

Could the Microbiota Be a Predictive Factor for the Clinical Response to Probiotic Supplementation in IBS-D? A Cohort Study
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Ethics Statement
2.2. Supplementation
2.3. Patients
2.4. Study Procedure
2.5. Definition of Clinical Response
2.6. Evaluation of Intestinal Permeability
2.7. Rectosigmoidoscopy and Probe-Based Confocal Laser Endomicroscopy (pCLE) Procedure
2.8. Microbiota Analysis
2.8.1. 16S rRNA Sequencing
2.8.2. 16S Data Analysis
2.9. Statistical Analysis
3. Results
3.1. Patient Population
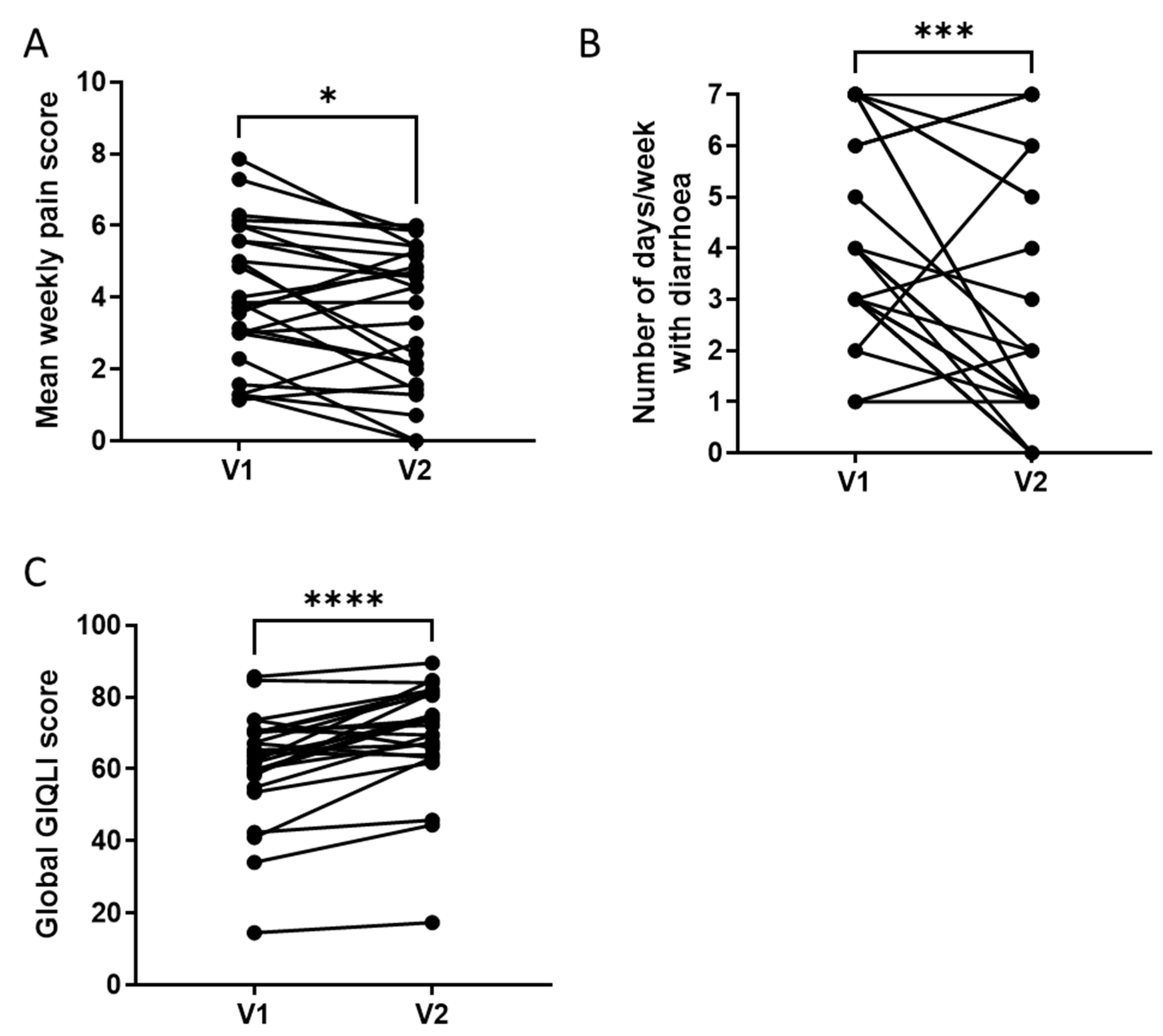
3.2. Clinical Response to a 4-Week Supplementation with the Multistrain Probiotic
3.3. Effects of a 4-Week Supplementation with the Multistrain Probiotic on Intestinal Permeability
3.4. Effects of a 4-Week Supplementation with the Multistrain Probiotic on pCLE Parameters
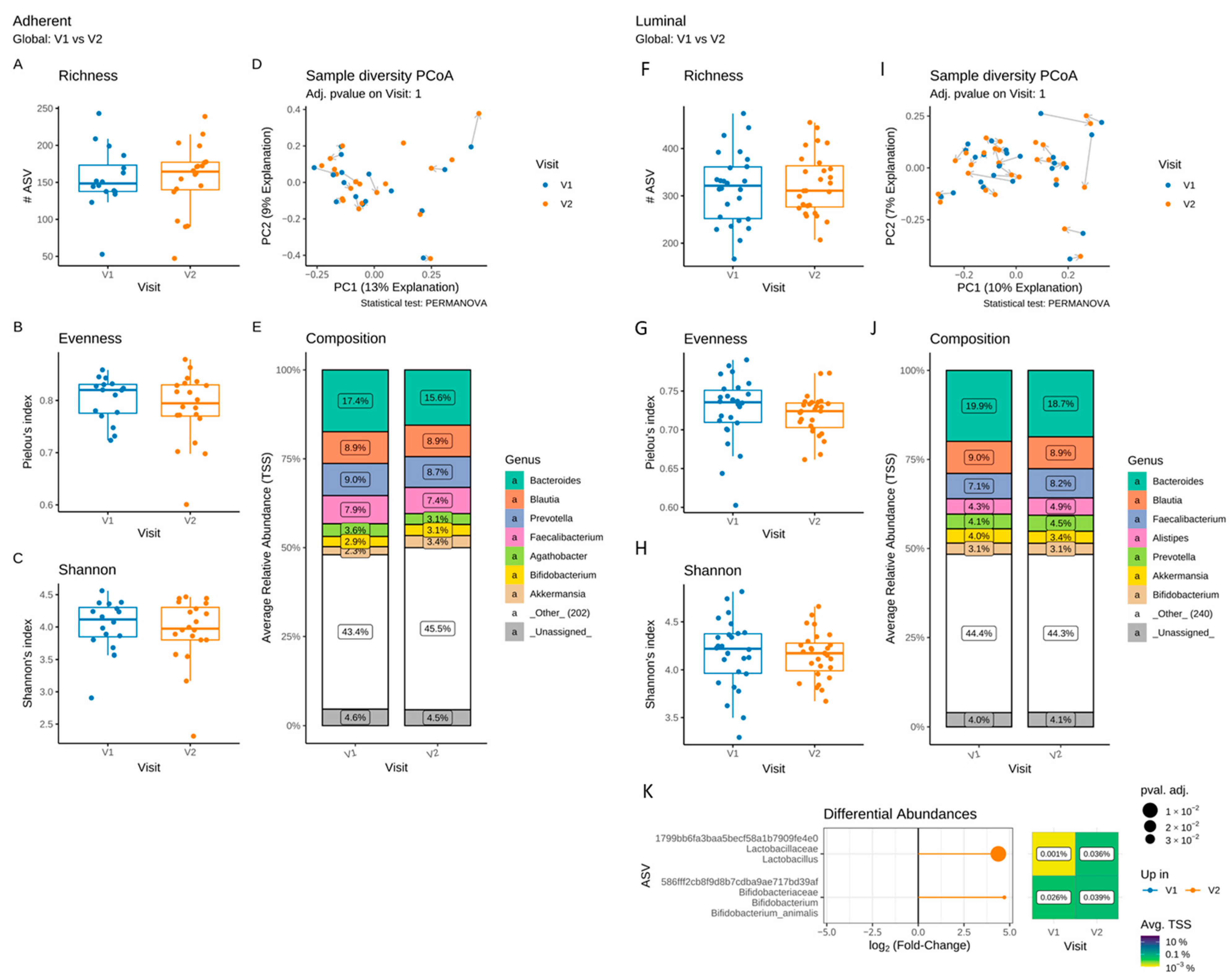
3.5. Effects of a 4-Week Supplementation with the Multistrain Probiotic on the Adherent and Luminal Gut Microbiota
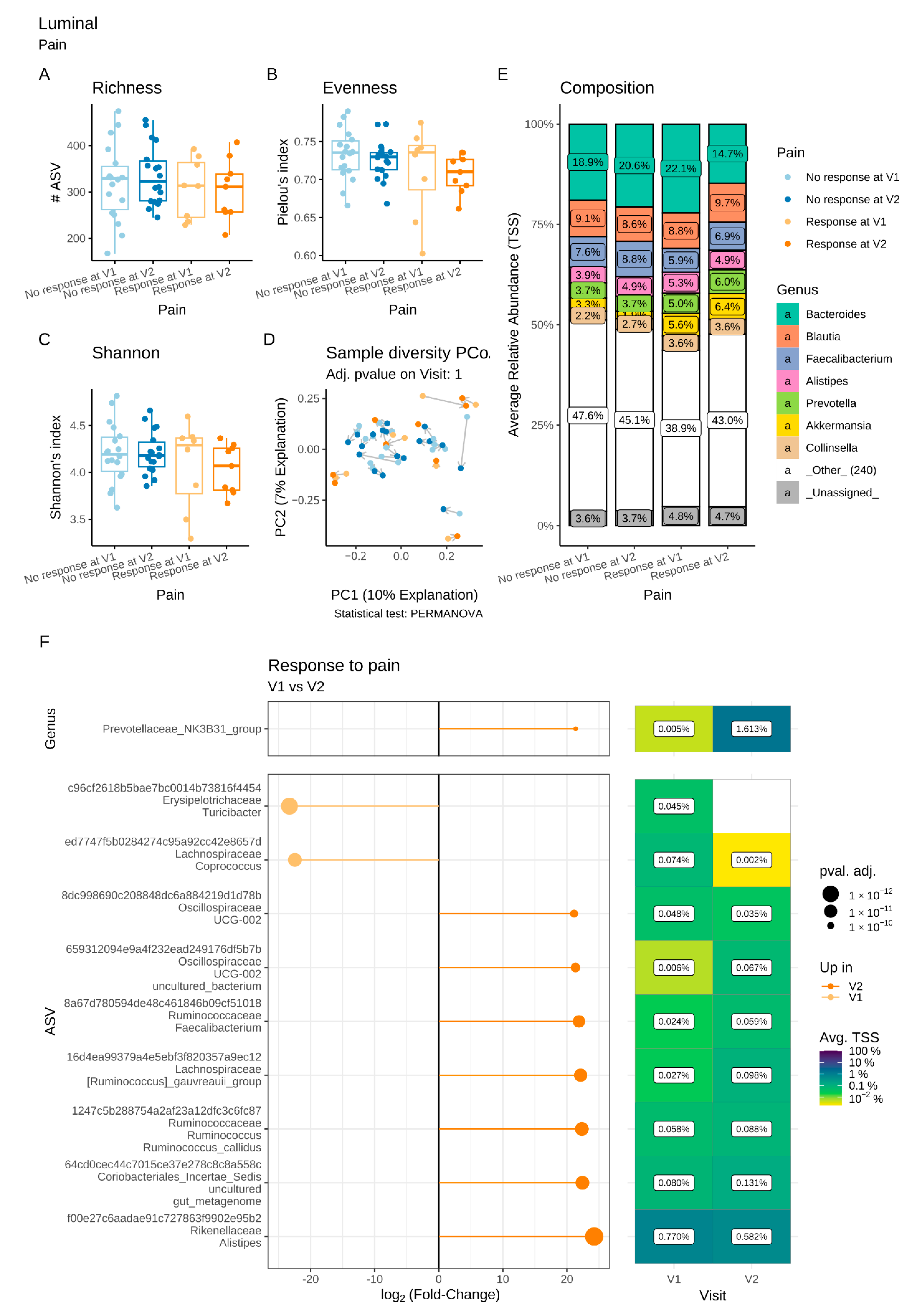
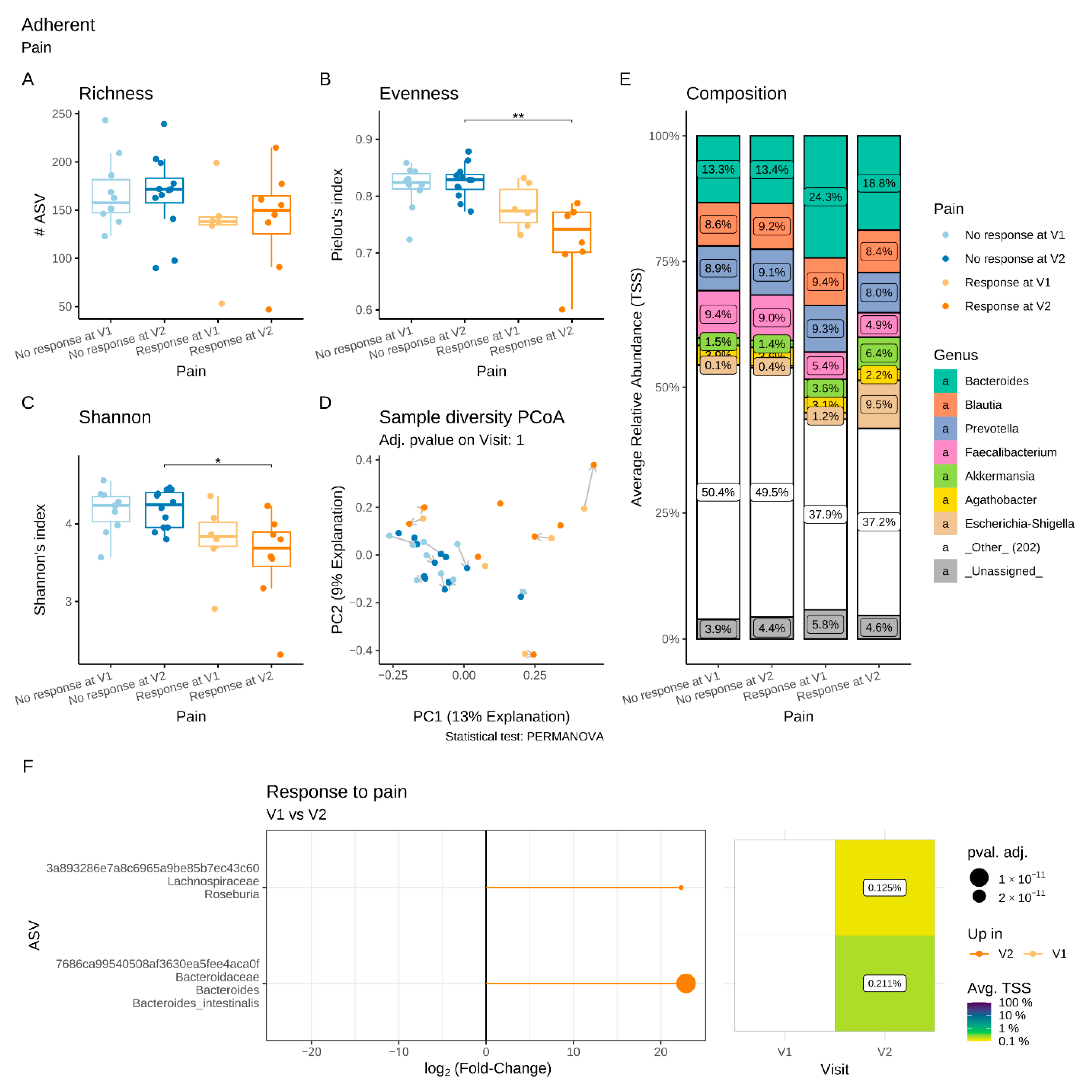
3.6. Differential Luminal and Adherent Microbiota Composition in Pain R and Diarrhoea R
3.6.1. Microbiota Changes in Pain R
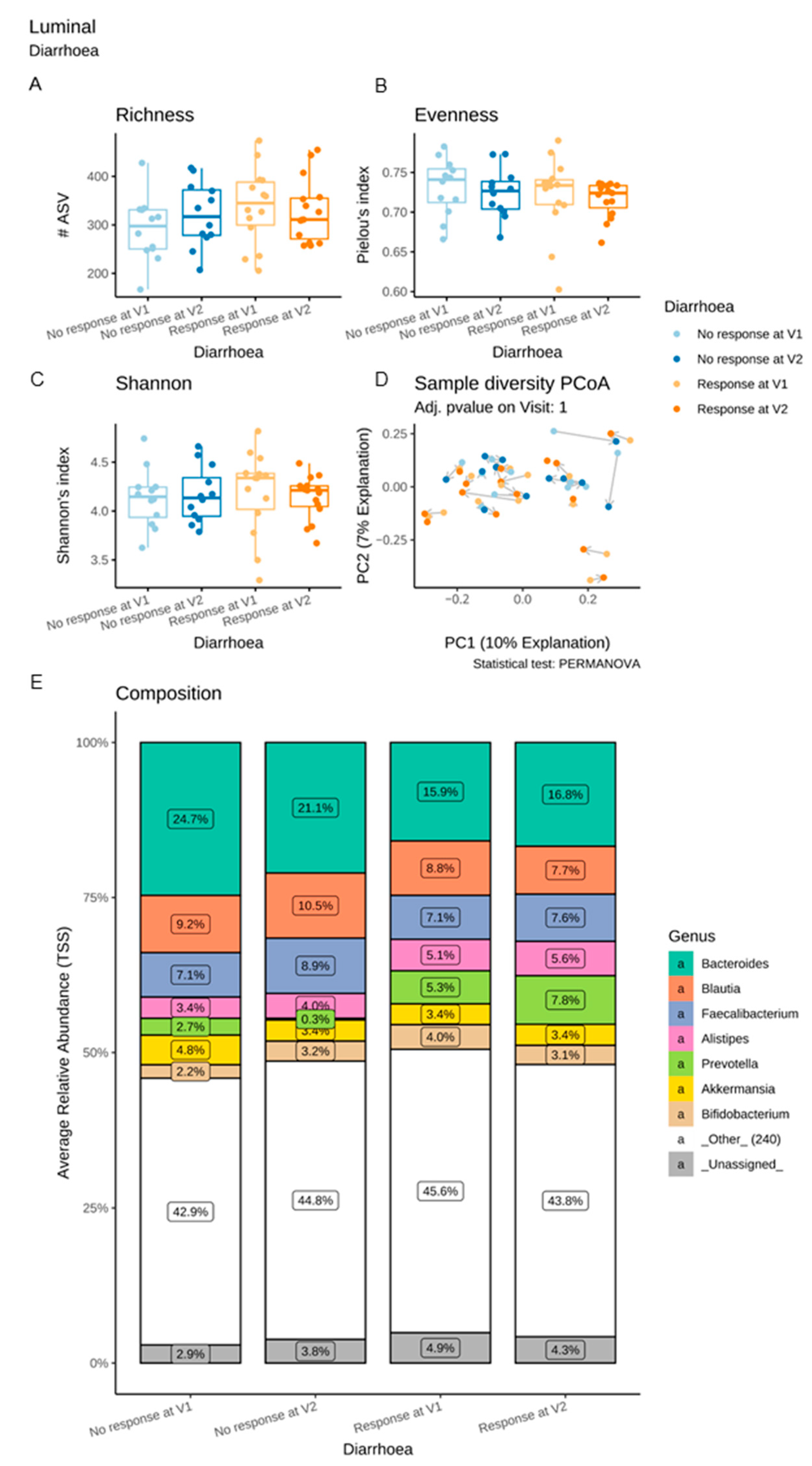
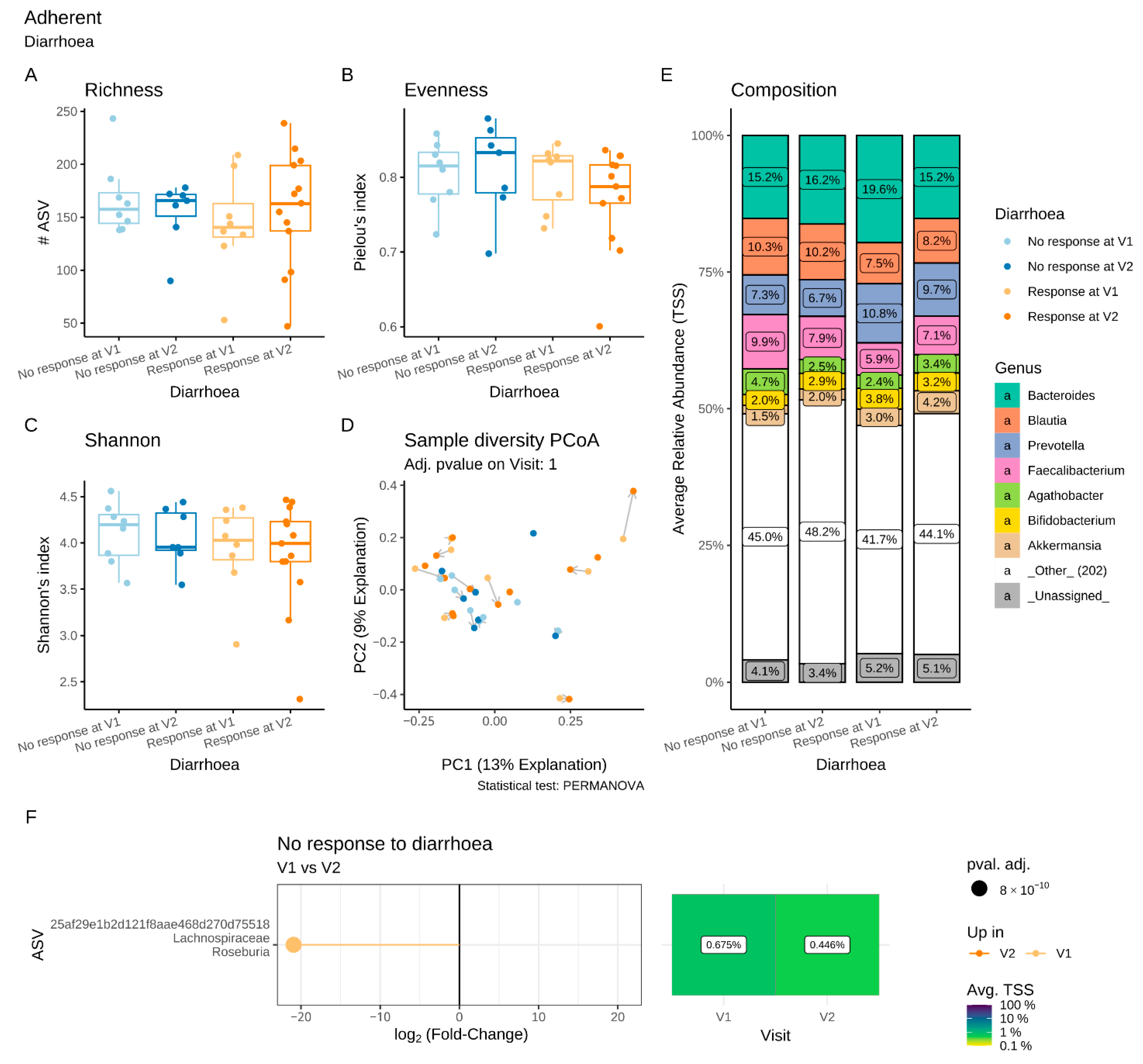
3.6.2. Microbiota Changes in Diarrhoea R
3.7. Compliance and Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ducrotte, P.; Sawant, P.; Jayanthi, V. Clinical trial: Lactobacillus plantarum 299v (DSM 9843) improves symptoms of irritable bowel syndrome. World J. Gastroenterol. 2012, 18, 4012–4018. [Google Scholar] [CrossRef] [PubMed]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e3. [Google Scholar] [CrossRef] [PubMed]
- Carroll, I.M.; Ringel-Kulka, T.; Keku, T.O.; Chang, Y.-H.; Packey, C.D.; Sartor, R.B.; Ringel, Y. Molecular analysis of the luminal- and mucosal-associated intestinal microbiota in diarrhea-predominant irritable bowel syndrome. Am. J. Physiol. Gastrointest. Liver Physiol. 2011, 301, G799–G807. [Google Scholar] [CrossRef] [PubMed]
- Carroll, I.M.; Ringel-Kulka, T.; Siddle, J.P.; Ringel, Y. Alterations in composition and diversity of the intestinal microbiota in patients with diarrhea-predominant irritable bowel syndrome. Neurogastroenterol. Motil. 2012, 24, 521–530.e248. [Google Scholar] [CrossRef] [PubMed]
- Pozuelo, M.; Panda, S.; Santiago, A.; Mendez, S.; Accarino, A.; Santos, J.; Guarner, F.; Azpiroz, F.; Manichanh, C. Reduction of butyrate- and methane-producing microorganisms in patients with Irritable Bowel Syndrome. Sci. Rep. 2015, 5, 12693. [Google Scholar] [CrossRef]
- Liu, H.-N.; Wu, H.; Chen, Y.-Z.; Chen, Y.-J.; Shen, X.-Z.; Liu, T.-T. Altered molecular signature of intestinal microbiota in irritable bowel syndrome patients compared with healthy controls: A systematic review and meta-analysis. Dig. Liver Dis. 2017, 49, 331–337. [Google Scholar] [CrossRef]
- Lee, B.J.; Bak, Y.-T. Irritable bowel syndrome, gut microbiota and probiotics. J. Neurogastroenterol. Motil. 2011, 17, 252–266. [Google Scholar] [CrossRef]
- Alard, J.; Peucelle, V.; Boutillier, D.; Breton, J.; Kuylle, S.; Pot, B.; Holowacz, S.; Grangette, C. New probiotic strains for inflammatory bowel disease management identified by combining in vitro and in vivo approaches. Benef. Microbes 2018, 9, 317–331. [Google Scholar] [CrossRef]
- Carco, C.; Young, W.; Gearry, R.B.; Talley, N.J.; McNabb, W.C.; Roy, N.C. Increasing Evidence That Irritable Bowel Syndrome and Functional Gastrointestinal Disorders Have a Microbial Pathogenesis. Front. Cell. Infect. Microbiol. 2020, 10, 468. [Google Scholar] [CrossRef]
- Barbara, G.; Zecchi, L.; Barbaro, R.; Cremon, C.; Bellacosa, L.; Marcellini, M.; de Giorgio, R.; Corinaldesi, R.; Stanghellini, V. Mucosal Permeability and Immune Activation as Potential Therapeutic Targets of Probiotics in Irritable Bowel Syndrome. J. Clin. Gastroenterol. 2012, 46, S52–S55. [Google Scholar] [CrossRef]
- Ishaque, S.M.; Khosruzzaman, S.M.; Ahmed, D.S.; Sah, M.P. A randomized placebo-controlled clinical trial of a multi-strain probiotic formulation (Bio-Kult®) in the management of diarrhea-predominant irritable bowel syndrome. BMC Gastroenterol. 2018, 18, 1075. [Google Scholar] [CrossRef]
- Tiequn, B.; Guanqun, C.; Shuo, Z. Therapeutic effects of Lactobacillus in treating irritable bowel syndrome: A meta-analysis. Intern Med. 2015, 54, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Liang, L.; Deng, H.; Guo, J.; Shu, H.; Zhang, L. Efficacy and Safety of Probiotics in Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2020, 11, 332. [Google Scholar] [CrossRef]
- Sun, J.-R.; Kong, C.-F.; Qu, X.-K.; Deng, C.; Lou, Y.-N.; Jia, L.-Q. Efficacy and safety of probiotics in irritable bowel syndrome: A systematic review and meta-analysis. Saudi J. Gastroenterol. 2020, 26, 66–77. [Google Scholar] [CrossRef]
- Zhang, T.; Zhang, C.; Zhang, J.; Sun, F.; Duan, L. Efficacy of Probiotics for Irritable Bowel Syndrome: A Systematic Review and Network Meta-Analysis. Front. Cell. Infect. Microbiol. 2022, 12, 859967. [Google Scholar] [CrossRef] [PubMed]
- Hungin, A.P.; Mulligan, C.; Pot, B.; Whorwell, P.; Agreus, L.; Fracasso, P.; Lionis, C.; Mendive, J.; Philippart de Foy, J.M.; Rubin, G.; et al. Systematic review: Probiotics in the management of lower gastrointestinal symptoms in clinical practice—An evidence-based international guide. Aliment. Pharmacol. Ther 2013, 38, 864–886. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Habukawa, C.; Nobuta, Y.; Moriguchi, N.; Takemura, T. The effect of Lactobacillus brevis KB290 against irritable bowel syndrome: A placebo-controlled double-blind crossover trial. Biopsychosoc. Med. 2012, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.P.; Choi, Y.M.; Kim, W.H.; Hong, S.P.; Park, J.-M.; Kim, J.; Kwon, O.; Lee, E.H.; Hahm, K.B. A double blind, placebo-controlled, randomized clinical trial that breast milk derived-Lactobacillus gasseri BNR17 mitigated diarrhea-dominant irritable bowel syndrome. J. Clin. Biochem. Nutr. 2018, 62, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.D.; Antony, J.M.; Crowley, D.C.; Piano, A.; Bhardwaj, R.; Tompkins, T.A.; Evans, M. Efficacy of Lactobacillus paracasei HA-196 and Bifidobacterium longum R0175 in Alleviating Symptoms of Irritable Bowel Syndrome (IBS): A Randomized, Placebo-Controlled Study. Nutrients 2020, 12, 1159. [Google Scholar] [CrossRef]
- Martoni, C.J.; Srivastava, S.; Leyer, G.J. Lactobacillus acidophilus DDS-1 and Bifidobacterium lactis UABla-12 Improve Abdominal Pain Severity and Symptomology in Irritable Bowel Syndrome: Randomized Controlled Trial. Nutrients 2020, 12, 363. [Google Scholar] [CrossRef]
- American Gastroenterological Association. Clinical Decision Support Tool: IBS Treatment. Gastroenterology 2022, 163, 152. [Google Scholar] [CrossRef]
- Tap, J.; Derrien, M.; Törnblom, H.; Brazeilles, R.; Cools-Portier, S.; Doré, J.; Störsrud, S.; Le Nevé, B.; Öhman, L.; Simrén, M. Identification of an Intestinal Microbiota Signature Associated with Severity of Irritable Bowel Syndrome. Gastroenterology 2017, 152, 111–123.e8. [Google Scholar] [CrossRef] [PubMed]
- Nebot-Vivinus, M.; Harkat, C.; Bzioueche, H.; Cartier, C.; Plichon-Dainese, R.; Moussa, L.; Eutamene, H.; Pishvaie, D.; Holowacz, S.; Seyrig, C.; et al. Multispecies probiotic protects gut barrier function in experimental models. World J. Gastroenterol. 2014, 20, 6832–6843. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Bousquet, J.; Kwiatkowski, F.; Lescure, G.; Pezet, D.; Chipponi, J. Première validation de la version française de l’index de qualité de vie pour les maladies digestives (GIQLI). Gastroenterol. Clin. Biol. 1999, 23, 25–31. [Google Scholar]
- Pimentel, M.; Cash, B.D.; Lembo, A.; Wolf, R.A.; Israel, R.J.; Schoenfeld, P. Repeat Rifaximin for Irritable Bowel Syndrome: No Clinically Significant Changes in Stool Microbial Antibiotic Sensitivity. Dig. Dis. Sci. 2017, 62, 2455–2463. [Google Scholar] [CrossRef]
- Sequeira, I.R.; Lentle, R.G.; Kruger, M.C.; Hurst, R.D.; Hogan, S.P. Standardising the Lactulose Mannitol Test of Gut Permeability to Minimise Error and Promote Comparability. PLoS ONE 2014, 9, e99256. [Google Scholar] [CrossRef]
- Meurette, G.; Blanchard, C.; Duchalais-Dassonneville, E.; Coquenlorge, S.; Aubert, P.; Wong, M.; Lehur, P.-A.; Neunlist, M. Sacral nerve stimulation enhances epithelial barrier of the rectum: Results from a porcine model. Neurogastroenterol. Motil. 2012, 24, 267–273.e110. [Google Scholar] [CrossRef]
- Quénéhervé, L.; David, G.; Bourreille, A.; Hardouin, J.B.; Rahmi, G.; Neunlist, M.; Brégeon, J.; Coron, E. Quantitative assessment of mucosal architecture using computer-based analysis of confocal laser endomicroscopy in inflammatory bowel diseases. Gastrointest. Endosc. 2019, 89, 626–636. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef]
- Sisson, G.; Ayis, S.; Sherwood, R.A.; Bjarnason, I. Randomised clinical trial: A liquid multi-strain probiotic vs. placebo in the irritable bowel syndrome—A 12 week double-blind study. Aliment. Pharmacol. Ther. 2014, 40, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Skrzydło-Radomańska, B.; Prozorow-Król, B.; Cichoż-Lach, H.; Majsiak, E.; Bierła, J.B.; Kanarek, E.; Sowińska, A.; Cukrowska, B. The Effectiveness and Safety of Multi-Strain Probiotic Preparation in Patients with Diarrhea-Predominant Irritable Bowel Syndrome: A Randomized Controlled Study. Nutrients 2021, 13, 756. [Google Scholar] [CrossRef] [PubMed]
- Hanning, N.; Edwinson, A.L.; Ceuleers, H.; Peters, S.A.; de Man, J.G.; Hassett, L.C.; de Winter, B.Y.; Grover, M. Intestinal barrier dysfunction in irritable bowel syndrome: A systematic review. Ther. Adv. Gastroenterol. 2021, 14, 1756284821993586. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Zhang, B.; Verne, G.N. Intestinal membrane permeability and hypersensitivity in the irritable bowel syndrome. Pain 2009, 146, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Gecse, K.; Roka, R.; Sera, T.; Rosztoczy, A.; Annahazi, A.; Izbeki, F.; Nagy, F.; Molnar, T.; Szepes, Z.; Pavics, L.; et al. Leaky gut in patients with diarrhea-predominant irritable bowel syndrome and inactive ulcerative colitis. Digestion 2012, 85, 40–46. [Google Scholar] [CrossRef]
- Boonma, P.; Shapiro, J.M.; Hollister, E.B.; Badu, S.; Wu, Q.; Weidler, E.M.; Abraham, B.P.; Devaraj, S.; Luna, R.A.; Versalovic, J.; et al. Probiotic VSL#3 Treatment Reduces Colonic Permeability and Abdominal Pain Symptoms in Patients with Irritable Bowel Syndrome. Front. Pain Res. 2021, 2, S230. [Google Scholar] [CrossRef]
- Zeng, J.; Li, Y.-Q.; Zuo, X.-L.; Zhen, Y.-B.; Yang, J.; Liu, C.-H. Clinical trial: Effect of active lactic acid bacteria on mucosal barrier function in patients with diarrhoea-predominant irritable bowel syndrome. Aliment. Pharmacol. Ther. 2008, 28, 994–1002. [Google Scholar] [CrossRef]
- Caviglia, G.P.; Tucci, A.; Pellicano, R.; Fagoonee, S.; Rosso, C.; Abate, M.L.; Olivero, A.; Armandi, A.; Vanni, E.; Saracco, G.M.; et al. Clinical Response and Changes of Cytokines and Zonulin Levels in Patients with Diarrhoea-Predominant Irritable Bowel Syndrome Treated with Bifidobacterium Longum ES1 for 8 or 12 Weeks: A Preliminary Report. J. Clin. Med. 2020, 9, 2353. [Google Scholar] [CrossRef]
- Ait Abdellah, S.; Gal, C.; Laterza, L.; Velenza, V.; Settanni, C.R.; Napoli, M.; Schiavoni, E.; Mora, V.; Petito, V.; Gasbarrini, A. Effect of a multistrain probiotic on leaky gut in patients with diarrhea-predominant irritable bowel syndrome (IBS-D): A pilot study. Dig. Dis. 2022. [Google Scholar] [CrossRef]
- Rajilić-Stojanović, M.; Biagi, E.; Heilig, H.G.H.J.; Kajander, K.; Kekkonen, R.A.; Tims, S.; de Vos, W.M. Global and deep molecular analysis of microbiota signatures in fecal samples from patients with irritable bowel syndrome. Gastroenterology 2011, 141, 1792–1801. [Google Scholar] [CrossRef]
- Hod, K.; Dekel, R.; Aviv Cohen, N.; Sperber, A.; Ron, Y.; Boaz, M.; Berliner, S.; Maharshak, N. The effect of a multispecies probiotic on microbiota composition in a clinical trial of patients with diarrhea-predominant irritable bowel syndrome. Neurogastroenterol. Motil. 2018, 30, e13456. [Google Scholar] [CrossRef] [PubMed]
- Michail, S.; Kenche, H. Gut microbiota is not modified by Randomized, Double-blind, Placebo-controlled Trial of VSL#3 in Diarrhea-predominant Irritable Bowel Syndrome. Probiotics Antimicrob. Proteins 2011, 3, 1–7. [Google Scholar] [PubMed]
- Shin, S.Y.; Park, S.; Moon, J.M.; Kim, K.; Kim, J.W.; Chun, J.; Lee, T.H.; Choi, C.H. Compositional Changes in the Gut Microbiota of Responders and Non-responders to Probiotic Treatment Among Patients with Diarrhea-predominant Irritable Bowel Syndrome: A Post Hoc Analysis of a Randomized Clinical Trial. J. Neurogastroenterol. Motil. 2022, 28, 642–654. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Teng, K.; Liu, Y.; Shi, W.; Zhang, J.; Dong, E.; Zhang, X.; Tao, Y.; Zhong, J. Lactobacillus plantarum PFM 105 Promotes Intestinal Development Through Modulation of Gut Microbiota in Weaning Piglets. Front. Microbiol. 2019, 10, 90. [Google Scholar] [CrossRef] [PubMed]
- Deleu, S.; Machiels, K.; Raes, J.; Verbeke, K.; Vermeire, S. Short chain fatty acids and its producing organisms: An overlooked therapy for IBD? EBioMedicine 2021, 66, 103293. [Google Scholar] [CrossRef] [PubMed]
- Mazzawi, T.; Hausken, T.; Hov, J.R.; Valeur, J.; Sangnes, D.A.; El-Salhy, M.; Gilja, O.H.; Hatlebakk, J.G.; Lied, G.A. Clinical response to fecal microbiota transplantation in patients with diarrhea-predominant irritable bowel syndrome is associated with normalization of fecal microbiota composition and short-chain fatty acid levels. Scand. J. Gastroenterol. 2019, 54, 690–699. [Google Scholar] [CrossRef]
- El-Salhy, M.; Mazzawi, T.; Hausken, T.; Hatlebakk, J.G. Irritable bowel syndrome patients who are not likely to respond to fecal microbiota transplantation. Neurogastroenterol. Motil. 2022, 34, e14353. [Google Scholar] [CrossRef]
- Pittayanon, R.; Lau, J.T.; Yuan, Y.; Leontiadis, G.I.; Tse, F.; Surette, M.; Moayyedi, P. Gut Microbiota in Patients with Irritable Bowel Syndrome-A Systematic Review. Gastroenterology 2019, 157, 97–108. [Google Scholar] [CrossRef]
- Janda, J.M.; Abbott, S.L. The Genus Hafnia: From Soup to Nuts. Clin. Microbiol. Rev. 2006, 19, 12–28. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| V1 | V2 | p | |
|---|---|---|---|
| Global | 60.6 ± 14.4 | 68.7 ± 14.95 | <0.0001 |
| Sub-dimensions | |||
| Symptom | 59.6 ± 12.3 | 68.6 ± 14.5 | <0.0001 |
| Emotion | 61.9 ± 18.0 | 72.2 ± 20.8 | 0.0008 |
| Physical function | 54.1 ± 23.4 | 60.7 ± 22.0 | 0.007 |
| Social function | 67.8 ± 23.3 | 73.0 ± 21.6 | 0.03 |
| Medical treatment | 98.8 ± 5.5 | 93.0 ± 17.0 | 0.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchix, J.; Quénéhervé, L.; Bordron, P.; Aubert, P.; Durand, T.; Oullier, T.; Blondeau, C.; Ait Abdellah, S.; Bruley des Varannes, S.; Chaffron, S.; et al. Could the Microbiota Be a Predictive Factor for the Clinical Response to Probiotic Supplementation in IBS-D? A Cohort Study. Microorganisms 2023, 11, 277. https://doi.org/10.3390/microorganisms11020277
Marchix J, Quénéhervé L, Bordron P, Aubert P, Durand T, Oullier T, Blondeau C, Ait Abdellah S, Bruley des Varannes S, Chaffron S, et al. Could the Microbiota Be a Predictive Factor for the Clinical Response to Probiotic Supplementation in IBS-D? A Cohort Study. Microorganisms. 2023; 11(2):277. https://doi.org/10.3390/microorganisms11020277
Chicago/Turabian StyleMarchix, Justine, Lucille Quénéhervé, Philippe Bordron, Philippe Aubert, Tony Durand, Thibauld Oullier, Claude Blondeau, Samira Ait Abdellah, Stanislas Bruley des Varannes, Samuel Chaffron, and et al. 2023. "Could the Microbiota Be a Predictive Factor for the Clinical Response to Probiotic Supplementation in IBS-D? A Cohort Study" Microorganisms 11, no. 2: 277. https://doi.org/10.3390/microorganisms11020277
APA StyleMarchix, J., Quénéhervé, L., Bordron, P., Aubert, P., Durand, T., Oullier, T., Blondeau, C., Ait Abdellah, S., Bruley des Varannes, S., Chaffron, S., Coron, E., & Neunlist, M. (2023). Could the Microbiota Be a Predictive Factor for the Clinical Response to Probiotic Supplementation in IBS-D? A Cohort Study. Microorganisms, 11(2), 277. https://doi.org/10.3390/microorganisms11020277