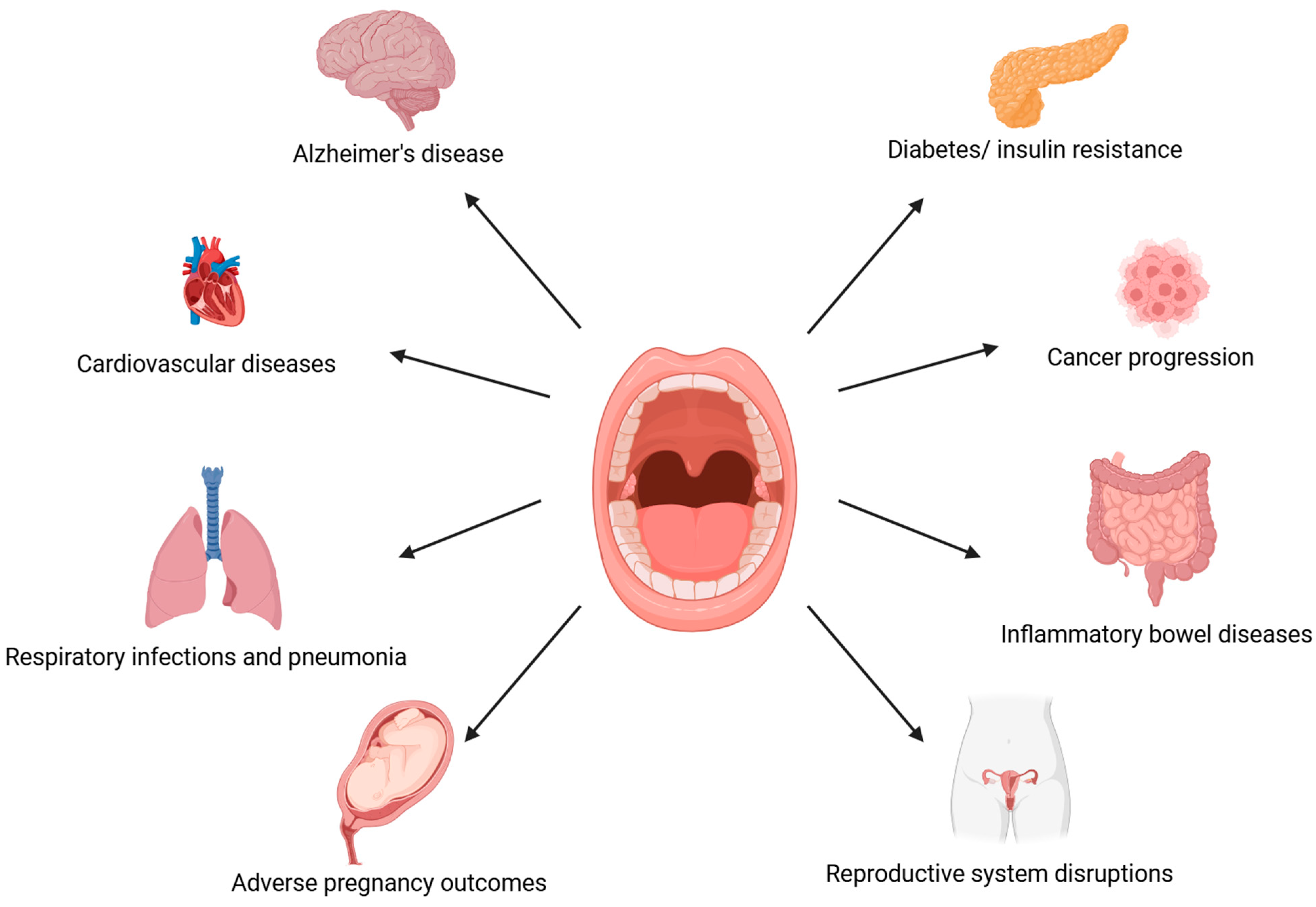
- Pisano, M. Oral Dysbiosis and Systemic Diseases: A Two-Way Relationship? Medicina 2023, 59, 1933. [Google Scholar] [CrossRef]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease—Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef]
- Lan, Z.; Liu, W.-J.; Cui, H.; Zou, K.-L.; Chen, H.; Zhao, Y.-Y.; Yu, G.-T. The Role of Oral Microbiota in Cancer. Front. Microbiol. 2023, 14, 1253025. [Google Scholar] [CrossRef] [PubMed]
- Maitre, Y.; Mahalli, R.; Micheneau, P.; Delpierre, A.; Amador, G.; Denis, F. Evidence and Therapeutic Perspectives in the Relationship between the Oral Microbiome and Alzheimer’s Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11157. [Google Scholar] [CrossRef] [PubMed]
- Singhrao, S.K.; Harding, A. Is Alzheimer’s Disease a Polymicrobial Host Microbiome Dysbiosis? Expert Rev. Anti Infect. Ther. 2020, 18, 275–277. [Google Scholar] [CrossRef]
- Wan, J.; Fan, H. Oral Microbiome and Alzheimer’s Disease. Microorganisms 2023, 11, 2550. [Google Scholar] [CrossRef]
- Shi, Q.; Zhang, B.; Xing, H.; Yang, S.; Xu, J.; Liu, H. Patients with Chronic Obstructive Pulmonary Disease Suffer from Worse Periodontal Health—Evidence from a Meta-Analysis. Front. Physiol. 2018, 9, 33. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, S.; Harish, Y.; Hiremath, S.; Puranik, M. A Cross-Sectional Survey to Study the Relationship of Periodontal Disease with Cardiovascular Disease, Respiratory Disease, and Diabetes Mellitus. J. Indian Soc. Periodontol. 2016, 20, 446. [Google Scholar] [CrossRef]
- Larvin, H.; Kang, J.; Aggarwal, V.R.; Pavitt, S.; Wu, J. Risk of Incident Cardiovascular Disease in People with Periodontal Disease: A Systematic Review and Meta-analysis. Clin. Exp. Dent. Res. 2021, 7, 109–122. [Google Scholar] [CrossRef]
- Zhang, Y.; Qiao, D.; Chen, R.; Zhu, F.; Gong, J.; Yan, F. The Association between Periodontitis and Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Chen, X.; Sun, B.; Li, L.; Sun, Z.; Zhu, X.; Zhong, X.; Xu, Y. The Oral Microbiome Analysis Reveals the Similarities and Differences between Periodontitis and Crohn’s Disease-Associated Periodontitis. FEMS Microbiol. Lett. 2022, 369, fnac054. [Google Scholar] [CrossRef]
- Bahekar, A.A.; Singh, S.; Saha, S.; Molnar, J.; Arora, R. The Prevalence and Incidence of Coronary Heart Disease Is Significantly Increased in Periodontitis: A Meta-Analysis. Am. Heart J. 2007, 154, 830–837. [Google Scholar] [CrossRef]
- Dekel, N.; Gnainsky, Y.; Granot, I.; Racicot, K.; Mor, G. The Role of Inflammation for a Successful Implantation. Am. J. Reprod. Immunol. 2014, 72, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Nwhator, S.; Opeodu, O.; Ayanbadejo, P.; Umeizudike, K.; Olamijulo, J.; Alade, G.; Agbelusi, G.; Arowojolu, M.; Sorsa, T. Could Periodontitis Affect Time to Conception? Ann. Med. Health Sci. Res. 2014, 4, 817. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.; Doherty, D.A.; Pennell, C.E.; Newnham, I.A.; Newnham, J.P. Periodontal Disease: A Potential Modifiable Risk Factor Limiting Conception. Hum. Reprod. 2012, 27, 1332–1342. [Google Scholar] [CrossRef]
- Paju, S.; Oittinen, J.; Haapala, H.; Asikainen, S.; Paavonen, J.; Pussinen, P.J. Porphyromonas gingivalis May Interfere with Conception in Women. J. Oral Microbiol. 2017, 9, 1330644. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Magon, N. Hormones in Pregnancy. Niger. Med. J. 2012, 53, 179. [Google Scholar] [CrossRef]
- Mesa, M.D.; Loureiro, B.; Iglesia, I.; Fernandez Gonzalez, S.; Llurba Olivé, E.; García Algar, O.; Solana, M.J.; Cabero Perez, M.J.; Sainz, T.; Martinez, L.; et al. The Evolving Microbiome from Pregnancy to Early Infancy: A Comprehensive Review. Nutrients 2020, 12, 133. [Google Scholar] [CrossRef]
- Kornman, K.S.; Loesche, W.J. Effects of Estradiol and Progesterone on Bacteroides melaninogenicus and Bacteroides gingivalis. Infect. Immun. 1982, 35, 256–263. [Google Scholar] [CrossRef]
- Fujiwara, N.; Tsuruda, K.; Iwamoto, Y.; Kato, F.; Odaki, T.; Yamane, N.; Hori, Y.; Harashima, Y.; Sakoda, A.; Tagaya, A.; et al. Significant Increase of Oral Bacteria in the Early Pregnancy Period in Japanese Women. J. Investig. Clin. Dent. 2017, 8, e12189. [Google Scholar] [CrossRef]
- Sooriyamoorthy, M.; Gower, D.B. Hormonal Influences on Gingival Tissue: Relationship to Periodontal Disease. J. Clin. Periodontol. 1989, 16, 201–208. [Google Scholar] [CrossRef]
- Vittek, J.; Hernandez, M.R.; Wenk, E.J.; Rappaport, S.C.; Southren, A.L. Specific Estrogen Receptors in Human Gingiva. J. Clin. Endocrinol. Metab. 1982, 54, 608–612. [Google Scholar] [CrossRef]
- Liu, Z.; Li, Z.; Wang, L.; Gu, Z.; Ma, L. Bibliometric Analysis of the Knowledge Landscape of Periodontal Disease in Pregnancy: A Noteworthy Multidisciplinary Issue. J. Multidiscip. Healthc. 2023, 16, 3941–3957. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Chen, S.-W.; Su, W.-L.; Zhu, H.-Y.; Ouyang, S.-Y.; Cao, Y.-T.; Jiang, S.-Y. Sex Hormones Enhance Gingival Inflammation without Affecting IL-1 β and TNF- α in Periodontally Healthy Women during Pregnancy. Mediators Inflamm. 2016, 2016, 4897890. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Timofeeva, I.; Bouchoucha, E.; Canceill, T.; Champion, C.; Groussolles, M.; Arnaud, C.; Vayssière, C.; Nabet, C.; Laurencin-Dalicieux, S. Oral and Periodontal Assessment at the First Trimester of Pregnancy: The PERISCOPE Longitudinal Study. Acta Obstet. Gynecol. Scand. 2023, 102, 669–680. [Google Scholar] [CrossRef]
- Massoni, R.S.D.S.; Aranha, A.M.F.; Matos, F.Z.; Guedes, O.A.; Borges, Á.H.; Miotto, M.; Porto, A.N. Correlation of Periodontal and Microbiological Evaluations, with Serum Levels of Estradiol and Progesterone, during Different Trimesters of Gestation. Sci. Rep. 2019, 9, 11762. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Jiang, W.; Hu, X.; Gao, L.; Ai, D.; Pan, H.; Niu, C.; Yuan, K.; Zhou, X.; Xu, C.; et al. Ecological Shifts of Supragingival Microbiota in Association with Pregnancy. Front. Cell. Infect. Microbiol. 2018, 8, 24. [Google Scholar] [CrossRef]
- Balan, P.; Chong, Y.S.; Umashankar, S.; Swarup, S.; Loke, W.M.; Lopez, V.; He, H.G.; Seneviratne, C.J. Keystone Species in Pregnancy Gingivitis: A Snapshot of Oral Microbiome During Pregnancy and Postpartum Period. Front. Microbiol. 2018, 9, 2360. [Google Scholar] [CrossRef]
- Aagaard, K.; Ma, J.; Antony, K.M.; Ganu, R.; Petrosino, J.; Versalovic, J. The Placenta Harbors a Unique Microbiome. Sci. Transl. Med. 2014, 6, 237ra65. [Google Scholar] [CrossRef]
- Han, Y.W.; Shen, T.; Chung, P.; Buhimschi, I.A.; Buhimschi, C.S. Uncultivated Bacteria as Etiologic Agents of Intra-Amniotic Inflammation Leading to Preterm Birth. J. Clin. Microbiol. 2009, 47, 38–47. [Google Scholar] [CrossRef]
- Fardini, Y.; Chung, P.; Dumm, R.; Joshi, N.; Han, Y.W. Transmission of Diverse Oral Bacteria to Murine Placenta: Evidence for the Oral Microbiome as a Potential Source of Intrauterine Infection. Infect. Immun. 2010, 78, 1789–1796. [Google Scholar] [CrossRef]
- Wen, X.; Fu, X.; Zhao, C.; Yang, L.; Huang, R. The Bidirectional Relationship between Periodontal Disease and Pregnancy via the Interaction of Oral Microorganisms, Hormone and Immune Response. Front. Microbiol. 2023, 14, 1070917. [Google Scholar] [CrossRef]
- Ye, C.; Kapila, Y. Oral Microbiome Shifts during Pregnancy and Adverse Pregnancy Outcomes: Hormonal and Immunologic Changes at Play. Periodontol. 2000 2021, 87, 276–281. [Google Scholar] [CrossRef]
- Moore, S.; Ide, M.; Coward, P.Y.; Randhawa, M.; Borkowska, E.; Baylis, R.; Wilson, R.F. A Prospective Study to Investigate the Relationship between Periodontal Disease and Adverse Pregnancy Outcome. Br. Dent. J. 2004, 197, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Farrell, S.; Ide, M.; Wilson, R.F. The Relationship between Maternal Periodontitis, Adverse Pregnancy Outcome and Miscarriage in Never Smokers. J. Clin. Periodontol. 2006, 33, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Konopka, T.; Zakrzewska, A. Periodontitis and Risk for Preeclampsia—A Systematic Review. Ginekol. Pol. 2020, 91, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.; Patoine, A.; Wu, T.T.; Castillo, D.A.; Xiao, J. Oral Microflora and Pregnancy: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 16870. [Google Scholar] [CrossRef]
- Barak, S.; Oettinger-Barak, O.; Machtei, E.E.; Sprecher, H.; Ohel, G. Evidence of Periopathogenic Microorganisms in Placentas of Women with Preeclampsia. J. Periodontol. 2007, 78, 670–676. [Google Scholar] [CrossRef]
- Lima, K.M.; Alves, C.M.; Vidal, F.C.; Gomes-Filho, I.S.; Costa, J.C.; Coletta, R.D.; Rodrigues, V.P.; Lopes, F.F. Fusobacterium Nucleatum and Prevotella in Women with Periodontitis and Preterm Birth. Med. Oral Patol. Oral Cir. Bucal 2023, 28, e450–e456. [Google Scholar] [CrossRef]
- Cooper, S.M.; Borgida, A.; Thacker, S.; Hammer, E.; Hariharan, A.; Kuo, C.; Blanck, N.; Yuan, H.; Panier, H.; Lin, Q.; et al. Oral Origin of the Placenta Microbiome in Pregnant Women with Preeclampsia. Front. Bacteriol. 2024, 2, 1322165. [Google Scholar] [CrossRef]
- Shaggag, L.M.; ALhabardi, N.; Adam, I. The Association between Maternal Periodontitis and Preterm Birth: A Case-Control Study in a Low-Resource Setting in Sudan, Africa. Medicina 2022, 58, 632. [Google Scholar] [CrossRef]
- De Oliveira, L.J.C.; Cademartori, M.G.; Schuch, H.S.; Barros, F.C.; Silveira, M.F.; Correa, M.B.; Demarco, F.F. Periodontal Disease and Preterm Birth: Findings from the 2015 Pelotas Birth Cohort Study. Oral Dis. 2021, 27, 1519–1527. [Google Scholar] [CrossRef]
- Katz, J.; Chegini, N.; Shiverick, K.T.; Lamont, R.J. Localization of P. gingivalis in Preterm Delivery Placenta. J. Dent. Res. 2009, 88, 575–578. [Google Scholar] [CrossRef]
- Ye, C.; Katagiri, S.; Miyasaka, N.; Kobayashi, H.; Khemwong, T.; Nagasawa, T.; Izumi, Y. The Periodontopathic Bacteria in Placenta, Saliva and Subgingival Plaque of Threatened Preterm Labor and Preterm Low Birth Weight Cases: A Longitudinal Study in Japanese Pregnant Women. Clin. Oral Investig. 2020, 24, 4261–4270. [Google Scholar] [CrossRef] [PubMed]
- Haerian-Ardakani, A.; Haerian, A. Relationship between Maternal Periodontal Disease and Low Birth Weight Babies. Iran J. Reprod. Med. 2013, 11, 625–630. [Google Scholar] [PubMed]
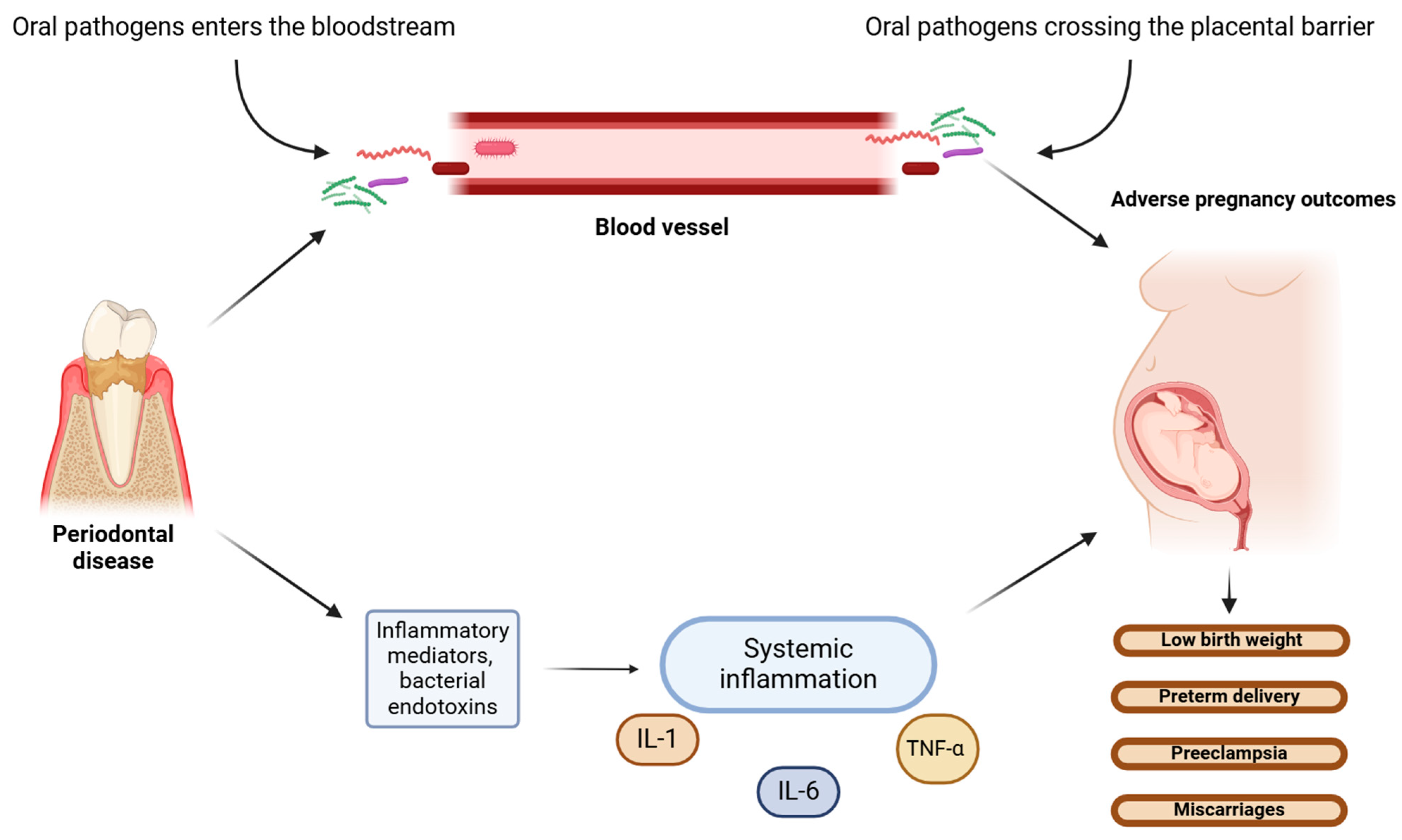
- Loos, B.G. Systemic Markers of Inflammation in Periodontitis. J. Periodontol. 2005, 76, 2106–2115. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; He, L.; Kang, J.; Huang, Z.; Sha, Y.; Zhu, W.; Yan, L. Relationship between the preterm low birth weight infant and the periodontal pathogen bacteria in maternal saliva. Beijing Da Xue Xue Bao Yi Xue Ban 2012, 44, 29–33. [Google Scholar]
- Kothwiale, S.V.; Desai, B.R.; Kothwiale, V.A.; Ganhid, M.; Konin, S. Periodontal Disease as a Potential Risk Factor for Low Birth Weight and Reduced Maternal Haemomglobin Levels. Oral Health Prev. Dent. 2014, 12, 83–90. [Google Scholar] [CrossRef]
- Perunovic, N.D.J.; Rakic, M.M.; Nikolic, L.I.; Jankovic, S.M.; Aleksic, Z.M.; Plecas, D.V.; Madianos, P.N.; Cakic, S.S. The Association Between Periodontal Inflammation and Labor Triggers (Elevated Cytokine Levels) in Preterm Birth: A Cross-Sectional Study. J. Periodontol. 2016, 87, 248–256. [Google Scholar] [CrossRef]
- Kunnen, A.; Van Pampus, M.; Aarnoudse, J.; Van Der Schans, C.; Abbas, F.; Faas, M. The Effect of Porphyromonas gingivalis Lipopolysaccharide on Pregnancy in the Rat. Oral Dis. 2014, 20, 591–601. [Google Scholar] [CrossRef]
- Han, Y.W.; Redline, R.W.; Li, M.; Yin, L.; Hill, G.B.; McCormick, T.S. Fusobacterium nucleatum Induces Premature and Term Stillbirths in Pregnant Mice: Implication of Oral Bacteria in Preterm Birth. Infect. Immun. 2004, 72, 2272–2279. [Google Scholar] [CrossRef]
- Hajishengallis, G. Periodontitis: From Microbial Immune Subversion to Systemic Inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef]
- Polyzos, N.P.; Polyzos, I.P.; Mauri, D.; Tzioras, S.; Tsappi, M.; Cortinovis, I.; Casazza, G. Effect of Periodontal Disease Treatment during Pregnancy on Preterm Birth Incidence: A Metaanalysis of Randomized Trials. Am. J. Obstet. Gynecol. 2009, 200, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Kurien, S.; Kattimani, V.S.; Sriram, R.R.; Sriram, S.K.; Bhupathi, A.; Bodduru, R.R.; Patil, N.N. Management of Pregnant Patient in Dentistry. J. Int. Oral Health 2013, 5, 88–97. [Google Scholar] [PubMed]
- Bostanci, N. Periodontal Health and Pregnancy Outcomes: Time to Deliver. Acta Obstet. Gynecol. Scand. 2023, 102, 648–651. [Google Scholar] [CrossRef]
- Zegers-Hochschild, F.; Adamson, G.D.; De Mouzon, J.; Ishihara, O.; Mansour, R.; Nygren, K.; Sullivan, E.; Vanderpoel, S. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) Revised Glossary of ART Terminology, 2009. Fertil. Steril. 2009, 92, 1520–1524. [Google Scholar] [CrossRef]
- World Health Organization. Infertility Prevalence Estimates, 1990–2021, 1st ed.; World Health Organization: Geneva, Switzerland, 2023; ISBN 978-92-4-006831-5. [Google Scholar]
- Koroma, L.; Stewart, L. Infertility: Evaluation and Initial Management. J. Midwifery Womens Health 2012, 57, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Jafri, Z.; Bhardwaj, A.; Sawai, M.; Sultan, N. Influence of Female Sex Hormones on Periodontium: A Case Series. J. Nat. Sci. Biol. Med. 2015, 6, 146. [Google Scholar] [CrossRef]
- Jakubowska-Kowal, K.M.; Skrzynska, K.J.; Gawlik-Starzyk, A.M. Prevalence and Diagnosis of Polycystic Ovary Syndrome (PCOS) in Adolescents—What’s New in 2023? Systematic Review. Ginekol. Pol. 2024, 95, 643–649. [Google Scholar] [CrossRef]
- The Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop group. Revised 2003 Consensus on Diagnostic Criteria and Long-Term Health Risks Related to Polycystic Ovary Syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef]
- Achu Joseph, R.; Ajitkumar, S.; Subbusamy Kanakasabapathy, B.; Santhanakrishnan, M. Evaluation of Microbial Profile in Patients with Polycystic Ovary Syndrome and Periodontal Disease: A Case-Control Study. Int. J. Fertil. Steril. 2023, 17, 248–253. [Google Scholar] [CrossRef]
- Jaglan, S.; Tewari, S.; Singhal, S.R.; Sharma, R.K. Impact of Polycystic Ovary Syndrome on Periodontal Status of Women of Adolescent and Adult Age Groups: A Cross-Sectional Study. Med. Princ. Pract. 2024, 33, 148–156. [Google Scholar] [CrossRef]
- Pavankumar, S.; Yellarthi, P.K.; Sandeep, J.N.; Boyapati, R.; Damera, T.K. Evaluation of Periodontal Status in Women with Polycystic Ovary Syndrome versus Healthy Women: A Cross-Sectional Study. J. Yeungnam Med. Sci. 2023, 40, S17–S22. [Google Scholar] [CrossRef] [PubMed]
- Machado, V.; Escalda, C.; Proença, L.; Mendes, J.J.; Botelho, J. Is There a Bidirectional Association between Polycystic Ovarian Syndrome and Periodontitis? A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1961. [Google Scholar] [CrossRef]
- Tanguturi, S.; Nagarakanti, S. Polycystic Ovary Syndrome and Periodontal Disease: Underlying Links- A Review. Indian J. Endocrinol. Metab. 2018, 22, 267. [Google Scholar] [CrossRef] [PubMed]
- Özçaka, Ö.; Buduneli, N.; Ceyhan, B.O.; Akcali, A.; Hannah, V.; Nile, C.; Lappin, D.F. Is Interleukin-17 Involved in the Interaction Between Polycystic Ovary Syndrome and Gingival Inflammation? J. Periodontol. 2013, 84, 1827–1837. [Google Scholar] [CrossRef] [PubMed]
- Özçaka, Ö.; Ceyhan, B.Ö.; Akcali, A.; Biçakci, N.; Lappin, D.F.; Buduneli, N. Is There an Interaction Between Polycystic Ovary Syndrome and Gingival Inflammation? J. Periodontol. 2012, 83, 1529–1537. [Google Scholar] [CrossRef]
- Tsilchorozidou, T.; Overton, C.; Conway, G.S. The Pathophysiology of Polycystic Ovary Syndrome. Clin. Endocrinol. 2004, 60, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Asnani, K.; Hingorani, D.; Kheur, S.; Deshmukh, V.; Romanos, G. Expression of Nuclear Receptors of Gingiva in Polycystic Ovarian Syndrome: A Preliminary Case Study. Aust. Dent. J. 2014, 59, 252–257. [Google Scholar] [CrossRef]
- Dou, Y.; Xin, J.; Zhou, P.; Tang, J.; Xie, H.; Fan, W.; Zhang, Z.; Wu, D. Bidirectional Association between Polycystic Ovary Syndrome and Periodontal Diseases. Front. Endocrinol. 2023, 14, 1008675. [Google Scholar] [CrossRef]
- Välimaa, H.; Savolainen, S.; Soukka, T.; Silvoniemi, P.; Mäkelä, S.; Kujari, H.; Gustafsson, J.-Å.; Laine, M. Estrogen Receptor- Is the Predominant Estrogen Receptor Subtype in Human Oral Epithelium and Salivary Glands. J. Endocrinol. 2004, 180, 55–62. [Google Scholar] [CrossRef]
- Nebel, D.; Bratthall, G.; Ekblad, E.; Norderyd, O.; Nilsson, B.-O. Estrogen Regulates DNA Synthesis in Human Gingival Epithelial Cells Displaying Strong Estrogen Receptor β Immunoreactivity: Estrogen Receptors in Human Gingiva. J. Periodontal Res. 2011, 46, 622–628. [Google Scholar] [CrossRef]
- Palanisamy, S. The Impact of Estrogen on Periodontal Tissue Integrity and Inflammation—A Mini Review. Front. Dent. Med. 2025, 6, 1455755. [Google Scholar] [CrossRef] [PubMed]
- Mariotti, A. Sex Steroid Hormones and Cell Dynamics in the Periodontium. Crit. Rev. Oral Biol. Med. 1994, 5, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Ojanotko-Harri, A.; Forssell, H.; Laine, M.; Hurttia, H.; Bläuer, M.; Tuohimaa, P. Immunohistochemical Detection of Androgen Receptors in Human Oral Mucosa. Arch. Oral Biol. 1992, 37, 511–514. [Google Scholar] [CrossRef]
- Gurav, A.N. Periodontitis and Insulin Resistance: Casual or Causal Relationship? Diabetes Metab. J. 2012, 36, 404. [Google Scholar] [CrossRef]
- Minty, M.; Canceil, T.; Serino, M.; Burcelin, R.; Tercé, F.; Blasco-Baque, V. Oral Microbiota-Induced Periodontitis: A New Risk Factor of Metabolic Diseases. Rev. Endocr. Metab. Disord. 2019, 20, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Barber, T.M.; Dimitriadis, G.K.; Andreou, A.; Franks, S. Polycystic Ovary Syndrome: Insight into Pathogenesis and a Common Association with Insulin Resistance. Clin. Med. 2016, 16, 262–266. [Google Scholar] [CrossRef]
- Rathi, N.; Reche, A. Risk of Periodontal Diseases in Women with Polycystic Ovary Syndrome: An Overview. Cureus 2023, 15, e47169. [Google Scholar] [CrossRef]
- Farook, F.F.; Ng, K.T.; Mnm, N.; Koh, W.J.; Teoh, W.Y. Association of Periodontal Disease and Polycystic Ovarian Syndrome: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. Open Dent. J. 2019, 13, 478–487. [Google Scholar] [CrossRef]
- Márquez-Arrico, C.F.; Silvestre-Rangil, J.; Gutiérrez-Castillo, L.; Martinez-Herrera, M.; Silvestre, F.J.; Rocha, M. Association between Periodontal Diseases and Polycystic Ovary Syndrome: A Systematic Review. J. Clin. Med. 2020, 9, 1586. [Google Scholar] [CrossRef]
- Rahiminejad, M.; Moaddab, A.; Zaryoun, H.; Rabiee, S.; Moaddab, A.; Khodadoustan, A. Comparison of Prevalence of Periodontal Disease in Women with Polycystic Ovary Syndrome and Healthy Controls. Dent. Res. J. 2015, 12, 507. [Google Scholar] [CrossRef]
- Dursun, E.; Akalın, F.A.; Güncü, G.N.; Çınar, N.; Aksoy, D.Y.; Tözüm, T.F.; Kılınc, K.; Yıldız, B.O. Periodontal Disease in Polycystic Ovary Syndrome. Fertil. Steril. 2011, 95, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Porwal, S.; Tewari, S.; Sharma, R.K.; Singhal, S.R.; Narula, S.C. Periodontal Status and High-Sensitivity C-Reactive Protein Levels in Polycystic Ovary Syndrome with and Without Medical Treatment. J. Periodontol. 2014, 85, 1380–1389. [Google Scholar] [CrossRef]
- Akcalı, A.; Bostanci, N.; Özçaka, Ö.; Öztürk-Ceyhan, B.; Gümüş, P.; Buduneli, N.; Belibasakis, G.N. Association between Polycystic Ovary Syndrome, Oral Microbiota and Systemic Antibody Responses. PLoS ONE 2014, 9, e108074. [Google Scholar] [CrossRef]
- Yang, N.; Zhang, Q.; Li, J.; Yang, S.; Shi, Q. Progression of Periodontal Inflammation in Adolescents Is Associated with Increased Number of Porphyromonas gingivalis, Prevotella intermedia, Tannerella forsythensis, and Fusobacterium nucleatum. Int. J. Paediatr. Dent. 2014, 24, 226–233. [Google Scholar] [CrossRef]
- Li, N.; Li, Y.; Qian, C.; Liu, Q.; Cao, W.; Ma, M.; He, R.; Chen, R.; Geng, R.; Liu, Y. Dysbiosis of the Saliva Microbiome in Patients with Polycystic Ovary Syndrome. Front. Cell. Infect. Microbiol. 2021, 10, 624504. [Google Scholar] [CrossRef] [PubMed]
- Lindheim, L.; Bashir, M.; Münzker, J.; Trummer, C.; Zachhuber, V.; Pieber, T.R.; Gorkiewicz, G.; Obermayer-Pietsch, B. The Salivary Microbiome in Polycystic Ovary Syndrome (PCOS) and Its Association with Disease-Related Parameters: A Pilot Study. Front. Microbiol. 2016, 7, 1270. [Google Scholar] [CrossRef]
- Liu, B.; Faller, L.L.; Klitgord, N.; Mazumdar, V.; Ghodsi, M.; Sommer, D.D.; Gibbons, T.R.; Treangen, T.J.; Chang, Y.-C.; Li, S.; et al. Deep Sequencing of the Oral Microbiome Reveals Signatures of Periodontal Disease. PLoS ONE 2012, 7, e37919. [Google Scholar] [CrossRef]
- Wang, J.; Qi, J.; Zhao, H.; He, S.; Zhang, Y.; Wei, S.; Zhao, F. Metagenomic Sequencing Reveals Microbiota and Its Functional Potential Associated with Periodontal Disease. Sci. Rep. 2013, 3, 1843. [Google Scholar] [CrossRef] [PubMed]
- Deepti; Tewari, S.; Narula, S.C.; Singhal, S.R.; Sharma, R.K. Effect of Non-Surgical Periodontal Therapy Along with Myo-Inositol on High-Sensitivity C-Reactive Protein and Insulin Resistance in Women with Polycystic Ovary Syndrome and Chronic Periodontitis: A Randomized Controlled Trial. J. Periodontol. 2017, 88, 999–1011. [Google Scholar] [CrossRef]
- Luthra, S.; Orlandi, M.; Hussain, S.B.; Leira, Y.; Botelho, J.; Machado, V.; Mendes, J.J.; Marletta, D.; Harden, S.; D’Aiuto, F. Treatment of Periodontitis and C -reactive Protein: A Systematic Review and Meta-analysis of Randomized Clinical Trials. J. Clin. Periodontol. 2023, 50, 45–60. [Google Scholar] [CrossRef]
- Wendland, N.; Opydo-Szymaczek, J.; Formanowicz, D.; Blacha, A.; Jarząbek-Bielecka, G.; Mizgier, M. Association between Metabolic and Hormonal Profile, Proinflammatory Cytokines in Saliva and Gingival Health in Adolescent Females with Polycystic Ovary Syndrome. BMC Oral Health 2021, 21, 193. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.M.; Bokor, A.; Heikinheimo, O.; Horne, A.; Jansen, F.; Kiesel, L.; King, K.; Kvaskoff, M.; Nap, A.; Petersen, K.; et al. ESHRE Guideline: Endometriosis. Hum. Reprod. Open 2022, 2022, hoac009. [Google Scholar] [CrossRef]
- Meuleman, C.; Vandenabeele, B.; Fieuws, S.; Spiessens, C.; Timmerman, D.; D’Hooghe, T. High Prevalence of Endometriosis in Infertile Women with Normal Ovulation and Normospermic Partners. Fertil. Steril. 2009, 92, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Bulletti, C.; Coccia, M.E.; Battistoni, S.; Borini, A. Endometriosis and Infertility. J. Assist. Reprod. Genet. 2010, 27, 441–447. [Google Scholar] [CrossRef]
- Sobstyl, A.; Chałupnik, A.; Mertowska, P.; Grywalska, E. How Do Microorganisms Influence the Development of Endometriosis? Participation of Genital, Intestinal and Oral Microbiota in Metabolic Regulation and Immunopathogenesis of Endometriosis. Int. J. Mol. Sci. 2023, 24, 10920. [Google Scholar] [CrossRef]
- Shan, J.; Ni, Z.; Cheng, W.; Zhou, L.; Zhai, D.; Sun, S.; Yu, C. Gut Microbiota Imbalance and Its Correlations with Hormone and Inflammatory Factors in Patients with Stage 3/4 Endometriosis. Arch. Gynecol. Obstet. 2021, 304, 1363–1373. [Google Scholar] [CrossRef]
- Ata, B.; Yildiz, S.; Turkgeldi, E.; Brocal, V.P.; Dinleyici, E.C.; Moya, A.; Urman, B. The Endobiota Study: Comparison of Vaginal, Cervical and Gut Microbiota Between Women with Stage 3/4 Endometriosis and Healthy Controls. Sci. Rep. 2019, 9, 2204. [Google Scholar] [CrossRef] [PubMed]
- Talwar, C.; Singh, V.; Kommagani, R. The Gut Microbiota: A Double-Edged Sword in Endometriosis. Biol. Reprod. 2022, 107, ioac147. [Google Scholar] [CrossRef]
- Yuan, M.; Li, D.; Zhang, Z.; Sun, H.; An, M.; Wang, G. Endometriosis Induces Gut Microbiota Alterations in Mice. Hum. Reprod. 2018, 33, 607–616. [Google Scholar] [CrossRef]
- Leonardi, M.; Hicks, C.; El-Assaad, F.; El-Omar, E.; Condous, G. Endometriosis and the Microbiome: A Systematic Review. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 239–249. [Google Scholar] [CrossRef]
- Akiyama, K.; Nishioka, K.; Khan, K.N.; Tanaka, Y.; Mori, T.; Nakaya, T.; Kitawaki, J. Molecular Detection of Microbial Colonization in Cervical Mucus of Women with and without Endometriosis. Am. J. Reprod. Immunol. 2019, 82, e13147. [Google Scholar] [CrossRef] [PubMed]
- Salliss, M.E.; Farland, L.V.; Mahnert, N.D.; Herbst-Kralovetz, M.M. The Role of Gut and Genital Microbiota and the Estrobolome in Endometriosis, Infertility and Chronic Pelvic Pain. Hum. Reprod. Update 2021, 28, 92–131. [Google Scholar] [CrossRef]
- Plottel, C.S.; Blaser, M.J. Microbiome and Malignancy. Cell Host Microbe 2011, 10, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Wu, Y.; Chai, X.; Wu, X. The Colonized Microbiota Composition in the Peritoneal Fluid in Women with Endometriosis. Arch. Gynecol. Obstet. 2022, 305, 1573–1580. [Google Scholar] [CrossRef]
- Wei, W.; Zhang, X.; Tang, H.; Zeng, L.; Wu, R. Microbiota Composition and Distribution along the Female Reproductive Tract of Women with Endometriosis. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 15. [Google Scholar] [CrossRef]
- Lee, S.-R.; Lee, J.-C.; Kim, S.-H.; Oh, Y.-S.; Chae, H.-D.; Seo, H.; Kang, C.-S.; Shin, T.-S. Altered Composition of Microbiota in Women with Ovarian Endometrioma: Microbiome Analyses of Extracellular Vesicles in the Peritoneal Fluid. Int. J. Mol. Sci. 2021, 22, 4608. [Google Scholar] [CrossRef] [PubMed]
- Jiang, I.; Yong, P.J.; Allaire, C.; Bedaiwy, M.A. Intricate Connections between the Microbiota and Endometriosis. Int. J. Mol. Sci. 2021, 22, 5644. [Google Scholar] [CrossRef]
- Qin, R.; Tian, G.; Liu, J.; Cao, L. The Gut Microbiota and Endometriosis: From Pathogenesis to Diagnosis and Treatment. Front. Cell. Infect. Microbiol. 2022, 12, 1069557. [Google Scholar] [CrossRef]
- Kavoussi, S.K.; West, B.T.; Taylor, G.W.; Lebovic, D.I. Periodontal Disease and Endometriosis: Analysis of the National Health and Nutrition Examination Survey. Fertil. Steril. 2009, 91, 335–342. [Google Scholar] [CrossRef]
- Thomas, V.; Uppoor, A.; Pralhad, S.; Naik, D.; Kushtagi, P. Towards a Common Etiopathogenesis: Periodontal Disease and Endometriosis. J. Hum. Reprod. Sci. 2018, 11, 269. [Google Scholar] [CrossRef]
- Ono, Y.; Kobayashi, Y.; Shimada, S.; Fukushi, Y.; Yoshino, O.; Wada, S.; Yamada, H. Uterine Endometrium Microbiome in Women with Repeated Implantation Failure Complicated by Endometriosis. J. Clin. Med. 2024, 13, 4605. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, C.T.L.; Gornic, C.; Barbosa, A.S.; Peixoto, R.J.M.; Colombo, A.P.V. Detection of Dialister Pneumosintes in the Subgingival Biofilm of Subjects with Periodontal Disease. Anaerobe 2007, 13, 244–248. [Google Scholar] [CrossRef]
- Doan, N.; Contreras, A.; Flynn, J.; Slots, J.; Chen, C. Molecular Identification of Dialister Pneumosintes in Subgingival Plaque of Humans. J. Clin. Microbiol. 2000, 38, 3043–3047. [Google Scholar] [CrossRef]
- Shaikh, H.F.M.; Oswal, P.U.; Kugaji, M.S.; Katti, S.S.; Bhat, K.G.; Kandaswamy, E.; Joshi, V.M. Association of F. Alocis and D. Pneumosintes with Periodontitis Disease Severity and Red Complex Bacteria. Dent. J. 2024, 12, 105. [Google Scholar] [CrossRef]
- Gare, J.; Kanoute, A.; Meda, N.; Viennot, S.; Bourgeois, D.; Carrouel, F. Periodontal Conditions and Pathogens Associated with Pre-Eclampsia: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7194. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.; Wang, P.; Liu, P.; Wang, Y.; Guo, Y.; Wang, C.; Jia, Y.; Zou, R.; Dong, S.; Niu, L. Association between Periodontitis and Endometriosis: A Bidirectional Mendelian Randomization Study. Front. Endocrinol. 2024, 15, 1271351. [Google Scholar] [CrossRef]
- Young, V.J.; Brown, J.K.; Saunders, P.T.K.; Horne, A.W. The Role of the Peritoneum in the Pathogenesis of Endometriosis. Hum. Reprod. Update 2013, 19, 558–569. [Google Scholar] [CrossRef]
- Muraoka, A.; Suzuki, M.; Hamaguchi, T.; Watanabe, S.; Iijima, K.; Murofushi, Y.; Shinjo, K.; Osuka, S.; Hariyama, Y.; Ito, M.; et al. Fusobacterium Infection Facilitates the Development of Endometriosis through the Phenotypic Transition of Endometrial Fibroblasts. Sci. Transl. Med. 2023, 15, eadd1531. [Google Scholar] [CrossRef] [PubMed]
- Vander Haar, E.L.; So, J.; Gyamfi-Bannerman, C.; Han, Y.W. Fusobacterium Nucleatum and Adverse Pregnancy Outcomes: Epidemiological and Mechanistic Evidence. Anaerobe 2018, 50, 55–59. [Google Scholar] [CrossRef]
- Blancafort, C.; Llácer, J. Can Probiotics Enhance Fertility Outcome? Capacity of Probiotics as a Single Intervention to Improve the Feminine Genital Tract Microbiota in Non-Symptomatic Reproductive-Aged Women. Front. Endocrinol. 2023, 13, 1081830. [Google Scholar] [CrossRef]
- Ayivi, R.D.; Gyawali, R.; Krastanov, A.; Aljaloud, S.O.; Worku, M.; Tahergorabi, R.; Silva, R.C.D.; Ibrahim, S.A. Lactic Acid Bacteria: Food Safety and Human Health Applications. Dairy 2020, 1, 202–232. [Google Scholar] [CrossRef]
- O’Hanlon, D.E.; Moench, T.R.; Cone, R.A. Vaginal pH and Microbicidal Lactic Acid When Lactobacilli Dominate the Microbiota. PLoS ONE 2013, 8, e80074. [Google Scholar] [CrossRef]
- Tachedjian, G.; Aldunate, M.; Bradshaw, C.S.; Cone, R.A. The Role of Lactic Acid Production by Probiotic Lactobacillus Species in Vaginal Health. Res. Microbiol. 2017, 168, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Tomusiak, A.; Strus, M.; Heczko, P.; Adamski, P.; Stefański, G.; Mikołajczyk-Cichońska, A.; Suda-Szczurek, M. Efficacy and Safety of a Vaginal Medicinal Product Containing Three Strains of Probiotic Bacteria: A Multicenter, Randomized, Double-Blind, and Placebo-Controlled Trial. Drug Des. Dev. Ther. 2015, 9, 5345–5354. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, P.; Chatterjee, A.; Raghunathan, V. Probiotics in the Treatment of Periodontal Disease: A Systematic Review. J. Indian Soc. Periodontol. 2016, 20, 488. [Google Scholar] [CrossRef]
- Baddouri, L.; Hannig, M. Probiotics as an Adjunctive Therapy in Periodontitis Treatment—Reality or Illusion—A Clinical Perspective. Npj Biofilms Microbiomes 2024, 10, 148. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, R.; Ostadmohammadi, V.; Akbari, M.; Lankarani, K.B.; Vakili, S.; Peymani, P.; Karamali, M.; Kolahdooz, F.; Asemi, Z. The Effects of Probiotic Supplementation on Clinical Symptom, Weight Loss, Glycemic Control, Lipid and Hormonal Profiles, Biomarkers of Inflammation, and Oxidative Stress in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Probiot. Antimicrob. Proteins 2022, 14, 1–14. [Google Scholar] [CrossRef]
- Calcaterra, V.; Rossi, V.; Massini, G.; Casini, F.; Zuccotti, G.; Fabiano, V. Probiotics and Polycystic Ovary Syndrome: A Perspective for Management in Adolescents with Obesity. Nutrients 2023, 15, 3144. [Google Scholar] [CrossRef]
- Miao, C.; Guo, Q.; Fang, X.; Chen, Y.; Zhao, Y.; Zhang, Q. Effects of Probiotic and Synbiotic Supplementation on Insulin Resistance in Women with Polycystic Ovary Syndrome: A Meta-Analysis. J. Int. Med. Res. 2021, 49, 03000605211031758. [Google Scholar] [CrossRef]
- Uchida, M.; Kobayashi, O. Effects of Lactobacillus gasseri OLL2809 on the Induced Endometriosis in Rats. Biosci. Biotechnol. Biochem. 2013, 77, 1879–1881. [Google Scholar] [CrossRef]
- Khodaverdi, S.; Mohammadbeigi, R.; Khaledi, M.; Mesdaghinia, L.; Sharifzadeh, F.; Nasiripour, S.; Gorginzadeh, M. Beneficial Effects of Oral Lactobacillus on Pain Severity in Women Suffering from Endometriosis: A Pilot Placebo-Controlled Randomized Clinical Trial. Int. J. Fertil. Steril. 2019, 13, 178–183. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Study | n | Study Design | Investigated Pregnancy Outcome | Results |
|---|---|---|---|---|
| Moore et al. [52] (2004) | n = 3738 | Prospective study | Preterm birth Low birth weight Miscarriage | Poorer periodontal health was associated with an increased risk of late miscarriage; however, no significant relationships between the severity of periodontal disease and preterm birth or low birth weight were shown. |
| Farrell et al. [53] (2006) | n = 1793 | Prospective study | Preterm birth Low birth weight Miscarriage | No association between periodontitis and preterm birth or low birth weight among never-smokers was found; however, late miscarriage was associated with some measures of periodontal disease, like higher mean probing depth at mesial sites. |
| Barak et al. [56] (2007) | Cases: n = 16 Controls: n = 14 | Case–control study | Preeclampsia | A significant presence of periopathogenic microorganisms (A. actinomycetemcomitans, F. nucleatum ssp., P. gingivalis, P. intermedia, T. forsythensis, and T. denticola) or their products was detected in human placentas of women with preeclampsia. |
| Katz et al. [61] (2009) | Cases: n = 9 Controls: n = 5 | Case–control study | Preterm birth | The presence of Porphyromonas gingivalis antigens in placental tissues was associated with preterm delivery. |
| Chen et al. [65] (2012) | Cases: n = 72 Controls: n = 38 | Retrospective study | Low birth weight | A significantly lower birth weight, as well as higher plaque index, probing depth, and clinical attachment loss, were observed in the P. gingivalis-positive group. |
| Haerian-Ardakani et al. [63] (2013) | Cases: n = 44 Controls: n = 44 | Case–control study | Low birth weight | An association was found between a greater number of deep periodontal pockets, poorer maternal oral health, and low birth weight. |
| Kothwiale et al. [66] (2014) | n = 770 | Observational study | Preterm birth Low birth weight | Periodontitis was significantly associated with low birth weight, and the increase in the severity of periodontal disease was associated with a higher rate of preterm birth. |
| Perunovic et al. [67] (2016) | Cases: n = 60 Controls: n = 60 | Cross-sectional study | Preterm birth | Poorer oral health, higher rate of periodontitis, and significantly higher levels of proinflammatory cytokines (IL-6 * and PGE2 **) in GCF *** were observed among women with preterm birth. |
| Ye et al. [62] (2020) | Cases: n = 28 Controls: n = 36 | Longitudinal study | Preterm birth | The presence of F. nucleatum in placental tissues was significantly associated with a threatened preterm birth. |
| De Oliveira [60] (2021) | n = 2474 | Cohort study | Preterm birth | Periodontal disease increased the risk of early preterm delivery, making it almost two times higher. |
| Shaggag et al. [59] (2022) | n = 165 | Case–control study | Preterm birth | A strong association was found between periodontitis and low hemoglobin levels with preterm birth among women with spontaneous preterm delivery. |
| Lima et al. [57] (2023) | Cases: n = 40 Controls: n = 80 | Case–control study | Preterm birth Low birth weight | A possible relationship was observed between periodontitis and preterm birth, as well as low birth weight, based on clinical parameters and the ratio of P. intermedia and F. nucleatum at periodontal sites. |
| Cooper et al. [58] (2024) | n = 54 | Prospective, cross-sectional cohort study | Preeclampsia | A significant presence of a combined group of oral-origin bacteria was detected in the placentas of pregnant women with preeclampsia. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcickiewicz, J.; Jamka, M.; Walkowiak, J. A Potential Link Between Oral Microbiota and Female Reproductive Health. Microorganisms 2025, 13, 619. https://doi.org/10.3390/microorganisms13030619
Marcickiewicz J, Jamka M, Walkowiak J. A Potential Link Between Oral Microbiota and Female Reproductive Health. Microorganisms. 2025; 13(3):619. https://doi.org/10.3390/microorganisms13030619
Chicago/Turabian StyleMarcickiewicz, Justyna, Małgorzata Jamka, and Jarosław Walkowiak. 2025. "A Potential Link Between Oral Microbiota and Female Reproductive Health" Microorganisms 13, no. 3: 619. https://doi.org/10.3390/microorganisms13030619
APA StyleMarcickiewicz, J., Jamka, M., & Walkowiak, J. (2025). A Potential Link Between Oral Microbiota and Female Reproductive Health. Microorganisms, 13(3), 619. https://doi.org/10.3390/microorganisms13030619