
Etiology and Oral Antibiotic Susceptibility Patterns of the First Urinary Tract Infection Episode in Infants Under 6 Months of Age: A 17-Year, Retrospective, Single-Center Study in Italy
 , , , , , , , , , and
, , , , , , , , , and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Distribution of the Most Frequently Isolated Bacteria
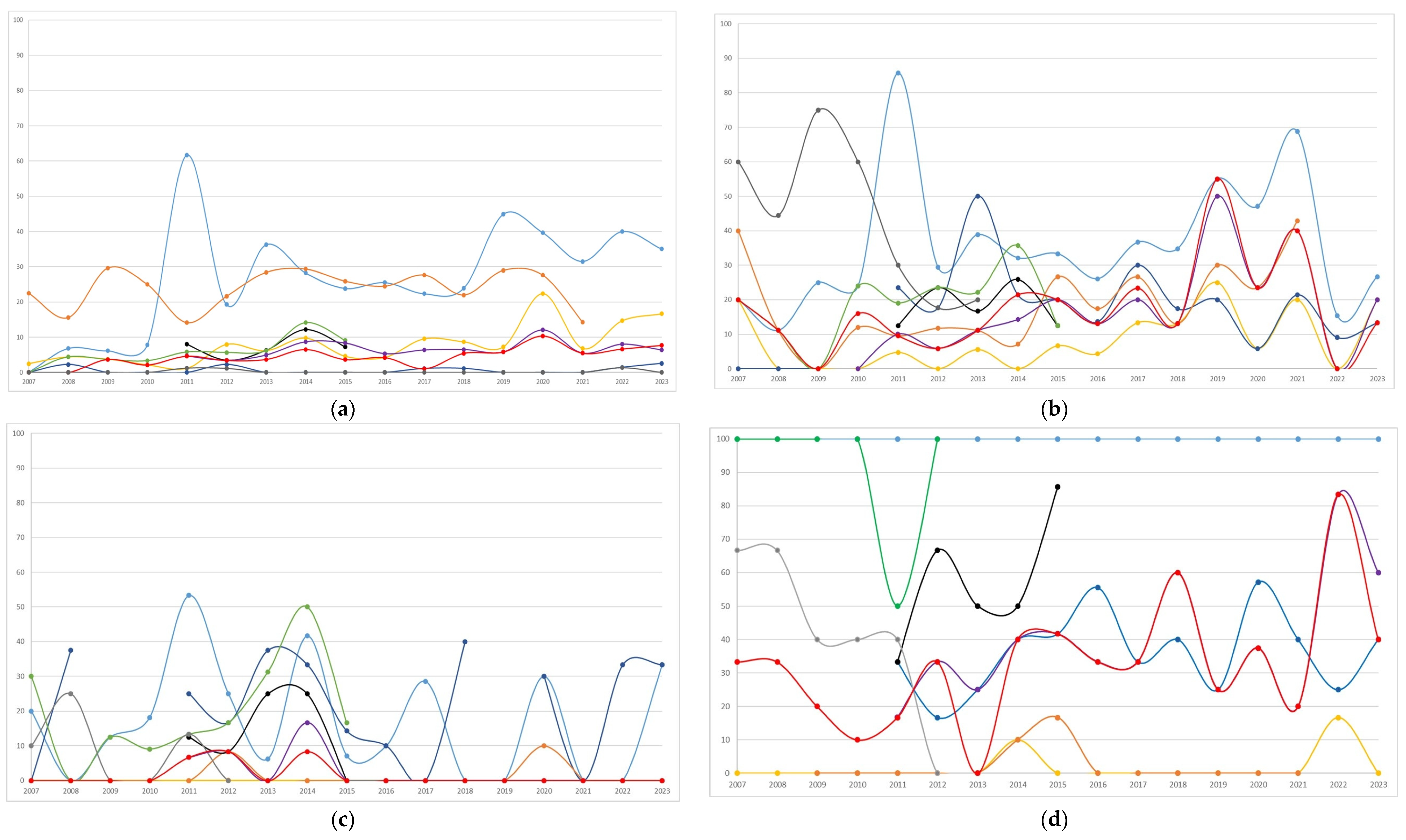
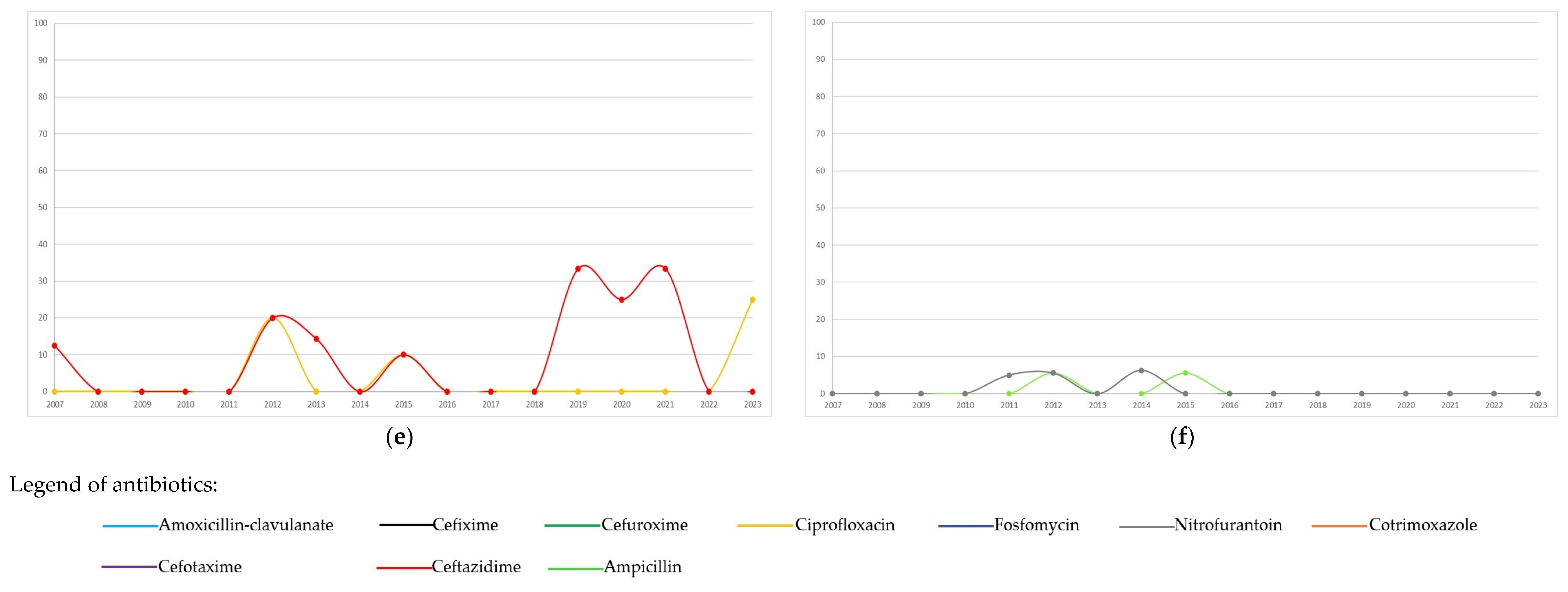
3.2. Temporal Trends in Antibiotic Resistance by Pathogen
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| UTI | Urinary tract infections |
| IGG | Istituto Giannina Gaslini |
| ESBL | Extended-spectrum beta-lactamase |
| IQR | Interquartile range |
| CFU | Colony-forming units |
| CLSI | Clinical and Laboratory Standards Institute |
| EUCAST | European Committee on Antimicrobial Susceptibility Testing |
References
- Greenhow, T.L.; Hung, Y.Y.; Herz, A.M.; Losada, E.; Pantell, R.H. The changing epidemiology of serious bacterial infections in young infants. Pediatr. Infect. Dis. J. 2014, 33, 595–599. [Google Scholar] [CrossRef]
- Stephens, G.M.; Akers, S.; Nguyen, H.; Woxland, H. Evaluation and management of urinary tract infections in the school-aged child. Prim. Care 2015, 42, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Korbel, L.; Howell, M.; Spencer, J.D. The clinical diagnosis and management of urinary tract infections in children and adolescents. Paediatr. Int. Child. Health. 2017, 37, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Balighian, E.; Burke, M. Urinary Tract Infections in Children. Pediatr. Rev. 2018, 39, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Maglietta, G.; Di Costanzo, M.; Ceccoli, M.; Vergine, G.; La Scola, C.; Malaventura, C.; Falcioni, A.; Iacono, A.; Crisafi, A.; et al. Retrospective 8-Year Study on the Antibiotic Resistance of Uropathogens in Children Hospitalised for Urinary Tract Infection in the Emilia-Romagna Region, Italy. Antibiotics 2021, 10, 1207. [Google Scholar] [CrossRef]
- GBD 2021 Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance 1990–2021: A systematic analysis with forecasts to 2050. Lancet 2024, 404, 1199–1226. [Google Scholar] [CrossRef]
- Shkalim Zemer, V.; Ashkenazi, S.; Levinsky, Y.; Richenberg, Y.; Jacobson, E.; Nathanson, S.; Shochat, T.; Kushnir, S.; Cohen, M.; Cohen, A.H. Pathogens Causing Pediatric Community Acquired Urinary Tract Infections and Their Increasing Antimicrobial Resistance: A Nationwide Study. Pathogens 2024, 13, 201. [Google Scholar] [CrossRef]
- Bagnasco, F.; Piaggio, G.; Mesini, A.; Mariani, M.; Russo, C.; Saffioti, C.; Losurdo, G.; Palmero, C.; Castagnola, E. Epidemiology of Antibiotic Resistant Pathogens in Pediatric Urinary Tract Infections as a Tool to Develop a Prediction Model for Early Detection of Drug-Specific Resistance. Antibiotics 2022, 11, 720. [Google Scholar] [CrossRef]
- Pierantoni, L.; Andreozzi, L.; Ambretti, S.; Dondi, A.; Biagi, C.; Baccelli, F.; Lanari, M. Three-Year Trend in Escherichia coli Antimicrobial Resistance among Children’s Urine Cultures in an Italian Metropolitan Area. Children 2021, 8, 597. [Google Scholar] [CrossRef]
- Zhang, K.; Fang, X.; Zhang, Y.; Chao, M. A retrospective study of uropathogen and its antibiotic resistance among children with urinary tract infection from a single center in China. Heliyon 2024, 10, e31902. [Google Scholar] [CrossRef]
- Mohamed, A.A.; Bastug, Y.; Senol, C.; Kassim, M.M.; Yusuf, A.A.; Mohamed, A.H. Antimicrobial resistance pattern and uropathogens distribution in children visiting a referral hospital in Mogadishu. Future Sci. OA 2024, 10, FSO978. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Thänert, R.; Reske, K.A.; Nickel, K.B.; Olsen, M.A.; Hink, T.; Thänert, A.; Wallace, M.A.; Wang, B.; Cass, C.; et al. Gut microbiome correlates of recurrent urinary tract infection: A longitudinal, multi-center study. EClinicalMedicine 2024, 71, 102490. [Google Scholar] [CrossRef]
- Washahi, M.; Miron, D.; Steinberg Ben Zeev, Z.; Chayen, G.; Jacob, R. High Rates of ESBL-producing and Gentamycin-resistant Gram-negative Bacteria During the First Week of Life: A Multicenter Cross-sectional Study Among Infants Younger Than 2 Months With Urinary Tract Infection. Pediatr. Infect. Dis. J. 2023, 42, 750–753. [Google Scholar] [CrossRef] [PubMed]
- Flokas, M.E.; Karanika, S.; Alevizakos, M.; Mylonakis, E. Prevalence of ESBL-Producing Enterobacteriaceae in Pediatric Bloodstream Infections: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0171216. [Google Scholar] [CrossRef]
- Kubes, J.N.; Fridkin, S.K. Factors affecting the geographic variability of antibiotic-resistant healthcare-associated infections in the United States using the CDC Antibiotic Resistance Patient Safety Atlas. Infect. Control Hosp. Epidemiol. 2019, 40, 597–599. [Google Scholar] [CrossRef]
- Tullus, K.; Shaikh, N. Urinary tract infections in children. Lancet 2020, 395, 1659–1668. [Google Scholar] [CrossRef] [PubMed]
- Brandström, P.; Hansson, S. Urinary Tract Infection in Children. Pediatr. Clin. N. Am. 2022, 69, 1099–1114. [Google Scholar] [CrossRef]
- Piñeiro Pérez, R.; Cilleruelo Ortega, M.J.; Ares Álvarez, J.; Baquero-Artigao, F.; Silva Rico, J.C.; Velasco Zúñiga, R.; Martínez Campos, L.; Carazo Gallego, B.; Conejo Fernández, A.J.; Calvo, C.; et al. Recomendaciones sobre el diagnóstico y tratamiento de la infección urinaria [Recommendations on the diagnosis and treatment of urinary tract infection]. An. Pediatría (Engl. Ed.) 2019, 90, e1–e400. (In Spanish) [Google Scholar] [CrossRef]
- Belko, N.A.; Pohl, H.G. Pediatric Urinary Tract Infections. Urol. Clin. N. Am. 2024, 51, 537–549. [Google Scholar] [CrossRef]
- Ismaili, K.; Lolin, K.; Damry, N.; Alexander, M.; Lepage, P.; Hall, M. Febrile urinary tract infections in 0- to 3-month-old infants: A prospective follow-up study. J. Pediatr. 2011, 158, 91–94. [Google Scholar] [CrossRef]
- Lohr, J.A.; Downs, S.M.; Dudley, S.; Donowitz, L.G. Hospital-acquired urinary tract infections in the pediatric patient: A prospective study. Pediatr. Infect. Dis. J. 1994, 13, 8–12. [Google Scholar] [CrossRef]
- Srivastava, S.; Shetty, N. Healthcare-associated infections in neonatal units: Lessons from contrasting worlds. J. Hosp. Infect. 2007, 65, 292–306. [Google Scholar] [CrossRef] [PubMed]
- Montagnani, C.; Tersigni, C.; D’Arienzo, S.; Miftode, A.; Venturini, E.; Bortone, B.; Bianchi, L.; Chiappini, E.; Forni, S.; Gemmi, F.; et al. Resistance Patterns from Urine Cultures in Children Aged 0 to 6 Years: Implications for Empirical Antibiotic Choice. Infect. Drug Resist. 2021, 14, 2341–2348. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, R.; Boutzoukas, A.E.; Chan, E.; Girgis, V.; Kinduelo, V.; Kwabia, S.A.; Yan, J.; Clark, R.H.; Zimmerman, K.O.; Greenberg, R.G. Urinary Tract Infection Epidemiology in NICUs in the United States. Am. J. Perinatol. 2024, 41 (Suppl. S1), e2202–e2208. [Google Scholar] [CrossRef] [PubMed]
- Tishberg, L.M.; Kusulas, M.P. Management of pediatric urinary tract infections in the emergency department. Pediatr. Emerg. Med. Pract. 2024, 21, 1–28. [Google Scholar]
- Nuutinen, M.; Uhari, M. Recurrence and follow-up after urinary tract infection under the age of 1 year. Pediatr. Nephrol. 2001, 16, 69–72. [Google Scholar] [CrossRef]
- He, X.T.; Chang, C.N.; Yu, C.H.; Wang, C.C. The risk factors, antimicrobial resistance patterns, and outcomes associated with extended-spectrum β-lactamases-Producing pathogens in pediatric urinary tract infection. Pediatr. Neonatol. 2024, 65, 242–248. [Google Scholar] [CrossRef]
- Sabih, A.; Leslie, S.W. Complicated Urinary Tract Infections. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK436013/ (accessed on 8 January 2025).
- Fernandes, A.; Oliveira, Í.; Pereira, M.; Mendes, P.; Virtuoso, M.J.; Pereira, A. Local Antimicrobial Resistance Trends in Pediatric Urinary Tract Infection: The Importance of Local Surveillance of a Global Problem. Cureus 2024, 16, e54700. [Google Scholar] [CrossRef]
- Ammenti, A.; Alberici, I.; Brugnara, M.; Chimenz, R.; Guarino, S.; La Manna, A.; La Scola, C.; Maringhini, S.; Marra, G.; Materassi, M.; et al. Updated Italian recommendations for the diagnosis, treatment and follow-up of the first febrile urinary tract infection in young children. Acta Paediatr. 2020, 109, 236–247. [Google Scholar] [CrossRef]
- Dejonckheere, Y.; Desmet, S.; Knops, N. A study of the 20-year evolution of antimicrobial resistance patterns of pediatric urinary tract infections in a single center. Eur. J. Pediatr. 2022, 181, 3271–3281. [Google Scholar] [CrossRef]
- Kawalec, A.; Józefiak, J.; Kiliś-Pstrusińska, K. Urinary Tract Infection and Antimicrobial Resistance Patterns: 5-Year Experience in a Tertiary Pediatric Nephrology Center in the Southwestern Region of Poland. Antibiotics 2023, 12, 1454. [Google Scholar] [CrossRef] [PubMed]
- Devrim, F.; Serdaroğlu, E.; Çağlar, İ.; Oruç, Y.; Demiray, N.; Bayram, N.; Ağın, H.; Çalkavur, S.; Sorguç, Y.; Dinçel, N.; et al. The Emerging Resistance in Nosocomial Urinary Tract Infections: From the Pediatrics Perspective. Mediterr. J. Hematol. Infect. Dis. 2018, 10, e2018055. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Total Infants, n (%) | 2473 (100.0) |
|---|---|
| Sex, M | 1549 (62.6) |
| Months at the 1st UTI, median (IQR) | 2.8 (1.2–4.7) |
| Total of UTI, median (IQR), min–max values | 1 (1–2), 1–23 |
| 1 | 1854 (75) |
| 2 | 347 (14) |
| >2 | 272 (11) |
| Department of admission | |
| Emergency | 1366 (55.2) |
| Neonatal/Pediatric ICU | 336 (13.6) |
| Infectious Diseases | 221 (8.9) |
| Surgery/Orthopedics/Neurosurgery | 128 (5.2) |
| Nephrology | 115 (4.7) |
| Hematology/Oncology | 7 (0.3) |
| Others | 300 (12.1) |
| Year of the 1st UTI, median (IQR) | 2015 (2011–2018) |
| 2007 | 99 (4.0) |
| 2008 | 85 (3.4) |
| 2009 | 118 (4.8) |
| 2010 | 181 (7.3) |
| 2011 | 181 (7.3) |
| 2012 | 163 (6.6) |
| 2013 | 151 (6.1) |
| 2014 | 191 (7.7) |
| 2015 | 201 (8.1) |
| 2016 | 176 (7.1) |
| 2017 | 163 (6.6) |
| 2018 | 159 (6.4) |
| 2019 | 114 (4.6) |
| 2020 | 110 (4.4) |
| 2021 | 125 (5.0) |
| 2022 | 134 (5.4) |
| 2023 | 122 (4.9) |
| Group of Pathogens | Pathogens | n (%) | ||
|---|---|---|---|---|
| Gram-positives, 281 (11.2) | Enterococcus | 241 (85.8) | ||
| faecalis | 209 | |||
| faecium | 26 | |||
| spp. | 6 | |||
| Streptococcus agalactiae | 24 (8.5) | |||
| Staphylococcus aureus | 16 (5.7) | |||
| Gram-negatives, 2217 (88.8) | Enterobacterales | 2116 (95.4) | ||
| Escherichia coli | 1324 | |||
| Klebsiella pneumoniae | 308 | |||
| Klebsiella oxytoca | 164 | |||
| Enterobacter cloacae | 106 | |||
| Enterobacter aerogenes | 60 | |||
| Citrobacter koseri | 31 | |||
| Proteus mirabilis | 32 | |||
| Citrobacter freundi | 27 | |||
| Serratia marcescens | 22 | |||
| Other | 42 | |||
| Klebsiella aerogenes | 8 | |||
| Enterobacter spp. | 6 | |||
| Klebsiella spp. | 6 | |||
| Morganella morganii | 4 | |||
| Serratia spp. | 3 | |||
| Citrobacter spp. | 3 | |||
| Citrobacter farmeri | 2 | |||
| Enterobacter hormaechei | 2 | |||
| Salmonella spp. | 2 | |||
| Enterobacter kobei | 1 | |||
| Citrobacter braakii | 1 | |||
| Citrobacter werkmanii | 1 | |||
| Proteus spp. | 1 | |||
| Serratia liquefaciens | 1 | |||
| Serratia plymuthica | 1 | |||
| Glucose non fermenting | 101 (4.6) | |||
| Pseudomonas aeruginosa | 90 | |||
| Other | 11 | |||
| Pseudomonas spp. | 5 | |||
| Stenotrophomonas maltophilia | 2 | |||
| Acinetobacter lwoffii | 1 | |||
| Acinetobacter spp. | 1 | |||
| Pseudomonas fluorescens | 1 | |||
| Pseudomonas putida | 1 | |||
| Escherichia coli, n = 1324 | Klebsiella pneumoniae, n = 308 | Klebsiella oxytoca, n = 164 | Enterobacter cloacae, n = 106 | Pseudomonas aeruginosa, n = 90 | Enterococcus faecalis, n = 209 | p-Value | |
|---|---|---|---|---|---|---|---|
| Sex, F, n (%) | 496 (37.5) | 129 (41.9) | 55 (33.5) | 36 (34) | 38 (42.2) | 80 (38.3) | 0.424 |
| Sex, M, n (%) | 828 (62.5) | 179 (58.1) | 109 (66.5) | 70 (66) | 52 (57.8) | 129 (61.7) | |
| Age, <3 months, n (%) | 618 (46.7) | 193 (62.7) | 98 (59.8) | 62 (58.5) | 36 (40.0) | 139 (66.5) | <0.001 |
| Age, ≥3 months, n (%) | 706 (53.3) | 115 (37.3) | 66 (40.2) | 44 (41.5) | 54 (60.0) | 70 (33.5) | |
| Year of the first UTI, <2015, n (%) | 687 (51.9) | 146 (47.4) | 106 (64.6) | 59 (55.7) | 57 (63.3) | 131 (62.7) | <0.001 |
| Year of the first UTI, ≥2015, n (%) | 637 (48.1) | 162 (52.6) | 58 (35.4) | 47 (44.3) | 33 (36.7) | 78 (37.3) |
| Susceptible, n | Resistant, n | Not Tested, n | % Resistant/Tested | % Resistant/Tested <2015 | % Resistant/Tested ≥2015 | p-Value | |
|---|---|---|---|---|---|---|---|
| Oral | |||||||
| Amoxicillin-clavulanate | |||||||
| Escherichia coli | 937 | 362 | 25 | 27.9 | 24.1 | 31.8 | 0.002 |
| Klebsiella pneumoniae | 188 | 115 | 5 | 37.9 | 37 | 38.8 | 0.738 |
| Klebsiella oxytoca | 133 | 30 | 1 | 18.4 | 21.7 | 12.3 | 0.139 |
| Enterobacter cloacae | 0 | 99 | 7 | 100 | 100 | 100 | |
| Cefixime | |||||||
| Escherichia coli | 336 | 27 | 961 | 7.4 | 7.4 | - | |
| Klebsiella pneumoniae | 69 | 17 | 222 | 19.8 | 19.8 | - | |
| Klebsiella oxytoca | 45 | 9 | 110 | 16.7 | 16.7 | - | |
| Enterobacter cloacae | 12 | 18 | 76 | 60 | 60 | - | |
| Cefuroxime | |||||||
| Escherichia coli | 590 | 40 | 694 | 6.3 | 6.3 | - | |
| Klebsiella pneumoniae | 108 | 31 | 169 | 22.3 | 22.3 | - | |
| Klebsiella oxytoca | 77 | 21 | 66 | 21.4 | 21.4 | - | |
| Enterobacter cloacae | 3 | 26 | 77 | 89.7 | 89.7 | - | |
| Ciprofloxacin | |||||||
| Escherichia coli | 1216 | 102 | 6 | 7.7 | 5 | 10.7 | <0.001 |
| Klebsiella pneumoniae | 278 | 24 | 6 | 7.9 | 2.7 | 12.8 | 0.001 |
| Klebsiella oxytoca | 163 | 0 | 1 | 0 | 0 | 0 | |
| Enterobacter cloacae | 102 | 2 | 2 | 1.9 | 1.7 | 2.2 | 1.000 |
| Pseudomonas aeruginosa | 83 | 3 | 4 | 3.5 | 3.6 | 3.3 | 1.000 |
| Fosfomycin | |||||||
| Escherichia coli | 1159 | 8 | 157 | 0.7 | 0.5 | 0.8 | 0.728 |
| Klebsiella pneumoniae | 213 | 52 | 43 | 19.6 | 22.1 | 17.8 | 0.377 |
| Klebsiella oxytoca | 107 | 31 | 26 | 22.5 | 23.5 | 21 | 0.739 |
| Enterobacter cloacae | 57 | 30 | 19 | 34.5 | 26.7 | 42.9 | 0.112 |
| Nitrofurantoin | |||||||
| Escherichia coli | 1279 | 3 | 73 | 0.2 | 0.2 | - | |
| Klebsiella pneumoniae | 59 | 39 | 210 | 39.8 | 39.8 | - | |
| Klebsiella oxytoca | 70 | 5 | 89 | 6.7 | 6.7 | - | |
| Enterobacter cloacae | 27 | 12 | 67 | 30.8 | 30.8 | - | |
| Enterococcus faecalis | 133 | 3 | 73 | 2.2 | 2.2 | - | |
| Cotrimoxazole | |||||||
| Escherichia coli | 846 | 273 | 205 | 24.4 | 23.9 | 25.1 | 0.656 |
| Klebsiella pneumoniae | 220 | 46 | 42 | 17.3 | 12.3 | 23.3 | 0.018 |
| Klebsiella oxytoca | 146 | 2 | 16 | 1.3 | 0.9 | 2.4 | 0.488 |
| Enterobacter cloacae | 83 | 6 | 17 | 6.7 | 10.2 | 0 | 0.093 |
| Intravenous | |||||||
| Cefotaxime | |||||||
| Escherichia coli | 1050 | 71 | 203 | 6.3 | 5.7 | 6.8 | 0.472 |
| Klebsiella pneumoniae | 210 | 47 | 51 | 18.3 | 11.9 | 22.4 | 0.033 |
| Klebsiella oxytoca | 123 | 4 | 37 | 3.1 | 5.6 | 0 | 0.130 |
| Enterobacter cloacae | 50 | 34 | 22 | 40.5 | 35.9 | 44.4 | 0.426 |
| Ceftazidime | |||||||
| Escherichia coli | 1260 | 59 | 5 | 4.5 | 3.5 | 5.5 | 0.075 |
| Klebsiella pneumoniae | 246 | 56 | 6 | 18.5 | 13.7 | 23.1 | 0.036 |
| Klebsiella oxytoca | 160 | 3 | 1 | 1.8 | 2.8 | 0 | 0.552 |
| Enterobacter cloacae | 69 | 35 | 2 | 33.6 | 27.1 | 42.2 | 0.106 |
| Pseudomonas aeruginosa | 79 | 7 | 4 | 8.1 | 7.1 | 10 | 0.691 |
| Ampicillin | |||||||
| Enterococcus faecalis | 195 | 2 | 12 | 1.0 | 1.5 | 0 | 0.549 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagnasco, F.; Lorenzini Ceradelli, F.; Mesini, A.; Saffioti, C.; Ricci, E.; Russo, C.; Mariani, M.; Ugolotti, E.; Caci, E.; Contu, D.; et al. Etiology and Oral Antibiotic Susceptibility Patterns of the First Urinary Tract Infection Episode in Infants Under 6 Months of Age: A 17-Year, Retrospective, Single-Center Study in Italy. Microorganisms 2025, 13, 607. https://doi.org/10.3390/microorganisms13030607
Bagnasco F, Lorenzini Ceradelli F, Mesini A, Saffioti C, Ricci E, Russo C, Mariani M, Ugolotti E, Caci E, Contu D, et al. Etiology and Oral Antibiotic Susceptibility Patterns of the First Urinary Tract Infection Episode in Infants Under 6 Months of Age: A 17-Year, Retrospective, Single-Center Study in Italy. Microorganisms. 2025; 13(3):607. https://doi.org/10.3390/microorganisms13030607
Chicago/Turabian StyleBagnasco, Francesca, Francesca Lorenzini Ceradelli, Alessio Mesini, Carolina Saffioti, Erica Ricci, Chiara Russo, Marcello Mariani, Elisabetta Ugolotti, Emanuela Caci, Debora Contu, and et al. 2025. "Etiology and Oral Antibiotic Susceptibility Patterns of the First Urinary Tract Infection Episode in Infants Under 6 Months of Age: A 17-Year, Retrospective, Single-Center Study in Italy" Microorganisms 13, no. 3: 607. https://doi.org/10.3390/microorganisms13030607
APA StyleBagnasco, F., Lorenzini Ceradelli, F., Mesini, A., Saffioti, C., Ricci, E., Russo, C., Mariani, M., Ugolotti, E., Caci, E., Contu, D., Tavella, E., Cafaro, A., Piaggio, G., Verrina, E., Bandettini, R., & Castagnola, E. (2025). Etiology and Oral Antibiotic Susceptibility Patterns of the First Urinary Tract Infection Episode in Infants Under 6 Months of Age: A 17-Year, Retrospective, Single-Center Study in Italy. Microorganisms, 13(3), 607. https://doi.org/10.3390/microorganisms13030607