
Six-Month Synbio® Administration Affects Nutritional and Inflammatory Parameters of Older Adults Included in the PROBIOSENIOR Project

 , ,
, , 
 , , ,
, , ,  ,
,  ,
,  , and add
Show full author list
, and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. PROBIOSENIOR Study Design
2.2. Detection and Quantification of Biogenic Amines
2.3. Gene Expression and Protein Quantification of TNF-α and IGF-1
2.4. Detection and Quantification of Cytokines in Blood and Faeces
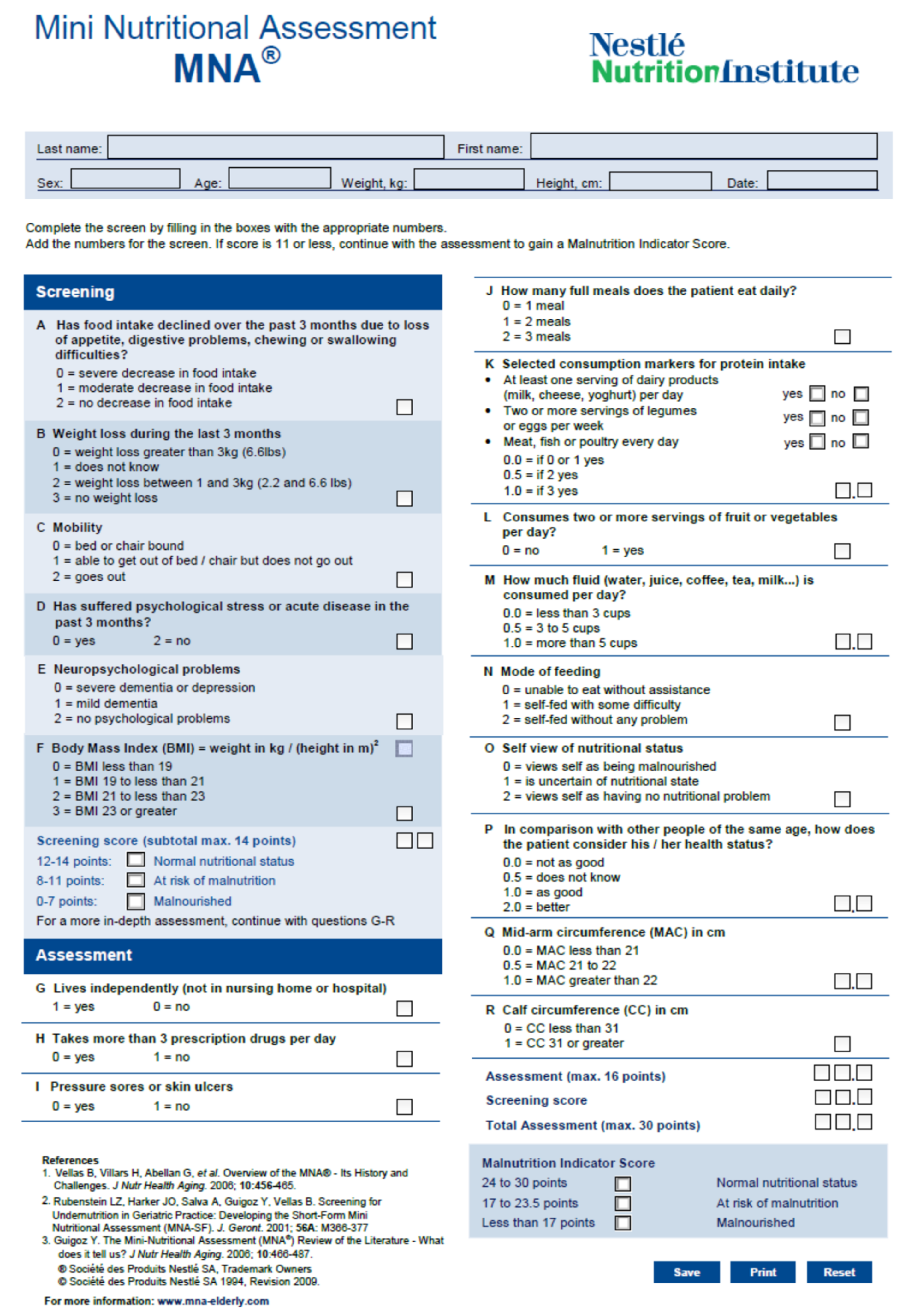
2.5. Mini Nutritional Assessment (MNA)
2.6. Statistical Analysis
3. Results
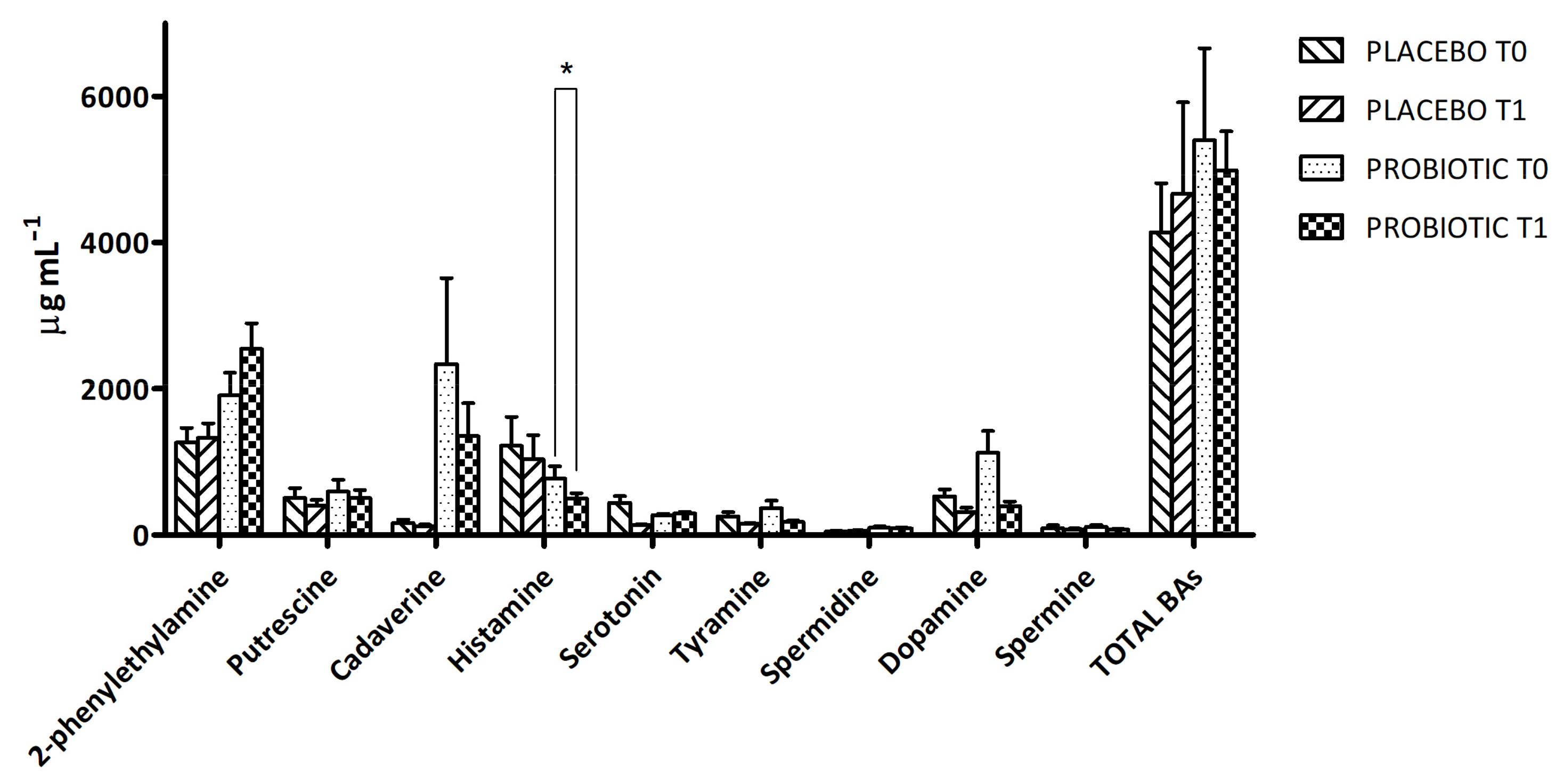
3.1. Detection and Quantification of Biogenic Amines
3.2. Evaluation of TNF-α and IGF-1
3.3. Detection and Quantification of Cytokines
3.3.1. Serum Cytokines’ Profile
3.3.2. Faeces Cytokines’ Profile
3.4. Nutritional Status Assessment
4. Discussion
5. Conclusions
Supplementary Materials
 T0 and
T0 and  T1).
T1).Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Cohen, J.E. Human Population: The Next Half Century. Science 2003, 302, 1172–1175. [Google Scholar] [CrossRef] [PubMed]
- Fane, M.; Weeraratna, A.T. How the ageing microenvironment influences tumour progression. Nat. Rev. Cancer. 2020, 20, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Dan, X.; Babbar, M.; Wei, Y.; Hasselbalch, S.G.; Croteau, D.L.; Bohr, V.A. Ageing as a risk factor for neurodegenerative disease. Nat. Rev. Neurol. 2019, 15, 565–581. [Google Scholar] [CrossRef] [PubMed]
- North, B.J.; Sinclair, D.A. The Intersection between Aging and Cardiovascular Disease. Circ. Res. 2012, 110, 1097–1108. [Google Scholar] [CrossRef]
- Franceschi, C.; Campisi, J. Chronic Inflammation (Inflammaging) and Its Potential Contribution to Age-Associated Diseases. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, S4–S9. [Google Scholar] [CrossRef]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The Hallmarks of Aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef]
- Pataky, M.W.; Young, W.F.; Nair, K.S. Hormonal and Metabolic Changes of Aging and the Influence of Lifestyle Modifications. Mayo Clin. Proc. 2021, 96, 788–814. [Google Scholar] [CrossRef]
- Ungvari, Z.; Tarantini, S.; Donato, A.J.; Galvan, V.; Csiszar, A. Mechanisms of Vascular Aging. Circ. Res. 2018, 123, 849–867. [Google Scholar] [CrossRef]
- Colloca, G.; Di Capua, B.; Bellieni, A.; Fusco, D.; Ciciarello, F.; Tagliaferri, L.; Valentini, V.; Balducci, L. Biological and Functional Biomarkers of Aging: Definition, Characteristics, and How They Can Impact Everyday Cancer Treatment. Curr. Oncol. Rep. 2020, 22, 115. [Google Scholar] [CrossRef]
- Balducci, L. Studying Cancer Treatment in the Elderly Patient Population. Cancer Cont. 2014, 21, 215–220. [Google Scholar] [CrossRef]
- Kirkwood, K.L. Inflammaging. Immunol. Investig. 2018, 47, 770–773. [Google Scholar] [CrossRef]
- Calder, P.C.; Bosco, N.; Bourdet-Sicard, R.; Capuron, L.; Delzenne, N.; Doré, J.; Franceschi, C.; Lehtinen, M.J.; Recker, T.; Salvioli, S.; et al. Health relevance of the modification of low grade inflammation in ageing (inflammageing) and the role of nutrition. Ageing Res. Rev. 2017, 40, 95–119. [Google Scholar] [CrossRef]
- Hutchinson, A.N.; Tingö, L.; Brummer, R.J. The Potential Effects of Probiotics and ω-3 Fatty Acids on Chronic Low-Grade Inflammation. Nutrients 2020, 12, 2402. [Google Scholar] [CrossRef]
- Rea, I.M.; Gibson, D.S.; McGilligan, V.; McNerlan, S.E.; Alexander, H.D.; Ross, O.A. Age and Age-Related Diseases: Role of Inflammation Triggers and Cytokines. Front. Immunol. 2018, 9, 586. [Google Scholar] [CrossRef]
- Baylis, D.; Bartlett, D.B.; Patel, H.P.; Roberts, H.C. Understanding how we age: Insights into inflammaging. Longev. Healthspan. 2013, 2, 8. [Google Scholar] [CrossRef]
- Chung, H.Y.; Kim, D.H.; Lee, E.K.; Chung, K.W.; Chung, S.; Lee, B.; Seo, A.Y.; Chung, J.H.; Jung, Y.S.; Im, E.; et al. Redefining Chronic Inflammation in Aging and Age-Related Diseases: Proposal of the Senoinflammation Concept. Aging Dis. 2019, 10, 367. [Google Scholar] [CrossRef]
- Inouye, S.K.; Studenski, S.; Tinetti, M.E.; Kuchel, G.A. Geriatric Syndromes: Clinical, Research, and Policy Implications of a Core Geriatric Concept: (See Editorial Comments by Dr. William Hazzard on pp 794–796). J. Am. Geriatr. Soc. 2007, 55, 780–791. [Google Scholar] [CrossRef]
- Cesari, M.; Calvani, R.; Marzetti, E. Frailty in Older Persons. Clin. Geriatr. Med. 2017, 33, 293–303. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. A Biol Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Kim, T.N.; Choi, K.M. Sarcopenia: Definition, Epidemiology, and Pathophysiology. J. Bone Metab. 2013, 20, 1. [Google Scholar] [CrossRef]
- Basualto-AlarcÃn, C.; Varela, D.; Duran, J.; Maass, R.; Estrada, M. Sarcopenia and Androgens: A Link between Pathology and Treatment. Front. Endocrinol. 2014, 5, 217. [Google Scholar] [CrossRef]
- Sattler, F.R. Growth hormone in the aging male. Best. Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 541–555. [Google Scholar] [CrossRef]
- Dai, Z.; Wu, F.; Yeung, E.W.; Li, Y. IGF-IEc expression, regulation and biological function in different tissues. Growth Horm. IGF Res. 2010, 20, 275–281. [Google Scholar] [CrossRef]
- Sorenson, E.J.; Windbank, A.J.; Mandrekar, J.N.; Bamlet, W.R.; Appel, S.H.; Armon, C.; Barkhaus, P.E.; Bosch, P.; Boylan, K.; David, W.S.; et al. Subcutaneous IGF-1 is not beneficial in 2-year ALS trial. Neurology 2008, 71, 1770–1775. [Google Scholar] [CrossRef]
- Rauschenbach, I.Y.; Bogomolova, E.V.; Karpova, E.K.; Adonyeva, N.V.; Faddeeva, N.V.; Menshanov, P.N.; Gruntenko, N.E. Mechanisms of age-specific regulation of dopamine metabolism by juvenile hormone and 20-hydroxyecdysone in Drosophila females. J. Comp. Physiol. B 2011, 181, 19–26. [Google Scholar] [CrossRef]
- Seid, M.A.; Traniello, J.F.A. Age-related changes in biogenic amines in individual brains of the ant Pheidole dentata. Naturwissenschaften 2005, 92, 198–201. [Google Scholar] [CrossRef]
- El Husseiny, I.M.; El Kholy, S.; Mohamed, A.Z.; Meshrif, W.S.; Elbrense, H. Alterations in biogenic amines levels associated with age-related muscular tissue impairment in Drosophila melanogaster. Saudi J. Biol. Sci. 2022, 29, 3739–3748. [Google Scholar] [CrossRef]
- He, Y.; Jasper, H. Studying aging in Drosophila. Methods 2014, 68, 129–133. [Google Scholar] [CrossRef]
- Van Lancker, A.; Verhaeghe, S.; Van Hecke, A.; Vanderwee, K.; Goossens, J.; Beeckman, D. The association between malnutrition and oral health status in elderly in long-term care facilities: A systematic review. Int. J. Nurs. Stud. 2012, 49, 1568–1581. [Google Scholar] [CrossRef]
- Salvesi, C.; Silvi, S.; Fiorini, D.; Scortichini, S.; Sagratini, G.; Palermo, F.A.; De Leone, R.; Egidi, N.; Fatone, L.; Cifani, C.; et al. Impact of a probiotic diet on well-being of healthy senior: THE PROBIOSENIOR PROJECT. J. Appl. Microbiol. 2022, 133, 2941–2953. [Google Scholar] [CrossRef]
- Verdenelli, M.C.; Ghelfi, F.; Silvi, S.; Orpianesi, C.; Cecchini, C.; Cresci, A. Probiotic properties of Lactobacillus rhamnosus and Lactobacillus paracasei isolated from human faeces. Eur. J. Nutr. 2009, 48, 355–363. [Google Scholar] [CrossRef]
- Tamtaji, O.R.; Kouchaki, E.; Salami, M.; Aghadavod, E.; Akbari, E.; Tajabadi-Ebrahimi, M.; Asemi, Z. The Effects of Probiotic Supplementation on Gene Expression Related to Inflammation, Insulin, and Lipids in Patients With Multiple Sclerosis: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Am. Coll. Nutr. 2017, 36, 660–665. [Google Scholar] [CrossRef]
- Zhang, M.; Xu, J.; Wang, T.; Wan, X.; Zhang, F.; Wang, L.; Zhu, X.; Gao, P.; Shu, G.; Jiang, Q.; et al. The Dipeptide Pro-Gly Promotes IGF-1 Expression and Secretion in HepG2 and Female Mice via PepT1-JAK2/STAT5 Pathway. Front. Endocrinol. 2018, 9, 424. [Google Scholar] [CrossRef]
- Bollwein, J.; Volkert, D. Nutritional status according to the mini nutritional assessment (MNA®) and frailty in community dwelling older persons: A close relationship. J. Nutr. Health Aging 2013, 17, 351–356. [Google Scholar] [CrossRef]
- Khan, S.S.; Singer, B.D.; Vaughan, D.E. Molecular and physiological manifestations and measurement of aging in humans. Aging Cell. 2017, 16, 624–633. [Google Scholar] [CrossRef]
- Singh, T.; Newman, A.B. Inflammatory markers in population studies of aging. Ageing Res. Rev. 2011, 10, 319–329. [Google Scholar] [CrossRef]
- Gosetti, F.; Mazzucco, E.; Gennaro, M.C.; Marengo, E. Simultaneous determination of sixteen underivatized biogenic amines in human urine by HPLC-MS/MS. Anal. Bioanal. Chem. 2013, 405, 907–916. [Google Scholar] [CrossRef]
- Friedrich, N.; Krebs, A.; Nauck, M.; Wallaschofski, H. Age- and gender-specific reference ranges for serum insulin-like growth factor I (IGF-I) and IGF-binding protein-3 concentrations on the Immulite 2500: Results of the Study of Health in Pomerania (SHIP). Clin. Chem. Lab. Med. 2010, 48, 115–120. [Google Scholar] [CrossRef]
- Lahiri, S.; Kim, H.; Garcia-Perez, I.; Reza, M.M.; Martin, K.A.; Kundu, P.; Cox, L.M.; Selkrig, J.; Posma, J.M.; Zhang, H.; et al. The gut microbiota influences skeletal muscle mass and function in mice. Sci. Transl. Med. 2019, 011, eaan5662. [Google Scholar] [CrossRef]
- Yan, J.; Herzog, J.W.; Tsang, K.; Brennan, C.A.; Bower, M.A.; Garrett, W.S.; Sartor, B.R.; Aliprantis, A.O.; Charles, J.F. Gut microbiota induce IGF-1 and promote bone formation and growth. Proc. Natl. Acad. Sci. USA 2016, 113, E7554–E7563. [Google Scholar] [CrossRef]
- Yan, J.; Charles, J.F. Gut Microbiota and IGF-1. Calcif. Tissue Int. 2018, 102, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Bruunsgaard, H.; Andersen-Ranberg, K.; Hjelmborg, J.V.B.; Pedersen, B.K.; Jeune, B. Elevated levels of tumor necrosis factor alpha and mortality in centenarians. Am. J. Med. 2003, 115, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Baggiolini, M.; Dewald, B.; Moser, B. Human chemokines: An update. Annu. Rev. Immunol. 1997, 15, 675–705. [Google Scholar] [CrossRef] [PubMed]
- Westbury, L.D.; Fuggle, N.R.; Syddall, H.E.; Duggal, N.A.; Shaw, S.C.; Maslin, K.; Dennison, E.M.; Lord, J.M.; Cooper, C. Relationships Between Markers of Inflammation and Muscle Mass, Strength and Function: Findings from the Hertfordshire Cohort Study. Calcif. Tissue Int. 2018, 102, 287–295. [Google Scholar] [CrossRef]
- Daws, L.C.; Owens, W.A.; Toney, G.M. Using High-Speed Chronoamperometry to Measure Biogenic Amine Release and Uptake In Vivo. In Neurotransmitter Transporters; Humana Press: New York, NY, USA, 2016; pp. 53–81. ISBN 08932336. [Google Scholar]
- Civelli, O.; Bunzow, J.R.; Grandy, D.K. Molecular Diversity of the Dopamine Receptors. Annu. Rev. Pharmacol. Toxicol. 1993, 33, 281–307. [Google Scholar] [CrossRef]
- Maráková, K.; Piešťanský, J.; Zelinková, Z.; Mikuš, P. Simultaneous determination of twelve biogenic amines in human urine as potential biomarkers of inflammatory bowel diseases by capillary electrophoresis—Tandem mass spectrometry. J. Pharm. Biomed. Anal. 2020, 186, 113294. [Google Scholar] [CrossRef]
- Ward, K.D.; Garvey, A.J.; Bliss, R.E.; Sparrow, D.; Young, J.B.; Landsberg, L. Changes in urinary catecholamine excretion after smoking cessation. Pharmacol. Biochem. Behav. 1991, 40, 937–940. [Google Scholar] [CrossRef]
- Guigoz, Y.; Vellas, B. Nutritional Assessment in Older Adults: MNA® 25 years of a Screening Tool & a Reference Standard for Care and Research; What Next? J. Nutr. Health Aging 2021, 25, 528–583. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Biogenic Amines (BAs) | LOQ (µg L−1) | LOD (µg L−1) |
|---|---|---|
| Putrescine (Put) | 7.50 | 2.81 |
| Cadaverine (Cad) | 5.63 | 2.81 |
| Spermidine (Spd) | 7.50 | 2.81 |
| Spermine (Spm) | 5.63 | 2.81 |
| 2-Phenylethylamine (Pea) | 7.50 | 5.63 |
| Histamine (His) | 37.50 | 9.38 |
| Serotonin (5-HT) | 37.50 | 9.38 |
| Tyramine (Tyr) | 9.38 | 7.50 |
| Dopamine (DA) | 75.00 | 37.50 |
| Tryptamine (Try) | 9.38 | 5.63 |
| Epinephrine (E) | 37.50 | 18.75 |
| Gene | Primer Sequence (5′-3′) | Product (bp) | Reference |
|---|---|---|---|
| TNF-α | GTCAACCTCCTCTCTGCCATC CAAAGTAGACCTGCCCAGA | 188 | [32] |
| IGF-1 | CATGTCCTCCTCGCATCTCTA GCAGCACTCATCCACGATA | 212 | [33] |
| GAPDH | AAGCTCATTTCCTGGTATGACAA CGTCTTCCTCTTGTGCTCTTGCTGG | 126 | [32] |
| Analyte | MinDC + 2SD |
|---|---|
| IL-1α | 4.51 |
| IL-22 | 13.60 |
| IP-10 | 4.40 |
| IL-21 | 6.80 |
| G-CSF | 5.66 |
| IFN-γ | 1.79 |
| IL-1β | 2.13 |
| IL-2 | 0.41 |
| IL-4 | 0.38 |
| IL-6 | 0.20 |
| IL-8 | 0.42 |
| IL-10 | 0.93 |
| IL-15 | 0.92 |
| IL-17A | 1.35 |
| MIP-1α | 8.87 |
| PLACEBO | PROBIOTIC | PLACEBO: T0 vs. T1 (p-Value) | PROBIOTIC: T0 vs. T1 (p-Value) | T1: PLACEBO vs. PROBIOTIC (p-Value) | |||
|---|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | ||||
| TNF-α (Δct) | 3.44 ± 1.13 | 4.28 ± 1.12 | 2.95 ± 1.27 | 3.94 ± 1.69 | 0.01366 * | 0.00383 * | 0.21686 |
| TNF-α (pg mL−1) | 57.82 ± 23.52 | 48.60 ± 19.68 | 58.15 ± 19.49 | 46.52 ± 20.85 | 0.09922 | 0.00979 * | 0.36123 |
| IGF-1 (Δct) | 3.11 ± 1.15 | 3.20 ± 0.99 | 2.57 ± 1.08 | 3.05 ± 0.94 | 0.39388 | 0.02684 * | 0.28737 |
| IGF-1 (pg mL−1) | 118.31 ± 23.56 | 121.88 ± 25.68 | 118.80 ± 35.79 | 141.09 ± 44.56 | 0.32885 | 0.01271 * | 0.04523* |
| Placebo | Probiotic | |||
|---|---|---|---|---|
| T0 | T1 | T0 | T1 | |
| G-CSF | 56.53 ± 43.34 | 72.75 ± 60.39 | 52.09 ± 18.12 | 59.03 ± 23.99 |
| IFN-γ | 3.71 ± 1.32 | 1.72 ± 0.88 | 4.12 ± 1.61 | 4.06 ± 3.49 |
| IL-1β | 6.43 ± 2.18 | 16.82 ± 12.64 | 9.62 ± 4.19 | 5.94 ± 2.36 |
| IL-2 | 0.45 ± 0.20 | 0.59 ± 0.45 | 0.39 ± 0.16 | 0.35 ± 0.19 |
| IL-4 | 3.53 ± 2.53 | 4.99 ± 3.61 | 2.21 ± 0.57 | 3.04 ± 1.07 |
| IL-6 | 8.69 ± 1.88 | 5.78 ± 1.16 | 8.96 ± 2.72 | 3.16 ± 0.68 * |
| IL-8 | 57.96 ± 25.16 | 14.96 ± 2.20 | 66.19 ± 29.33 | 12.46 ± 1.05 * |
| IL-10 | 17.23 ± 11.64 | 25.00 ± 18.28 | 11.02 ± 3.86 | 21.82 ± 7.89 |
| IL-15 | 9.66 ± 2.27 | 8.75 ± 2.35 | 7.78 ± 1.30 | 6.67 ± 0.66 |
| IL-17A | 4.49 ± 1.77 | 3.35 ± 2.15 | 5.87 ± 3.91 | 5.05 ± 2.59 |
| MIP-1α | 15.07 ± 5.06 | 6.75 ± 4.80 | 9.21 ± 2.87 | 3.48 ± 1.79 * |
| PLACEBO T0 | PLACEBO T1 | PROBIOTIC T0 | PROBIOTIC T1 * | ||||||
|---|---|---|---|---|---|---|---|---|---|
| MNA Score | Mean ± SD | % Subjects | Mean ± SD | % Subjects | Mean ± SD | % Subjects | Mean ± SD | % Subjects | |
| MALNOURISHED | <17 | 14.85 ± 1.41 | 25.0 | 14.50 ± 1.35 | 25.0 | 14.21 ± 2.32 | 16.6 | 15.67 ± 0.76 | 7.2 |
| AT RISK OF MALNUTRITION | 17–23.5 | 21.00 ± 1.45 | 39.3 | 20.10 ± 1.41 | 35.7 | 21.2 ± 1.19 | 54.8 | 21.18 ± 1.50 | 35.7 |
| NORMAL NUTRITIONAL STATUS | >24 | 25.35 ± 1.23 | 35.7 | 25.09 ± 1.18 | 39.3 | 26.9 ± 1.29 | 28.6 | 24.98 ± 1.42 | 57.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvesi, C.; Silvi, S.; Fiorini, D.; Alessandroni, L.; Sagratini, G.; Palermo, F.A.; De Leone, R.; Egidi, N.; Cifani, C.; Micioni Di Bonaventura, M.V.; et al. Six-Month Synbio® Administration Affects Nutritional and Inflammatory Parameters of Older Adults Included in the PROBIOSENIOR Project. Microorganisms 2023, 11, 801. https://doi.org/10.3390/microorganisms11030801
Salvesi C, Silvi S, Fiorini D, Alessandroni L, Sagratini G, Palermo FA, De Leone R, Egidi N, Cifani C, Micioni Di Bonaventura MV, et al. Six-Month Synbio® Administration Affects Nutritional and Inflammatory Parameters of Older Adults Included in the PROBIOSENIOR Project. Microorganisms. 2023; 11(3):801. https://doi.org/10.3390/microorganisms11030801
Chicago/Turabian StyleSalvesi, Chiara, Stefania Silvi, Dennis Fiorini, Laura Alessandroni, Gianni Sagratini, Francesco Alessandro Palermo, Renato De Leone, Nadaniela Egidi, Carlo Cifani, Maria Vittoria Micioni Di Bonaventura, and et al. 2023. "Six-Month Synbio® Administration Affects Nutritional and Inflammatory Parameters of Older Adults Included in the PROBIOSENIOR Project" Microorganisms 11, no. 3: 801. https://doi.org/10.3390/microorganisms11030801
APA StyleSalvesi, C., Silvi, S., Fiorini, D., Alessandroni, L., Sagratini, G., Palermo, F. A., De Leone, R., Egidi, N., Cifani, C., Micioni Di Bonaventura, M. V., Amedei, A., Niccolai, E., Scocchera, F., Mannucci, F., Valeriani, V., Malavasi, M., Servili, S., Casula, A., Cresci, A., ... Verdenelli, M. C. (2023). Six-Month Synbio® Administration Affects Nutritional and Inflammatory Parameters of Older Adults Included in the PROBIOSENIOR Project. Microorganisms, 11(3), 801. https://doi.org/10.3390/microorganisms11030801