
Detection of Bhanja Bandavirus in Patients with Neuroinvasive Disease of Unknown Etiology in Croatia

 ,
,  ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Anaylsis
3. Results
3.1. Prevalence of BHAV Antibodies in Patients with Neuroinvasive Disease
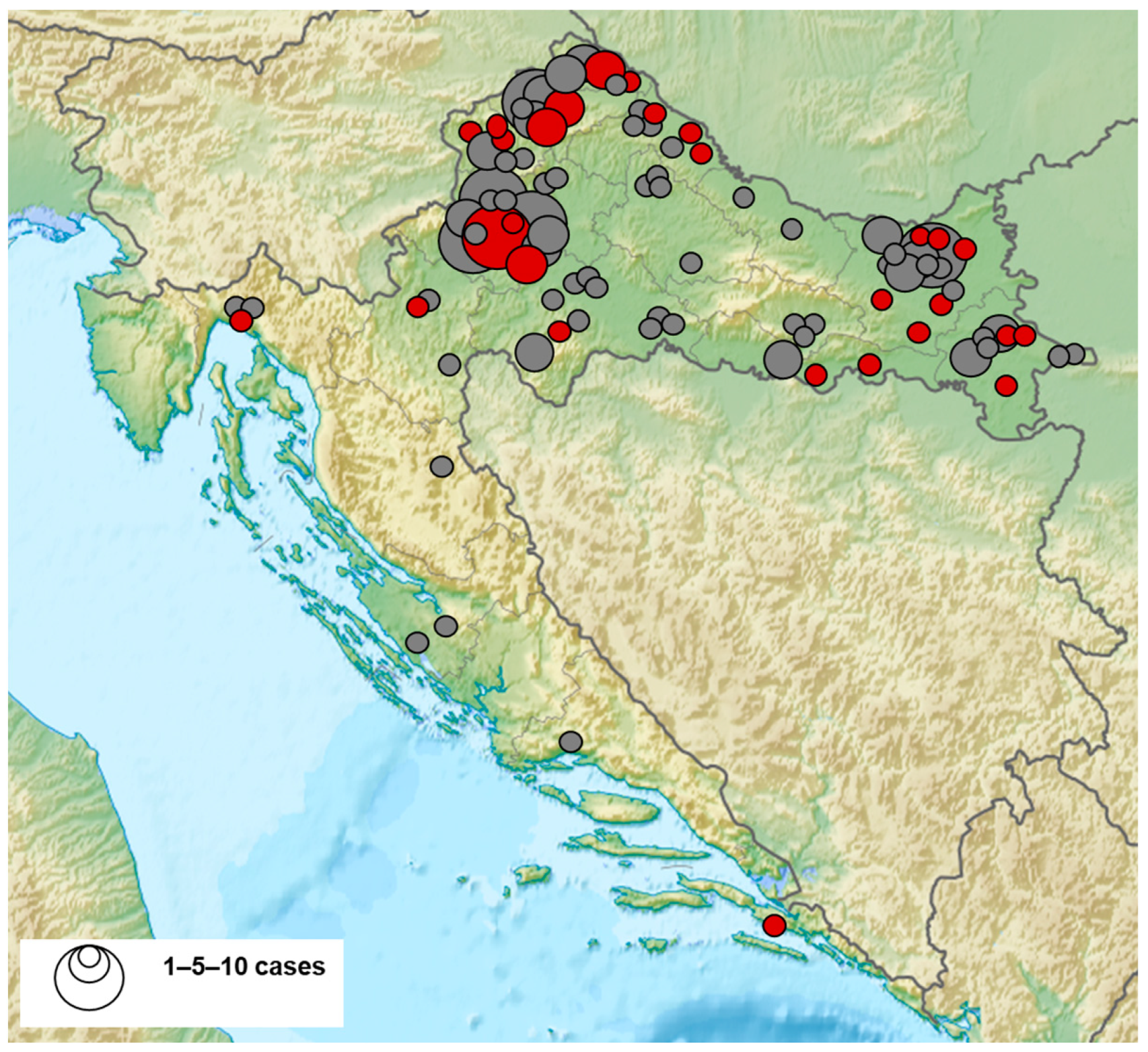
3.2. Geographic Distribution of BHAV-Seropositive Patients
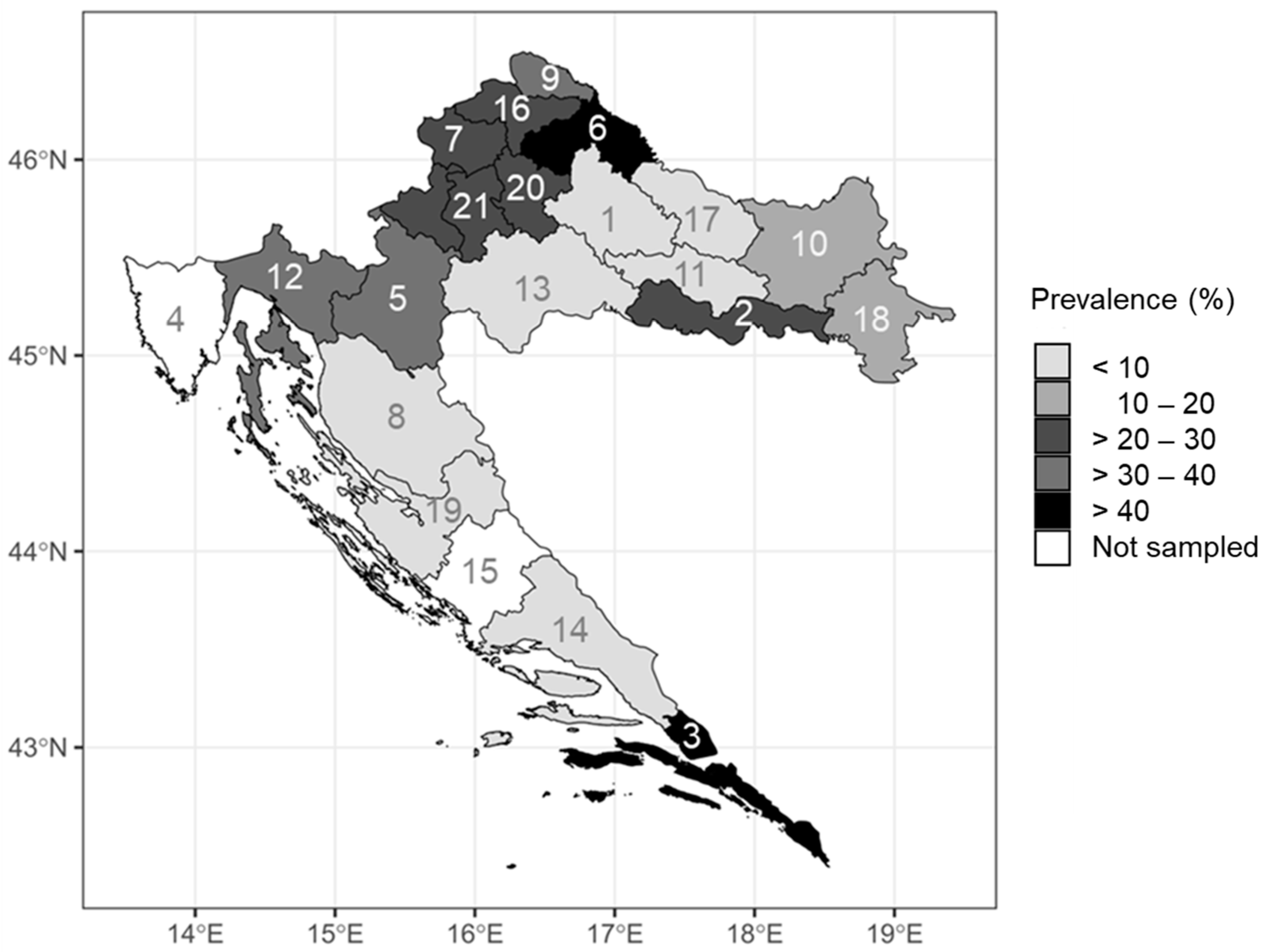
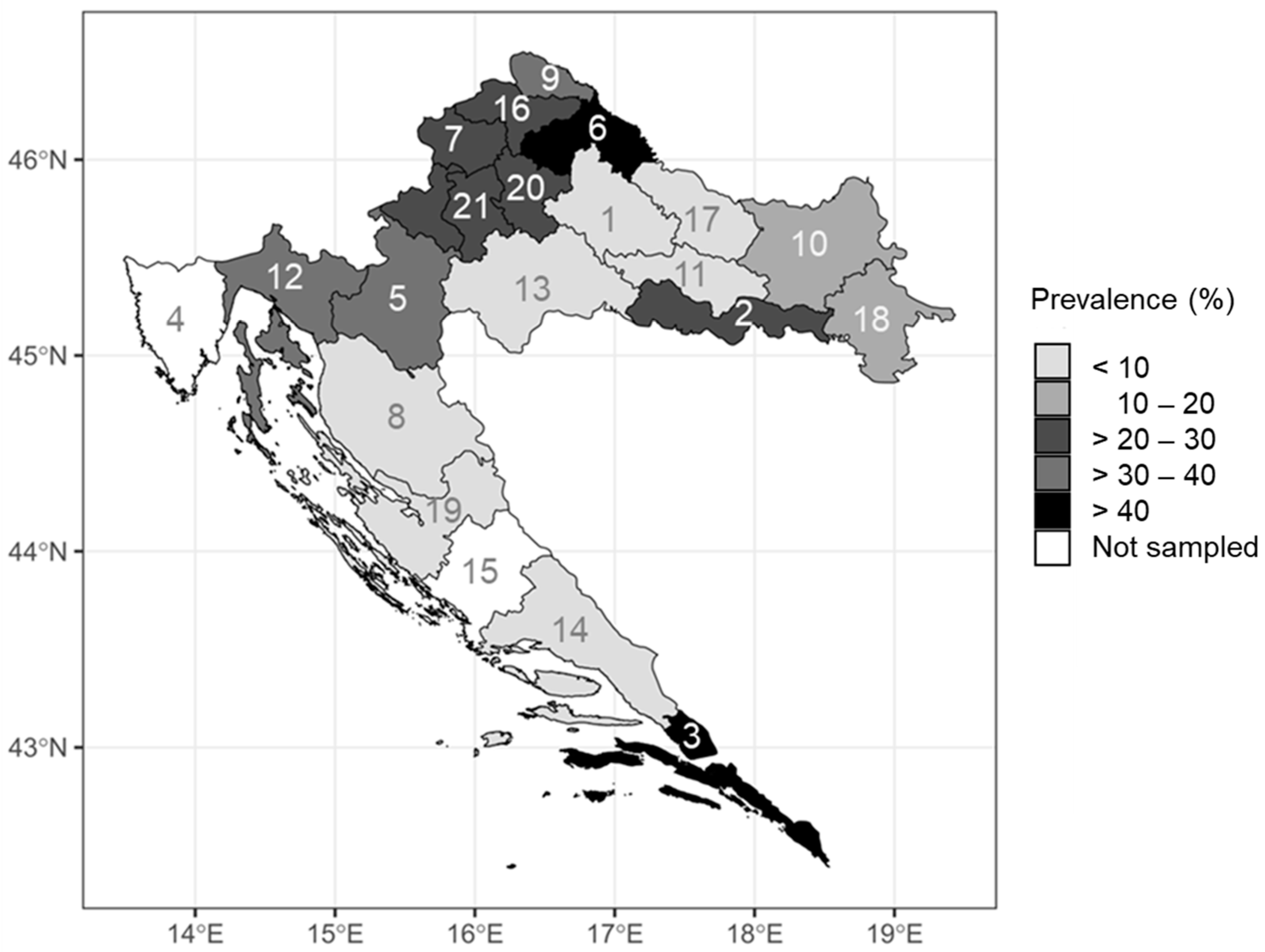
3.3. BHAV Prevalence Rates According to Region, Climate and Geographic Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Current International Committee on Taxonomy of Viruses (ICTV) Taxonomy Release. Available online: https://ictv.global/taxonomy/taxondetails?taxnode_id=202207635 (accessed on 6 August 2023).
- Shah, K.V.; Work, T.H. Bhanja virus: A new arbovirus from ticks Haemaphysalis intermedia Warburton and Nuttall, 1909, in Orissa, India. Indian J. Med. Res. 1969, 57, 793–798. [Google Scholar] [PubMed]
- Hubálek, Z. Biogeography of tick-borne Bhanja virus (bunyaviridae) in Europe. Interdiscip. Perspect. Infect. Dis. 2009, 2009, 372691. [Google Scholar] [CrossRef] [PubMed]
- Calisher, C.H.; Goodpasture, H.C. Human infection with Bhanja virus. Am. J. Trop. Med. Hyg. 1975, 24, 1040–1042. [Google Scholar] [CrossRef] [PubMed]
- Dilcher, M.; Alves, M.J.; Finkeisen, D.; Hufert, F.; Weidmann, M. Genetic characterization of Bhanja virus and Palma virus, two tick-borne phleboviruses. Virus Genes 2012, 45, 311–315. [Google Scholar] [CrossRef]
- Estrada-Peňa, A.; Pfäfle, M.P.; Petney, T.N. Genus Haemaphysalis Koch, 1844. In Ticks of Europe and North Africa—A Guide to Species Identification; Estrada-Peňa, A., Mihalca, A.D., Petney, T.N., Eds.; Springer: Cham, Switzerland, 2017; pp. 225–230. [Google Scholar]
- Krčmar, S. Hard ticks (Acari, Ixodidae) of Croatia. ZooKeys 2012, 234, 19–57. [Google Scholar] [CrossRef]
- Vesenjak-Hirjan, J.; Calisher, C.H.; Brudnjak, Z.; Tovornik, D.; Skrtic, N.; Lazuick, J.S. Isolation of Bhanja virus from ticks in Yugoslavia. Am. J. Trop. Med. Hyg. 1977, 26, 1003–1008. [Google Scholar] [CrossRef]
- Pfäffle, M.P.; Santos-Silva, M.; Jaenson, T.G.T.; Vatansever, Z.; Petney, T.N. Haemaphysalis punctata Canestrini and Fanzago, 1878 (Figs. 88–90). In Ticks of Europe and North Africa—A Guide to Species Identification; Estrada-Peňa, A., Mihalca, A.D., Petney, T.N., Eds.; Springer: Cham, Switzerland, 2017; pp. 237–242. [Google Scholar]
- Punda, V.; Beus, I.; Calisher, C.H.; Vesenjak-Hirjan, J. Laboratory infections with Bhanja virus. In Arboviruses in the Mediterranean Countries; Vesenjak-Hirjan, J., Ed.; Gustav Fischer Verlag: Stuttgart, Germany; New York, NY, USA, 1980; pp. 273–275. [Google Scholar]
- Vesenjak-Hirjan, J.; Calisher, C.H.; Beus, I.; Marton, E. First natural clinical human Bhanja virus infection. In Arboviruses in the Mediterranean Countries; Vesenjak-Hirjan, J., Ed.; Gustav Fischer Verlag: Stuttgart, Germany; New York, NY, USA, 1980; pp. 297–301. [Google Scholar]
- Vesenjak-Hirjan, J.; Galinović-Weisglass, M.; Brudnjak, Z.; Calisher, C.H.; Tovornik, D.; Lazuick, J.S.; Rendić, Z. Island of Brač—Focus of arbovirus infections. In Arboviruses in the Mediterranean Countries; Vesenjak-Hirjan, J., Ed.; Gustav Fischer Verlag: Stuttgart, Germany; New York, NY, USA, 1980; pp. 311–317. [Google Scholar]
- Vesenjak-Hirjan, J. Arboviruses in Yugoslavia. In Arboviruses in the Mediterranean Countries; Vesenjak-Hirjan, J., Ed.; Gustav Fischer Verlag: Stuttgart, Germany; New York, NY, USA, 1980; pp. 164–177. [Google Scholar]
- Vesenjak-Hirjan, J.; Galinović-Weisglass, M.; Urlić, V.; Bendiš, M.; Miović, P.; Vujošević, N.; Vuksanović, P. Occurrence of arboviruses in the Middle and the South Adriatic (Yugoslavia). In Arboviruses in the Mediterranean Countries; Vesenjak-Hirjan, J., Ed.; Gustav Fischer Verlag: Stuttgart, Germany; New York, NY, USA, 1980; pp. 303–310. [Google Scholar]
- Schwaiger, M.; Cassinotti, P. Development of a quantitative real-time RT-PCR assay with internal control for the laboratory detection of tick-borne encephalitis virus (TBEV) RNA. J. Clin. Virol. 2003, 27, 136–145. [Google Scholar] [CrossRef]
- Tang, Y.; Anne Hapip, C.; Liu, B.; Fang, C.T. Highly sensitive TaqMan RT-PCR assay for detection and quantification of both 456 lineages of West Nile virus RNA. J. Clin. Virol. 2006, 36, 177–182. [Google Scholar] [CrossRef]
- Nikolay, B.; Weidmann, M.; Dupressoir, A.; Faye, O.; Boye, C.S.; Diallo, M.; Sall, A.A. Development of a Usutu virus specific real-time reverse transcription PCR assay based on sequenced strains from Africa and Europe. J. Virol. Methods. 2014, 197, 51–54. [Google Scholar] [CrossRef]
- Weidmann, M.; Sanchez-Seco, M.P.; Sall, A.A.; Ly, P.O.; Thiongane, Y.; Lo, M.M.; Schley, H.; Hufert, F.T. Rapid detection of important human pathogenic Phleboviruses. J. Clin. Virol. 2008, 41, 138–142. [Google Scholar] [CrossRef]
- Li, H.; Cao, Y.X.; He, X.X.; Fu, S.H.; Lyu, Z.; He, Y.; Gao, X.Y.; Liang, G.D.; Wang, H.Y. Real-time RT-PCR Assay for the detection of Tahyna Virus. Biomed. Environ. Sci. 2015, 28, 374–377. [Google Scholar] [PubMed]
- Di Gennaro, A.; Lorusso, A.; Casaccia, C.; Conte, A.; Monaco, F.; Savini, G. Serum neutralization assay can efficiently replace plaque reduction neutralization test for detection and quantitation of West Nile virus antibodies in human and animal serum samples. Clin. Vaccine Immunol. 2014, 21, 1460–1462. [Google Scholar] [CrossRef]
- Reed, L.J.; Muench, H. A simple method of estimating fifty percent endpoints. Am. J. Hyg. 1938, 27, 493–497. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/imer/ (accessed on 2 August 2023).
- Croatian Meteorological and Hydrological Service. Available online: https://meteo.hr/index_en.php (accessed on 2 August 2023).
- Piantadosi, A.; Kanjilal, S. Diagnostic Approach for Arboviral Infections in the United States. J. Clin. Microbiol. 2020, 58, e01926-19. [Google Scholar] [CrossRef] [PubMed]
- Punda, V.; Ropac, D.; Vesenjak-Hirjan, J. Incidence of hemagglutination-inhibiting antibodies for Bhanja virus in humans along the north-west border of Yugoslavia. Zentralbl. Bakteriol. Mikrobiol. Hyg. A 1987, 265, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Verani, P.; Balducci, M.; Lopes, M.C. Isolation of Bhanja virus in Italy and serologic evidence of its distribution in man and animals of different Italian regions. Folia Parasitol. 1970, 17, 367–374. [Google Scholar]
- Hubálek, Z.; Juricová, Z. A serological survey for Bhanja virus in Czechoslovakia. Zentralbl. Bakteriol. Mikrobiol. Hyg. A 1984, 258, 540–543. [Google Scholar] [CrossRef]
- Hubálek, Z.; Bárdos, V.; Mittermayer, T.; Kuhn, J. Detection of human Bhanja virus-specific antibodies in Czechoslovakia. J. Hyg. Epidemiol. Microbiol. Immunol. 1982, 26, 181–186. [Google Scholar]
- Dahl, V.; Wisell, K.T.; Giske, C.G.; Tegnell, A.; Wallensten, A. Lyme neuroborreliosis epidemiology in Sweden 2010 to 2014: Clinical microbiology laboratories are a better data source than the hospital discharge diagnosis register. Euro Surveill. 2019, 24, 1800453. [Google Scholar] [CrossRef]
- Mikačić, D. Ixodidae of the Islands of Cres and Lošinj with a map of distribution of ticks species in Yugoslavia. Vet. Arh. 1949, 19, 14–32. [Google Scholar]
- Konjević, D.; Janicki, Z.; Severin, K.; Stanko, M.; Živičnjak, T.; Slavica, A.; Starešina, V. An outbreak of tick paralysis in free-ranging mouflon (Ovis ammon musimon). J. Zoo Wildl. Med. 2007, 38, 585–587. [Google Scholar] [CrossRef] [PubMed]
- Duh, D.; Punda-Polić, V.; Trilar, T.; Avšič-Županc, T. Molecular detection of Theileria sp. in ticks and naturally infected sheep. Vet. Parasitol. 2008, 151, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Dumić, T.; Jurković, D.; Florijanči, T.; Ozimec, S.; Pintur, K.; Fabijanić, N.; Filipeti, B.; Beck, R. Tick infestation of Balkan chamois (Rupicapra rupicapra balcanica) from the area of Biokovo mountain in the Republic of Croatia. In Proceedings of the III International Rupicapra Symposium, Makarska, Croatia, 16–18 June 2021. [Google Scholar]
- Mičetić, A. Fauna of Hard Ticks (Fam. Ixodidae) in Private Forests at Vicinity of Ponikve (Municipality Bakar). Master’s Thesis, Faculty of Forestry and Wood Technology, University of Zagreb, Zagreb, Croatia, 2021. [Google Scholar]
- Krčmar, S.; Klobučar, A.; Vucelja, M.; Boljfetić, M.; Kučinić, M.; Madić, J.; Cvek, M.; Bruvo Mađarić, B. DNA barcoding of hard ticks (Ixodidae), notes on distribution of vector species and new faunal record for Croatia. Ticks Tick-Borne Dis. 2022, 13, 101920. [Google Scholar] [CrossRef] [PubMed]
- Calisher, C.H. From Adamovec to Dubrovnik: An extended adventure, 1971–1992. Croat. Med. J. 2009, 50, 600–603. [Google Scholar] [CrossRef]
- Jemeršić, L.; Dežđek, D.; Brnić, D.; Prpić, J.; Janicki, Z.; Keros, T.; Roić, B.; Slavica, A.; Terzić, S.; Konjević, D.; et al. Detection and genetic characterization of tick-borne encephalitis virus (TBEV) derived from ticks removed from red foxes (Vulpes vulpes) and isolated from spleen samples of red deer (Cervus elaphus) in Croatia. Ticks Tick-Borne Dis. 2014, 5, 7–13. [Google Scholar] [CrossRef]
- Perez, K. Hard Tick Prevalence in Karlovac County. Master’s Thesis, Faculty of Veterinary Medicine, University of Zagreb, Zagreb, Croatia, 2021. [Google Scholar]
- Caminade, C.; McIntyre, K.M.; Jones, A.E. Impact of recent and future climate change on vector-borne diseases. Ann. N. Y. Acad. Sci. 2019, 1436, 157–173. [Google Scholar] [CrossRef]
- Ogden, N.H.; Lindsay, L.R. Effects of Climate and Climate Change on Vectors and Vector-Borne Diseases: Ticks Are Different. Trends Parasitol. 2016, 32, 646–656. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Patient 1 | Patient 2 | |
|---|---|---|---|
| Demographic characteristics | Gender Age | Male 72 years | Male 60 years |
| Geographic characteristics | Area of residence Geographic coordinates | Rural, near the river N 46°17′10″; E 16°18′10″ | Rural, near the river N 46°24′43″; E 16°37′30″ |
| UTM | 33 T | 33 T | |
| Altitude | 177 m | 146 m | |
| Epidemiological characteristics | Risk factors | No data | Tick bite on the head during fishing two weeks before disease onset |
| Date of disease onset | November 2018 | June 2019 | |
| Vaccination (tick-borne encephalitis, yellow fever) | No data | No | |
| Clinical characteristics | Clinical presentation | Meningoencephalitis | Febrile headache |
| Clinical symptoms | Fever, seizures, disorientation | Fever, headache, malaise | |
| Underlying diseases | Alcoholism | No | |
| Outcome | Improvement | Full recovery |
| Parameter | Patient 1 | Patient 2 | Reference Range |
|---|---|---|---|
| Laboratory results (blood/CSF) | |||
| L (Blood) | 12.3 | 11.1 | ×109/L |
| CRP (Blood) | 22.8 | 22.6 | <5 mg/L |
| Cells (CSF) | 144 | 5 | <5/mm3 |
| Mononuclear cells (CSF) | 85 | – | 100% |
| Proteins (CSF) | 0.400 | 0.520 | 0.17–0.37 g/L |
| Glucose (CSF) | 3.4 | 3.0 | 2.5–3.3 mmol/L |
| Virology results (serum/CSF/urine) | |||
| RT-qPCR (CSF) | Negative | Negative | |
| RT-qPCR (Urine) | Negative | Negative | |
| VNT titer (Serum) | 20 | Negative | ≥10 Positive |
| VNT titer (CSF) | 20 | 20 | ≥5 Positive |
| Characteristic | Tested | BHAV NT Antibodies N (%) | 95% CI | p | |
|---|---|---|---|---|---|
| N (%) | |||||
| Gender | Male | 165 (64.9) | 34 (20.6) | 14.7–27.5 | 0.728 |
| Female | 89 (35.1) | 20 (22.4) | 14.3–32.5 | ||
| Age group | <20 years | 24 (9.4) | 7 (29.1) | 12.6–51.1 | 0.907 |
| 20–29 years | 31 (12.2) | 8 (25.8) | 11.8–44.6 | ||
| 30–39 years | 43 (16.9) | 9 (20.9) | 10.0–36.0 | ||
| 40–49 years | 23 (9.1) | 5 (21.7) | 7.4–43.7 | ||
| 50–59 years | 33 (13.0) | 5 (15.2) | 3.4–28.2 | ||
| 60–69 years | 49 (19.3) | 10 (20.4) | 10.2–34.3 | ||
| ≥70 years | 51 (20.1) | 10 (19.6) | 9.8–33.1 | ||
| Area of residence | Urban | 181 (71.2) | 35 (19.3) | 13.8–25.8 | 0.238 |
| Suburban/rural | 73 (28.8) | 19 (26.0) | 16.4–37.6 | ||
| Clinical presentation | Febrile headache | 18 (7.1) | 4 (22.2) | 6.4–47.6 | <0.001 |
| Meningitis | 76 (29.9) | 34 (44.7) | 33.3–56.5 | ||
| Meningoencephalitis | 150 (59.1) | 15 (10.0) | 5.7–15.9 | ||
| Myelitis | 10 (3.9) | 1 (10.0) | 2.5–44.5 |
| Characteristic | OR | 95% CI OR | p |
|---|---|---|---|
| Male (Ref.) vs. female gender | 1.116 | 0.598–2.085 | 0.728 |
| Age | |||
| <20 years | Ref. | ||
| 20–29 years | 0.844 | 0.256–2.783 | 0.781 |
| 30–39 years | 0.642 | 0.204–2.023 | 0.450 |
| 40–49 years | 0.674 | 0.179–2.538 | 0.560 |
| 50–59 years | 0.433 | 0.118–1.585 | 0.206 |
| 60–69 years | 0.622 | 0.193–1.814 | 0.407 |
| ≥70 years | 0.592 | 0.774–1.814 | 0.359 |
| Suburban/rural (Ref.) vs. urban area of residence | 1.467 | 0.774–2.783 | 0.239 |
| Clinical presentation | |||
| Febrile headache | Ref. | ||
| Meningitis | 2.833 | 0.853–9.404 | 0.088 |
| Meningoencephalitis | 0.388 | 0.113–1.334 | 0.133 |
| Myelitis | 0.388 | 0.037–4.061 | 0.430 |
| County (Label) | Population Density (/km2) | Altitude (m) | Mean Temperature (°C) | N Cold Days (≤0 °C) | N Warm Days (≥25 °C) | N Hot Days (≥30 °C) | Insolation (h) | Total Precipitation (mm) | N Cases | Prevalence Rate |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 38.6 | 135 | 10.9 | 90 | 84 | 24 | 1948.9 | 809.3 | 0 | 0 |
| 2 | 64.0 | 92 | 12.2 | 93 | 93 | 31 | 1899.3 | 768.2 | 2 | 1.5 |
| 3 | 64.9 | 3 | 16.7 | 2 | 104 | 28 | 2636.5 | 1156.1 | 1 | 0.9 |
| 5 | 31.1 | 112 | 11.1 | 84 | 87 | 26 | 1908.8 | 1107.1 | 1 | 0.9 |
| 6 | 58.2 | 149 | 10.4 | 91 | 72 | 16 | 1974.1 | 795.6 | 3 | 2.9 |
| 7 | 98.8 | 203 | 10.4 | 92 | 70 | 16 | 2038.4 | 873 | 3 | 2.5 |
| 8 | 8.0 | 656 | 8.8 | 114 | 57 | 13 | 2018.2 | 1496.4 | 0 | 0 |
| 9 | 145.0 | 164 | 10.4 | 92 | 70 | 16 | 2038.4 | 873 | 6 | 5.7 |
| 10 | 62.5 | 94 | 11.1 | 82 | 93 | 32 | 1963.4 | 692.5 | 6 | 2.3 |
| 11 | 34.9 | 311 | 12.2 | 93 | 93 | 31 | 1899.3 | 768.2 | 0 | 0 |
| 12 | 74.4 | 13 | 14.2 | 18 | 87 | 27 | 2209.9 | 1554.2 | 1 | 0.4 |
| 13 | 31.4 | 98 | 11.2 | 82 | 84 | 24 | 1923.3 | 908.6 | 1 | 0.7 |
| 14 | 93.8 | 0 | 16.4 | 6 | 108 | 44 | 2637.3 | 785 | 0 | 0 |
| 16 | 127.1 | 173 | 10.4 | 92 | 70 | 16 | 2038.4 | 873 | 10 | 6.2 |
| 17 | 34.2 | 122 | 10.9 | 90 | 84 | 24 | 1948.9 | 809.3 | 0 | 0 |
| 18 | 59.0 | 108 | 11.1 | 82 | 93 | 32 | 1963.4 | 692.5 | 3 | 2.1 |
| 19 | 44.0 | 0 | 15.2 | 9 | 93 | 22 | 2578.4 | 911.8 | 0 | 0 |
| 20 | 97.9 | 158 | 11.6 | 59 | 73 | 17 | 1940 | 886 | 5 | 1.7 |
| 21 | 1200.6 | 158 | 11.6 | 59 | 73 | 17 | 1940 | 886 | 11 | 1.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilibic-Cavlek, T.; Stevanovic, V.; Krcmar, S.; Savic, V.; Kovac, S.; Bogdanic, M.; Mauric Maljkovic, M.; Sabadi, D.; Santini, M.; Potocnik-Hunjadi, T.; et al. Detection of Bhanja Bandavirus in Patients with Neuroinvasive Disease of Unknown Etiology in Croatia. Microorganisms 2023, 11, 2155. https://doi.org/10.3390/microorganisms11092155
Vilibic-Cavlek T, Stevanovic V, Krcmar S, Savic V, Kovac S, Bogdanic M, Mauric Maljkovic M, Sabadi D, Santini M, Potocnik-Hunjadi T, et al. Detection of Bhanja Bandavirus in Patients with Neuroinvasive Disease of Unknown Etiology in Croatia. Microorganisms. 2023; 11(9):2155. https://doi.org/10.3390/microorganisms11092155
Chicago/Turabian StyleVilibic-Cavlek, Tatjana, Vladimir Stevanovic, Stjepan Krcmar, Vladimir Savic, Snjezana Kovac, Maja Bogdanic, Maja Mauric Maljkovic, Dario Sabadi, Marija Santini, Tanja Potocnik-Hunjadi, and et al. 2023. "Detection of Bhanja Bandavirus in Patients with Neuroinvasive Disease of Unknown Etiology in Croatia" Microorganisms 11, no. 9: 2155. https://doi.org/10.3390/microorganisms11092155
APA StyleVilibic-Cavlek, T., Stevanovic, V., Krcmar, S., Savic, V., Kovac, S., Bogdanic, M., Mauric Maljkovic, M., Sabadi, D., Santini, M., Potocnik-Hunjadi, T., Al-Mufleh, M., & Barbic, L. (2023). Detection of Bhanja Bandavirus in Patients with Neuroinvasive Disease of Unknown Etiology in Croatia. Microorganisms, 11(9), 2155. https://doi.org/10.3390/microorganisms11092155