
Lumbar Puncture and Meningitis in Infants with Proven Early- or Late-Onset Sepsis: An Italian Prospective Multicenter Observational Study

 , , ,
, , ,  ,
,  , ,
, ,  ,
, 
 , add
Show full author list
, add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions
- Preterm neonates: neonates born at less than 37 (<37) weeks’ gestation.
- Very-low-birth-weight (VLBW) neonates: neonates with a birth weight under 1500 (<1500) grams.
- Asymptomatic neonate: infant without any symptoms of sepsis, with positive blood culture collected because of the presence of maternal risk factors.
- Disease severity: mild, moderate, or severe disease according to the clinical judgment of the attending physician.
2.3. Statistical Analysis
3. Results
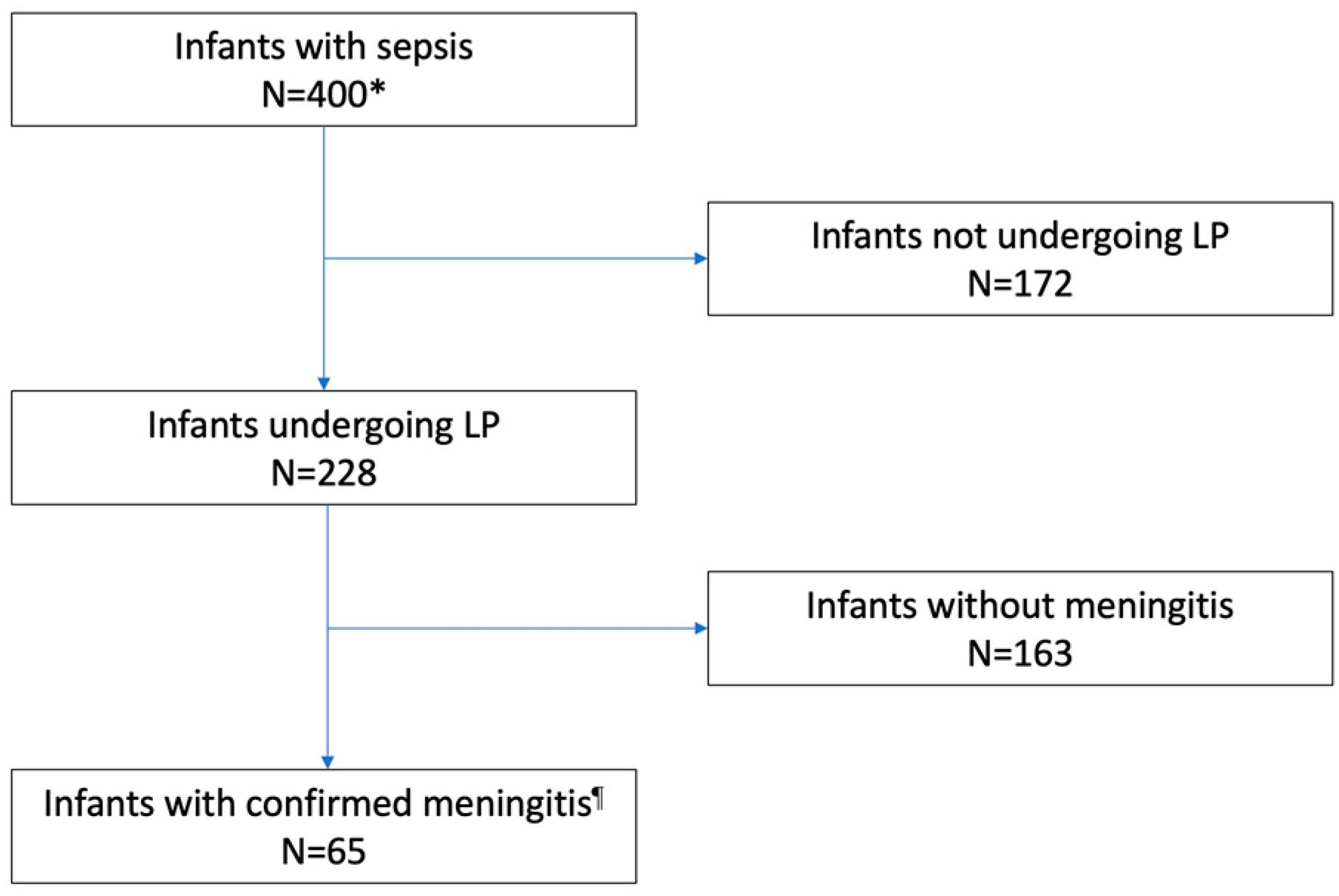
3.1. Performing an LP
3.2. CSF Parameters, Culture, Polymerase Chain Reaction, and Antibiotic Administration
3.3. Use of Antibiotics and Outcome according to LP
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Gordon, S.; Srinivasan, L.; Harris, M.C. Neonatal Meningitis: Overcoming Challenges in Diagnosis, Prognosis, and Treatment with Omics. Front. Pediatr. 2017, 5, 139. [Google Scholar] [CrossRef]
- Chatue Kamga, H.B. Neuroimaging complication of neonatal meningitis in full-term and near-term newborns: A retrospective study of one Center. Glob. Pediatr. Health 2016, 3, 2333794X16681673. [Google Scholar] [CrossRef]
- Tibussek, D.; Sinclair, A.; Yau, I.; Teatero, S.; Fittipaldi, N.; Richardson, S.E.; Mayatepek, E.; Jahn, P.; Askalan, R. Late-Onset Group B Streptococcal Meningitis Has Cerebrovascular Complications. J. Pediatr. 2015, 166, 1187–1192.e1. [Google Scholar] [CrossRef]
- de Louvois, J.; Halket, S.; Harvey, D. Neonatal meningitis in England and Wales: Sequelae at 5 years of age. Eur. J. Pediatr. 2005, 164, 730–734. [Google Scholar] [CrossRef]
- Ku, L.C.; Boggess, K.A.; Cohen-Wolkowiez, M. Bacterial meningitis in infants. Clin. Perinatol. 2015, 42, 29–45. [Google Scholar] [CrossRef]
- Nizet, V.; Klein, J.O. Bacterial Sepsis and Meningitis. In Infectious Diseases of the Fetus and Newborn Infant; Elsevier: Amsterdam, The Netherlands, 2010; pp. 222–275. [Google Scholar] [CrossRef]
- Bedetti, L.; Marrozzini, L.; Baraldi, A.; Spezia, E.; Iughetti, L.; Lucaccioni, L.; Berardi, A. Pitfalls in the diagnosis of meningitis in neonates and young infants: The role of lumbar puncture. J. Matern. Neonatal Med. 2019, 32, 4029–4035. [Google Scholar] [CrossRef]
- Bedetti, L.; Lugli, L.; Marrozzini, L.; Baraldi, A.; Leone, F.; Baroni, L.; Lucaccioni, L.; Rossi, C.; Roversi, M.F.; D’Amico, R.; et al. Safety and Success of Lumbar Puncture in Young Infants: A Prospective Observational Study. Front. Pediatr. 2021, 9, 692652. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.S.J.; Scrivens, A.; Bell, J.L.; Linsell, L.; Hardy, P.; Yong, J.; Williams, R.; Adams, E.; Sadarangani, M.; Juszczak, E.; et al. Assessment of infant position and timing of stylet removal to improve lumbar puncture success in neonates (NeoCLEAR): An open-label, 2 × 2 factorial, randomised, controlled trial. Lancet Child Adolesc. Health 2023, 7, 91–100. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Women’s and Children’s Health (UK). Bacterial Meningitis and Meningococcal Septicaemia: Management of Bacterial Meningitis and Meningococcal Septicaemia in Children and Young People Younger Than 16 Years in Primary and Secondary Care; RCOG Press: London, UK, 2010. [Google Scholar]
- Polin, R.A. Committee on Fetus and New- born. Management of neonates with suspected or proven early-onset bacterial sepsis. Pediatrics 2012, 129, 1006–1015. [Google Scholar] [CrossRef]
- Berardi, A.; Lugli, L.; Rossi, C.; China, M.C.; Vellani, G.; Contiero, R.; Calanca, F.; Camerlo, F.; Casula, F.; Di Carlo, C.; et al. Neonatal bacterial meningitis. Minerva Pediatr. 2010, 62 (Suppl. S1), 51–54. [Google Scholar] [PubMed]
- Srinivasan, L.; Harris, M.C.; Shah, S.S. Lumbar Puncture in the Neonate: Challenges in Decision Making and Interpretation. Semin. Perinatol. 2012, 36, 445–453. [Google Scholar] [CrossRef]
- UK National Institute for Health and Care Excellence. Neonatal Infection: Antibiotics for Prevention and Treatment. 20 April 2021. Available online: https://www.nice.org.uk/guidance/ng195 (accessed on 25 April 2023).
- Stoll, B.J.; Puopolo, K.M.; Hansen, N.I.; Sánchez, P.J.; Bell, E.F.; Carlo, W.A.; Cotten, C.M.; D’angio, C.T.; Kazzi, S.N.J.; Poindexter, B.B.; et al. Early-Onset Neonatal Sepsis 2015 to 2017, the Rise of Escherichia coli, and the Need for Novel Prevention Strategies. JAMA Pediatr. 2020, 174, e200593. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Sánchez, P.J.; Faix, R.G.; Poindexter, B.B.; Van Meurs, K.P.; Bizzarro, M.J.; Goldberg, R.N.; Frantz, I.D.; Hale, E.C.; et al. Early Onset Neonatal Sepsis: The Burden of Group B Streptococcal and E. coli Disease Continues. Pediatrics 2011, 127, 817–826. [Google Scholar] [CrossRef]
- Berardi, A.; Di Fazzio, G.; Gavioli, S.; Di Grande, E.; Groppi, A.; Papa, I.; Piccinini, G.; Simoni, A.; Tridapalli, E.; Volta, A.; et al. Universal Antenatal Screening for Group B Streptococcus in Emilia-romagna. J. Med. Screen. 2011, 18, 60–64. [Google Scholar] [CrossRef]
- Berardi, A.; Lugli, L.; Baronciani, D.; Creti, R.; Rossi, K.; Ciccia, M.; Gambini, L.; Mariani, S.; Papa, I.; Serra, L.; et al. Group B Streptococcal Infections in a Northern Region of Italy. Pediatrics 2007, 120, e487–e493. [Google Scholar] [CrossRef]
- Berardi, A.; Baroni, L.; Reggiani, M.L.B.; Ambretti, S.; Biasucci, G.; Bolognesi, S.; Capretti, M.G.; Carretto, E.; Ciccia, M.; Fiorini, V.; et al. The burden of early-onset sepsis in Emilia-Romagna (Italy): A 4-year, population-based study. J. Matern. Neonatal Med. 2016, 29, 3126–3131. [Google Scholar] [CrossRef]
- Verani, J.R.; McGee, L.; Schrag, S.J.; Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases; Centers for Disease Control and Prevention (CDC). Prevention of Perinatal Group B Streptococcal Disease–Revised Guidelines from CDC, 2010. MMWR Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2010, 59, 1–36. [Google Scholar]
- Miselli, F.; Costantini, R.C.; Creti, R.; Sforza, F.; Fanaro, S.; Ciccia, M.; Piccinini, G.; Rizzo, V.; Pasini, L.; Biasucci, G.; et al. Escherichia Coli Is Overtaking Group B Streptococcus in Early-Onset Neonatal Sepsis. Microorganisms 2022, 10, 1878. [Google Scholar] [CrossRef] [PubMed]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Haque, K.N. Definitions of bloodstream infection in the newborn. Pediatr. Crit. Care Med. 2005, 6 (Suppl. S3), S45–S49. [Google Scholar] [CrossRef]
- Farrell, J.J.; Hujer, A.M.; Sampath, R.; Bonomo, R.A. Salvage microbiology: Opportunities and challenges in the detection of bacterial path-ogens following initiation of antimicrobial treatment. Expert Rev. Mol. Diagn. 2015, 15, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Stocker, M.; Klingenberg, C.; Navér, L.; Nordberg, V.; Berardi, A.; el Helou, S.; Fusch, G.; Bliss, J.M.; Lehnick, D.; Dimopoulou, V.; et al. Less is more: Antibiotics at the beginning of life. Nat. Commun. 2023, 14, 1–9. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.; Fanaroff, A.A.; Wright, L.L.; Carlo, W.A.; Ehrenkranz, R.A.; Lemons, J.A.; Donovan, E.F.; Stark, A.R.; Tyson, J.E.; et al. To Tap or Not to Tap: High Likelihood of Meningitis Without Sepsis Among Very Low Birth Weight Infants. Pediatrics 2004, 113, 1181–1186. [Google Scholar] [CrossRef]
- Garges, H.P.; Moody, M.A.; Cotton, C.M.; Smith, P.B.; Tiffany, K.F.; Lenfestey, R.; Li, J.S.; Fowler, V.G.; Benjamin, D.K. Neonatal meningitis: What is the correlation among cerebrospinal fluid cultures, blood cultures, and cerebrospinal fluid parameters? Pediatrics 2006, 117, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, K.A.; Anderson-Berry, A.L.; Delair, S.F.; Davies, H.D. Early-onset neonatal sepsis. Clin. Microbiol. Rev. 2014, 27, 21–47. [Google Scholar] [CrossRef] [PubMed]
- Nigrovic, L.E.; Malley, R.; Macias, C.G.; Kanegaye, J.T.; Moro-Sutherland, D.M.; Schremmer, R.D.; Schwab, S.H.; Agrawal, D.; Mansour, K.M.; Bennett, J.E.; et al. Effect of Antibiotic Pretreatment on Cerebrospinal Fluid Profiles of Children with Bacterial Meningitis. Pediatrics 2008, 122, 726–730. [Google Scholar] [CrossRef] [PubMed]
- Kanegaye, J.T.; Soliemanzadeh, P.; Bradley, J.S. Lumbar puncture in pediatric bacterial meningitis: Defining the time interval for recovery of cerebrospinal fluid pathogens after parenteral antibiotic pretreatment. Pediatrics 2001, 108, 1169–1174. [Google Scholar] [CrossRef]
- Esparcia, O.; Montemayor, M.; Ginovart, G.; Pomar, V.; Soriano, G.; Pericas, R.; Gurgui, M.; Sulleiro, E.; Prats, G.; Navarro, F.; et al. Diagnostic accuracy of a 16S ribosomal DNA gene-based molecular technique (RT-PCR, microarray, and sequencing) for bacterial meningitis, early-onset neonatal sepsis, and spontaneous bacterial perito-nitis. Diagn. Microbiol. Infect. Dis. 2011, 69, 153–160. [Google Scholar] [CrossRef]
- Morrissey, S.M.; Nielsen, M.; Ryan, L.; Al Dhanhani, H.; Meehan, M.; McDermott, S.; O’sullivan, N.; Doyle, M.; Gavin, P.; Cunney, R.; et al. Group B streptococcal PCR testing in comparison to culture for diagnosis of late onset bacteraemia and meningitis in infants aged 7–90 days: A multi-centre diagnostic accuracy study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1317–1324. [Google Scholar] [CrossRef]


{kind=link}
| Variables | All Infants N = 400 | EOS N = 144 | LOS N = 256 | p |
|---|---|---|---|---|
| Pathogen, N (%) | ||||
| GBS | 251 (62.7) | 89 (61.8) | 162 (63.3) | 0.770 |
| E. coli | 149 (37.3) | 55 (38.2) | 94 (36.7) | |
| GA, wks (IQR) | 38 (31–40) | 38 (32–40) | 38 (31–40) | 0.356 |
| Preterm delivery, N (%) | 156 (39.1) | 52 (36.1) | 104 (40.8) | 0.358 |
| Body weight at birth, g (IQR) | 2887 (1476–3415) | 2932 (1517–3430) | 2877 (1475–3410) | 0.661 |
| Very-low-birth-weight neonates, n (%) | 102 (25.5%) | 36 (25.0) | 66 (25.8) | 0.863 |
| Sex (male), N (%) | 220 (55) | 65 (45.1) | 155 (60.5) | 0.003 |
| Twins, N (%) | 42 (10.5) | 7 (4.8) | 35 (13.7) | 0.006 |
| Mode of delivery, n (%) | ||||
| Vaginal | 249 (62.3) | 95 (66) | 154 (60.2) | 0.249 |
| Cesarean Section | 151 (37.7) | 49 (34) | 102 (39.8) |
| Variables | All N = 400 | EOS N = 144 | LOS N = 256 | p | GBS N = 251 | E. coli N = 149 | p |
|---|---|---|---|---|---|---|---|
| LP performed, N (%) | 228 (57) | 77 (53.5) | 151 (59.0) | 0.285 | 179 (71.3) | 49 (32.9) | <0.001 |
| LP performed in preterm infants, N (%) † | 84 (53.9) | 19 (36.6) | 65 (62.5) | 0.002 | 66 (72.5) | 18 (27.7) | <0.001 |
| LP in VLBW neonates, n (%) ¶ | 50 (49) | 11 (30.6) | 39 (59.1) | 0.006 | 38 (65.5) | 12 (27.3) | <0.001 |
| LP performed after initiation of antibiotics, N (%) § | 123 (53.9) | 55 (71.4) | 68 (45.0) | <0.001 | 94 (52.8) | 28 (57.1) | 0.590 |
| Hours lasting from initiation of antibiotics to LP, median (IQR) | 12 (24–48) | 24 (20–48) | 16 (6–36) | 0.014 | 24 (12–48) | 22 (8–34) | 0.438 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Pathogen (GBS vs. E. coli) | 0.197 | 0.12–0.30 | <0.001 | 0.20 | 0.13–0.32 | <0.001 |
| Preterm delivery | 0.815 | 0.54–1.22 | 0.325 | - | - | - |
| Birth weight | 1.00 | 0.99–1.00 | 0.153 | - | - | - |
| Higher disease severity | 1.435 | 1.11–1.84 | 0.005 | 1.34 | 1.02–1.77 | 0.031 |
| Center level | 0.505 | 0.28–0.91 | 0.023 | 0.72 | 0.37–1.39 | 0.335 |
| EOS vs. LOS | 1.25 | 0.82–1.88 | 0.285 | - | - | - |
| Postmenstrual age | 1.02 | 0.99–1.05 | 0.078 | - | - | - |
| Days of life at the sepsis | 1.00 | 0.99–1.00 | 0.756 | - | - | - |
| Variables | Culture or PCR Positive CSF (N = 42) | Sterile CSF (N = 93) | Missing | p | CSF Prior to Antibiotic Initiation in Positive PCR/Culture (N = 21) | CSF after Antibiotic Initiation in Positive PCR/Culture (N = 18) | Missing | p |
|---|---|---|---|---|---|---|---|---|
| Proteins | ||||||||
| Median (IQR) | 290 (198–500) | 80 (52–115) | 10 | <0.001 | 292 (216–500) | 243 (197–463) | 3 | 0.639 |
| Glucose | ||||||||
| Median (IQR) | 19 (9–35) | 51.5 (44.5–64) | 13 | <0.001 | 19 (9–32) | 23 (15–35) | 3 | 0.354 |
| Number of cells | ||||||||
| Median (IQR) | 345.5 (19–884.5) | 4 (2–11) | 13 | <0.001 | 500 (8–869) | 341 (53–1660) | 3 | 0.536 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bedetti, L.; Miselli, F.; Minotti, C.; Latorre, G.; Loprieno, S.; Foglianese, A.; Laforgia, N.; Perrone, B.; Ciccia, M.; Capretti, M.G.; et al. Lumbar Puncture and Meningitis in Infants with Proven Early- or Late-Onset Sepsis: An Italian Prospective Multicenter Observational Study. Microorganisms 2023, 11, 1546. https://doi.org/10.3390/microorganisms11061546
Bedetti L, Miselli F, Minotti C, Latorre G, Loprieno S, Foglianese A, Laforgia N, Perrone B, Ciccia M, Capretti MG, et al. Lumbar Puncture and Meningitis in Infants with Proven Early- or Late-Onset Sepsis: An Italian Prospective Multicenter Observational Study. Microorganisms. 2023; 11(6):1546. https://doi.org/10.3390/microorganisms11061546
Chicago/Turabian StyleBedetti, Luca, Francesca Miselli, Chiara Minotti, Giuseppe Latorre, Sabrina Loprieno, Alessandra Foglianese, Nicola Laforgia, Barbara Perrone, Matilde Ciccia, Maria Grazia Capretti, and et al. 2023. "Lumbar Puncture and Meningitis in Infants with Proven Early- or Late-Onset Sepsis: An Italian Prospective Multicenter Observational Study" Microorganisms 11, no. 6: 1546. https://doi.org/10.3390/microorganisms11061546
APA StyleBedetti, L., Miselli, F., Minotti, C., Latorre, G., Loprieno, S., Foglianese, A., Laforgia, N., Perrone, B., Ciccia, M., Capretti, M. G., Giugno, C., Rizzo, V., Merazzi, D., Fanaro, S., Taurino, L., Pulvirenti, R. M., Orlandini, S., Auriti, C., Haass, C., ... Berardi, A. (2023). Lumbar Puncture and Meningitis in Infants with Proven Early- or Late-Onset Sepsis: An Italian Prospective Multicenter Observational Study. Microorganisms, 11(6), 1546. https://doi.org/10.3390/microorganisms11061546