
The Incidence and Risk Factors for Enterotoxigenic E. coli Diarrheal Disease in Children under Three Years Old in Lusaka, Zambia

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Procedures
2.3. Laboratory Procedures
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic and Household Characteristics of Participants
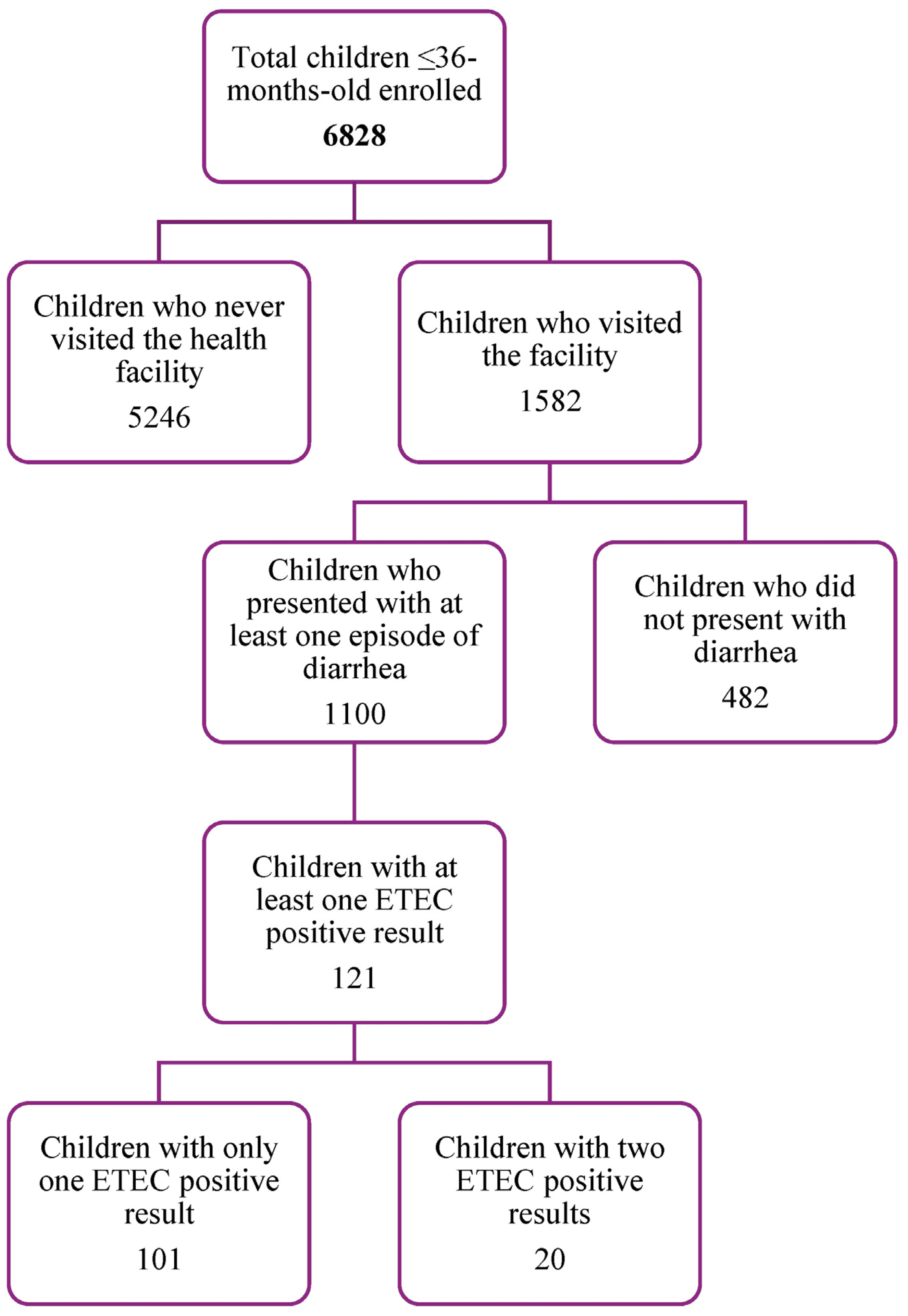
3.2. Incidence of Enterotoxigenic Escherichia coli (ETEC) Diarrhea and Associated Risk Factors
3.3. Enterotoxigenic Escherichia coli (ETEC) Characterization
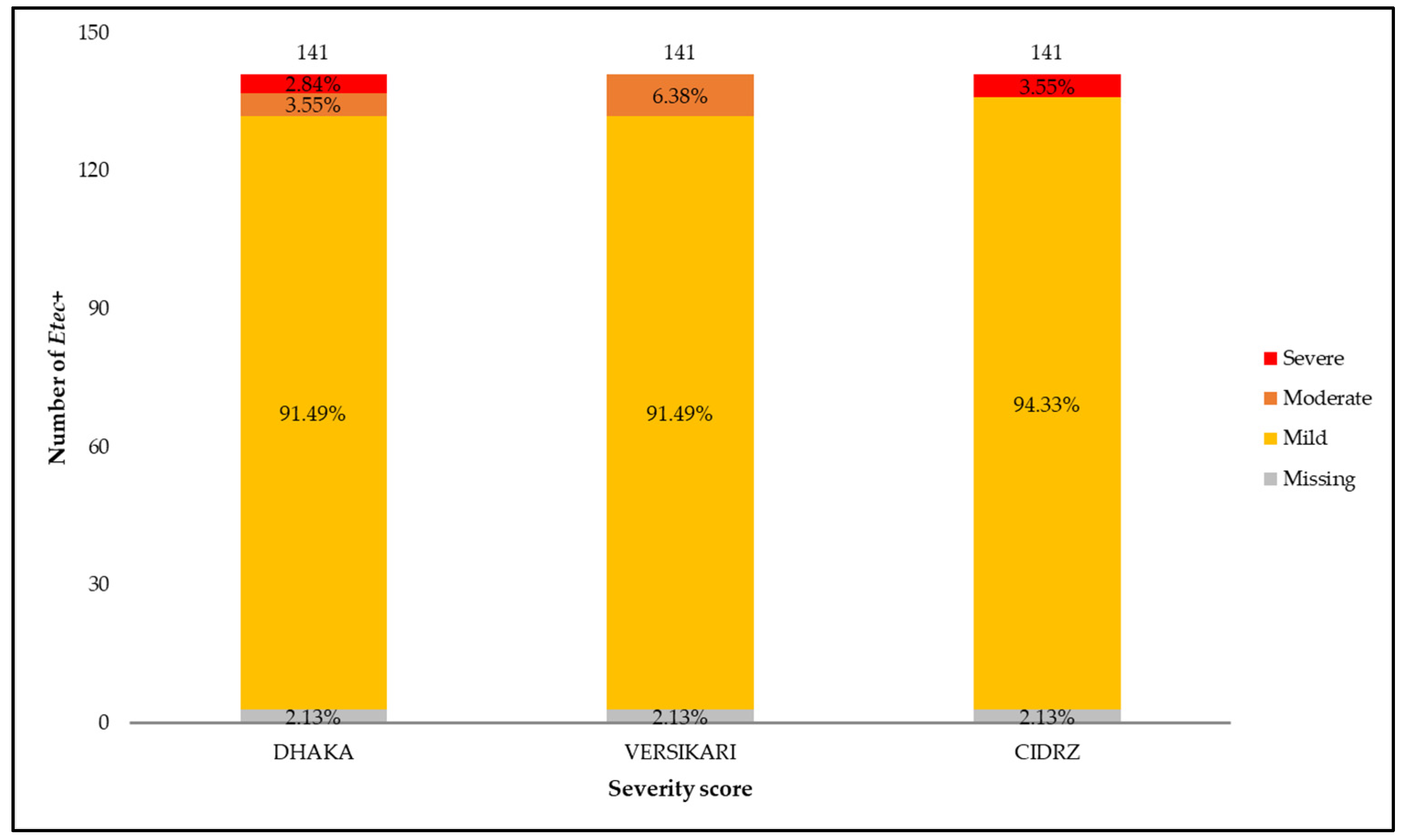
3.4. Enterotoxigenic Escherichia coli (ETEC) Diarrhea Disease Severity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Schaumburg, F.; Correa-Martinez, C.L.; Niemann, S.; Köck, R.; Becker, K. Aetiology of traveller’s diarrhea: A nested case-control study. Travel Med. Infect. Dis. 2020, 37, 101696. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.W.; Riddle, M.S.; Taylor, D.N.; DuPont, H.L. 18—Epidemiology of Travelers’ Diarrhea. In Leder KBT-TM, 4th ed.; Keystone, J.S., Kozarsky, P.E., Connor, B.A., Nothdurft, H.D., Mendelson, M., Eds.; Elsevier: London, UK, 2019; pp. 187–198. ISBN 978-0-323-54696-6. [Google Scholar] [CrossRef]
- Khalil, I.A.; Troeger, C.; Blacker, B.F.; Rao, P.C.; Brown, A.; Atherly, D.E.; Brewer, T.G.; Engmann, C.M.; Houpt, E.R.; Kang, G.; et al. Morbidity and mortality due to shigella and enterotoxigenic Escherichia coli diarrhoea: The Global Burden of Disease Study 1990–2016. Lancet Infect. Dis. 2018, 18, 1229–1240. [Google Scholar] [CrossRef] [PubMed]
- Pires, S.M.; Fischer-Walker, C.L.; Lanata, C.F.; Devleesschauwer, B.; Hall, A.J.; Kirk, M.D.; Duarte, A.S.R.; Black, R.E.; Angulo, F.J. Aetiology-specific estimates of the global and regional incidence and mortality of diarrhoeal diseases commonly transmitted through food. PLoS ONE 2015, 10, e0142927. [Google Scholar] [CrossRef] [PubMed]
- Hart, C.A.; Umar, L.W. Diarrhoeal disease. Trop. Dr. 2000, 30, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Chisenga, C.C.; Bosomprah, S.; Makabilo Laban, N.; Mwila- Kazimbaya, K.; Mwaba, J.; Simuyandi, M.; Chilengi, R. Aetiology of Diarrhoea in Children Under Five in Zambia Detected Using Luminex xTAG Gastrointestinal Pathogen Panel. Pediatr. Infect. Dis. Open Access 2018, 3, 1–6. [Google Scholar] [CrossRef]
- Wolf, J.; Hubbard, S.; Brauer, M.; Ambelu, A.; Arnold, B.F.; Bain, R.; Bauza, V.; Brown, J.; Caruso, B.A.; Clasen, T.; et al. Effectiveness of interventions to improve drinking water, sanitation, and handwashing with soap on risk of diarrhoeal disease in children in low-income and middle-income settings: A systematic review and meta-analysis. Lancet 2022, 400, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tan, P.; Zhao, Y.; Ma, X. Enterotoxigenic Escherichia coli: Intestinal pathogenesis mechanisms and colonization resistance by gut microbiota. Gut Microbes 2022, 14, 2055943. [Google Scholar] [CrossRef] [PubMed]
- Silwamba, S.; Chilyabanyama, O.N.; Liswaniso, F.; Chisenga, C.C.; Chilengi, R.; Dougan, G.; Kwenda, G.; Chakraborty, S.; Simuyandi, M. Field evaluation of a novel, rapid diagnostic assay, and molecular epidemiology of enterotoxigenic E. coli among Zambian children presenting with diarrhea. PLoS Negl. Trop. Dis. 2022, 16, e0010207. [Google Scholar] [CrossRef]
- Khalil, I.; Walker, R.; Porter, C.K.; Muhib, F.; Chilengi, R.; Cravioto, A.; Guerrant, R.; Svennerholm, A.-M.; Qadri, F.; Baqar, S.; et al. Enterotoxigenic Escherichia coli (ETEC) vaccines: Priority activities to enable product development, licensure, and global access. Vaccine 2021, 39, 4266–4277. [Google Scholar] [CrossRef]
- Farfán-García, A.E.; Zhang, C.; Imdad, A.; Arias-Guerrero, M.Y.; Sánchez-Alvarez, N.T.; Shah, R.; Iqbal, J.; Tamborski, M.E.; Gómez-Duarte, O.G. Case-control pilot study on acute diarrheal disease in a geographically defined pediatric population in a middle income country. Int. J. Pediatr. 2017, 2017, 6357597. [Google Scholar] [CrossRef]
- Sjoling, A.; Wiklund, G.; Savarino, S.J.; Cohen, D.I.; Svennerholm, A.-M. Comparative analyses of phenotypic and genotypic methods for detection of enterotoxigenic Escherichia coli toxins and colonization factors. J. Clin. Microbiol. 2007, 45, 3295–3301. [Google Scholar] [CrossRef]
- Levine, A.C.; Glavis-Bloom, J.; Modi, P.; Nasrin, S.; Atika, B.; Rege, S.; Robertson, S.; Schmid, C.H.; Alam, N.H. External validation of the DHAKA score and comparison with the current IMCI algorithm for the assessment of dehydration in children with diarrhoea: A prospective cohort study. Lancet Glob. Health 2016, 4, e744–e751. [Google Scholar] [CrossRef] [PubMed]
- Schnadower, D.; Tarr, P.I.; Gorelick, M.H.; O’Connell, K.; Roskind, C.G.; Powell, E.C.; Rao, J.; Bhatt, S.; Freedman, S.B. Validation of the Modified Vesikari Score in Children with Gastroenteritis in 5 US Emergency Departments. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 514–519. [Google Scholar] [CrossRef] [PubMed]
- St Jean, D.T.; Chilyabanyama, O.N.; Bosomprah, S.; Asombang, M.; Velu, R.M.; Chibuye, M.; Mureithi, F.; Sukwa, N.; Chirwa, M.; Mokha, P. Development of a diarrhoea severity scoring scale in a passive health facility-based surveillance system. PLoS ONE 2022, 17, e0272981. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Szucs, T.D.; Steffen, R. Economic aspects of travelers’ diarrhea. J. Travel Med. 2008, 15, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Dupont, H.L.; Ericsson, C.D.; Farthing, M.J.G.; Gorbach, S.; Pickering, L.K.; Rombo, L.; Steffen, R.; Weinke, T. Expert review of the evidence base for prevention of travelers’ diarrhea. J. Travel Med. 2009, 16, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Isidean, S.D.; Riddle, M.S.; Savarino, S.J.; Porter, C.K. A systematic review of ETEC epidemiology focusing on colonization factor and toxin expression. Vaccine 2011, 29, 6167–6178. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, S.; von Mentzer, A.; Begum, Y.A.; Manzur, M.; Hasan, M.; Ghosh, A.N.; Hossain, M.A.; Camilli, A.; Qadri, F. Phenotypic and genomic analyses of bacteriophages targeting environmental and clinical CS3-expressing enterotoxigenic Escherichia coli (ETEC) strains. PLoS ONE 2018, 13, e0209357. [Google Scholar] [CrossRef] [PubMed]
- Svennerholm, A.-M. From cholera to enterotoxigenic Escherichia coli (ETEC) vaccine development. Indian J. Med. Res. 2011, 133, 188–196. [Google Scholar]
- Simuyandi, M.; Chilengi, R.; Connor, S.B.; Voeglein, J.B.; Laban, N.M.; Mwila-Kazimbaya, K.; Chisenga, C.C.; Mwaba, J.; Sack, D.A.; Chakraborty, S. Enterotoxigenic Escherichia Coli Toxins and Colonization Factors Among Zambian Children Presenting with Moderate to Severe Diarrhea to Selected Health Facilities. Arch. Microbiol. Immunol. 2019, 3, 173–184. [Google Scholar] [CrossRef]
- Jiang, Z.-D.; Lowe, B.; Verenkar, M.P.; Ashley, D.; Steffen, R.; Tornieporth, N.; von Sonnenburg, F.; Waiyaki, P.; DuPont, H.L. Prevalence of Enteric Pathogens among International Travelers with Diarrhea Acquired in Kenya (Mombasa), India (Goa), or Jamaica (Montego Bay). J. Infect. Dis. 2002, 185, 497–502. [Google Scholar] [CrossRef]
- Işeri, L.; Zafer Apan, T.; Aksoy, A.; Koç, F.; Sedef Göçmen, J.; Nuristani, D. The prevalence of enterotoxigenic e. Coli isolated from the stools of children aged 0-10 years with diarrhea in mid-anatolia region, Turkey. Braz. J. Microbiol. 2011, 42, 243–247. [Google Scholar] [CrossRef]
- Turunen, K.; Antikainen, J.; Lääveri, T.; Kirveskari, J.; Svennerholm, A.-M.; Kantele, A. Clinical aspects of heat-labile and heat-stable toxin-producing enterotoxigenic Escherichia coli: A prospective study among Finnish travellers. Travel Med. Infect. Dis. 2020, 38, 101855. [Google Scholar] [CrossRef] [PubMed]
- Kipkirui, E.; Koech, M.; Ombogo, A.; Kirera, R.; Ndonye, J.; Kipkemoi, N.; Kirui, M.; Philip, C.; Roth, A.; Flynn, A.; et al. Molecular characterization of enterotoxigenic Escherichia coli toxins and colonization factors in children under five years with acute diarrhea attending Kisii Teaching and Referral Hospital, Kenya. Trop. Dis. Travel Med. Vaccines 2021, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Trainor, E.; Iturriza-Gómara, M.; Ngwira, B.; Cunliffe, N. Detection of enterotoxigenic E. coli in hospitalised children with and without diarrhoea in Blantyre, Malawi. Paediatr. Int. Child Health 2016, 36, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Thea, D.M.; St. Louis, M.E.; Atido, U.; Kanjinga, K.; Kembo, B.; Matondo, M.; Tshiamala, T.; Kamenga, C.; Davachi, F.; Brown, C.; et al. A Prospective Study of Diarrhea and HIV-1 Infection among 429 Zairian Infants. N. Engl. J. Med. 1993, 329, 1696–1702. [Google Scholar] [CrossRef] [PubMed]
- Basile, F.W.; Fedele, M.C.; Lo Vecchio, A. Gastrointestinal Diseases in Children Living with HIV. Microorganisms 2021, 9, 1572. [Google Scholar] [CrossRef] [PubMed]
- van Eijk, A.M.; Brooks, J.T.; Adcock, P.M.; Garrett, V.; Eberhard, M.; Rosen, D.H.; Ayisi, J.G.; Ochieng, J.B.; Kumar, L.; Gentsch, J.R.; et al. Diarrhea in children less than two years of age with known HIV status in Kisumu, Kenya. Int. J. Infect. Dis. 2010, 14, e220–e225. [Google Scholar] [CrossRef] [PubMed]
- Pavlinac, P.B.; John-Stewart, G.C.; Naulikha, J.M.; Onchiri, F.M.; Denno, D.M.; Odundo, E.A.; Singa, B.O.; Richardson, B.A.; Walson, J.L. High-risk enteric pathogens associated with HIV infection and HIV exposure in Kenyan children with acute diarrhoea. AIDS 2014, 28, 2287–2296. [Google Scholar] [CrossRef] [PubMed]
- Bejide, O.S.; Odebode, M.A.; Ogunbosi, B.O.; Adekanmbi, O.; Akande, K.O.; Ilori, T.; Ogunleye, V.O.; Nwachukwu, V.U.; Grey-Areben, A.; Akande, E.T.; et al. Diarrhoeal pathogens in the stools of children living with HIV in Ibadan, Nigeria. Front. Cell. Infect. Microbiol. 2023, 13, 1108923. [Google Scholar] [CrossRef]
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef]
- Chakravarty, I.; Bhattacharya, A.; Das, S.K. Water, sanitation and hygiene: The unfinished agenda in the World Health Organization South-East Asia Region. WHO South-East Asia J. Public Health 2017, 6, 22–33. [Google Scholar] [CrossRef]
- Nyambe, S.; Yamauchi, T. Peri-urban water, sanitation and hygiene in Lusaka, Zambia: Photovoice empowering local assessment via ecological theory. Glob. Health Promot. 2021, 29, 66–76. [Google Scholar] [CrossRef]
- Ministry of Finance and National Planning. Republic of Zambia, Eighth national development plan (8NDP) 2022–2026; 2022. Available online: https://www.mot.gov.zm/?wpdmpro=eighth-national-development-plan-8ndp-2022-2026 (accessed on 17 September 2023).
- Le, K.; Nguyen, M. Shedding light on maternal education and child health in developing countries. World Dev. 2020, 133, 105005. [Google Scholar] [CrossRef]
- de Buhr, E.; Tannen, A. Parental health literacy and health knowledge, behaviours and outcomes in children: A cross-sectional survey. BMC Public Health 2020, 20, 1096. [Google Scholar] [CrossRef] [PubMed]
- Vanneman, R.; Vikram, K. Maternal education and the multidimensionality of child health outcomes in India. J. Biosoc. Sci. 2020, 52, 57–77. [Google Scholar] [CrossRef]
- Vikram, K.; Vanneman, R.; Desai, S. Linkages between maternal education and childhood immunization in India. Soc. Sci. Med. 2012, 75, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Vidal, R.M.; Muhsen, K.; Tennant, S.M.; Svennerholm, A.-M.; Sow, S.O.; Sur, D.; Zaidi, A.K.M.; Faruque, A.S.G.; Saha, D.; Adegbola, R.; et al. Colonization factors among enterotoxigenic Escherichia coli isolates from children with moderate-to-severe diarrhea and from matched controls in the Global Enteric Multicenter Study (GEMS). PLoS Negl. Trop. Dis. 2019, 13, e0007037. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Children Enrolled N (% of Total) | |
|---|---|
| Characteristics | 6828 (100) |
| Catchment area | |
| Chainda-South | 1371 (20.1) |
| Chawama | 1370 (20.1) |
| George | 1364 (20.0) |
| Kanyama | 1358 (19.9) |
| Matero | 1365 (20.0) |
| Household size | |
| <5 | 2935 (43.0) |
| 5+ | 3893 (57.0) |
| Age group in months | |
| 0 to 5 | 1032 (15.1) |
| 6 to <12 | 1349 (19.8) |
| 12 to <18 | 1299 (19.0) |
| 18 to <24 | 1167 (17.1) |
| 24 to 36 | 1981 (29.0) |
| Gender | |
| Male | 3454 (50.6) |
| Female | 3374 (49.4) |
| Stunted * | |
| No | 2220 (32.5) |
| Yes | 3762 (55.1) |
| Missing | 846 (12.4) |
| Wasted * | |
| No | 5504 (80.6) |
| Yes | 286 (4.2) |
| Missing | 1038 (15.2) |
| Underweight * | |
| No | 5021 (73.5) |
| Yes | 991 (14.5) |
| Missing | 816 (12.0) |
| MUAC * | |
| Normal: >12.5 cm | 5581 (81.7) |
| Moderate and severe acute malnutrition: ≤12.5 cm | 347 (5.1) |
| Missing | 900 (13.2) |
| Child HIV status | |
| Negative | 6107 (89.4) |
| Positive | 370 (5.4) |
| Missing | 351 (5.1) |
| Rotarix vaccination status * | |
| No—1 dose only or not vaccinated | 5536 (81.1) |
| Yes—Received both doses | 1169 (17.1) |
| Missing | 123 (1.8) |
| Mother breastfeed child | |
| Yes | 6660 (97.5) |
| No | 120 (1.8) |
| Missing | 48 (0.7) |
| Mothers HIV status | |
| Negative | 5582 (81.8) |
| Positive | 1003 (14.7) |
| Missing | 243 (3.6) |
| Primary caregiver * | |
| Mother | 6006 (88.0) |
| Other | 822 (12.0) |
| Mother’s highest level of education * | |
| None/Primary/Junior Secondary/Other | 4194 (61.4) |
| Senior Secondary/University/Tertiary | 2634 (38.6) |
| Drinking water source * | |
| Piped into house/Piped water into yard | 3052 (44.7) |
| Public tap/Borehole/Well | 3629 (53.1) |
| Sachet/Bottled/Filtered/Other | 147 (2.2) |
| Treated water | |
| No | 3915 (57.3) |
| Yes | 2913 (42.7) |
| Toilet facility | |
| Pit latrine | 4548 (66.6) |
| Flush toilet | 2211 (32.4) |
| No facility | 69 (1.0) |
| WASH * | |
| Improved toilet and water and good hand washing | 1657 (24.3) |
| Unimproved toilet and water and bad hand washing | 5171 (75.7) |
| Head of Household gender | |
| Male | 5430 (79.5) |
| Female | 1398 (20.5) |
| Household head marital status * | |
| Married/Cohabiting | 5820 (85.2) |
| Single/Divorced/Separated/Widowed | 1008 (14.8) |
| Household head age group | |
| 17–35 | 3481 (51.0) |
| 36–49 | 2445 (35.8) |
| 50+ | 902 (13.2) |
| ETEC + Diarrhea Episodes n | Number of Child Years Y | Incidence Rate per 100 CY IR (95% CI) | Univariable HR (95% CI) | p-Value | Multivariable aHR (95% CI) | p-Value | |
|---|---|---|---|---|---|---|---|
| Characteristics | 141 | 5697.37 | 2.47 (2.10–2.92) | - | - | - | - |
| Household size | |||||||
| <5 | 70 | 2435.4 | 2.87 (2.27–3.63) | 1 | 0.145 | ||
| 5+ | 71 | 3262 | 2.18 (1.72–2.75) | 0.76 (0.52–1.1) | |||
| Age group in months | |||||||
| 0 to 5 | 28 | 865.85 | 3.23 (2.23–4.68) | 1 | 0.083 | ||
| 6 to <12 | 32 | 1125.83 | 2.84 (2.01–4.02) | 0.88 (0.49–1.57) | |||
| 12 to <18 | 33 | 1073.43 | 3.07 (2.19–4.32) | 0.95 (0.54–1.66) | |||
| 18 to <24 | 23 | 968.68 | 2.37 (1.58–3.57) | 0.73 (0.4–1.36) | |||
| 24 to 36 | 25 | 1663.58 | 1.5 (1.02–2.22) | 0.46 (0.26–0.85) | |||
| Gender | |||||||
| Male | 67 | 2882.1 | 2.32 (1.83–2.95) | 1 | 0.515 | ||
| Female | 74 | 2815.3 | 2.63 (2.09–3.3) | 1.13 (0.78–1.64) | |||
| Stunted * | |||||||
| No | 41 | 1858.84 | 2.21 (1.62–3) | 1 | 0.356 | ||
| Yes | 85 | 3156.85 | 2.69 (2.18–3.33) | 1.22 (0.8–1.87) | |||
| Wasted * | |||||||
| No | 117 | 4604.86 | 2.54 (2.12–3.05) | 1 | 0.918 | ||
| Yes | 6 | 246.92 | 2.43 (1.09–5.41) | 0.96 (0.42–2.17) | |||
| Underweight * | |||||||
| No | 96 | 4198.07 | 2.29 (1.87–2.79) | 1 | 0.027 | ||
| Yes | 31 | 840.41 | 3.69 (2.59–5.25) | 1.62 (1.05–2.47) | |||
| MUAC * | |||||||
| Normal: >12.5 cm | 115 | 4682.47 | 2.46 (2.05–2.95) | 1 | 0.072 | ||
| Moderate and severe acute malnutrition: ≤12.5 cm | 13 | 293.47 | 4.43 (2.57–7.63) | 1.81 (0.95–3.45) | |||
| Child HIV status | |||||||
| Negative | 115 | 5092.48 | 2.26 (1.88–2.71) | 1 | <0.001 | 1 | 0.017 |
| Positive | 20 | 318.55 | 6.28 (4.05–9.73) | 2.78 (1.64–4.72) | 2.14 (1.14–3.99) | ||
| Rotarix vaccination status at 6 and 10 weeks * | |||||||
| No—1 dose only or not vaccinated | 112 | 4629.62 | 2.42 (2.01–2.91) | 1 | 0.364 | ||
| Yes—Received both doses | 29 | 972.38 | 2.98 (2.07–4.29) | 1.23 (0.79–1.93) | |||
| Mother breastfeed child | |||||||
| Yes | 140 | 5557.64 | 2.52 (2.13–2.97) | 1 | 0.351 | ||
| No | 1 | 101.23 | 0.99 (0.14–7.01) | 0.39 (0.06–2.8) | |||
| Mothers HIV status | |||||||
| Negative | 102 | 4664.76 | 2.19 (1.8–2.65) | 1 | <0.001 | ||
| Positive | 37 | 836.3 | 4.42 (3.21–6.11) | 2.03 (1.34–3.06) | |||
| Primary caregiver * | |||||||
| Mother | 132 | 5010.11 | 2.63 (2.22–3.12) | 1 | 0.065 | ||
| Other | 9 | 687.26 | 1.31 (0.68–2.52) | 0.5 (0.24–1.04) | |||
| Mother’s highest level of education * | |||||||
| None—Junior Secondary | 111 | 3511.2 | 3.16 (2.62–3.81) | 1 | <0.001 | 1 | 0.008 |
| Senior Secondary—Tertiary | 30 | 2186.2 | 1.37 (0.96–1.96) | 0.44 (0.28–0.68) | 0.49 (0.29–0.83) | ||
| Drinking water source * | |||||||
| Piped water—house/yard | 28 | 2516.62 | 1.11 (0.77–1.61) | 1 | <0.001 | 1 | |
| Public tap/Borehole/Well | 107 | 3053.92 | 3.5 (2.9–4.23) | 3.15 (1.99–4.99) | 2.45 (1.48–4.06) | 0.002 | |
| Sachet/Bottled/Filtered/Other | 6 | 126.83 | 4.73 (2.13–10.53) | 4.3 (1.59–11.65) | 2.99 (0.84–10.57) | ||
| Anything done to water to make it safe to drink | |||||||
| No | 78 | 3250.6 | 2.4 (1.92–3) | 1 | 0.699 | ||
| Yes | 63 | 2446.7 | 2.57 (2.01–3.3) | 1.08 (0.74–1.56) | |||
| Toilet facility | |||||||
| Pit latrine | 116 | 3820.35 | 3.04 (2.53–3.64) | 1 | 0.002 | ||
| Flush toilet | 22 | 1819.85 | 1.21 (0.8–1.84) | 0.4 (0.23–0.68) | |||
| No facility | 3 | 57.18 | 5.25 (1.69–16.27) | 1.72 (0.56–5.28) | |||
| WASH * | |||||||
| Improved toilet and water and good hand washing | 15 | 1358.1 | 1.1 (0.67–1.83) | 1 | 0.003 | ||
| Unimproved toilet and water and bad hand washing | 126 | 4339.3 | 2.9 (2.44–3.46) | 2.63 (1.4–4.93) | |||
| Head of Household gender | |||||||
| Male | 106 | 4527.1 | 2.34 (1.94–2.83) | 1 | 0.265 | ||
| Female | 35 | 1170.3 | 2.99 (2.15–4.17) | 1.28 (0.83–1.98) | |||
| Household head marital status * | |||||||
| Married/Cohabitating | 123 | 4853.27 | 2.53 (2.12–3.02) | 1 | 0.539 | ||
| Single/Divorced/Separated/Widowed | 18 | 844.1 | 2.13 (1.34–3.38) | 0.84 (0.49–1.45) | |||
| Household head age group | |||||||
| 17–35 | 81 | 2901.55 | 2.79 (2.25–3.47) | 1 | 0.391 | ||
| 36–49 | 44 | 2034.54 | 2.16 (1.61–2.91) | 0.78 (0.51–1.17) | |||
| 50+ | 16 | 761.28 | 2.1 (1.29–3.43) | 0.76 (0.42–1.37) |
| Enterotoxin | Total n = 125 * | None (n = 80, 64%) | CFA/I (n = 1, 0.8%) | CS1, CS3 (n = 1, 0.8%) | CS2, CS3 (n = 12, 9.6%) | CS3 (n = 2, 1.6%) | CS5, CS6, CS7 (n = 4, 3.2%) | CS17 (n = 3, 2.4%) | CS6 (n = 10, 8%) | CS7 (n = 4, 3.2%) | CS14 (n = 7, 5.6%) | CS17 (n = 1, 0.8%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| LT | 59 (47.2) | 44 (74.6) | 0 (0.0) | 0 (0.0) | 3 (5.1) | 0 (0.0) | 1 (1.7) | 3 (5.1) | 4 (6.8) | 3 (5.1) | 1 (1.7) | 0 (0.0) |
| LT/STh | 13 (10.4) | 5 (38.5) | 0 (0.0) | 0 (0.0) | 6 (46.2) | 2 (15.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| LT/STp | 7 (5.6) | 4 (57.1) | 0 (0.0) | 0 (0.0) | 2 (28.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| STh | 25 (20.0) | 13 (52.0) | 0 (0.0) | 1 (4.0) | 1 (4.0) | 0 (0.0) | 2 (8.0) | 0 (0.0) | 2 (8.0) | 0 (0.0) | 6 (24.0) | 0 (0.0) |
| STh/STp | 1 (0.8) | 1 (100.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| STp | 20 (16.0) | 13 (65.0) | 1 (5.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (5.0) | 0 (0.0) | 3 (15.0) | 1 (5.0) | 0 (0.0) | 1 (5.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sukwa, N.; Bosomprah, S.; Somwe, P.; Muyoyeta, M.; Mwape, K.; Chibesa, K.; Luchen, C.C.; Silwamba, S.; Mulenga, B.; Munyinda, M.; et al. The Incidence and Risk Factors for Enterotoxigenic E. coli Diarrheal Disease in Children under Three Years Old in Lusaka, Zambia. Microorganisms 2024, 12, 698. https://doi.org/10.3390/microorganisms12040698
Sukwa N, Bosomprah S, Somwe P, Muyoyeta M, Mwape K, Chibesa K, Luchen CC, Silwamba S, Mulenga B, Munyinda M, et al. The Incidence and Risk Factors for Enterotoxigenic E. coli Diarrheal Disease in Children under Three Years Old in Lusaka, Zambia. Microorganisms. 2024; 12(4):698. https://doi.org/10.3390/microorganisms12040698
Chicago/Turabian StyleSukwa, Nsofwa, Samuel Bosomprah, Paul Somwe, Monde Muyoyeta, Kapambwe Mwape, Kennedy Chibesa, Charlie Chaluma Luchen, Suwilanji Silwamba, Bavin Mulenga, Masiliso Munyinda, and et al. 2024. "The Incidence and Risk Factors for Enterotoxigenic E. coli Diarrheal Disease in Children under Three Years Old in Lusaka, Zambia" Microorganisms 12, no. 4: 698. https://doi.org/10.3390/microorganisms12040698
APA StyleSukwa, N., Bosomprah, S., Somwe, P., Muyoyeta, M., Mwape, K., Chibesa, K., Luchen, C. C., Silwamba, S., Mulenga, B., Munyinda, M., Muzazu, S., Chirwa, M., Chibuye, M., Simuyandi, M., Chilengi, R., & Svennerholm, A.-M. (2024). The Incidence and Risk Factors for Enterotoxigenic E. coli Diarrheal Disease in Children under Three Years Old in Lusaka, Zambia. Microorganisms, 12(4), 698. https://doi.org/10.3390/microorganisms12040698