
Improvements in Gut Microbiome Composition Predict the Clinical Efficacy of a Novel Synbiotics Formula in Children with Mild to Moderate Atopic Dermatitis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Recruitment and Study Design
2.2. Library Preparation and 16S rRNA Sequencing
2.3. Probiotic Mixture
2.4. Quantitative Real-Time PCR
2.5. Bioinformatics Analysis
2.6. Statistical Analysis
3. Results
3.1. Study Cohort
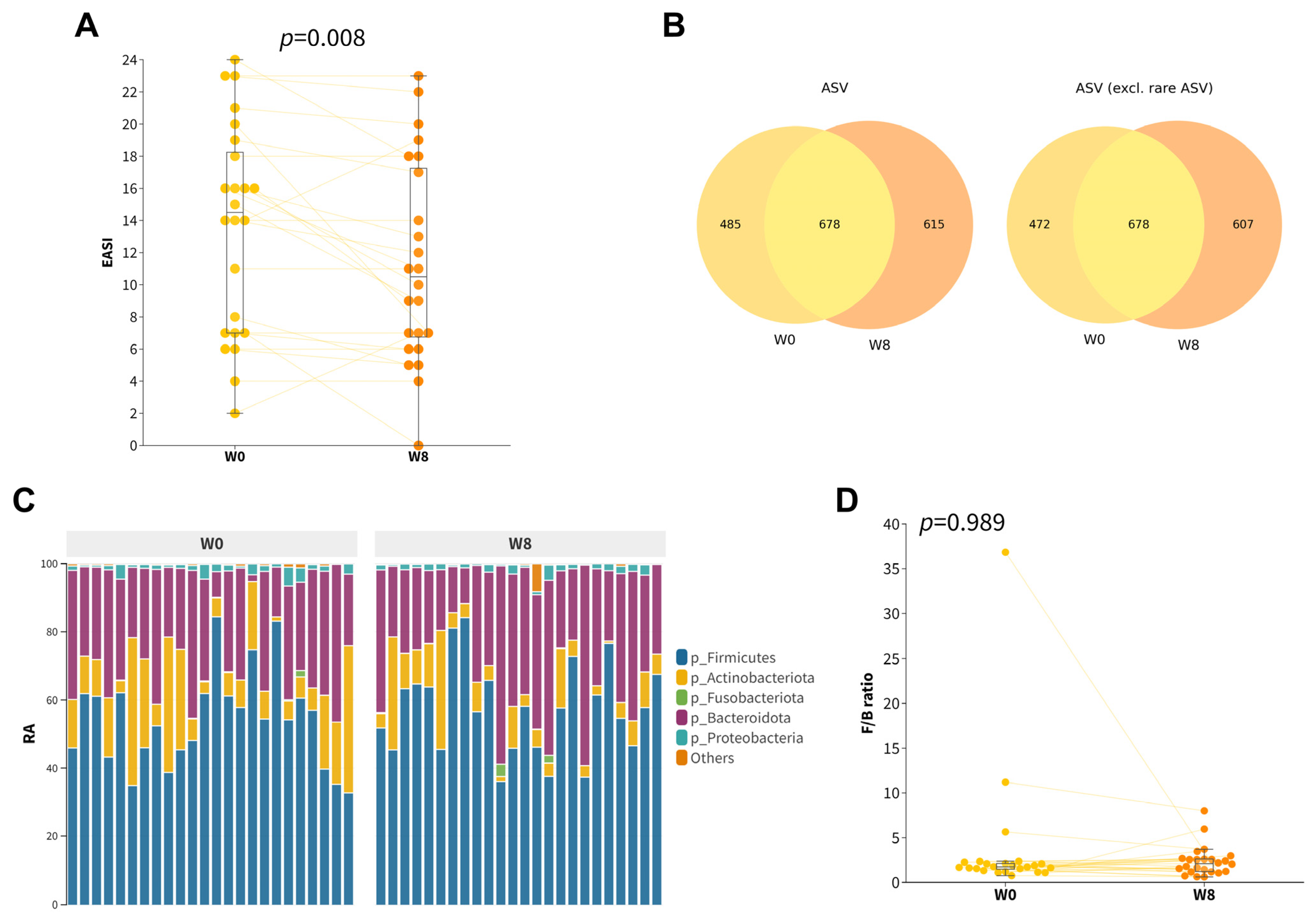
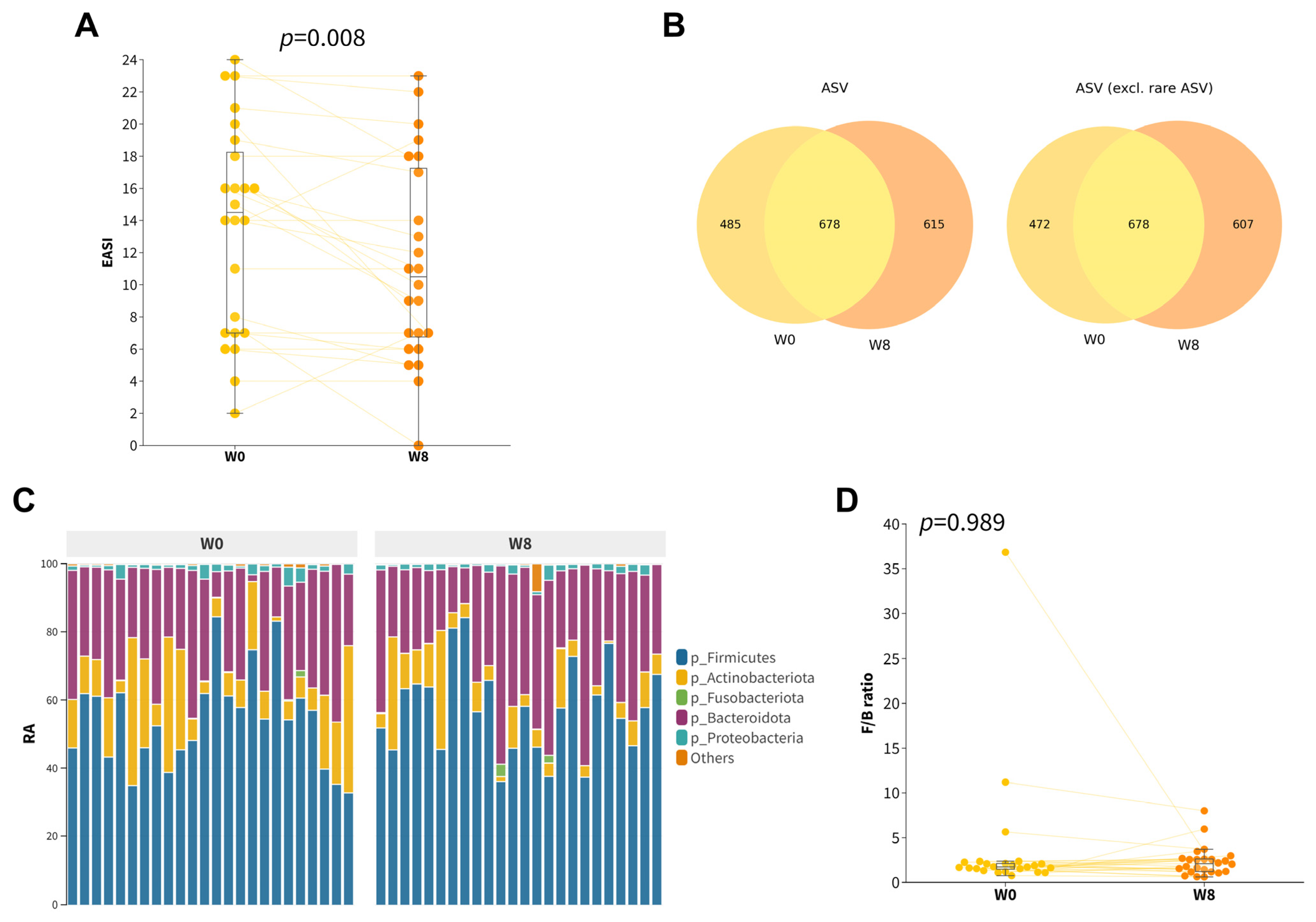
3.2. Effect of 8-Week Probiotic Intake on Gut Microbiome Composition
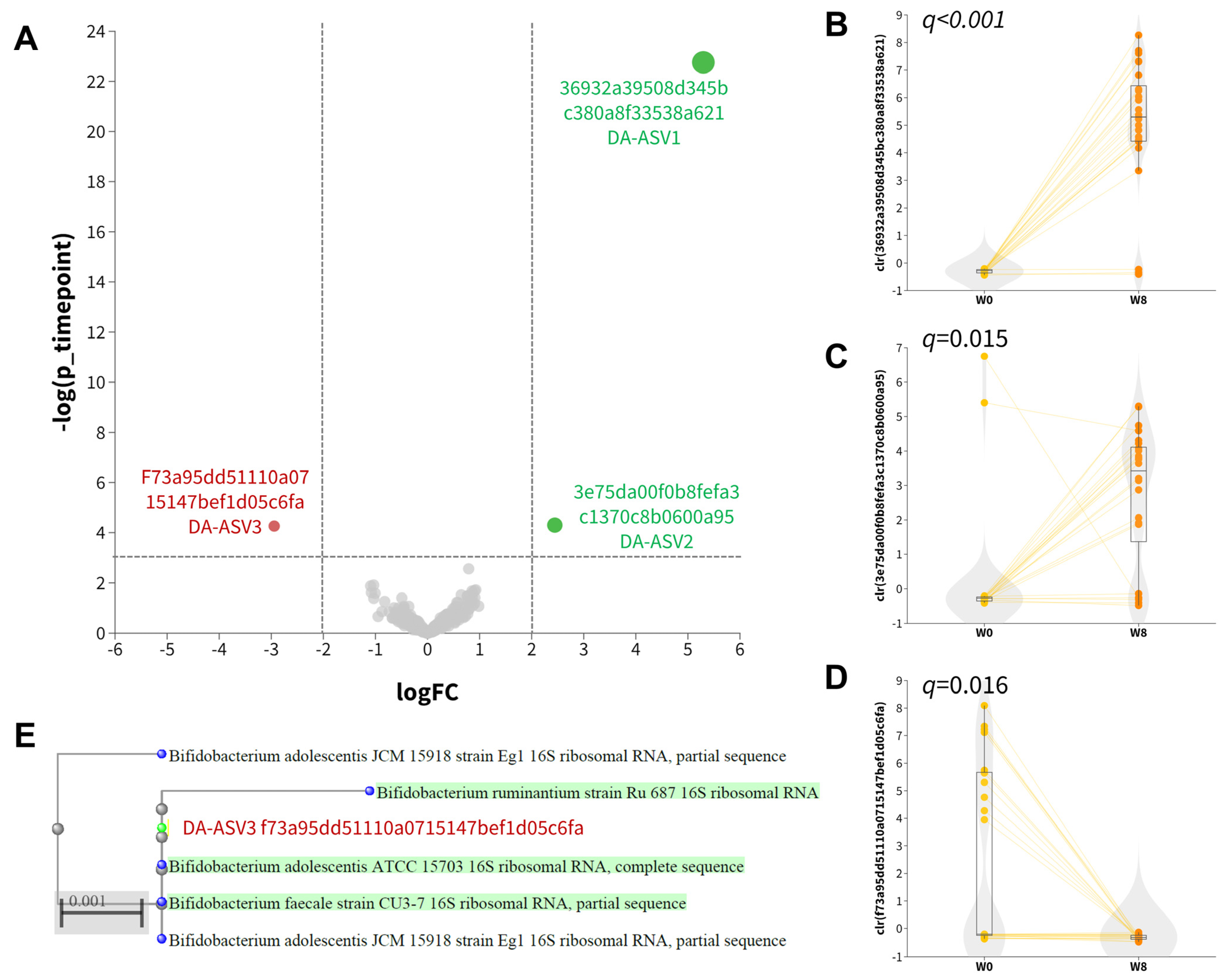
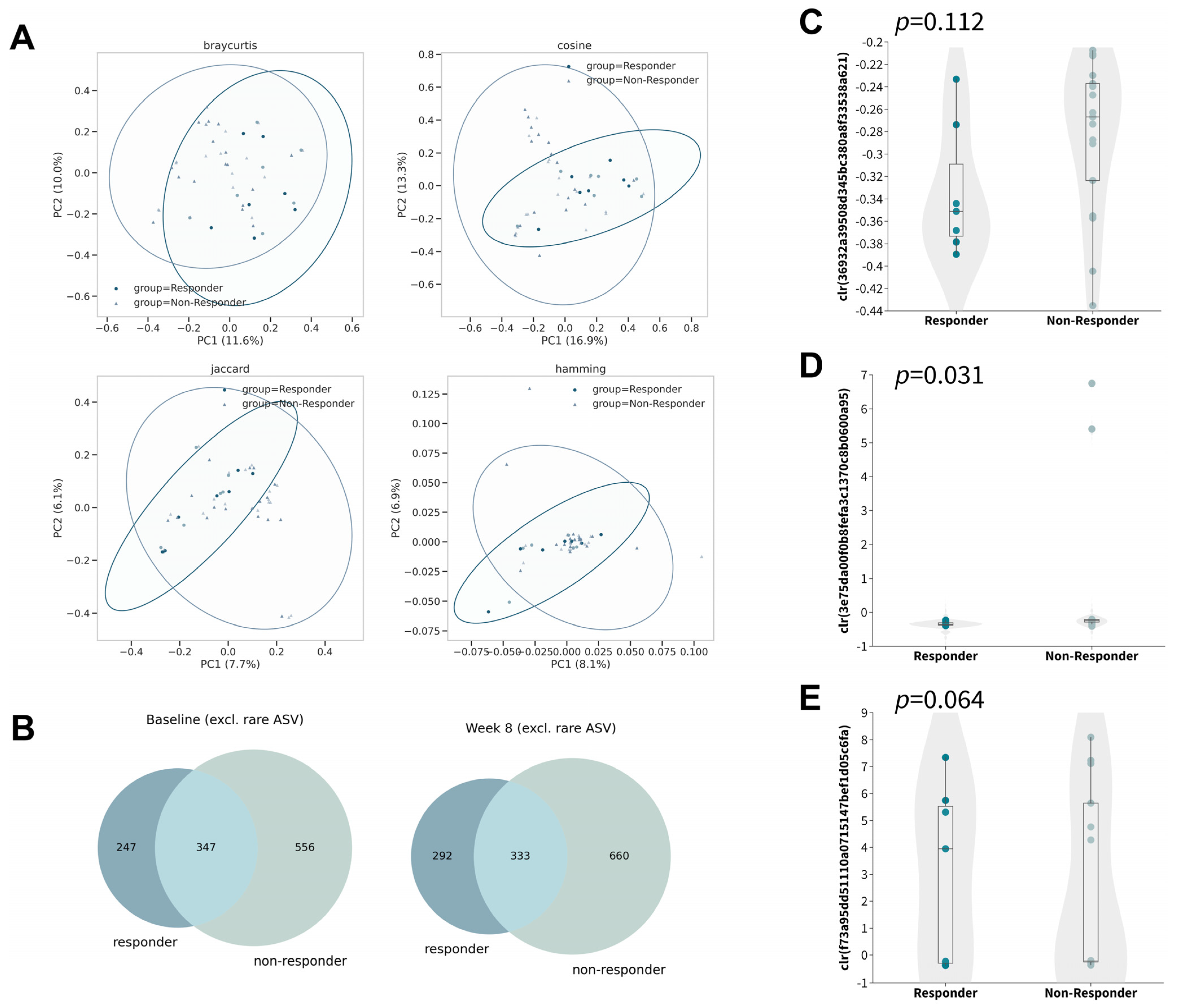
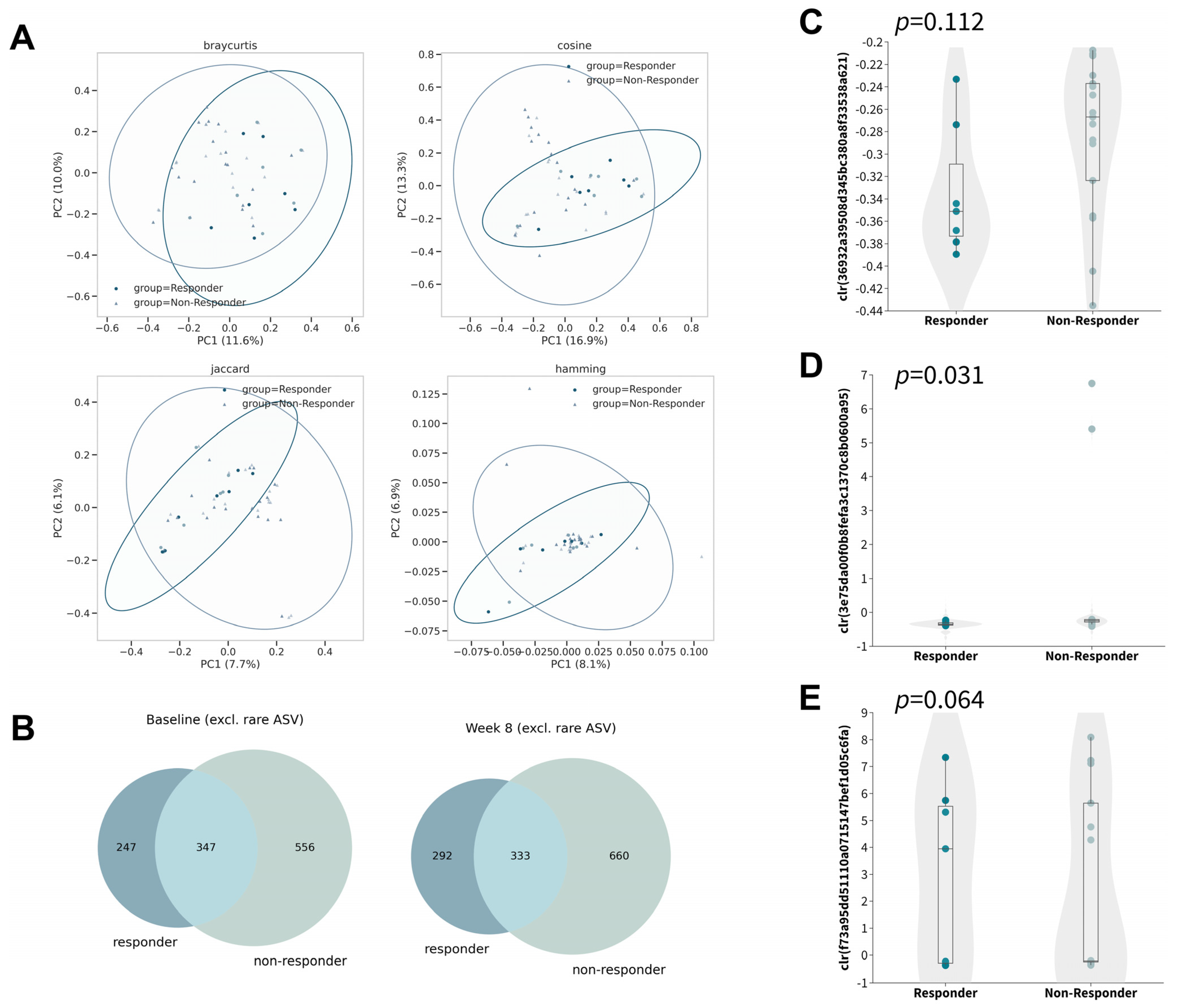
3.3. Distinctive Changes in the Gut Microbiota among Responders
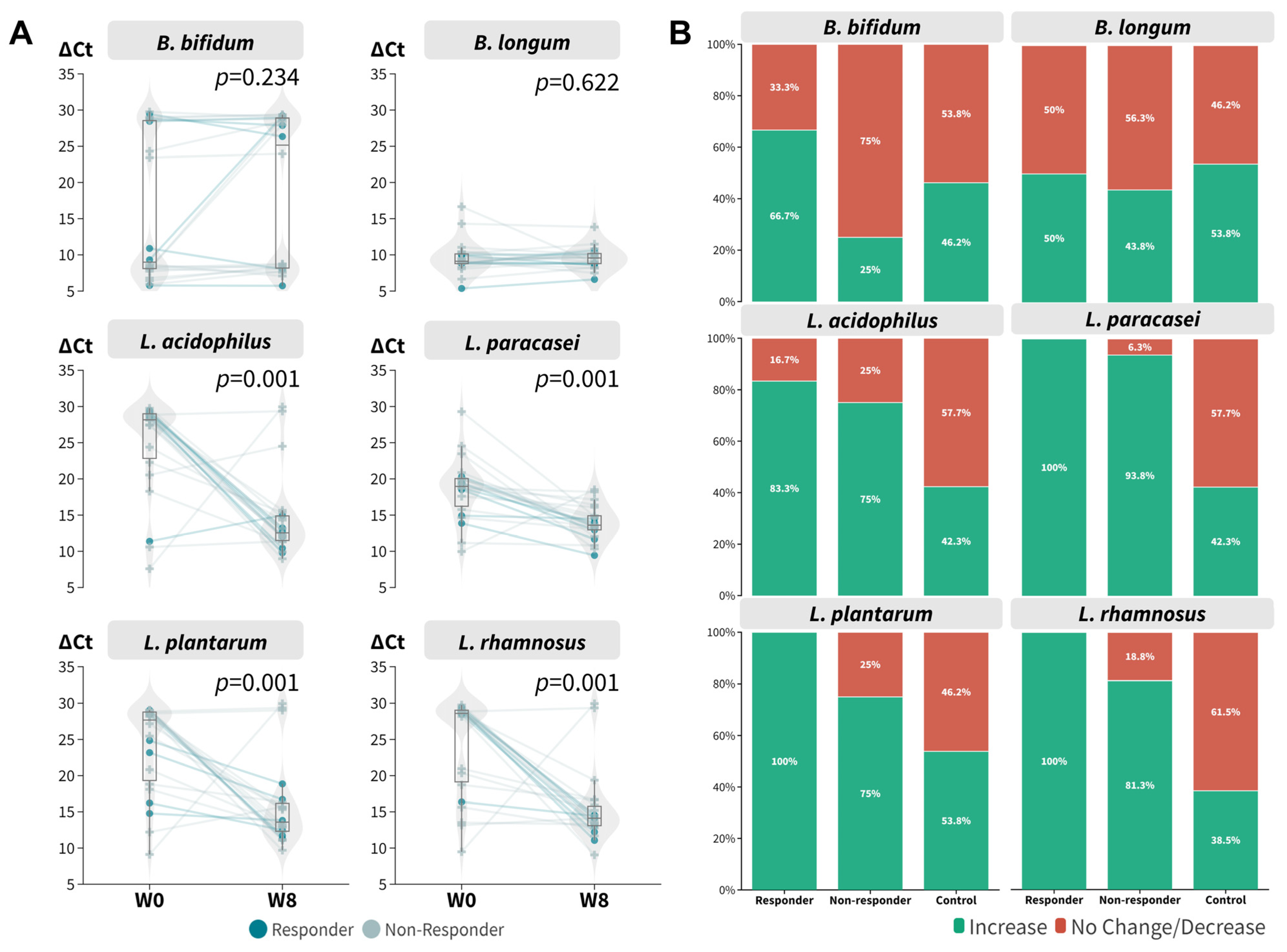
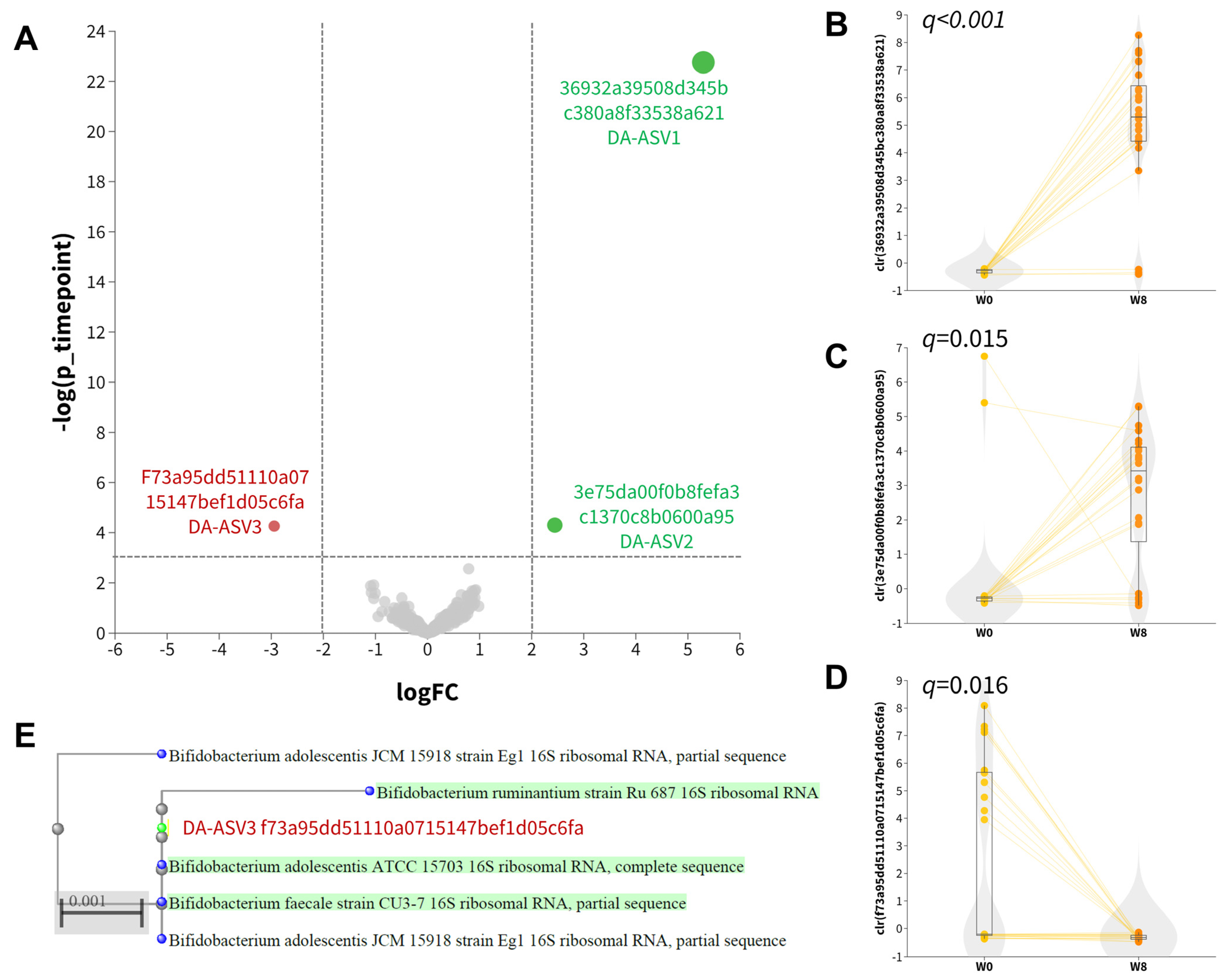
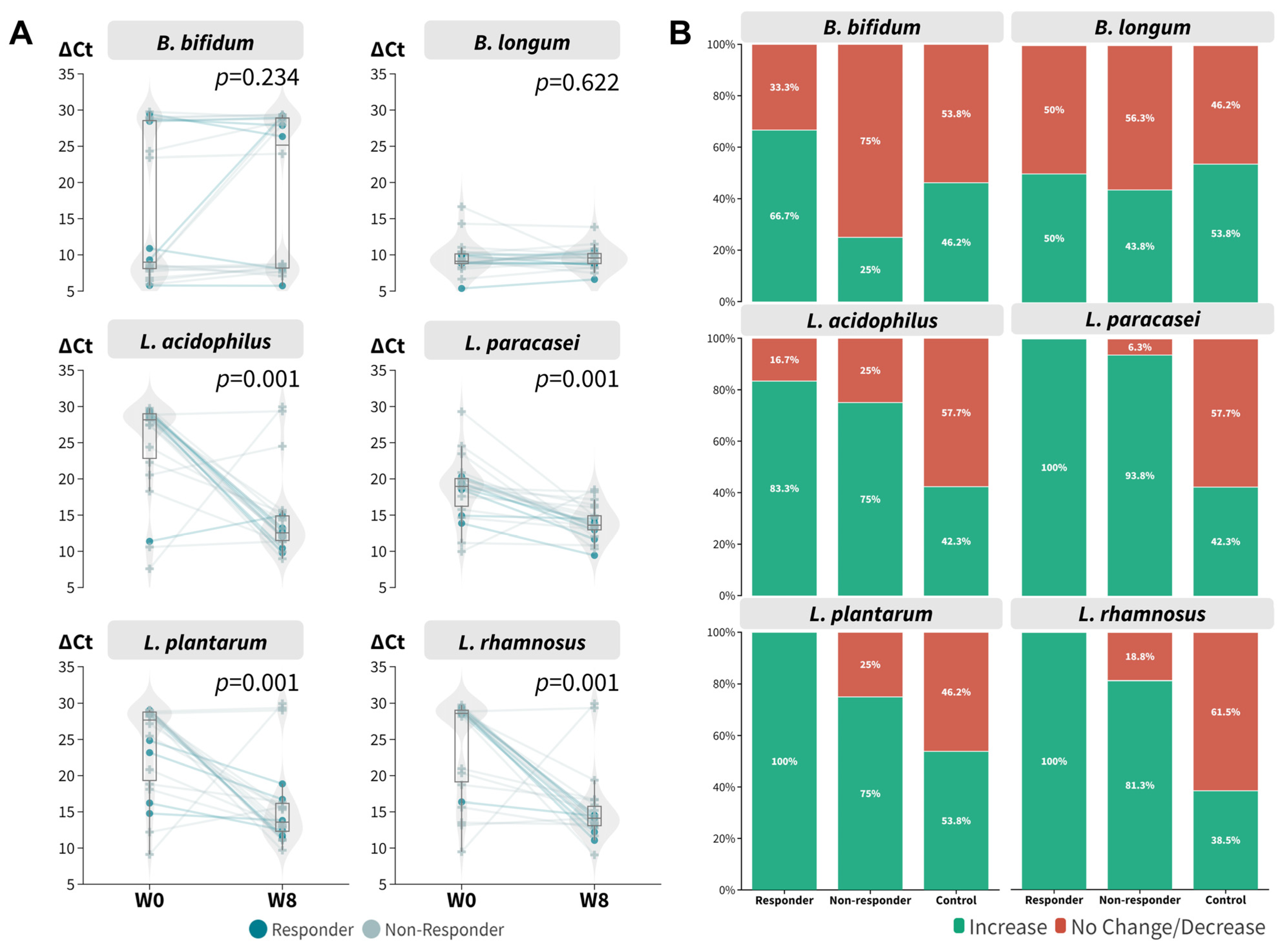
3.4. The Dynamics of Probiotic Species in Relation to Probiotic Intake Responsiveness
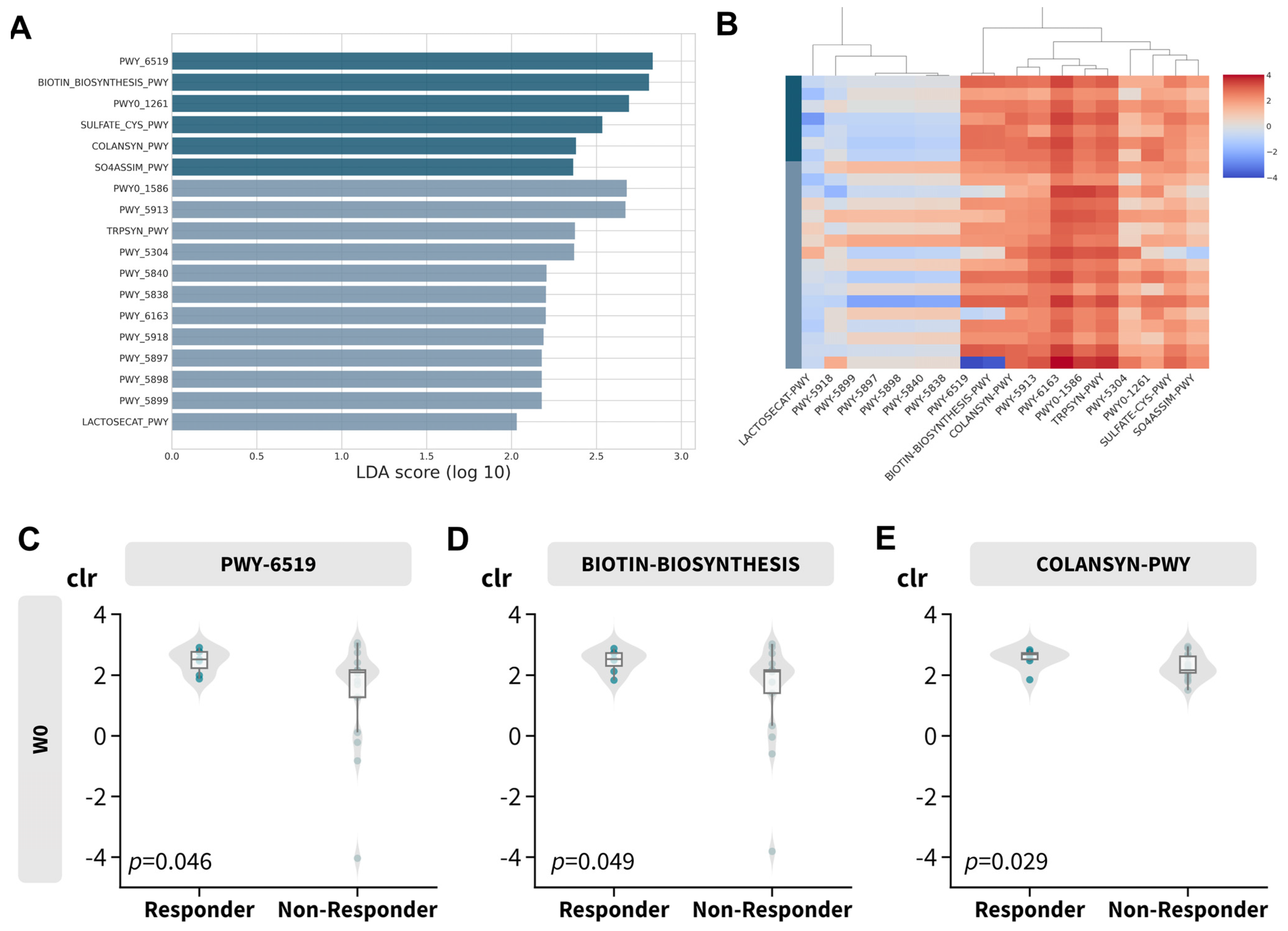
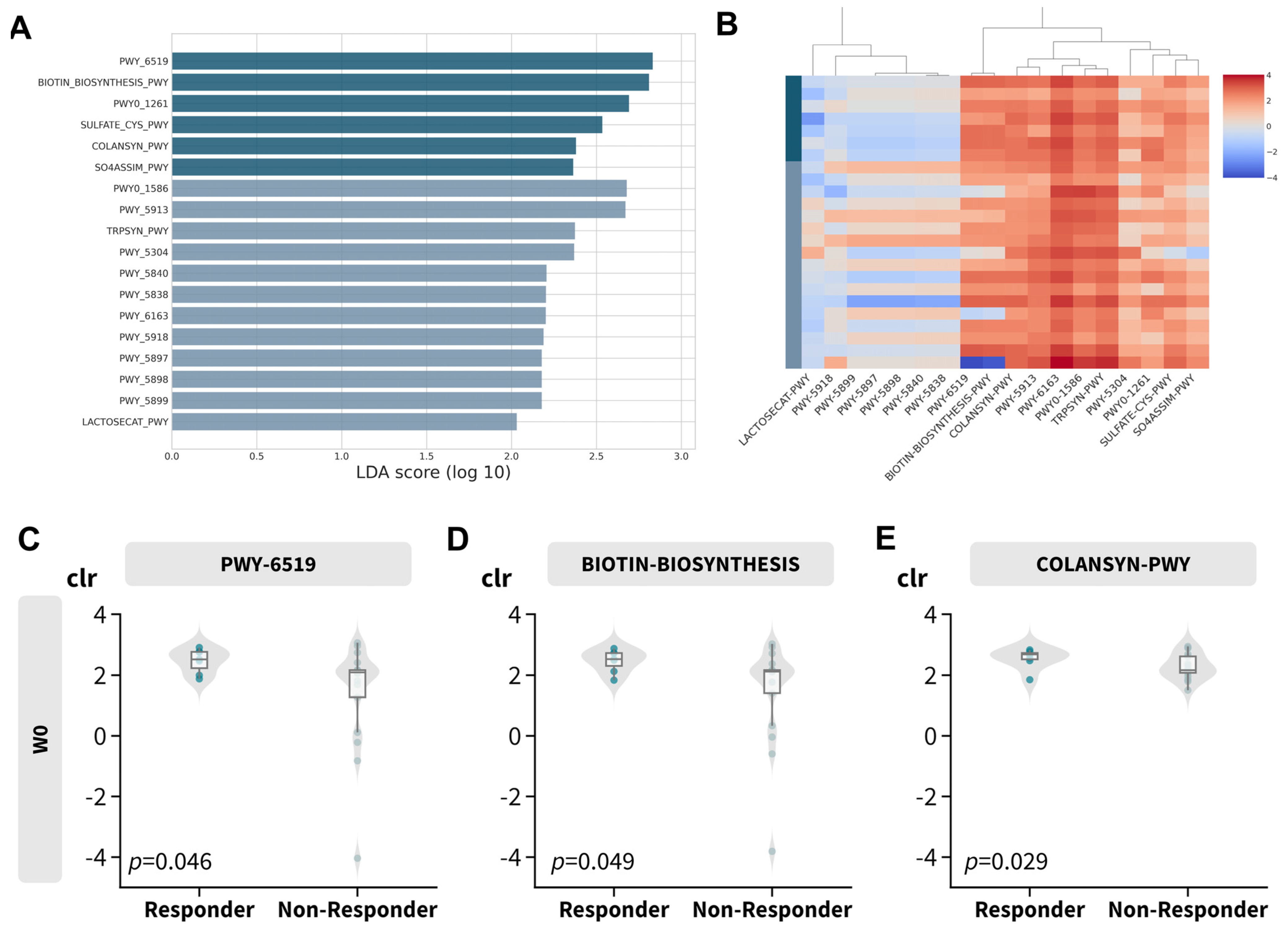
3.5. Distinctive Functional Abundance Profile among Responders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weidinger, S.; Beck, L.A.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic Dermatitis. Nat. Rev. Dis. Primers 2018, 4, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Sorrell, J.; Petukhova, L.; Reingold, R.; Christiano, A.; Garzon, M. Shedding Light on Alopecia Areata in Pediatrics: A Retrospective Analysis of Comorbidities in Children in the National Alopecia Areata Registry. Pediatr. Dermatol. 2017, 34, e271–e272. [Google Scholar] [CrossRef]
- Schmitt, J.; Schwarz, K.; Baurecht, H.; Hotze, M.; Fölster-Holst, R.; Rodríguez, E.; Lee, Y.A.E.; Franke, A.; Degenhardt, F.; Lieb, W.; et al. Atopic Dermatitis Is Associated with an Increased Risk for Rheumatoid Arthritis and Inflammatory Bowel Disease, and a Decreased Risk for Type 1 Diabetes. J. Allergy Clin. Immunol. 2016, 137, 130–136. [Google Scholar] [CrossRef]
- Thyssen, J.P.; Hamann, C.R.; Linneberg, A.; Dantoft, T.M.; Skov, L.; Gislason, G.H.; Wu, J.J.; Egeberg, A. Atopic Dermatitis Is Associated with Anxiety, Depression, and Suicidal Ideation, but Not with Psychiatric Hospitalization or Suicide. Allergy 2018, 73, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Yaghmaie, P.; Koudelka, C.W.; Simpson, E.L. Mental Health Comorbidity in Patients with Atopic Dermatitis. J. Allergy Clin. Immunol. 2013, 131, 428–433. [Google Scholar] [CrossRef]
- Pinart, M.; Benet, M.; Annesi-Maesano, I.; von Berg, A.; Berdel, D.; Carlsen, K.C.L.; Carlsen, K.H.; Bindslev-Jensen, C.; Eller, E.; Fantini, M.P.; et al. Comorbidity of Eczema, Rhinitis, and Asthma in IgE-Sensitised and Non-IgE-Sensitised Children in MeDALL: A Population-Based Cohort Study. Lancet Respir. Med. 2014, 2, 131–140. [Google Scholar] [CrossRef]
- Kapoor, R.; Menon, C.; Hoffstad, O.; Bilker, W.; Leclerc, P.; Margolis, D.J. The Prevalence of Atopic Triad in Children with Physician-Confirmed Atopic Dermatitis. J. Am. Acad. Dermatol. 2008, 58, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Van der Hulst, A.E.; Klip, H.; Brand, P.L.P. Risk of Developing Asthma in Young Children with Atopic Eczema: A Systematic Review. J. Allergy Clin. Immunol. 2007, 120, 565–569. [Google Scholar] [CrossRef]
- Werfel, T.; Heratizadeh, A.; Niebuhr, M.; Kapp, A.; Roesner, L.M.; Karch, A.; Erpenbeck, V.J.; Losche, C.; Jung, T.; Krug, N.; et al. Exacerbation of Atopic Dermatitis on Grass Pollen Exposure in an Environmental Challenge Chamber. J. Allergy Clin. Immunol. 2015, 136, 96–103.e9. [Google Scholar] [CrossRef]
- Longo, G.; Berti, I.; Burks, A.W.; Krauss, B.; Barbi, E. IgE-Mediated Food Allergy in Children. Lancet 2013, 382, 1656–1664. [Google Scholar] [CrossRef]
- Bergmann, M.M.; Caubet, J.C.; Boguniewicz, M.; Eigenmann, P.A. Evaluation of Food Allergy in Patients with Atopic Dermatitis. J. Allergy Clin. Immunol. Pract. 2013, 1, 22–28. [Google Scholar] [CrossRef]
- Manam, S.; Tsakok, T.; Till, S.; Flohr, C. The Association between Atopic Dermatitis and Food Allergy in Adults. Curr. Opin. Allergy Clin. Immunol. 2014, 14, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Flohr, C.; Johansson, S.G.O.; Wahlgren, C.F.; Williams, H. How Atopic Is Atopic Dermatitis? J. Allergy Clin. Immunol. 2004, 114, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.I.; Montefort, S.; Björkstén, B.; Lai, C.K.; Strachan, D.P.; Weiland, S.K.; Williams, H. Worldwide Time Trends in the Prevalence of Symptoms of Asthma, Allergic Rhinoconjunctivitis, and Eczema in Childhood: ISAAC Phases One and Three Repeat Multicountry Cross-Sectional Surveys. Lancet 2006, 368, 733–743. [Google Scholar] [CrossRef]
- Mallol, J.; Crane, J.; von Mutius, E.; Odhiambo, J.; Keil, U.; Stewart, A. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: A Global Synthesis. Allergol. Immunopathol. 2013, 41, 73–85. [Google Scholar] [CrossRef]
- Williams, H.; Stewart, A.; von Mutius, E.; Cookson, W.; Anderson, H.R. Is Eczema Really on the Increase Worldwide? J. Allergy Clin. Immunol. 2008, 121, 947–954.e15. [Google Scholar] [CrossRef]
- Liu, W.; Cai, J.; Sun, C.; Zou, Z.; Zhang, J.; Huang, C. Time-Trends for Eczema Prevalences among Children and Adults from 1985 to 2015 in China: A Systematic Review. BMC Public Health 2022, 22, 1294. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.L.; Wong, W.; Lau, Y.L. Increasing Prevalence of Allergic Rhinitis but Not Asthma among Children in Hong Kong from 1995 to 2001 (Phase 3 International Study of Asthma and Allergies in Childhood). Pediatr. Allergy Immunol. 2004, 15, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Survey Findings on Prevalence of Allergic Diseases among Hong Kong Primary and Secondary Schoolchildren—All News—Media—HKU. Available online: https://www.hku.hk/press/news_detail_23934.html (accessed on 10 May 2023).
- Leung, R.; Wong, G.; Lau, J.; Ho, A.; Chan, J.K.W.; Choy, D.; Douglass, C.; Lai, C.K.W. Prevalence of Asthma and Allergy in Hong Kong Schoolchildren: An ISAAC Study. Eur. Respir. J. 1997, 10, 354–360. [Google Scholar] [CrossRef]
- Hong Kong Journal of Paediatrics [HK J Paediatr (New Series) 2021, 26, 42–57]. Available online: https://www.hkjpaed.org/details.asp?id=1323&show=1234 (accessed on 10 May 2023).
- Lewis, M.C.; Inman, C.F.; Patel, D.; Schmidt, B.; Mulder, I.; Miller, B.; Gill, B.P.; Pluske, J.; Kelly, D.; Stokes, C.R.; et al. Direct Experimental Evidence That Early-Life Farm Environment Influences Regulation of Immune Responses. Pediatr. Allergy Immunol. 2012, 23, 265–269. [Google Scholar] [CrossRef]
- Okada, H.; Kuhn, C.; Feillet, H.; Bach, J.F. The “hygiene Hypothesis” for Autoimmune and Allergic Diseases: An Update. Clin. Exp. Immunol. 2010, 160, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Grobe, W.; Bieber, T.; Novak, N. Pathophysiology of Atopic Dermatitis. J. Dtsch. Dermatol. Ges. 2019, 17, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Reddel, S.; Del Chierico, F.; Quagliariello, A.; Giancristoforo, S.; Vernocchi, P.; Russo, A.; Fiocchi, A.; Rossi, P.; Putignani, L.; El Hachem, M. Gut Microbiota Profile in Children Affected by Atopic Dermatitis and Evaluation of Intestinal Persistence of a Probiotic Mixture. Sci. Rep. 2019, 9, 4996. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Du, X.; Zhai, S.; Tang, X.; Liu, C.; Li, W. Gut Microbiota and Atopic Dermatitis in Children: A Scoping Review. BMC Pediatr. 2022, 22, 323. [Google Scholar] [CrossRef]
- Petersen, E.B.M.; Skov, L.; Thyssen, J.P.; Jensen, P. Role of the Gut Microbiota in Atopic Dermatitis: A Systematic Review. Acta. Derm. Venereol. 2018, 99, 5–11. [Google Scholar] [CrossRef]
- Candela, M.; Rampelli, S.; Turroni, S.; Severgnini, M.; Consolandi, C.; De Bellis, G.; Masetti, R.; Ricci, G.; Pession, A.; Brigidi, P. Unbalance of Intestinal Microbiota in Atopic Children. BMC Microbiol. 2012, 12, 95. [Google Scholar] [CrossRef]
- Penders, J.; Stobberingh, E.E.; van den Brandt, P.A.; Thijs, C. The Role of the Intestinal Microbiota in the Development of Atopic Disorders. Allergy 2007, 62, 1223–1236. [Google Scholar] [CrossRef]
- Chan, C.W.H.; Chan, J.Y.W.; Leung, T.F.; Choi, K.C.; Tsui, S.K.W.; Wong, C.L.; Chow, K.M. Altered Gut Microbiome and Environmental Factors Associated with Development of Eczema in Hong Kong Infants: A 4-Month Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 7634. [Google Scholar] [CrossRef]
- Melli, L.C.F.L.; do Carmo-Rodrigues, M.S.; Araújo-Filho, H.B.; Mello, C.S.; Tahan, S.; Pignatari, A.C.C.; Solé, D.; de Morais, M.B. Gut Microbiota of Children with Atopic Dermatitis: Controlled Study in the Metropolitan Region of São Paulo, Brazil. Allergol. Immunopathol. 2020, 48, 107–115. [Google Scholar] [CrossRef]
- Zheng, H.; Liang, H.; Wang, Y.; Miao, M.; Shi, T.; Yang, F.; Liu, E.; Yuan, W.; Ji, Z.S.; Li, D.K. Altered Gut Microbiota Composition Associated with Eczema in Infants. PLoS ONE 2016, 11, e0166026. [Google Scholar] [CrossRef]
- Abrahamsson, T.R.; Jakobsson, H.E.; Andersson, A.F.; Björkstén, B.; Engstrand, L.; Jenmalm, M.C. Low Diversity of the Gut Microbiota in Infants with Atopic Eczema. J. Allergy Clin. Immunol. 2012, 129, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Yoo, Y.; Hwang, J.; Na, Y.C.; Kim, H.S. Faecalibacterium prausnitzii Subspecies-Level Dysbiosis in the Human Gut Microbiome Underlying Atopic Dermatitis. J. Allergy Clin. Immunol. 2016, 137, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Pike, M.G.; Heddle, R.J.; Boulton, P.; Turner, M.W.; Atherton, D.J. Increased Intestinal Permeability in Atopic Eczema. J. Invest. Dermatol. 1986, 86, 101–104. [Google Scholar] [CrossRef]
- De Filippis, F.; Paparo, L.; Nocerino, R.; Della Gatta, G.; Carucci, L.; Russo, R.; Pasolli, E.; Ercolini, D.; Berni Canani, R. Specific Gut Microbiome Signatures and the Associated Pro-Inflamatory Functions Are Linked to Pediatric Allergy and Acquisition of Immune Tolerance. Nat. Commun. 2021, 12, 5958. [Google Scholar] [CrossRef] [PubMed]
- Baker, B.S. The Role of Microorganisms in Atopic Dermatitis. Clin. Exp. Immunol. 2006, 144, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Qian, L.J.; Kang, S.M.; Xie, J.L.; Huang, L.; Wen, Q.; Fan, Y.Y.; Lu, L.J.; Jiang, L. Early-Life Gut Microbial Colonization Shapes Th1/Th2 Balance in Asthma Model in BALB/c Mice. BMC Microbiol. 2017, 17, 135. [Google Scholar] [CrossRef] [PubMed]
- Jakobsson, H.E.; Abrahamsson, T.R.; Jenmalm, M.C.; Harris, K.; Quince, C.; Jernberg, C.; Björkstén, B.; Engstrand, L.; Andersson, A.F. Decreased Gut Microbiota Diversity, Delayed Bacteroidetes Colonisation and Reduced Th1 Responses in Infants Delivered by Caesarean Section. Gut 2014, 63, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Gensollen, T.; Blumberg, R.S. Correlation between Early-Life Regulation of the Immune System by Microbiota and Allergy Development. J. Allergy Clin. Immunol. 2017, 139, 1084–1091. [Google Scholar] [CrossRef]
- Mashiah, J.; Karady, T.; Fliss-Isakov, N.; Sprecher, E.; Slodownik, D.; Artzi, O.; Samuelov, L.; Ellenbogen, E.; Godneva, A.; Segal, E.; et al. Clinical Efficacy of Fecal Microbial Transplantation Treatment in Adults with Moderate-to-Severe Atopic Dermatitis. Immun. Inflamm. Dis. 2022, 10, e570. [Google Scholar] [CrossRef]
- Bath-Hextall, F.; Delamere, F.M.; Williams, H.C. Dietary Exclusions for Improving Established Atopic Eczema in Adults and Children: Systematic Review. Allergy 2009, 64, 258–264. [Google Scholar] [CrossRef]
- Fiocchi, A.; Pawankar, R.; Cuello-Garcia, C.; Ahn, K.; Al-Hammadi, S.; Agarwal, A.; Beyer, K.; Burks, W.; Canonica, G.W.; Ebisawa, M.; et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Probiotics. World Allergy Organ. J. 2015, 8, 10. [Google Scholar] [CrossRef]
- Makrgeorgou, A.; Leonardi-Bee, J.; Bath-Hextall, F.J.; Murrell, D.F.; Tang, M.L.K.; Roberts, A.; Boyle, R.J. Probiotics for Treating Eczema. Cochrane Database Syst. Rev. 2018, 11, CD006135. [Google Scholar] [CrossRef] [PubMed]
- Osborn, D.A.; Sinn, J.K. Probiotics in Infants for Prevention of Allergic Disease and Food Hypersensitivity. Cochrane Database Syst. Rev. 2007, 11, CD006475. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Ni, B.; Liu, Z.; Liu, X.; Xie, W.; Wu, I.X.Y.; Li, X. The Role of Probiotics in the Prevention and Treatment of Atopic Dermatitis in Children: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Paediatr. Drugs 2020, 22, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Tan-Lim, C.S.C.; Esteban-Ipac, N.A.R.; Recto, M.S.T.; Castor, M.A.R.; Casis-Hao, R.J.; Nano, A.L.M. Comparative Effectiveness of Probiotic Strains on the Prevention of Pediatric Atopic Dermatitis: A Systematic Review and Network Meta-Analysis. Pediatr. Allergy Immunol. 2021, 32, 1255–1270. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Su, J. Association of Probiotics with Atopic Dermatitis among Infant: A Meta-Analysis of Randomized Controlled Trials. Oxid. Med. Cell. Longev. 2022, 1–7. [Google Scholar] [CrossRef]
- Chen, L.; Ni, Y.; Wu, X.; Chen, G. Probiotics for the Prevention of Atopic Dermatitis in Infants from Different Geographic Regions: A Systematic Review and Meta-Analysis. J. Dermatolog. Treat. 2022, 33, 2931–2939. [Google Scholar] [CrossRef]
- Zhao, M.; Shen, C.; Ma, L. Treatment Efficacy of Probiotics on Atopic Dermatitis, Zooming in on Infants: A Systematic Review and Meta-Analysis. Int. J. Dermatol. 2018, 57, 635–641. [Google Scholar] [CrossRef]
- Huang, R.; Ning, H.; Shen, M.; Li, J.; Zhang, J.; Chen, X. Probiotics for the Treatment of Atopic Dermatitis in Children: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Cell Infect. Microbiol. 2017, 7, 392. [Google Scholar] [CrossRef]
- Nermes, M.; Kantele, J.M.; Atosuo, T.J.; Salminen, S.; Isolauri, E. Interaction of Orally Administered Lactobacillus rhamnosus GG with Skin and Gut Microbiota and Humoral Immunity in Infants with Atopic Dermatitis. Clin. Exp. Allergy 2011, 41, 370–377. [Google Scholar] [CrossRef]
- Fölster-Holst, R.; Müller, F.; Schnopp, N.; Abeck, D.; Kreiselmaier, I.; Lenz, T.; Von Rüden, U.; Schrezenmeir, J.; Christophers, E.; Weichenthal, M. Prospective, Randomized Controlled Trial on Lactobacillus rhamnosus in Infants with Moderate to Severe Atopic Dermatitis. Br. J. Dermatol. 2006, 155, 1256–1261. [Google Scholar] [CrossRef] [PubMed]
- Pessi, T.; Sütas, Y.; Hurme, M.; Isolauri, E. Interleukin-10 Generation in Atopic Children Following Oral Lactobacillus rhamnosus GG. Clin. Exp. Allergy 2000, 30, 1804–1808. [Google Scholar] [CrossRef] [PubMed]
- Costea, P.I.; Hildebrand, F.; Manimozhiyan, A.; Bäckhed, F.; Blaser, M.J.; Bushman, F.D.; De Vos, W.M.; Ehrlich, S.D.; Fraser, C.M.; Hattori, M.; et al. Enterotypes in the Landscape of Gut Microbial Community Composition. Nat. Microbiol. 2018, 3, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Guo, R.; Zhong, H.; Feng, Q.; Lan, Z.; Qin, B.; Ward, K.J.; Jackson, M.A.; Xia, Y.; Chen, X.; et al. Shotgun Metagenomics of 250 Adult Twins Reveals Genetic and Environmental Impacts on the Gut Microbiome. Cell Syst. 2016, 3, 572–584.e3. [Google Scholar] [CrossRef] [PubMed]
- Climent, E.; Martinez-blanch, J.F.; Llobregat, L.; Ruzafa-costas, B.; Carrión-gutiérrez, M.Á.; Ramírez-boscá, A.; Prieto-merino, D.; Genovés, S.; Codoñer, F.M.; Ramón, D.; et al. Changes in Gut Microbiota Correlates with Response to Treatment with Probiotics in Patients with Atopic Dermatitis. A Post Hoc Analysis of a Clinical Trial. Microorganisms 2021, 9, 854. [Google Scholar] [CrossRef]
- Caporaso, J.G.; Lauber, C.L.; Walters, W.A.; Berg-Lyons, D.; Huntley, J.; Fierer, N.; Owens, S.M.; Betley, J.; Fraser, L.; Bauer, M.; et al. Ultra-High-Throughput Microbial Community Analysis on the Illumina HiSeq and MiSeq Platforms. ISME J. 2012, 6, 1621–1624. [Google Scholar] [CrossRef]
- Swanson, K.S.; Gibson, G.R.; Hutkins, R.; Reimer, R.A.; Reid, G.; Verbeke, K.; Scott, K.P.; Holscher, H.D.; Azad, M.B.; Delzenne, N.M.; et al. The International Scientific Association for Probiotics and Prebiotics (ISAPP) Consensus Statement on the Definition and Scope of Synbiotics. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 687–701. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, Interactive, Scalable and Extensible Microbiome Data Science Using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-Resolution Sample Inference from Illumina Amplicon Data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Holmes, S.P. Exact Sequence Variants Should Replace Operational Taxonomic Units in Marker-Gene Data Analysis. ISME J. 2017, 11, 2639–2643. [Google Scholar] [CrossRef]
- Katoh, K.; Misawa, K.; Kuma, K.; Miyata, T. MAFFT: A Novel Method for Rapid Multiple Sequence Alignment Based on Fast Fourier Transform. Nucleic Acids Res. 2002, 30, 3059–3066. [Google Scholar] [CrossRef]
- Price, M.N.; Dehal, P.S.; Arkin, A.P. FastTree 2—Approximately Maximum-Likelihood Trees for Large Alignments. PLoS ONE 2010, 5, e9490. [Google Scholar] [CrossRef] [PubMed]
- Bokulich, N.A.; Kaehler, B.D.; Rideout, J.R.; Dillon, M.; Bolyen, E.; Knight, R.; Huttley, G.A.; Gregory Caporaso, J. Optimizing Taxonomic Classification of Marker-Gene Amplicon Sequences with QIIME 2’s Q2-Feature-Classifier Plugin. Microbiome 2018, 6, 90. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, P.; Parfrey, L.W.; Yarza, P.; Gerken, J.; Pruesse, E.; Quast, C.; Schweer, T.; Peplies, J.; Ludwig, W.; Glöckner, F.O. The SILVA and “All-Species Living Tree Project (LTP)” Taxonomic Frameworks. Nucleic. Acids Res. 2013, 42, D643–D648. [Google Scholar] [CrossRef] [PubMed]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA Ribosomal RNA Gene Database Project: Improved Data Processing and Web-Based Tools. Nucleic. Acids Res. 2012, 41, D590–D596. [Google Scholar] [CrossRef]
- Anderson, M.J. Permutational Multivariate Analysis of Variance (PERMANOVA). Wiley StatsRef: Stat. Ref. Online 2017, 1–15. [Google Scholar] [CrossRef]
- Anderson, M.J. A New Method for Non-Parametric Multivariate Analysis of Variance. Austral. Ecol. 2001, 26, 32–46. [Google Scholar] [CrossRef]
- Lin, H.; Peddada, S. Das Analysis of Compositions of Microbiomes with Bias Correction. Nat. Commun. 2020, 11, 3514. [Google Scholar] [CrossRef]
- Kurtz, Z.D.; Müller, C.L.; Miraldi, E.R.; Littman, D.R.; Blaser, M.J.; Bonneau, R.A. Sparse and Compositionally Robust Inference of Microbial Ecological Networks. PLoS Comput. Biol. 2015, 11, e1004226. [Google Scholar] [CrossRef]
- Meinshausen, N.; Bühlmann, P. High-Dimensional Graphs and Variable Selection with the Lasso. Ann. Statist. 2006, 34, 1436–1462. [Google Scholar] [CrossRef]
- Stewart, C.J.; Ajami, N.J.; O’Brien, J.L.; Hutchinson, D.S.; Smith, D.P.; Wong, M.C.; Ross, M.C.; Lloyd, R.E.; Doddapaneni, H.V.; Metcalf, G.A.; et al. Temporal Development of the Gut Microbiome in Early Childhood from the TEDDY Study. Nature 2018, 562, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Laman, J.D.; ’t Hart, B.A.; Power, C.; Dziarski, R. Bacterial Peptidoglycan as a Driver of Chronic Brain Inflammation. Trends Mol. Med. 2020, 26, 670–682. [Google Scholar] [CrossRef] [PubMed]
- Wollenberg, A.; Barbarot, S.; Bieber, T.; Christen-Zaech, S.; Deleuran, M.; Fink-Wagner, A.; Gieler, U.; Girolomoni, G.; Lau, S.; Muraro, A.; et al. Consensus-Based European Guidelines for Treatment of Atopic Eczema (Atopic Dermatitis) in Adults and Children: Part I. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 657–682. [Google Scholar] [CrossRef]
- Wollenberg, A.; Barbarot, S.; Bieber, T.; Christen-Zaech, S.; Deleuran, M.; Fink-Wagner, A.; Gieler, U.; Girolomoni, G.; Lau, S.; Muraro, A.; et al. Consensus-Based European Guidelines for Treatment of Atopic Eczema (Atopic Dermatitis) in Adults and Children: Part II. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 850–878. [Google Scholar] [CrossRef] [PubMed]
- Blome, C.; Radtke, M.A.; Eissing, L.; Augustin, M. Quality of Life in Patients with Atopic Dermatitis: Disease Burden, Measurement, and Treatment Benefit. Am. J. Clin. Dermatol. 2016, 17, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Her, Y.; Kim, C.W.; Kim, S.S. Topical Corticosteroid Phobia among Parents of Children with Atopic Eczema in Korea. Ann. Dermatol. 2015, 27, 499. [Google Scholar] [CrossRef]
- Zheng, D.; Liwinski, T.; Elinav, E. Interaction between Microbiota and Immunity in Health and Disease. Cell Res. 2020, 30, 492–506. [Google Scholar] [CrossRef]
- Lozupone, C.A.; Stombaugh, J.I.; Gordon, J.I.; Jansson, J.K.; Knight, R. Diversity, Stability and Resilience of the Human Gut Microbiota. Nature 2012, 489, 220–230. [Google Scholar] [CrossRef]
- Faith, J.J.; Guruge, J.L.; Charbonneau, M.; Subramanian, S.; Seedorf, H.; Goodman, A.L.; Clemente, J.C.; Knight, R.; Heath, A.C.; Leibel, R.L.; et al. The Long-Term Stability of the Human Gut Microbiota. Science 2013, 341, 1237439. [Google Scholar] [CrossRef]
- Greenhalgh, K.; Meyer, K.M.; Aagaard, K.M.; Wilmes, P. The Human Gut Microbiome in Health: Establishment and Resilience of Microbiota over a Lifetime. Environ. Microbiol. 2016, 18, 2103–2116. [Google Scholar] [CrossRef]
- Sommer, F.; Anderson, J.M.; Bharti, R.; Raes, J.; Rosenstiel, P. The Resilience of the Intestinal Microbiota Influences Health and Disease. Nat. Rev. Microbiol. 2017, 15, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Meng, D.; Weng, M.; Zhu, W.; Wu, W.; Kasper, D.; Walker, W.A. The Symbiotic Bacterial Surface Factor Polysaccharide A on Bacteroides fragilis Inhibits IL-1β-Induced Inflammation in Human Fetal Enterocytes via Toll Receptors 2 and 4. PLoS ONE 2017, 12, e0172738. [Google Scholar] [CrossRef] [PubMed]
- Troy, E.B.; Kasper, D.L. Beneficial Effects of Bacteroides fragilis Polysaccharides on the Immune System. Front. Biosci. 2010, 15, 25. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, C.; Kujawski, M.; Chu, H.; Li, L.; Mazmanian, S.K.; Cantin, E.M. Bacteroides fragilis Polysaccharide A Induces IL-10 Secreting B and T Cells That Prevent Viral Encephalitis. Nat. Commun. 2019, 10, 2153. [Google Scholar] [CrossRef]
- Tang, C.; Tao, J.; Sun, J.; Lv, F.; Lu, Z.; Lu, Y. Regulatory Mechanisms of Energy Metabolism and Inflammation in Oleic Acid-Treated HepG2 Cells from Lactobacillus acidophilus NX2-6 Extract. J. Food Biochem. 2021, 45, e13925. [Google Scholar] [CrossRef]
- Chen, Y.H.; Tsai, W.H.; Wu, H.Y.; Chen, C.Y.; Yeh, W.L.; Chen, Y.H.; Hsu, H.Y.; Chen, W.W.; Chen, Y.W.; Chang, W.W.; et al. Probiotic Lactobacillus Spp. Act Against Helicobacter pylori-Induced Inflammation. J. Clin. Med. 2019, 8, 90. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, S.; Lee, J.H.; Kim, J.H.; Che, X.; Ma, H.W.; Seo, D.H.; Kim, T.I.I.; Kim, W.H.; Kim, S.W.; et al. Lactobacillus acidophilus Suppresses Intestinal Inflammation by Inhibiting Endoplasmic Reticulum Stress. J. Gastroenterol. Hepatol. 2019, 34, 178–185. [Google Scholar] [CrossRef]
- Kim, H.W.; Ju, D.B.; Kye, Y.C.; Ju, Y.J.; Kim, C.G.; Lee, I.K.; Park, S.M.; Choi, I.S.; Cho, K.K.; Lee, S.H.; et al. Galectin-9 Induced by Dietary Probiotic Mixture Regulates Immune Balance to Reduce Atopic Dermatitis Symptoms in Mice. Front. Immunol. 2020, 10, 3063. [Google Scholar] [CrossRef]
- Zmora, N.; Zilberman-Schapira, G.; Suez, J.; Mor, U.; Dori-Bachash, M.; Bashiardes, S.; Kotler, E.; Zur, M.; Regev-Lehavi, D.; Brik, R.B.Z.; et al. Personalized Gut Mucosal Colonization Resistance to Empiric Probiotics Is Associated with Unique Host and Microbiome Features. Cell 2018, 174, 1388–1405.e21. [Google Scholar] [CrossRef]
- Pedersen, H.K.; Gudmundsdottir, V.; Nielsen, H.B.; Hyotylainen, T.; Nielsen, T.; Jensen, B.A.H.; Forslund, K.; Hildebrand, F.; Prifti, E.; Falony, G.; et al. Human Gut Microbes Impact Host Serum Metabolome and Insulin Sensitivity. Nature 2016, 535, 376–381. [Google Scholar] [CrossRef]
- Dodd, D.; Spitzer, M.H.; Van Treuren, W.; Merrill, B.D.; Hryckowian, A.J.; Higginbottom, S.K.; Le, A.; Cowan, T.M.; Nolan, G.P.; Fischbach, M.A.; et al. A Gut Bacterial Pathway Metabolizes Aromatic Amino Acids into Nine Circulating Metabolites. Nature 2017, 551, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Zierer, J.; Jackson, M.A.; Kastenmüller, G.; Mangino, M.; Long, T.; Telenti, A.; Mohney, R.P.; Small, K.S.; Bell, J.T.; Steves, C.J.; et al. The Fecal Metabolome as a Functional Readout of the Gut Microbiome. Nat. Genet. 2018, 50, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Iikura, Y.; Odajima, Y.; Nagakura, T.; Iinuma, K.; Hayakawa, K.; Oizumi, J. Oral Biotin Treatment Is Effective for Atopic Dermatitis in Children with Low Biotinidase Activity. Acta Paediatr. Scand. 1988, 77, 762–763. [Google Scholar] [CrossRef]
- Kimura, M.; Fukui, T.; Tagami, Y.; Fujiwaki, T.; Yokoyama, M.; Ishioka, C.; Kumasaka, K.; Terada, N.; Yamaguchi, S. Normalization of Low Biotinidase Activity in a Child with Biotin Deficiency after Biotin Supplementation. J. Inherit. Metab. Dis. 2003, 26, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Stücker, M.; Pieck, C.; Stoerb, C.; Niedner, R.; Hartung, J.; Altmeyer, P. Topical Vitamin B12—A New Therapeutic Approach in Atopic Dermatitis-Evaluation of Efficacy and Tolerability in a Randomized Placebo-Controlled Multicentre Clinical Trial. Br. J. Dermatol. 2004, 150, 977–983. [Google Scholar] [CrossRef]
- Chesini, D.; Caminati, M. Vitamin B12 and Atopic Dermatitis: Any Therapeutic Relevance for Oral Supplementation? J. Diet. Suppl. 2022, 19, 238–242. [Google Scholar] [CrossRef]
- Galimberti, F.; Mesinkovska, N.A. Skin Findings Associated with Nutritional Deficiencies. Cleve Clin. J. Med. 2016, 83, 731–739. [Google Scholar] [CrossRef]
- Victoire, A.; Magin, P.; Coughlan, J.; Van Driel, M.L. Interventions for Infantile Seborrhoeic Dermatitis (Including Cradle Cap). Cochrane Database Syst. Rev. 2019, 4, CD011380. [Google Scholar] [CrossRef]
- Mardhiah, M.; Azize, N.A.A.; Yakob, Y.; Affandi, O.; Hock, N.L.; Rowani, M.R.; Habib, A. Clinical, Biochemical and Mutational Findings in Biotinidase Deficiency among Malaysian Population. Mol. Genet. Metab. Rep. 2019, 22, 100548. [Google Scholar] [CrossRef]
- Akgun, A.; Sen, A.; Onal, H. Clinical, Biochemical and Genotypical Characteristics in Biotinidase Deficiency. J. Pediatr. Endocrinol. Metab. 2021, 34, 1425–1433. [Google Scholar] [CrossRef]
- Sakurai-Yageta, M.; Mashimo, Y.; Kuroishi, T.; Ishihara, R.; Shimojo, N.; Kohno, Y.; Okamoto, Y.; Hata, A.; Suzuki, Y. Association between Serum Biotin Levels and Cedar Pollinosis in Japanese Schoolchildren. J. Nutr. Sci. Vitaminol. 2021, 67, 211–216. [Google Scholar] [CrossRef]
- Vieira, B.L.; Lim, N.R.; Lohman, M.E.; Lio, P.A. Complementary and Alternative Medicine for Atopic Dermatitis: An Evidence-Based Review. Am. J. Clin. Dermatol. 2016, 17, 557–581. [Google Scholar] [CrossRef] [PubMed]
- Januchowski, R. Evaluation of Topical Vitamin B12 for the Treatment of Childhood Eczema. J. Altern. Complement. Med. 2009, 15, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Nistico, S.P.; Del Duca, E.; Tamburi, F.; Pignataro, E.; De Carvalho, N.; Farnetani, F.; Pellacani, G. Superiority of a Vitamin B12-Barrier Cream Compared with Standard Glycerol-Petrolatum-Based Emollient Cream in the Treatment of Atopic Dermatitis: A Randomized, Left-to-Right Comparative Trial. Dermatol. Ther. 2017, 30, 12523. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Responder & (n =7) | Non-Responder (n = 17) | p-Value | |
|---|---|---|---|
| Sex, No. (%) | 0.3926 | ||
| Male | 3 (42.9) | 11 (64.7) | |
| Female | 4 (57.1) | 6 (35.3) | |
| Age, mean (SD) (range), y | 9 [3,4,5,6,7,8,9,10,11,12,13] | 4 [1,2,3,4,5,6,7,8,9,10] | 0.0524 |
| Mode of delivery, No. (%) | |||
| Vaginal | 6 (85.7) | 8 (47.1) | 0.1718 |
| Caesarean | 1 (14.3) | 9 (52.3) | |
| Other allergic comorbidities, No. (%) | 6 (85.7) | 14 (82.4) | >0.9999 |
| Gastrointestinal, No. (%) | |||
| Constipation | 0 (0) | 3 (17.6) | 0.5296 |
| Diarrhea | 1 (14.3) | 0 (0) | 0.2917 |
| EASI, mean (SD) ^ | 16.3 (5.2) | 12.5 (6.8) | 0.1707 |
| Feature ID | Taxon | LogFC | SE | W | p | q |
|---|---|---|---|---|---|---|
| 36932a39508d345bc380a8f33538a621 | g_Bacteroides; s_Bacteroides_fragilis | 5.297 | 0.530 | 9.986 | <0.0001 | <0.0001 |
| 3e75da00f0b8fefa3c1370c8b0600a95 | g_Lactobacillus; s_Lactobacillus_acidophilus | 2.444 | 0.603 | 4.056 | 0.0001 | 0.0145 |
| f73a95dd51110a0715147bef1d05c6fa | g_Bifidobacterium; s_metagenome | −2.944 | 0.730 | −4.035 | 0.0001 | 0.0158 |
| BioCyc ID | MetaCyc Pathway Name | Group | Log LDA | p-Value |
|---|---|---|---|---|
| PWY_6519 | 8-amino-7-oxononanoate biosynthesis I | Responder | 2.8318 | 0.0459 |
| BIOTIN_BIOSYNTHESIS_PWY | Biotin biosynthesis I | Responder | 2.8097 | 0.0485 |
| PWY0_1261 | Peptidoglycan recycling I | Responder | 2.6914 | 0.0057 |
| SULFATE_CYS_PWY | Superpathway of sulfate assimilation and cysteine biosynthesis | Responder | 2.5342 | 0.0207 |
| COLANSYN_PWY | Colanic acid building blocks biosynthesis | Responder | 2.3794 | 0.0294 |
| SO4ASSIM_PWY | Assimilatory sulfate reduction I | Responder | 2.3628 | 0.0111 |
| PWY0_1586 | Peptidoglycan maturation (meso-diaminopimelate containing) | Non-Responder | 2.6783 | 0.0435 |
| PWY_5913 | Partial TCA cycle (obligate autotrophs) | Non-Responder | 2.6711 | 0.0412 |
| TRPSYN_PWY | L-tryptophan biosynthesis | Non-Responder | 2.3738 | 0.0005 |
| PWY_5304 | Superpathway of sulfur oxidation (Acidianus ambivalens) | Non-Responder | 2.3687 | 0.0412 |
| PWY_5840 | Superpathway of menaquinol-7 biosynthesis | Non-Responder | 2.2056 | 0.0459 |
| PWY_5838 | Superpathway of menaquinol-8 biosynthesis I | Non-Responder | 2.2025 | 0.0435 |
| PWY_6163 | Chorismate biosynthesis from 3-dehydroquinate | Non-Responder | 2.2017 | 0.0435 |
| PWY_5918 | Superpathway of heme b biosynthesis from glutamate | Non-Responder | 2.1888 | 0.0195 |
| PWY_5897 | Superpathway of menaquinol-11 biosynthesis | Non-Responder | 2.1782 | 0.0485 |
| PWY_5898 | Superpathway of menaquinol-12 biosynthesis | Non-Responder | 2.1782 | 0.0485 |
| PWY_5899 | Superpathway of menaquinol-13 biosynthesis | Non-Responder | 2.1782 | 0.0485 |
| LACTOSECAT_PWY | Lactose degradation I | Non-Responder | 2.0306 | 0.0369 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choy, C.T.; Siu, P.L.K.; Zhou, J.; Wong, C.H.; Lee, Y.W.; Chan, H.W.; Tsui, J.C.C.; Lo, C.J.Y.; Loo, S.K.F.; Tsui, S.K.W. Improvements in Gut Microbiome Composition Predict the Clinical Efficacy of a Novel Synbiotics Formula in Children with Mild to Moderate Atopic Dermatitis. Microorganisms 2023, 11, 2175. https://doi.org/10.3390/microorganisms11092175
Choy CT, Siu PLK, Zhou J, Wong CH, Lee YW, Chan HW, Tsui JCC, Lo CJY, Loo SKF, Tsui SKW. Improvements in Gut Microbiome Composition Predict the Clinical Efficacy of a Novel Synbiotics Formula in Children with Mild to Moderate Atopic Dermatitis. Microorganisms. 2023; 11(9):2175. https://doi.org/10.3390/microorganisms11092175
Chicago/Turabian StyleChoy, Chi Tung, Pui Ling Kella Siu, Junwei Zhou, Chi Ho Wong, Yuk Wai Lee, Ho Wang Chan, Joseph Chi Ching Tsui, Claudia Jun Yi Lo, Steven King Fan Loo, and Stephen Kwok Wing Tsui. 2023. "Improvements in Gut Microbiome Composition Predict the Clinical Efficacy of a Novel Synbiotics Formula in Children with Mild to Moderate Atopic Dermatitis" Microorganisms 11, no. 9: 2175. https://doi.org/10.3390/microorganisms11092175
APA StyleChoy, C. T., Siu, P. L. K., Zhou, J., Wong, C. H., Lee, Y. W., Chan, H. W., Tsui, J. C. C., Lo, C. J. Y., Loo, S. K. F., & Tsui, S. K. W. (2023). Improvements in Gut Microbiome Composition Predict the Clinical Efficacy of a Novel Synbiotics Formula in Children with Mild to Moderate Atopic Dermatitis. Microorganisms, 11(9), 2175. https://doi.org/10.3390/microorganisms11092175