
Water Safety Plan, Monochloramine Disinfection and Extensive Environmental Sampling Effectively Control Legionella and Other Waterborne Pathogens in Nosocomial Settings: The Ten-Year Experience of an Italian Hospital

 ,
,
Abstract
1. Introduction
2. Materials and Methods
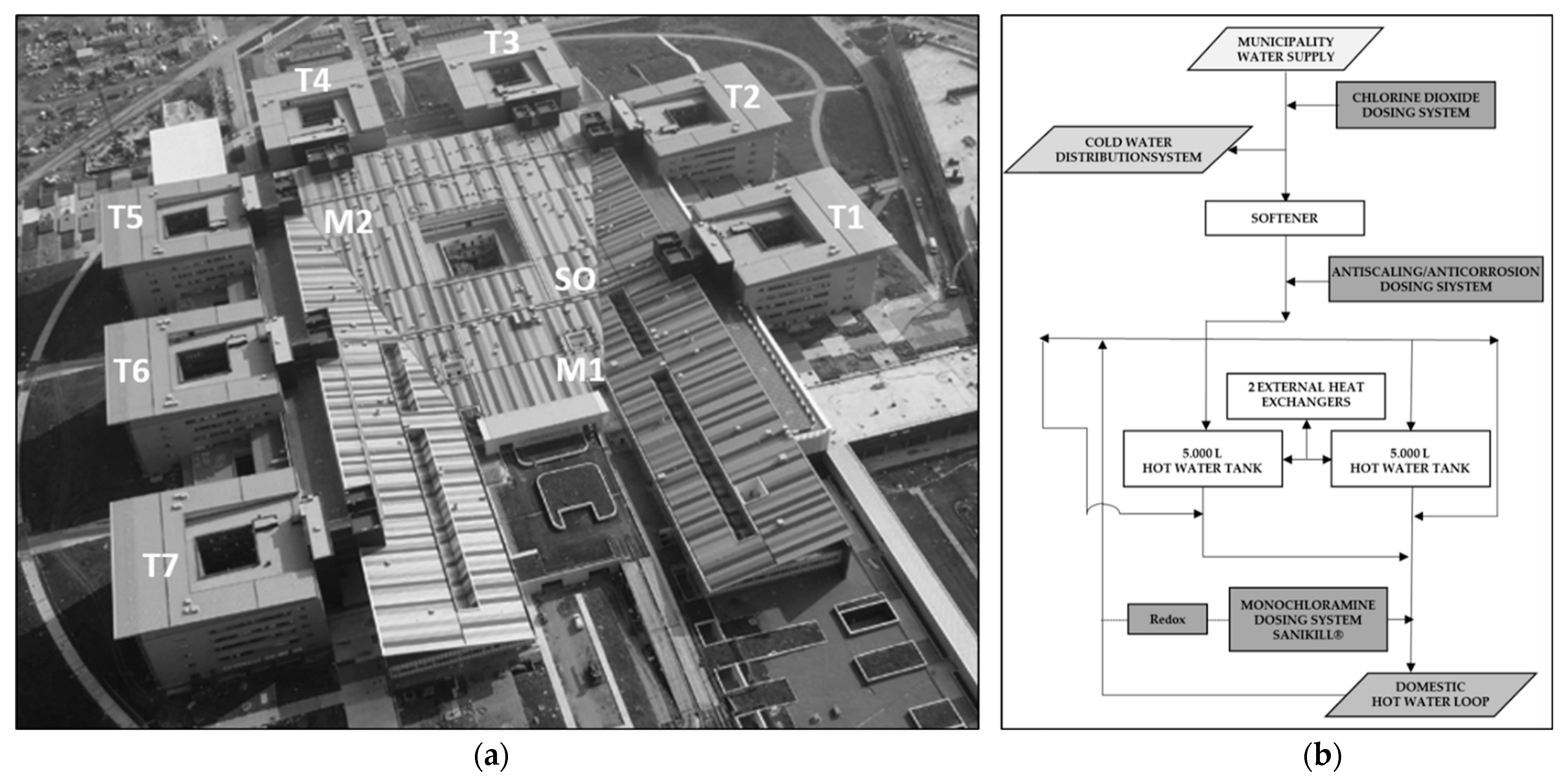
2.1. Setting
2.2. Piping and Water Treatment
2.3. Water Safety Group and Water Safety Plan
2.4. Sampling and Microbiological Analysis
3. Results
3.1. Water Safety Group, Water Safety Plan and Disinfection Strategy
3.2. Legionella Control
3.3. Additional Microbiological Monitoring
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- McDade, J.E.; Shepard, C.C.; Fraser, D.W.; Tsai, T.R.; Redus, M.A.; Dowdle, W.R. Legionnaires’ disease: Isolation of a bacterium and demonstration of its role in other respiratory disease. N. Engl. J. Med. 1977, 297, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Steigerwalt, A.G.; McDade, J.E. Classification of the Legionnaires’ disease bacterium: Legionella pneumophila, genus novum, species nova, of the family Legionellaceae, familia nova. Ann. Intern. Med. 1979, 90, 656–658. [Google Scholar] [CrossRef] [PubMed]
- Mondino, S.; Schmidt, S.; Rolando, M.; Escoll, P.; Gomez-Valero, L.; Buchrieser, C. Legionnaires’ disease: State of the art knowledge of pathogenesis mechanisms of Legionella. Annu. Rev. Pathol. Mech. Dis. 2020, 15, 439–466. [Google Scholar] [CrossRef] [PubMed]
- Bartram, J.; Chartier, Y.; Lee, J.V.; Pond, K.; Surman-Lee, S. Legionella and the Prevention of Legionellosis; World Health Organization: Genava, Switzerland, 2007. [Google Scholar]
- Parte, A.C.; Sardà Carbasse, J.; Meier-Kolthoff, J.P.; Reimer, L.C.; Göker, M. List of Prokaryotic names with Standing in Nomenclature (LPSN) moves to the DSMZ. Int. J. Syst. Evol. Microbiol. 2020, 70, 5607–5612. [Google Scholar] [CrossRef]
- Honigsbaum, M. Legionnaires’ disease: Revisiting the puzzle of the century. Lancet 2016, 388, 456–457. [Google Scholar] [CrossRef] [PubMed]
- Fields, B.S.; Benson, R.F.; Besser, R.E. Legionella and Legionnaires’ disease: 25 years of investigation. Clin. Microbiol. Rev. 2002, 15, 506–526. [Google Scholar] [CrossRef]
- Dideren, B.M.W. Legionella spp. and Legionnaires’ disease. J. Infect. 2008, 56, 1–12. [Google Scholar] [CrossRef]
- Cunha, B.A.; Burillo, A.; Bouza, E. Legionnaires’ disease. Lancet 2016, 387, 376–385. [Google Scholar] [CrossRef]
- Phin, N.; Parry-Ford, F.; Harrison, T.; Stagg, H.R.; Zhang, N.; Kumar, K.; Lortholary, O.; Zumla, A.; Abubakar, I. Epidemiology and clinical management of Legionnaires’ disease. Lancet Infect. Dis. 2014, 14, 1011–1121. [Google Scholar] [CrossRef]
- Stout, J.E.; Yu, V.L. Hospital-acquired Legionnaires’ disease: New developments. Curr. Opin. Infect. Dis. 2003, 16, 337–341. [Google Scholar] [CrossRef]
- Garcia-Nuñez, M.; Sopena, N.; Ragull, S.; Pedro-Botet, M.L.; Morera, J.; Sabria, M. Persistence of Legionella in hospital water supplies and nosocomial Legionnaires’ disease. FEMS Immunol. Med. Microbiol. 2008, 52, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Abell, V.; File, T.M., Jr. Nosocomial (Health Care-Associated) Legionnaire’s Disease. Infect. Dis. Clin. N. Am. 2017, 31, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Burillo, A.; Pedro-Botet, M.L.; Bouza, E. Microbiology and Epidemiology of Legionnaire’s Disease. Infec. Dis. Clin. N. Am. 2017, 31, 7–27. [Google Scholar] [CrossRef] [PubMed]
- Borella, P.; Bargellini, A.; Marchegiano, P.; Vecchi, E.; Marchesi, I. Hospital-acquired Legionella infections: An update on the procedures for controlling environmental contamination. Ann. Ig. 2016, 28, 98–108. [Google Scholar] [PubMed]
- Beauté, J.; The European Legionnaires’ Disease Surveillance Network. Legionnaires’ disease in Europe, 2011 to 2015. Eurosurveillance 2017, 22, 30566. [Google Scholar] [CrossRef]
- Rota, M.C.; Caporali, M.G.; Bella, A.; Scaturro, M.; Giannitelli, S.; Ricci, M.L. The National Surveillance System for legionellosis: Results for the year 2021. Boll. Epidemiol. Naz. 2022, 3, 30–37. [Google Scholar]
- Falkinham, J.O.; Pruden, A.; Edwards, M. Opportunistic Premise Plumbing Pathogens: Increasingly Important Pathogens in Drinking Water. Pathogens 2015, 4, 373–386. [Google Scholar] [CrossRef]
- Falkinham, J.O.; Hilborn, E.D.; Arduino, M.J.; Pruden, A.; Edwards, M.A. Epidemiology and Ecology of Opportunistic Premise Plumbing Pathogens: Legionella pneumophila, Mycobacterium avium, and Pseudomonas aeruginosa. Environ. Health Perspect. 2015, 123, 749–758. [Google Scholar] [CrossRef]
- Ashbolt, N.J. Environmental (Saprozoic) Pathogens of Engineered Water Systems: Understanding Their Ecology for Risk Assessment and Management. Pathogens 2015, 4, 390–405. [Google Scholar] [CrossRef]
- Squier, C.; Yu, V.L.; Stout, J.E. Waterborne Nosocomial Infections. Curr. Infect. Dis. Rep. 2000, 2, 490–496. [Google Scholar] [CrossRef]
- Decker, B.K.; Palmore, T.N. The role of water in healthcare-associated infections. Curr. Opin. Infect. Dis. 2013, 26, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Mermel, L.A.; Josephson, S.L.; Giorgio, C.H.; Dempsey, J.; Parenteau, S. Association of Legionnaires’ disease with construction: Contamination of potable water? Infect. Control Hosp. Epidemiol. 1995, 16, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.D.; Barr, B.A. Infection control issues in construction and renovation. Infect. Control Hosp. Epidemiol. 1997, 18, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Stout, J.E.; Brennen, C.; Muder, R.R. Legionnaires’ disease in a newly constructed long-term care facility. J. Am. Geriatr. Soc. 2000, 48, 1589–1592. [Google Scholar] [CrossRef]
- Sabria, M.; Yu, V.L. Hospital-acquired legionellosis: Solutions for a preventable infection. Lancet Infect. Dis. 2002, 2, 368–373. [Google Scholar] [CrossRef]
- Lin, Y.E.; Stout, J.E.; Yu, V.L. Prevention of hospital-acquired legionellosis. Curr. Opin. Infect. Dis. 2011, 24, 350–356. [Google Scholar] [CrossRef]
- UK Department of Health. Health Technical Memorandum 04-01: Safe Water in Healthcare Premises Part A: Design, Installation and Commissioning. 2016. Available online: https://www.england.nhs.uk/wp-content/uploads/2021/05/DH_HTM_0401_PART_A_acc.pdf (accessed on 24 May 2023).
- Ministero della Salute. Linee Guida per la Prevenzione e il Controllo della Legionellosi; Ministero della Salute: Rome, Italy, 2000.
- Ministero della Salute. Linee Guida per la Prevenzione e il Controllo della Legionellosi. 2015. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2362_allegato.pdf (accessed on 24 May 2023).
- Lin, Y.E.; Stout, J.E.; Yu, V.L. Controlling Legionella in hospital drinking water: An evidence-based review of disinfection methods. Infect. Control. Hosp. Epidemiol. 2011, 32, 166–173. [Google Scholar] [CrossRef]
- US Environmental Protection Agency. Technologies for Legionella Control in Premise Plumbing Systems: Scientific Literature Review; EPA 810-R-16-001; Office of Water: Washington, DC, USA, 2016.
- Marchesi, I.; Marchegiano, P.; Bargellini, A.; Cencetti, S.; Frezza, G.; Miselli, M.; Borella, P. Effectiveness of different methods to control Legionella in the water supply: Ten-year experience in an Italian university hospital. J. Hosp. Infect. 2011, 77, 47–51. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Legionnaires’ disease. In ECDC. Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Gamage, S.D.; Ambrose, M.; Kralovic, S.M.; Roselle, G.A. Water safety and Legionella in health care. Infect. Dis. Clin. N. Am. 2016, 30, 689–712. [Google Scholar] [CrossRef]
- Scanlon, M.M.; Gordon, J.L.; McCoy, W.F.; Cain, M.F. Water Management for Construction: Evidence for Risk Characterization in Community and Healthcare Settings: A Systematic Review. Int. J. Environ. Res. Public Health. 2020, 17, 2168. [Google Scholar] [CrossRef]
- Coniglio, M.A.; Ferrante, M.; Yassin, M.H. Preventing Healthcare-Associated Legionellosis: Results after 3 Years of Continuous Disinfection of Hot Water with Monochloramine and an Effective Water Safety Plan. Int. J. Environ. Res. Public Health. 2018, 15, 1594. [Google Scholar] [CrossRef] [PubMed]
- Gavaldà, L.; Garcia-Nuñez, M.; Quero, S.; Gutierrez-Milla, C.; Sabrià, M. Role of hot water temperature and water system use on Legionella control in a tertiary hospital: An 8-year longitudinal study. Water Res. 2019, 149, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Whiley, H.; Bentham, R.; Brown, M.H. Legionella Persistence in Manufactured Water Systems: Pasteurization Potentially Selecting for Thermal Tolerance. Front. Microbiol. 2017, 8, 1330. [Google Scholar] [CrossRef] [PubMed]
- Cervero-Aragó, S.; Schrammel, B.; Dietersdorfer, E.; Sommer, R.; Lück, C.; Walochnik, J.; Kirschner, A. Viability and infectivity of viable but nonculturable Legionella pneumophila strains induced at high temperatures. Water Res. 2019, 158, 268–279. [Google Scholar] [CrossRef]
- Ammar, T.A.; Abid, K.Y.; El-Bindary, A.A.; El-Sonbati, A.Z. Chlorine dioxide bulk decay prediction in desalinated drinking water. Desalination 2014, 352, 45–51. [Google Scholar] [CrossRef]
- Yu, W.; Azhdar, B.; Andersson, A.; Reitberger, T.; Hassinen, J.; Hjertberg, T.; Gedde, U.W. Deterioration of polyethylene pipes exposed to water containing chlorine dioxide. Polym. Degrad. Stab. 2011, 96, 790–797. [Google Scholar] [CrossRef]
- Vertova, A.; Miani, A.; Lesma, G.; Rondinini, S.; Minguzzi, A.; Falciola, L.; Ortenzi, M.A. Chlorine Dioxide Degradation Issues on Metal and Plastic Water Pipes Tested in Parallel in a Semi-Closed System. Int. J. Environ. Res. Public Health 2019, 16, 4582. [Google Scholar] [CrossRef]
- Chord, F.; Fascia, P.; Mallaval, F.; Cornillon, J.; Roesch, L.; Pozzetto, B.; Grattard, F.; Berthelot, P. Chlorine dioxide for Legionella spp. disinfection: A danger for cross-linked polyethylene pipes? J. Hosp. Infect. 2011, 78, 242–243. [Google Scholar] [CrossRef]
- Zhang, Z.; Stout, J.E.; Yu, V.L.; Vidic, R. Effect of pipe corrosion scales on chlorine dioxide consumption in drinking water distribution systems. Water Res. 2008, 42, 129–136. [Google Scholar] [CrossRef]
- Edmonds, N. Monochloramine in Drinking-Water. Background Document for Development of WHO Guidelines for Drinking-Water Quality; World Health Organization: Genava, Switzerland, 2004. [Google Scholar]
- Kool, J.L.; Carpenter, J.C.; Fields, B.S. Effect of monochloramine disinfection of municipal drinking water on risk of nosocomial Legionnaires’ disease. Lancet 1999, 353, 272–277. [Google Scholar] [CrossRef]
- Heffelfinger, J.D.; Kool, J.L.; Fridkin, S.; Fraser, V.J.; Hageman, J.; Carpenter, J.; Whitney, C.G. Risk of hospital-acquired Legionnaires’ disease in cities using monochloramine versus other water disinfectants. Infect. Control. Hosp. Epidemiol. 2003, 24, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Flannery, B.; Gelling, L.B.; Vugia, D.J.; Weintraub, J.M.; Salerno, J.J.; Conroy, M.J.; Stevens, V.A.; Rose, C.E.; Moore, M.R.; Fields, B.S.; et al. Reducing Legionella colonization in water systems with monochloramine. Emerg. Infect. Dis. 2006, 12, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Copeland, A.; Lytle, D.A. Measuring the oxidation-reduction potential of important oxidants in drinking water. J. AWWA 2014, 106, E10–E20. [Google Scholar] [CrossRef]
- Jacangelo, J.G.; Olivieri, V.P.; Kawata, K. Investigating the Mechanism of Inactivation of Escherichia coli B by Monochloramine. J. AWWA 1991, 83, 80–87. [Google Scholar] [CrossRef]
- Lee, W.H.; Wahman, D.G.; Bishop, P.L.; Pressman, J.G. Free chlorine and monochloramine application to nitrifying biofilm: Comparison of biofilm penetration, activity, and viability. Environ. Sci. Technol. 2011, 45, 1412–1419. [Google Scholar] [CrossRef]
- Marchesi, I.; Ferranti, G.; Mansi, A.; Marcelloni, A.M.; Proietto, A.R.; Saini, N.; Borella, P.; Bargellini, A. Control of Legionella Contamination and Risk of Corrosion in Hospital Water Networks following Various Disinfection Procedures. Appl. Environ. Microb. 2016, 82, 2959–2965. [Google Scholar] [CrossRef]
- Marchesi, I.; Cencetti, S.; Marchegiano, P.; Frezza, G.; Borella, P.; Bargellini, A. Control of Legionella contamination in a hospital water distribution system by monochloramine. Am. J. Infect. Control. 2012, 40, 279–281. [Google Scholar] [CrossRef]
- Kandiah, S.; Yassin, M.H.; Hariri, R.; Ferrelli, J.; Fabrizio, M.; Porter, L.; Duda, S.; Stout, J. Control of Legionella Contamination with Monochloramine Disinfection in a Large Urban Hospital Hot Water System. Am. J. Inf. Cont. 2012, 40, e84. [Google Scholar] [CrossRef]
- Duda, S.; Kandiah, S.; Stout, J.E.; Baron, J.L.; Yassin, M.; Fabrizio, M.; Ferrelli, J.; Hariri, R.; Wagener, M.M.; Goepfert, J.; et al. Evaluation of a New Monochloramine Generation System for Controlling Legionella in Building Hot Water Systems. Infect. Contr. Hosp. Epidemiol. 2014, 35, 1356–1363. [Google Scholar] [CrossRef]
- Lytle, D.A.; Pfaller, S.; Muhlen, C.; Struewing, I.; Triantafyllidou, S.; White, C.; Hayes, S.; King, D.; Lu, J. A comprehensive evaluation of monochloramine disinfection on water quality, Legionella and other important microorganisms in a hospital. Water Res. 2021, 189, 116656. [Google Scholar] [CrossRef]
- Rindi, L.; Garzelli, C. Increase in non-tuberculous mycobacteria isolated from humans in Tuscany, Italy, from 2004 to 2014. BMC Infect. Dis. 2016, 1, 16–44. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, S.; King, D.; Mistry, J.H.; Donohue, M. Occurrence revisited: Mycobacterium avium and Mycobacterium intracellulare in potable water in the USA. Appl. Microbiol. Biotechnol. 2022, 106, 2715–2727. [Google Scholar] [CrossRef] [PubMed]
- Casini, B.; Baggiani, A.; Totaro, M.; Mansi, A.; Costa, A.L.; Aquino, F.; Miccoli, M.; Valentini, P.; Bruschi, F.; Lopalco, P.L.; et al. Detection of viable but non-culturable legionella in hospital water network following monochloramine disinfection. J. Hosp. Infect. 2018, 98, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, I.; Paduano, S.; Frezza, G.; Sircana, L.; Vecchi, E.; Zuccarello, P.; Olivieri Conti, G.; Ferrante, M.; Borella, P.; Bargellini, A. Safety and Effectiveness of Monochloramine Treatment for Disinfecting Hospital Water Networks. Int. J. Environ. Res. Public Health 2020, 17, 6116. [Google Scholar] [CrossRef]
- Biswas, S.; Rolain, J.M. Use of MALDI-TOF mass spectrometry for identification of bacteria that are difficult to culture. J. Microbiol. Methods. 2013, 92, 14–24. [Google Scholar] [CrossRef]
- Nomura, F. Proteome-based bacterial identification using matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS): A revolutionary shift in clinical diagnostic microbiology. Biochim. Biophys. Acta 2015, 185, 528–537. [Google Scholar] [CrossRef]
- Capocefalo, M.; Ridley, E.V.; Tranfield, E.Y.; Thompson, K.C. MALDI-TOF MS: A rapid microbiological confirmation technique for food and water analysis. In Molecular Microbial Diagnostic Methods—Pathways to Implementation for the Food and Water Industry; Academic Press: Cambridge, MA, USA, 2016; Chapter 9; pp. 185–220. [Google Scholar]
- Moliner, C.; Ginevra, C.; Jarraud, S.; Flaudrops, C.; Bedotto, M.; Couderc, C.; Etienne, J.; Fournier, P. Rapid identification of Legionella species by mass spectrometry. J. Med. Microbiol. 2010, 59, 273–284. [Google Scholar] [CrossRef]
- Dilger, T.; Melz, H.; Gessner, A. Rapid and reliable identification of waterborne Legionella species by MALDI-TOF mass spectrometry. J. Microbiol. Methods. 2016, 127, 154–159. [Google Scholar] [CrossRef]
- Pascale, M.R.; Mazzotta, M.; Salaris, S.; Girolamini, L.; Grottola, A.; Simone, M.L.; Cordovana, M.; Bisognin, F.; Dal Monte, P.; Bucci Sabbatini, M.A.; et al. Evaluation of MALDI–TOF Mass Spectrometry in Diagnostic and Environmental Surveillance of Legionella Species: A Comparison With Culture and Mip-Gene Sequencing Technique. Front. Microbiol. 2020, 11, 589369. [Google Scholar] [CrossRef]
- Lode, H.; Schafer, H.; Grothe, R.; Hartmann, H.; Ehret, W.; Ruckdeschel, G. Significance of Non-pneumophila Legionella Species in Adult Community-Acquired and Nosocomial Pneumonias. Klin Wochenschr. 1987, 65, 463–468. [Google Scholar] [CrossRef]
- Muder, R.; Yu, V.L. Infection Due to Legionella Species Other than L. pneumophila. Clin. Infect. Dis. 2002, 35, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Trnková, K.; Kotrbancová, M.; Špaleková, M.; Fulová, M.; Boledovičová, J.; Vesteg, M. MALDI-TOF MS analysis as a useful tool for an identification of Legionella pneumophila, a facultatively pathogenic bacterium interacting with free-living amoebae: A case study from water supply system of hospitals in Bratislava (Slovakia). Exp. Parasitol. 2018, 184, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Falkinham, J.O. Living with Legionella and Other Waterborne Pathogens. Microorganisms 2020, 8, 2026. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Year | NH2Cl (mg/L) | NH4+ (mg/L) |
|---|---|---|
| 2013 | 2.57 ± 0.35 | 0.39 ± 0.13 |
| 2014 | 2.50 ± 0.43 | 0.43 ± 0.08 |
| 2015 | 2.58 ± 0.62 | 0.34 ± 0.11 |
| 2016 | 2.66 ± 0.21 | 0.35 ± 0.14 |
| 2017 | 2.56 ± 0.17 | 0.35 ± 0.11 |
| 2018 | 2.51 ± 0.27 | 0.37 ± 0.10 |
| 2019 | 2.51 ± 0.25 | 0.40 ± 0.06 |
| 2020 | 2.53 ± 0.56 | 0.37 ± 0.06 |
| 2021 | 2.48 ± 0.55 | 0.33 ± 0.11 |
| 2022 | 2.49 ± 0.46 | 0.33 ± 0.10 |
| Year | Total Samples | Positive Samples (%) | Samples > 100 CFU/L (%) | ||
|---|---|---|---|---|---|
| 2013 | 148 | h | 138 | 0 (0.0%) | 0 (0.0%) |
| c | 9 | 0 (0.0%) | 0 (0.0%) | ||
| 2014 | 183 | h | 161 | 0 (0.0%) | 0 (0.0%) |
| c | 21 | 0 (0.0%) | 0 (0.0%) | ||
| 2015 | 191 | h | 171 | 0 (0.0%) | 0 (0.0%) |
| c | 20 | 0 (0.0%) | 0 (0.0%) | ||
| 2016 | 191 | h | 169 | 2 (1.2%) | 1 (0.5%) |
| c | 22 | 0 (0.0%) | 0 (0.0%) | ||
| 2017 | 259 | h | 232 | 4 (1.7%) | 1 (0.4%) |
| c | 27 | 0 (0.0%) | 0 (0.0%) | ||
| 2018 | 300 | h | 264 | 5 (1.9%) | 3 (1.1%) * |
| c | 36 | 1 (2.8%) | 1 (2.8%) | ||
| 2019 | 255 | h | 210 | 3 (1.4%) * | 0 (0.0%) |
| c | 45 | 0 (0.0%) | 0 (0.0%) | ||
| 2020 ** | 317 | h | 251 | 0 (0.0%) | 0 (0.0%) |
| c | 66 | 0 (0.0%) | 0 (0.0%) | ||
| 2021 ** | 363 | h | 296 | 0 (0.0%) | 0 (0.0%) |
| c | 67 | 0 (0.0%) | 0 (0.0%) | ||
| 2022 ** | 344 | h | 281 | 3 (1.1%) | 3 (1.1%) * |
| c | 63 | 0 (0.0%) | 0 (0.0%) | ||
| Year | Total Samples | P. aeruginosa | A. baumannii | S. maltophilia | Fusarium spp. | Aspergillus spp. | ||
|---|---|---|---|---|---|---|---|---|
| 2016 | 135 | h | 124 | 1 (0.8%) | 0 (0.0%) | 4 (3.2%) | 0 (0.0%) | 1 (0.8%) |
| c | 11 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| 2017 | 225 | h | 196 | 4 (2.0%) | 0 (0.0%) | 10 (5.1%) | 2 (1.0%) | 4 (2.0%) |
| c | 27 | 3 (11.1%) | 0 (0.0%) | 2 (7.4%) | 0 (0.0%) | 0 (0.0%) | ||
| 2018 | 268 | h | 236 | 5 (2.1%) | 1 (0.4%) | 1 (0.4%) | 2 (0.8%) | 3 (1.3%) |
| c | 32 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| 2019 | 307 | h | 261 | 18 (6.9%) | 0 (0.0%) | 8 (3.1%) | 1 (0.4%) | 6 (2.3%) |
| c | 46 | 5 (10.8%) | 0 (0.0%) | 4 (8.7%) | 2 (4.3%) | 4 (8.7%) | ||
| 2020 | 180 | h | 147 | 12 (8.2%) | 0 (0.0%) | 2 (1.4%) | 0 (0.0%) | 0 (0.0%) |
| c | 33 | 1 (0.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| 2021 | 14 | h | 14 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| c | 0 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| 2022 | 76 | / | 3 (3.9%) | 0 (0.0%) | 4 (5.3%) | 0 (0.0%) | 0 (0.0%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farina, C.; Cacciabue, E.; Averara, F.; Ferri, N.; Vailati, F.; Del Castillo, G.; Serafini, A.; Fermi, B.; Doniselli, N.; Pezzoli, F. Water Safety Plan, Monochloramine Disinfection and Extensive Environmental Sampling Effectively Control Legionella and Other Waterborne Pathogens in Nosocomial Settings: The Ten-Year Experience of an Italian Hospital. Microorganisms 2023, 11, 1794. https://doi.org/10.3390/microorganisms11071794
Farina C, Cacciabue E, Averara F, Ferri N, Vailati F, Del Castillo G, Serafini A, Fermi B, Doniselli N, Pezzoli F. Water Safety Plan, Monochloramine Disinfection and Extensive Environmental Sampling Effectively Control Legionella and Other Waterborne Pathogens in Nosocomial Settings: The Ten-Year Experience of an Italian Hospital. Microorganisms. 2023; 11(7):1794. https://doi.org/10.3390/microorganisms11071794
Chicago/Turabian StyleFarina, Claudio, Eleonora Cacciabue, Franca Averara, Nadia Ferri, Francesca Vailati, Gabriele Del Castillo, Antonello Serafini, Beatrice Fermi, Nicola Doniselli, and Fabio Pezzoli. 2023. "Water Safety Plan, Monochloramine Disinfection and Extensive Environmental Sampling Effectively Control Legionella and Other Waterborne Pathogens in Nosocomial Settings: The Ten-Year Experience of an Italian Hospital" Microorganisms 11, no. 7: 1794. https://doi.org/10.3390/microorganisms11071794
APA StyleFarina, C., Cacciabue, E., Averara, F., Ferri, N., Vailati, F., Del Castillo, G., Serafini, A., Fermi, B., Doniselli, N., & Pezzoli, F. (2023). Water Safety Plan, Monochloramine Disinfection and Extensive Environmental Sampling Effectively Control Legionella and Other Waterborne Pathogens in Nosocomial Settings: The Ten-Year Experience of an Italian Hospital. Microorganisms, 11(7), 1794. https://doi.org/10.3390/microorganisms11071794