

Viral Identification Using Multiplex Polymerase Chain Reaction Testing Does Not Reduce Antibiotic Prescribing in Paediatric Intensive Care Units

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Setting
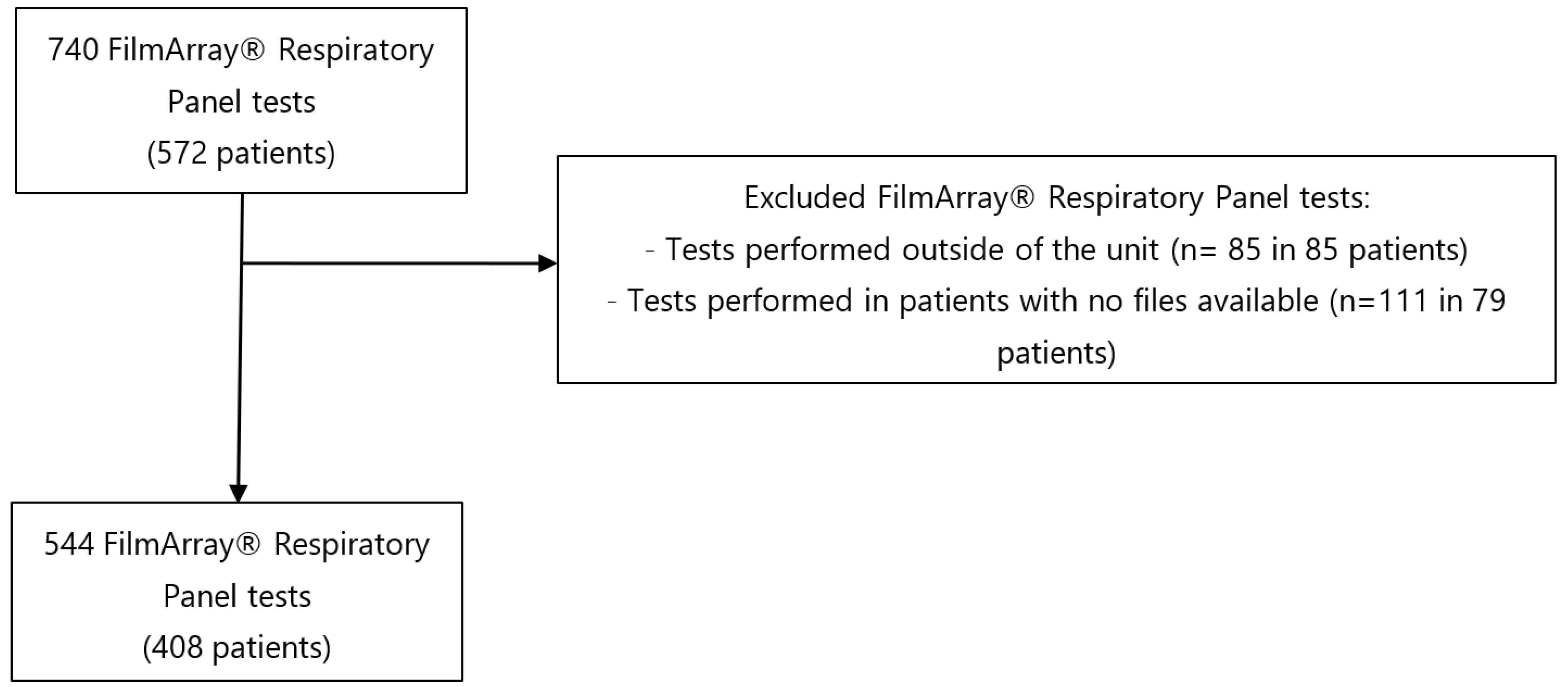
2.2. Population
2.3. Data Collection and Outcome Measures
2.4. Definition of Bacterial Infection
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Indication and Epidemiology of FilmArray® Respiratory Panel Tests
3.3. Bacterial Pulmonary Infection
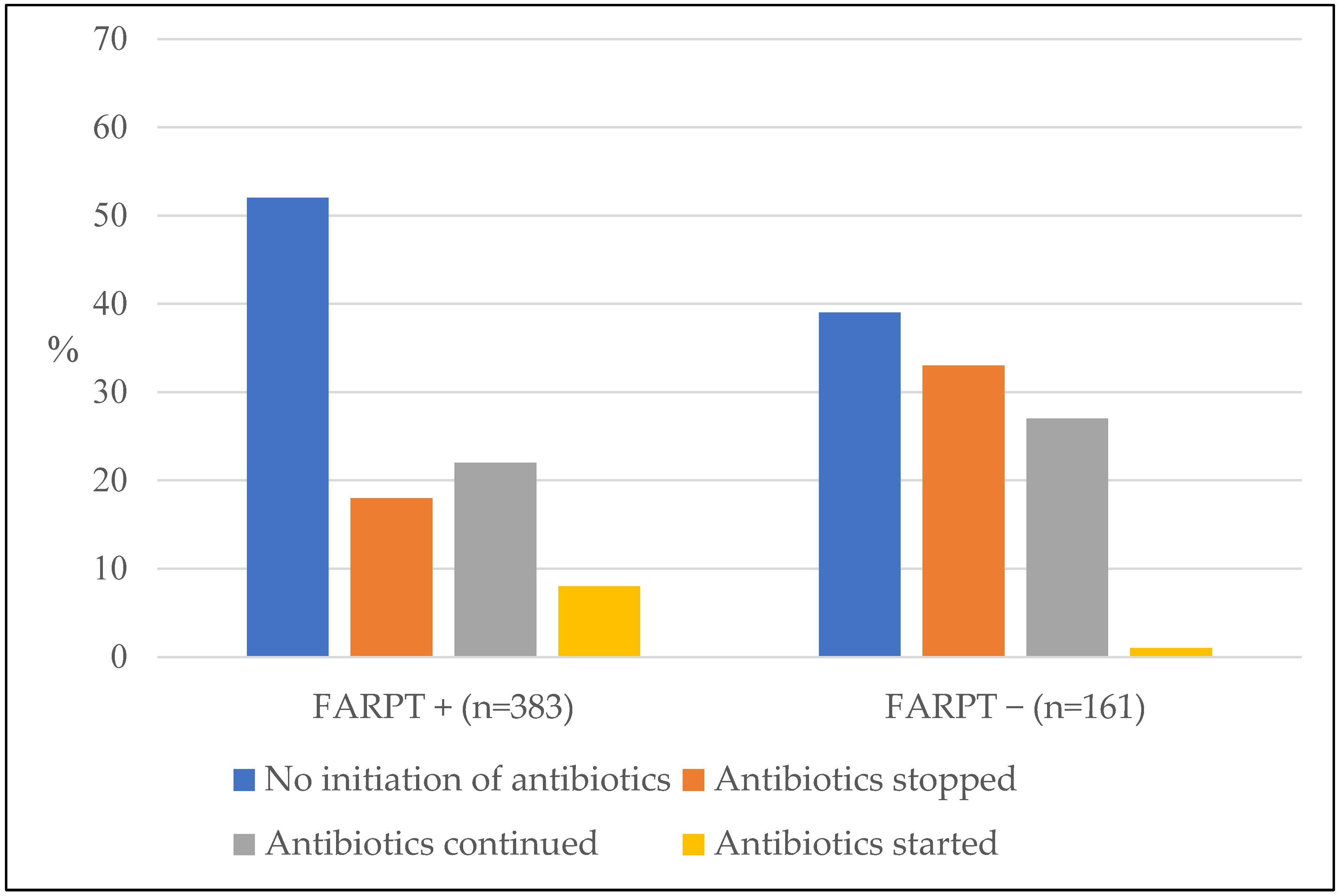
3.4. Impact of Viral Identification on Antibiotic Therapy Management and Factors Associated with the Absence of Antibiotics after the Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Basile, K.; Kok, J.; Dwyer, D.E. Point-of-Care Diagnostics for Respiratory Viral Infections. Expert Rev. Mol. Diagn. 2018, 18, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.J.; Hassan, F.; Lee, B.; Boom, J.; Sahni, L.C.; Johnson, C.; Dunn, J.; Payne, D.C.; Wikswo, M.E.; Parashar, U.; et al. Multiplex PCR Pathogen Detection in Acute Gastroenteritis Among Hospitalized US Children Compared with Healthy Controls During 2011-2016 in the Post-Rotavirus Vaccine Era. Open Forum Infect. Dis. 2021, 8, ofab592. [Google Scholar] [CrossRef]
- Lin, G.Y.-E.; Lin, C.-Y.; Chi, H.; Huang, D.T.-N.; Huang, C.-Y.; Chiu, N.-C. The Experience of Using FilmArray Meningitis/Encephalitis Panel for the Diagnosis of Meningitis and Encephalitis in Pediatric Patients. J. Microbiol. Immunol. Infect. 2022, 55, 1180–1187. [Google Scholar] [CrossRef]
- Brigadoi, G.; Gastaldi, A.; Moi, M.; Barbieri, E.; Rossin, S.; Biffi, A.; Cantarutti, A.; Giaquinto, C.; Da Dalt, L.; Donà, D. Point-of-Care and Rapid Tests for the Etiological Diagnosis of Respiratory Tract Infections in Children: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 1192. [Google Scholar] [CrossRef] [PubMed]
- Crook, J.; Xu, M.; Slaughter, J.C.; Willis, J.; Browning, W.; Estrada, C.; Gay, J.; Thomas, G.; Benton, A.; Quinn, C.; et al. Impact of Clinical Guidance and Rapid Molecular Pathogen Detection on Evaluation and Outcomes of Febrile or Hypothermic Infants. Infect. Control Hosp. Epidemiol. 2020, 41, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Babady, N.E. The FilmArray® Respiratory Panel: An Automated, Broadly Multiplexed Molecular Test for the Rapid and Accurate Detection of Respiratory Pathogens. Expert Rev. Mol. Diagn. 2013, 13, 779–788. [Google Scholar] [CrossRef]
- Mengelle, C.; Mansuy, J.M.; Pierre, A.; Claudet, I.; Grouteau, E.; Micheau, P.; Sauné, K.; Izopet, J. The Use of a Multiplex Real-Time PCR Assay for Diagnosing Acute Respiratory Viral Infections in Children Attending an Emergency Unit. J. Clin. Virol. 2014, 61, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Kitano, T.; Nishikawa, H.; Suzuki, R.; Onaka, M.; Nishiyama, A.; Kitagawa, D.; Oka, M.; Masuo, K.; Yoshida, S. The Impact Analysis of a Multiplex PCR Respiratory Panel for Hospitalized Pediatric Respiratory Infections in Japan. J. Infect. Chemother. 2020, 26, 82–85. [Google Scholar] [CrossRef]
- Esposito, S.; Mencacci, A.; Cenci, E.; Camilloni, B.; Silvestri, E.; Principi, N. Multiplex Platforms for the Identification of Respiratory Pathogens: Are They Useful in Pediatric Clinical Practice? Front. Cell. Infect. Microbiol. 2019, 9, 196. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 LRI Collaborators Age-Sex Differences in the Global Burden of Lower Respiratory Infections and Risk Factors, 1990–2019: Results from the Global Burden of Disease Study 2019. Lancet Infect. Dis. 2022, 22, 1626–1647. [CrossRef]
- Kissoon, N.; Uyeki, T.M. Sepsis and the Global Burden of Disease in Children. JAMA Pediatr. 2016, 170, 107–108. [Google Scholar] [CrossRef]
- Audry-Degardin, E.; Dubos, F.; Leteurtre, S.; Beaucaire, G.; Leclerc, F. Evaluation of the antibiotic prescription in a paediatric intensive care unit. Arch. Pediatr. 2007, 14, 157–163. [Google Scholar] [CrossRef]
- Maugat, S.; Berger-Carbonne, A.; Colomb-Cotinat, M.; Cavalié, P.; Coignard, B.; Dumartin, C.; Péfau, M.; Reyraud, E.; Dugravot, L.; Simon, L.; et al. Antibiotiques et Résistance Bactérienne: Une Menace Mondiale, des Conséquences Individuelles; Santé Publique France: Paris, France, 2019. [Google Scholar]
- Mortamet, G.; Morello, R.; Jokic, M.; Vabret, A.; Leroux, M.; Brouard, J.; Dina, J. Winter viral ecology in a pediatric intensive care unit: A prospective study. Arch. Pediatr. 2015, 22, 368–372. [Google Scholar] [CrossRef]
- Lee, K.H.; Gordon, A.; Foxman, B. The Role of Respiratory Viruses in the Etiology of Bacterial Pneumonia: An Ecological Perspective. Evol. Med. Public Health 2016, 2016, 95–109. [Google Scholar] [CrossRef]
- Pavia, A.T. Viral Infections of the Lower Respiratory Tract: Old Viruses, New Viruses, and the Role of Diagnosis. Clin. Infect. Dis. 2011, 52 (Suppl. 4), S284–S289. [Google Scholar] [CrossRef] [PubMed]
- Lamrani Hanchi, A.; Guennouni, M.; Rachidi, M.; Benhoumich, T.; Bennani, H.; Bourrous, M.; Maoulainine, F.M.R.; Younous, S.; Bouskraoui, M.; Soraa, N. Epidemiology of Respiratory Pathogens in Children with Severe Acute Respiratory Infection and Impact of the Multiplex PCR Film Array Respiratory Panel: A 2-Year Study. Int. J. Microbiol. 2021, 2021, 2276261. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Williams, D.J.; Arnold, S.R.; Ampofo, K.; Bramley, A.M.; Reed, C.; Stockmann, C.; Anderson, E.J.; Grijalva, C.G.; Self, W.H.; et al. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Children. N. Engl. J. Med. 2015, 372, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Launes, C.; de-Sevilla, M.-F.; Selva, L.; Garcia-Garcia, J.-J.; Pallares, R.; Muñoz-Almagro, C. Viral Coinfection in Children Less than Five Years Old with Invasive Pneumococcal Disease. Pediatr. Infect. Dis. J. 2012, 31, 650–653. [Google Scholar] [CrossRef]
- Rodrigues, C.M.C.; Groves, H. Community-Acquired Pneumonia in Children: The Challenges of Microbiological Diagnosis. J. Clin. Microbiol. 2018, 56, e01318-17. [Google Scholar] [CrossRef]
- Man, W.H.; van Houten, M.A.; Mérelle, M.E.; Vlieger, A.M.; Chu, M.L.J.N.; Jansen, N.J.G.; Sanders, E.A.M.; Bogaert, D. Bacterial and Viral Respiratory Tract Microbiota and Host Characteristics in Children with Lower Respiratory Tract Infections: A Matched Case-Control Study. Lancet Respir. Med. 2019, 7, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Zar, H.J.; Andronikou, S.; Nicol, M.P. Advances in the Diagnosis of Pneumonia in Children. BMJ 2017, 358, j2739. [Google Scholar] [CrossRef] [PubMed]
- 2016 CDC’s National Healthcare Safety Network Patient Safety Component Manual. Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/pcsmanual_current.pdf (accessed on 2 January 2023).
- Mayer, L.M.; Kahlert, C.; Rassouli, F.; Vernazza, P.; Albrich, W.C. Impact of Viral Multiplex Real-Time PCR on Management of Respiratory Tract Infection: A Retrospective Cohort Study. Pneumonia (Nathan) 2017, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Busson, L.; Bartiaux, M.; Brahim, S.; Konopnicki, D.; Dauby, N.; Gérard, M.; De Backer, P.; Van Vaerenbergh, K.; Mahadeb, B.; Mekkaoui, L.; et al. Contribution of the FilmArray Respiratory Panel in the Management of Adult and Pediatric Patients Attending the Emergency Room during 2015–2016 Influenza Epidemics: An Interventional Study. Int. J. Infect. Dis. 2019, 83, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Claassen-Weitz, S.; Lim, K.Y.L.; Mullally, C.; Zar, H.J.; Nicol, M.P. The Association between Bacteria Colonizing the Upper Respiratory Tract and Lower Respiratory Tract Infection in Young Children: A Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2021, 27, 1262–1270. [Google Scholar] [CrossRef]
- Fontela, P.S.; Quach, C.; Karim, M.E.; Willson, D.F.; Gilfoyle, E.; McNally, J.D.; Gonzales, M.; Papenburg, J.; Reynolds, S.; Lacroix, J.; et al. Determinants of Antibiotic Tailoring in Pediatric Intensive Care: A National Survey. Pediatr. Crit. Care Med. 2017, 18, e395–e405. [Google Scholar] [CrossRef]
- Moreno, L.; Barría, S.; Ferrero, F. Recommendations for the Management of Acute Lower Respiratory Tract Infections in Children under 2 Years of Age, 2021. Considerations for Strengthening the First Level of Care. Arch. Argent. Pediatr. 2021, 119, 292–293. [Google Scholar] [CrossRef]
- van de Maat, J.S.; Garcia Perez, D.; Driessen, G.J.A.; van Wermeskerken, A.-M.; Smit, F.J.; Noordzij, J.G.; Tramper-Stranders, G.; Obihara, C.C.; Punt, J.; Moll, H.A.; et al. The Influence of Chest X-Ray Results on Antibiotic Prescription for Childhood Pneumonia in the Emergency Department. Eur. J. Pediatr. 2021, 180, 2765–2772. [Google Scholar] [CrossRef]
- Bradshaw, M.L.; Déragon, A.; Puligandla, P.; Emeriaud, G.; Canakis, A.-M.; Fontela, P.S. Treatment of Severe Bronchiolitis: A Survey of Canadian Pediatric Intensivists. Pediatr. Pulmonol. 2018, 53, 613–618. [Google Scholar] [CrossRef]
- King, P.T.; Buttery, J. Emerging Role of Viral and Bacterial Co-Infection in Early Childhood. Respirology 2018, 23, 128–129. [Google Scholar] [CrossRef]
- Li, J.; Tao, Y.; Tang, M.; Du, B.; Xia, Y.; Mo, X.; Cao, Q. Rapid Detection of Respiratory Organisms with the FilmArray Respiratory Panel in a Large Children’s Hospital in China. BMC Infect. Dis. 2018, 18, 510. [Google Scholar] [CrossRef]
- Chakhunashvili, G.; Wagner, A.L.; Power, L.E.; Janusz, C.B.; Machablishvili, A.; Karseladze, I.; Tarkhan-Mouravi, O.; Zakhashvili, K.; Imnadze, P.; Gray, G.C.; et al. Severe Acute Respiratory Infection (SARI) Sentinel Surveillance in the Country of Georgia, 2015-2017. PLoS ONE 2018, 13, e0201497. [Google Scholar] [CrossRef] [PubMed]
- Garegnani, L.; Styrmisdóttir, L.; Roson Rodriguez, P.; Escobar Liquitay, C.M.; Esteban, I.; Franco, J.V. Palivizumab for Preventing Severe Respiratory Syncytial Virus (RSV) Infection in Children. Cochrane Database Syst. Rev. 2021, 11, CD013757. [Google Scholar] [CrossRef] [PubMed]
- Haute Autorité de Santé. Prise En Charge Du 1er Épisode de Bronchiolite Aiguë Chez Le Nourrisson de Moins de 12 Mois; HAS: Saint-Denis La Plaine, France, 2019. [Google Scholar]
- Duyu, M.; Karakaya, Z. Viral Etiology and Outcome of Severe Lower Respiratory Tract Infections among Critically Ill Children Admitted to the PICU. Med. Intensiva. (Engl. Ed.) 2021, 45, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Gastli, N.; Loubinoux, J.; Daragon, M.; Lavigne, J.-P.; Saint-Sardos, P.; Pailhoriès, H.; Lemarié, C.; Benmansour, H.; d’Humières, C.; Broutin, L.; et al. Multicentric Evaluation of BioFire FilmArray Pneumonia Panel for Rapid Bacteriological Documentation of Pneumonia. Clin. Microbiol. Infect. 2021, 27, 1308–1314. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | N = 544 n (%) Median (IQR) |
|---|---|
| Age (month) | 7 (2–31) |
| Sex (male) | 306 (56%) |
| PIM2 score | 1 (1–5) |
| PELOD-2 score | 1 (0–3) |
| Comorbidity | 370 (68%) |
| Prematurity | 115 (21%) |
| immunodeficiency | 24 (4%) |
| Heart disease | 88 (16%) |
| Pulmonary disease | 121 (22%) |
| Encephalopathy | 95 (17%) |
| Sickle cell disease | 29 (5%) |
| History of LRTI | 123 (23%) |
| Recent hospitalisation within 6 months | 129 (24%) |
| Reason for hospitalization | |
| Respiratory failure | 379 (70%) |
| Hemodynamic failure | 44 (8%) |
| Metabolic abnormality | 25 (5%) |
| Neurological failure | 70 (13%) |
| Faintness | 38 (7%) |
| Duration of Ventilation Support (days) | 3 (0–9) |
| Length of stay (PICU) (days) | 5 (3–12) |
| Death | 34 (6%) |
| FARPT + (n = 383) | FARPT − (n = 161) | ||
|---|---|---|---|
| n (%) Median (IQR) | n (%) Median (IQR) | p-Value | |
| Baseline characteristics | |||
| Age (month) | 7 (2–22) | 6 (1–71) | <0.001 |
| Score PIM-2 (%) | 1 (1–4) | 4 (1–10) | <0.001 |
| Score PELOD-2 (%) | 0 (0–3) | 2 (0–4) | <0.001 |
| Comorbidity | 250 (65%) | 120 (74%) | 0.04 |
| Prematurity | 96 (25%) | 19 (12%) | <0.001 |
| immunodeficiency | 11 (3%) | 13 (8%) | 0.01 |
| Heart disease | 57 (15%) | 31 (19%) | 0.26 |
| Pulmonary disease | 94 (25%) | 27 (17%) | 0.06 |
| Encephalopathy | 59 (15%) | 36 (22%) | 0.07 |
| Sickle cell disease | 12 (3%) | 17 (11%) | <0.001 |
| History of LRTI | 80 (21%) | 43 (26%) | 0.17 |
| Recent hospitalisation within 6 months | 286 (75%) | 93 (58%) | <0.01 |
| Reason for hospitalization | |||
| Respiratory failure | 286 (75%) | 93 (58%) | <0.001 |
| Hemodynamic failure | 31 (8%) | 13 (8%) | 0.99 |
| Neurological failure | 50 (13%) | 20 (12%) | 0.95 |
| Metabolic abnormality | 17 (4%) | 8 (5%) | 0.92 |
| Post-operative | 16 (4%) | 11 (7%) | 0.28 |
| Faintness | 23 (6%) | 15 (9%) | 0.23 |
| Symptoms and treatments before testing | |||
| Length of fever (days) | 1 (0–1) | 1 (0–2) | <0.001 |
| No fever | 111 (29%) | 43 (27%) | 0.65 |
| 1 day | 186 (49%) | 50 (31%) | <0.001 |
| 2 days | 85 (22%) | 68 (42%) | <0.001 |
| No antibiotics | 231 (60%) | 65 (40%) | <0.001 |
| Duration of antibiotics (days) | 0 (0–1) | 1 (0–2) | <0.001 |
| 1 day | 89 (23%) | 36 (22%) | 0.91 |
| 2 days | 63 (17%) | 60 (37%) | <0.001 |
| IMV | 69 (18%) | 61 (39%) | <0.001 |
| NIV | 216 (56%) | 94 (58%) | 0.74 |
| HFOT | 37 (10%) | 8 (5%) | 0.1 |
| Oxygen glasses | 116 (30%) | 29 (18%) | <0.01 |
| Fluid resuscitation | 86 (22%) | 40 (25%) | 0.62 |
| Presence of vasoactive drugs | 23 (6%) | 13 (8%) | 0.15 |
| Reason for testing | |||
| ACS | 5 (1%) | 14 (9%) | <0.001 |
| Bronchiolitis | 119 (31%) | 12 (7%) | <0.001 |
| Acute asthma | 59 (15%) | 6 (4%) | <0.001 |
| CAP | 61 (16%) | 23 (14%) | 0.72 |
| HAP | 53 (14%) | 52 (32%) | <0.001 |
| Faintness | 14 (4%) | 15 (9%) | 0.01 |
| Meningoencephalitis | 27 (7%) | 12 (8%) | 1 |
| Fever and complementary exams when FARPT was performed | |||
| Fever within 6 h | 245 (65%) | 101 (64%) | 0.86 |
| Radiological abnormality | 268 (70%) | 114 (71%) | 0.93 |
| Radiological focus | 47 (16%) | 14 (12%) | 0.03 |
| CRP (mg/L) | 19 (0–61) | 16 (0–64) | 0.85 |
| WBC (/mm3) | 12,810 (8600–17,600) | 12,960 (7993–19,760) | 0.65 |
| Evolution post-test | |||
| Duration of antibiotics (days) | 0 (0–1) | 0 (0–2) | 0.68 |
| Duration of hospitalization (days) | 5 (3–9) | 8 (3–20) | <0.001 |
| Duration of ventilation support (days) | 3 (0–6) | 6 (1–19) | <0.001 |
| Presence of vasoactive drugs | 28 (7%) | 16 (10%) | 0.39 |
| Death | 23 (6%) | 11 (7%) | 0.76 |
| Bacterial Infection (n = 96) | No Bacterial Infection (n = 287) | ||
|---|---|---|---|
| n (%) Median (IQR) | n (%) Median (IQR) | p-Value | |
| Baseline characteristics | |||
| Age (month) | 9 (2–54) | 7 (2–18) | 0.01 |
| Comorbidity | 70 (73%) | 180 (62%) | 0.09 |
| Prematurity | 28 (29%) | 68 (24%) | 0.35 |
| immunodeficiency | 2 (2%) | 9 (3%) | 0.74 |
| Heart disease | 18 (19%) | 39 (14%) | 0.29 |
| Pulmonary disease | 24 (25%) | 70 (24%) | 1 |
| Encephalopathy | 21 (22%) | 38 (13%) | 0.06 |
| Sickle cell disease | 4 (4%) | 8 (3%) | 0.50 |
| History of LRTI | 21 (22%) | 59 (21%) | 0.89 |
| Recent hospitalisation within 6 months | 19 (20%) | 59 (21%) | 0.99 |
| Reason for testing | |||
| ACS | 3 (3%) | 2 (<1%) | 0.10 |
| Bronchiolitis | 20 (21%) | 99 (18%) | 0.02 |
| Acute asthma | 10 (11%) | 49 (9%) | 0.16 |
| CAP | 36 (38%) | 25 (5%) | <0.001 |
| HAP | 17 (18%) | 36 (7%) | 0.27 |
| Faintness | 1 (1%) | 13 (2%) | 0.20 |
| Meningoencephalitis | 2 (2%) | 25 (5%) | 0.04 |
| Viral identification | |||
| RSV | 24 (25%) | 82 (29%) | 0.58 |
| HRV | 47 (49%) | 168 (58%) | 0.13 |
| Adenovirus | 14 (14%) | 41 (14%) | 1 |
| Metapneumovirus | 10 (10%) | 15 (5%) | 0.12 |
| Coronavirus | 7 (7%) | 17 (6%) | 0.92 |
| Influenza | 9 (9%) | 17 (6%) | 0.44 |
| Parainfluenza | 16 (17%) | 32 (11%) | 0.22 |
| Fever and complementary exams | |||
| Fever within 6 h | 73 (78%) | 172 (61%) | <0.01 |
| Radiological abnormality | 88 (88%) | 180 (37%) | <0.001 |
| CRP (mg/L) | 61 (13–109) | 14 (0–36) | <0.001 |
| WBC (/mm3) | 13,100 (7403–20,650) | 12,710 (9030–16,940) | 0.74 |
| Evolution | |||
| Duration of hospitalization (days) | 8 (5–16) | 4 (3–6) | <0.001 |
| Duration of ventilation support (days) | 6 (3–12) | 2 (0–5) | <0.001 |
| Death | 9 (9%) | 14 (5%) | 0.17 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR a Adjusted (CI 95%) | p-Value | OR b Adjusted (CI 95%) | p-Value | |
| Viral identification | 0.56 (0.35–0.89) | 0.01 | 0.31 (0.15–0.65) | <0.01 |
| RSV | 1.20 (0.67–2.14) | 0.54 | ||
| HRV | 1.41 (0.86–2.33) | 0.18 | ||
| Adenovirus | 1.10 (0.55–2.22) | 0.78 | ||
| Metapneumovirus | 0.42 (0.16–1.09) | 0.07 | ||
| Coronavirus | 1.53 (0.56–4.19) | 0.41 | ||
| Influenza | 0.78 (0.31–1.99) | 0.60 | ||
| Parainfluenza | 1.00 (0.48–2.08) | 0.99 | ||
| Antibiotics before test | 0.11 (0.07–0.17) | <0.001 | ||
| Baseline characteristics | ||||
| Age | 0.88 (0.83–0.92) | <0.001 | 0.91 (0.83–0.99) | 0.02 |
| Comorbidity | 0.43 (0.27–0.70) | <0.001 | ||
| Prematurity | 0.75 (0.45–1.24) | 0.26 | ||
| immunodeficiency | 0.47 (0.19–1,16) | 0.11 | ||
| Heart disease | 0.78 (0.47–1.67) | 0.39 | ||
| Pulmonary disease | 0.62 (0.38–1.01) | 0.06 | ||
| Encephalopathy | 0.70 (0.41–1.20) | 0.20 | ||
| Sickle cell disease | 0.24 (0.09–0.59) | <0.01 | ||
| History of LRTI | 0.54 (0.34–0.88) | 0.01 | ||
| Recent hospitalisation within 6 months | 0.67 (0.42–1.08) | 0.10 | ||
| Reason for testing | ||||
| Bronchiolitis | 1.65 (0.94–2.91) | 0.08 | ||
| Acute asthma | 1.27 (0.61–2.67) | 0.52 | ||
| CAP | 0.27 (0.15–0.46) | <0.001 | ||
| HAP | 0.77 (0.46–1.28) | 0.31 | ||
| Faintness | 6.40 (1.44–29.04) | 0.01 | ||
| Meningoencephalitis | 10.77 (2.45–47.36) | <0.01 | ||
| Fever and complementary exams | ||||
| CRP > 18 mg/L | 0.37 (0.22–0.61) | <0.001 | 0.45 (0.25–0.82) | <0.01 |
| WBC increased | 0.80 (0.50–1.29) | 0.37 | ||
| Presence of fever H-6 | 0.47 (0.29–0.76) | <0.01 | ||
| No radiological abnormalities | 6.93 (3.52–13.65) | <0.001 | 5.92 (2.60–13.51) | <0.001 |
| Focal infiltrates | 0.04 (0.01–0.10) | <0.001 | ||
| Treatments before testing | ||||
| IMV | 1.03 (0.64–1.66) | 0.91 | ||
| NIV | 0.42 (0.27–0.65) | <0.001 | 0.30 (0.16–0.59) | <0.001 |
| Presence of vasoactive drugs | 1.10 (0.52–2.35) | 0.81 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayotte, A.; Mariani-Kurkdjian, P.; Boizeau, P.; Dauger, S.; Riaud, C.; Lacarra, B.; Bourmaud, A.; Levy, M. Viral Identification Using Multiplex Polymerase Chain Reaction Testing Does Not Reduce Antibiotic Prescribing in Paediatric Intensive Care Units. Microorganisms 2023, 11, 884. https://doi.org/10.3390/microorganisms11040884
Hayotte A, Mariani-Kurkdjian P, Boizeau P, Dauger S, Riaud C, Lacarra B, Bourmaud A, Levy M. Viral Identification Using Multiplex Polymerase Chain Reaction Testing Does Not Reduce Antibiotic Prescribing in Paediatric Intensive Care Units. Microorganisms. 2023; 11(4):884. https://doi.org/10.3390/microorganisms11040884
Chicago/Turabian StyleHayotte, Aurélie, Patricia Mariani-Kurkdjian, Priscilla Boizeau, Stéphane Dauger, Charline Riaud, Boris Lacarra, Aurélie Bourmaud, and Michael Levy. 2023. "Viral Identification Using Multiplex Polymerase Chain Reaction Testing Does Not Reduce Antibiotic Prescribing in Paediatric Intensive Care Units" Microorganisms 11, no. 4: 884. https://doi.org/10.3390/microorganisms11040884
APA StyleHayotte, A., Mariani-Kurkdjian, P., Boizeau, P., Dauger, S., Riaud, C., Lacarra, B., Bourmaud, A., & Levy, M. (2023). Viral Identification Using Multiplex Polymerase Chain Reaction Testing Does Not Reduce Antibiotic Prescribing in Paediatric Intensive Care Units. Microorganisms, 11(4), 884. https://doi.org/10.3390/microorganisms11040884